
Abstract
Objective
To investigate the effect of individualized exercise on exercise capacity and health-related quality of life (HRQoL) in uraemic patients during maintenance haemodialysis (MHD).
Methods
Patients receiving MHD were divided randomly into a test group, who underwent recumbent cycling exercise during dialysis, and a control group, who performed simple stretching exercises. The same dialysis protocol was used for all study participants. At study start and after 12 weeks, exercise capacity was measured using tests of physical ability; HRQoL was measured using the kidney disease quality of life score (KDQOL-SF™).
Results
A total of 65 patients were included in the study: 33 in the control group and 32 in the test group. There were no significant differences in patient characteristics between the two groups at baseline. After 12 weeks, there were significant improvements in exercise capacity and in many of the items of the KDQOL-SF™ in the test group compared with the control group.
Conclusion
Individualized exercise during MHD significantly improved the exercise capacity and HRQoL for uraemic patients within a short time period, and could therefore be used as a simple, cost-effective therapeutic approach.
Introduction
Although the short-term survival of patients undergoing maintenance haemodialysis (MHD) has been substantially improved with the development of blood purification technology, 1 low exercise capacity continues to affect patients’ health-related quality of life (HRQoL). 2 It has been reported that exercise can have long-term benefits in a variety of chronic diseases. 3 A number of studies have shown that exercise, particularly during dialysis, can improve HRQoL in patients on haemodialysis, and prevent haemodialysis-associated complications.4–6 However, in these studies, the conclusions on the effects of exercise differ and there was a lack of uniform standards for the selection of exercise modalities and determination of the exercise load.4–6 In China, many patients are unwilling to do physical exercise and are even fearful of it due to a lack of knowledge of its benefits and the influence of the traditional idea that patients should rest. To date, few studies have investigated the beneficial effects of exercise in Chinese patients undergoing MHD. In the present study, individualized exercises performed on a recumbent stationary bike were used to investigate the effects of exercise on exercise capacity and HRQoL in patients with uraemia undergoing MHD.
Patients and methods
Patients
Outpatients receiving long-term MHD (haemodialysis three times per week) at the Beilun People’s Hospital, Ningbo, China, were enrolled sequentially in the study between March 2012 and June 2012. Inclusion criteria included relatively stable disease, good compliance and co-operation with the doctor, no apparent cardiovascular complications (such as heart failure, severe arrhythmia, angina or cerebrovascular disease) or infection, no orthopaedic problems that would prevent cycling during dialysis, blood pressure <180/100 mmHg, and haemodialysis duration >3 months. Patients with the following conditions were excluded from the study: any chronic diseases not under control; retinal laser treatment; history of acute myocardial infarction; joint replacement or fracture of the lower limb within the previous 6 months; severe cognitive disturbance. Patients fulfilling the inclusion criteria were divided randomly into a test group and a control group using a computerized random number generator.
Written informed consent was obtained from all study participants and the study protocol was approved by the Ethics Committee of Zhejiang University, Hangzhou, China.
Interventions
The exercise model and the optimum range of exercise loads suitable for use during haemodialysis were identified through pretrial research (unpublished data) involving monitoring bike energy consumption, heart rate and blood pressure.2,7 For each patient in the test group, the optimum individualized exercise load was calculated during the first dialysis session of the study by increasing gradually from a low exercise load until each session was associated with energy consumption of 70–100 calories, a Borg tiredness score 8 of 12–16 and an increase in the heart rate of 20 beats/min. This regimen was used for all the subsequent exercise sessions for that patient. Patients in the test group performed a 5-min warm-up on the bike and then performed 10–15 min of recumbent cycling during each haemodialysis session; the time period varied depending on the individualized regimen for each patient. Patients in the control group were required to do some simple stretching exercises for 10–15 min during dialysis. Blood pressure and heart rate were monitored every 5 min during exercise in both groups. All patients were studied for 12 weeks (36 haemodialysis sessions). Any adverse reactions were recorded.
Dialysis
The same dialysis protocol was used for all patients: haemodialysis was performed three times per week in 4-h sessions using a TS-1.6UL dialyser (Toray Medical, Tokyo, Japan) with bicarbonate dialysis solution, a blood flow rate of 200–250 ml/min and a dialysis flow rate of 500 ml/min.
All patients received standard monitoring during haemodialysis. Blood pressure was maintained around 140/90 mmHg by antihypertensive agents, and the intake of salt and water was controlled to keep weight gain within 3–5% of the baseline body weight.
