
Abstract
Objective
Pretreatment with intravenous 40 mg or 0.5 mg/kg lidocaine with venous occlusion is recommended to prevent pain following injection of lipid emulsion propofol. This approach is not sufficient to prevent pain from the injection of microemulsion propofol. The present study investigated whether a higher dose of lidocaine pretreatment with venous occlusion would be more effective for reducing pain following injection of microemulsion propofol compared with 40 mg lidocaine.
Methods
Patients undergoing elective surgery were randomly assigned to one of three groups: pretreatment with 40 mg (group L40), 60 mg (group L60) or 80 mg (group L80) lidocaine intravenously with venous occlusion, followed by injection with microemulsion propofol 1 min later. Pain was assessed on a four-point scale (severe, moderate, mild, none) based on physical responses to the injection.
Results
A total of 68 patients were included in the final analysis. Pain severity and incidence were significantly lower in patients in group L60 and L80 compared with patients in group L40. There were no statistically significant differences in pain incidence or severity between group L60 and group L80.
Conclusions
Pretreatment with 60 mg lidocaine intravenously with venous occlusion may be the most effective minimum dose for reducing injection pain following microemulsion propofol administration for induction of anaesthesia.
Introduction
Hydrosoluble, lipid-free microemulsion propofol and lipid emulsion propofol have comparable pharmacokinetic and pharmacodynamic profiles.1–6 Microemulsion propofol has several advantages over lipid emulsion propofol in that it demonstrates higher physicochemical stability and antimicrobial activity, 7 which avoids lipid solvent-related complications such as hyperlipidaemia, pulmonary fat embolism, pancreatitis and propofol-infusion syndrome. 8 It is, however, associated with more intense and frequent pain on injection compared with lipid emulsion propofol. 9 Thus interventions that aim to limit the injection pain caused by microemulsion propofol during induction of anaesthesia are important.
The most effective and easy to perform strategy for the prevention of pain on injection of propofol is intravenous lidocaine pretreatment with venous occlusion.10,11 A dose of 40 mg or 0.5 mg/kg lidocaine administered intravenously with venous occlusion into the upper limb is recommended for the alleviation of pain on injection with lipid emulsion propofol,10,12 and this approach has resulted in reports of pain reduction in 60–86% of patients.10,12 In contrast, other studies have failed to demonstrate a similar reduction of pain on injection of microemulsion propofol using 40 mg lidocaine, with only 24–38% of patients experiencing no injection pain. 13
The aim of the present study was to compare the efficacy of pretreatment with 60 mg and 80 mg lidocaine with venous occlusion with a 40 mg dose in reducing pain on injection of microemulsion propofol in patients undergoing elective surgery. It was hypothesized that the higher doses of lidocaine with venous occlusion would be more effective for reducing pain compared with 40 mg lidocaine.
Patients and methods
Study population
Patients with American Association of Anesthesiology physical status I or II who were 20–60 years of age and undergoing elective surgery at Ajou University Hospital, Suwon, Republic of Korea between 15 July and 9 August 2013 were recruited. Patients with a history of neurological problems or allergies and those who had taken medications including sedatives and analgesics within 24 h of surgery, which may affect the study results, were excluded. In addition, patients with a body weight of < 55 kg were excluded as the maximum dose of lidocaine in these patients would be <1.5 mg/kg.
Written informed consent was obtained from all patients and the study protocol was approved by the Ajou University Hospital Institutional Review Board.
Study design
Patients were randomly allocated into three groups using a sealed-envelope method immediately prior to induction of anaesthesia. Groups received: (i) 40 mg lidocaine (group L40); (ii) 60 mg lidocaine (group L60); (iii) 80 mg lidocaine (group L80). A placebo group was not included for ethical reasons. To preserve blinding, normal saline (0.9%) was added to give a total volume of study medication of 4 ml in groups L40 and L60. All study drugs were prepared just before injection at room temperature. Microemulsion propofol (Aquafol®; Daewon Pharmaceutical Co. Ltd, Seoul, Republic of Korea), which contained 1% propofol, 10% purified poloxamer 188 (PP188) as a nonionic block copolymer surfactant, and 0.7% polyethylene glycol (PEG) 660 hydroxystearate as a nonionic surfactant, was prepared in a 50 ml syringe. A commercially available, two-channel, target-controlled infusion (TCI) pump (Orchestra® Base Primea with a two-infusion pump module: Module DPS Orchestra® IS3; Fresenius Vial S.A.S, Brezins, France) was used for effect-site TCI of the microemulsion propofol. The pharmacokinetic model used to calculate target effect-site concentration (Ce) for microemulsion propofol was that of Marsh et al. 14
Before patients were transferred into the operating room, a 20-gauge venous cannula was placed in a vein of the forearm. No premedication was given before the administration of anaesthesia. On arrival in the operating room, patients underwent basic monitoring including electrocardiogram, pulse oximetry and noninvasive blood pressure measurement. After venous occlusion was applied with a rubber tourniquet, the allocated dose of lidocaine was injected. The tourniquet was released after 1 min and microemulsion propofol was administered through the same venous cannula to achieve a target Ce of 5.2 µg/ml at a maximum flow rate of 750 ml/h, which represented a bolus of 120 mg over 60 s for a 66 kg patient (the mean weight of the study patients) approximating to an infusion rate of 2 mg/kg per min.