Patient assessment
The primary monitoring indicators (exercise capacity and the kidney disease quality of life score [KDQOL-SF™; www.rand.org) were measured in both groups at the beginning of the study and after 12 weeks.
Exercise capacity
The purpose and methods for the exercise capacity tests were explained to the patient prior to the tests being performed. Patients were allowed to familiarize themselves with the test methods and environment, and were instructed to complete the tests at their own pace, slowing down or taking a break if necessary. The following tests were conducted:
Six-minute walk test
The patient was required to walk back and forth for 6 min in a quiet, well-ventilated 30 m corridor; the distance walked measured, as described previously by Guyatt et al. 9
Time to walk up and down 22 steps
the patient was required to climb up and down 22 steps (vertical height ∼3.3 m) and the time taken was documented.
Sit-to-stand test
The number of times the patient could stand up and then sit down repeatedly on a chair of standard height within 1 min was recorded.
Grip strength test
Grip strength was measured using a T.K.K.5001 Grip A dynamometer (Takei Scientific Instruments, Niigata City, Japan); the mean of three measurements of grip was calculated for each patient.
Time to perform 10 sit-to-stand manoeuvres
The time taken for 10 manoeuvres in which the patient moved from the sitting position to a full standing position, with an upright trunk and the hips and knees extended, then returned to the sitting position, was measured.
Heart rate, blood pressure and respiratory rate were recorded, and vital signs were monitored, before and after the tests. Tests were stopped if the patient developed arrhythmia, dizziness, angina or shortness of breath.
KDQOL-SF™
A Chinese version of the KDQOL-SF™ devised by Cheung et al. 10 (was used to assess HRQoL. This assessment consisted of two parts: kidney disease-targeted areas and a health status questionnaire (Short Form-36 [SF-36]). The kidney disease-targeted areas included 43 items in 11 categories: symptom/problem list; effects of kidney disease; burden of kidney disease; work status; cognitive function; quality of social interaction; social support; sexual function; sleep; patient satisfaction; encouragement given by dialysis staff. The SF-36 questionnaire includes eight categories assessing each patient’s subjective HRQoL: physical function; physical role limitations; body pain; general health; energy/fatigue; social function; emotional role limitations; emotional wellbeing. The questionnaire was completed by the patients themselves under the guidance of the research staff at the start of the study and after 12 weeks. Each category generates a score ranging between 0 and 100, with a higher score indicating a better HRQoL. Overall scores were also calculated for the kidney disease-targeted areas and SF-36 as described by Hays et al. 11
Data analyses
A normality test was performed for continuous variables; those with a normal distribution were expressed as mean ± SD, whereas those that did not have a normal distribution were expressed as the median and inter-quartile range. Comparisons between and within the groups were made using independent-samples Student’s t-test for continuous variables and χ2-test for numerical data. A P-value <0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS® software, version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
A total of 69 patients were initially enrolled in the study and were divided randomly between the test group (n = 34) and the control group (n = 35). Four patients were withdrawn from the study: in the test group one patient underwent a kidney transplant and one patient was transferred to another hospital for haemodialysis treatment; in the control group one patient was unwilling to continue and one patient died from an unrelated cause (Figure 1). Therefore, 65 patients completed the whole study, giving a completion rate of 94.2% and drop-out rates in the test and control groups of 5.9% and 5.7%, respectively.
Flow diagram of a study investigating the effects of exercise intervention in patients receiving maintenance haemodialysis.
Demographic and clinical characteristics of haemodialysis patients performing exercise during haemodialysis (test group) and controls.
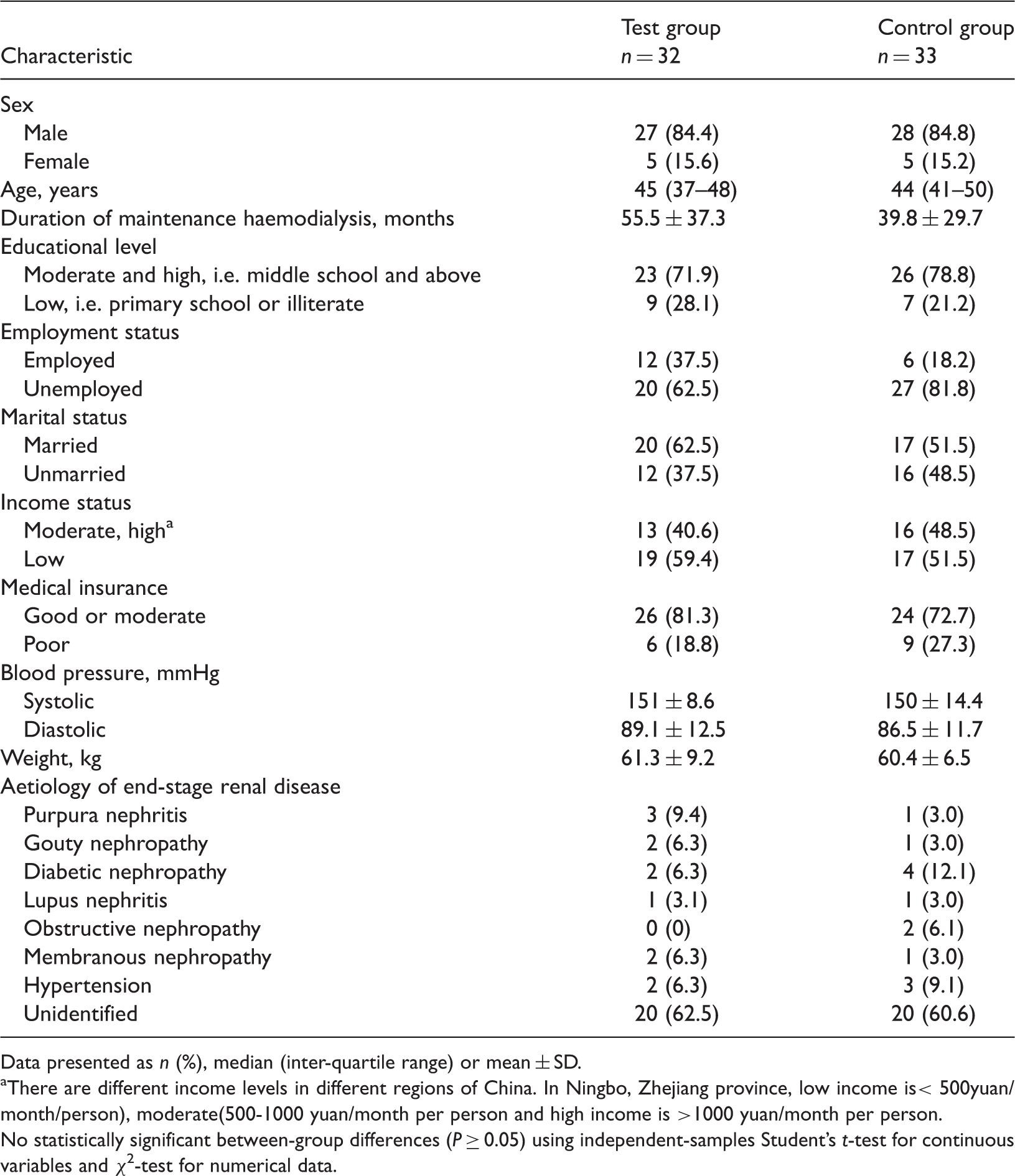
Data presented as n (%), median (inter-quartile range) or mean ± SD.
There are different income levels in different regions of China. In Ningbo, Zhejiang province, low income is< 500yuan/month/person), moderate(500-1000 yuan/month per person and high income is >1000 yuan/month per person.
No statistically significant between-group differences (P ≥ 0.05) using independent-samples Student’s t-test for continuous variables and χ2-test for numerical data.
Exercise capacity
Indicators of exercise capacity in patients performing exercise (test group) and controls, during maintenance haemodialysis.

Data presented as mean ± SD.
P < 0.05 for within-group comparison with baseline, bP < 0.01 and cP < 0.05 compared with control group (independent-samples Student’s t-test).
KDQOL-SF™
Kidney disease health-related quality of life score (KDQOL-SF™) parameters in maintenance haemodialysis patients performing exercise (test group) and controls.

Data presented as mean ± SD.
P < 0.05 for within-group comparison with baseline, bP < 0.01 and cP < 0.05 compared with control group (independent-samples Student’s t-test).
Adverse reactions
Adverse reactions in maintenance haemodialysis patients performing exercise (test group) and controls.
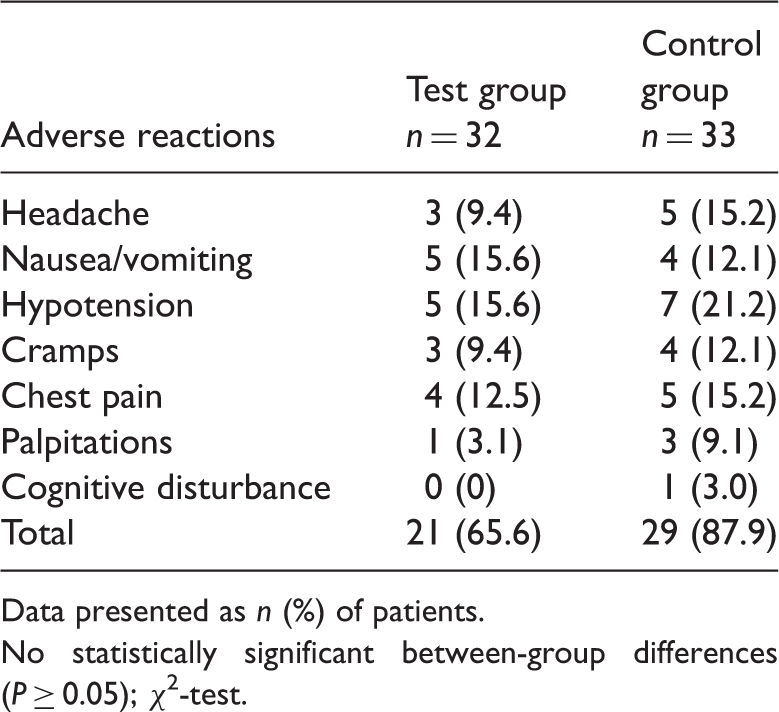
Data presented as n (%) of patients.
No statistically significant between-group differences (P ≥ 0.05); χ2-test.
Discussion
Patients undergoing MHD have been shown to have significantly lower exercise capacity and muscle strength compared with controls,
12
and increased frailty in patients with end-stage renal disease has been reported to be closely associated with higher mortality and a higher hospitalization rate, compared with patients who are stronger.
13
At present, the maximum oxygen uptake (V
The HRQoL in uraemic patients is universally low, and is influenced by factors such as age, sex, financial and work status, educational level and laboratory indicators.19,20 The KDQOL-SF™ is a international instrument with high reliability and validity that has been developed to evaluate HRQoL in patients with kidney disease undergoing dialysis. 21 In the present study, the KDQOL-SF™ was used for a comprehensive evaluation of HRQoL in patients receiving individualized exercise therapy during dialysis and controls. After 12 weeks’ exercise, there was no difference in the KDQOL-SF™ scores for pain, sexual function, work status and burden of kidney disease between the test and control groups. Compared with baseline and the control group scores, there were significant differences in the test group in the KDQOL-SF™ scores for physical function, physical role limitations, general health, energy/fatigue, sleep, quality of social interaction, dialysis staff encouragement and patient satisfaction. In a self-controlled study by Parsons et al., 22 13 patients underwent less-strenuous exercises during dialysis, and there were no observed changes in various dimensions of the SF-36 20 weeks later. A possible explanation for this might be the high baseline scores for HRQoL recorded for these patients. 22 Van Vilsteren et al. 7 reported that exercise was associated with improvements in the scores of three dimensions of the RAND-36 (vitality, general health perception and health change). In addition, Painter et al. 23 reported that exercise was associated with improved scores in five dimensions of the SF-36 (general health, emotional wellbeing, social function, emotional role limitations and energy/fatigue). These differences may be due to the relatively high proportion of males in the present study: these people generally were relatively young and had well-corrected malnutrition. The present results are consistent with studies by Afshar et al. 24 and Storer et al, 25 and suggest that exercise during dialysis could effectively improve HRQoL in patients on MHD by improving their physical performance, reducing the feeling of fatigue and improving the quality of sleep, helping them to look after themselves better in daily life and improving their performance status, thus enabling them to return to a normal social life.
No exercise-related adverse reactions were observed during the study; the only complications occurring were common complications of dialysis such as hypotension, cramps and headache.
In conclusion, individualized exercise during MHD improved the exercise capacity and HRQoL in patients with uraemia within a short time period. No adverse effects or safety issues were observed. Individualized exercise programmes could therefore be used as a simple, cost-effective therapeutic approach in people requiring MHD. However, further larger clinical studies are required to confirm the benefits.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.