Study assessments
Pain was assessed by H.S.C., who was blind to the pretreatment lidocaine dose, from the start of the microemulsion propofol injection to the point of loss of consciousness. The severity of pain was graded on a four-point scale: 15 ‘severe pain’ was manifest as a verbal response accompanied by facial grimacing or withdrawal of the arm; ‘moderate pain’ was defined as grimacing or arm withdrawal not accompanied by a verbal response; ‘mild pain’ was recorded if after 30 s the patient had not experienced moderate or severe pain but reported discomfort in the arms when questioned; ‘no pain’ was recorded if the patient did not report arm discomfort when questioned.
After loss of consciousness, anaesthetic management was left to the discretion of the attending anaesthesiologist. All patients were evaluated in the postanaesthesia care unit following surgery for abnormal injection-site responses including erythema, phlebitis, oedema and pain.
Statistical analyses
Based on preliminary unpublished data regarding the incidence of injection-site pain obtained at Ajou University Hospital, a total sample of 65 patients was determined to be sufficient to achieve 90% power to detect differences with a type I error of 0.05 (two-tailed) and a type II error of 0.10. Based on this assumption, a minimum of 22 patients per treatment group was required. Assuming some patients would drop-out of the study, the sample size was increased to 23 patients per group.
Statistical analyses were performed using SPSS® statistical software, version 11.0 (SPSS, Inc., Chicago, IL, USA) for Windows®. Data are expressed as mean ± SD or number (%) of patients. Patient characteristics were compared using one-way analysis of variance or χ2-test, as appropriate. Differences in pain grades between groups were analysed using Kruskal–Wallis test or χ2-test. Post hoc comparisons were performed using Mann–Whitney U-test with Bonferroni’s correction. Results were considered statistically significant when the P-value was < 0.05.
Results
In total, 69 patients undergoing elective surgery were included in the study. One patient in group L40 was excluded from the analyses because of concealed leakage between the line for fluid and the intravenous catheter (Figure 1). Demographic data for all patients included in the analyses are presented in Table 1; there were no significant differences between the three groups.
Flow diagram of patients enrolled into a randomized, double-blind study to evaluate the efficacy of three doses (40, 60 and 80 mg) of intravenous lidocaine pretreatment with venous occlusion for reducing pain induced by microemulsion propofol. Demographic data for patients undergoing elective surgery who received pretreatment with 40 mg (group L40), 60 mg (group L60) or 80 mg (group L80) lidocaine intravenously with venous occlusion followed by injection with microemulsion propofol for anaesthesia induction. Data presented as mean ± SD or n (%) of patients. No statistically significant differences were observed between treatment groups (one-way analysis of variance or χ2-test). ASA, American Society of Anesthesiologists.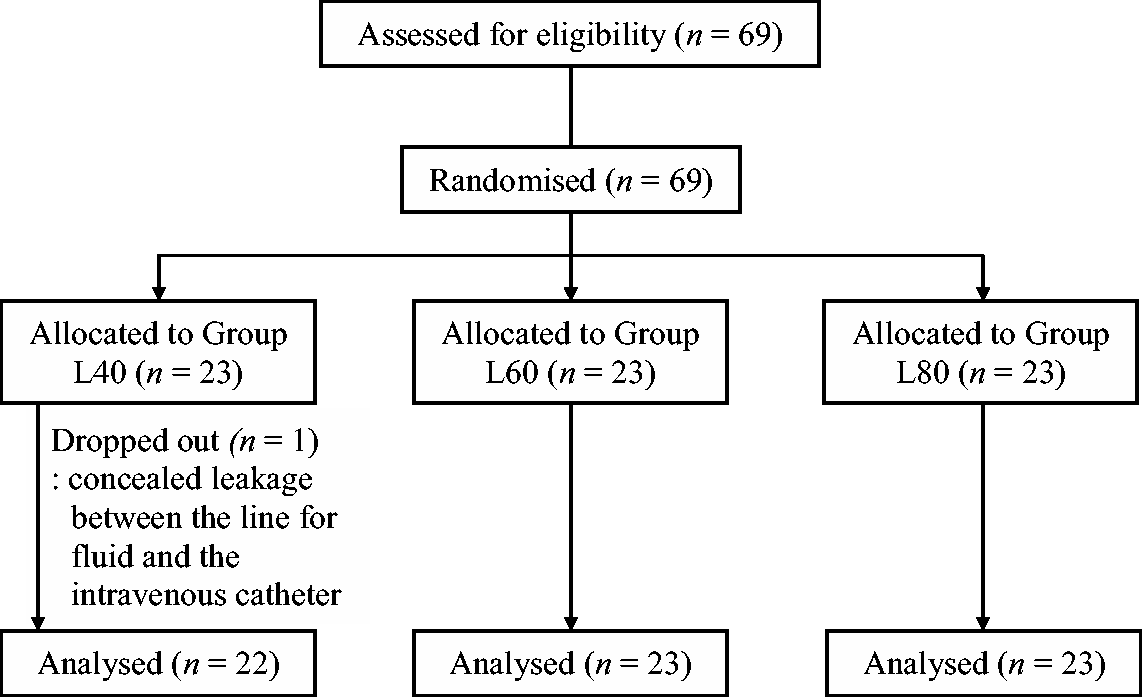

Incidence and severity of injection pain in patients undergoing elective surgery who received pretreatment with 40 mg (group L40), 60 mg (group L60) or 80 mg (group L80) lidocaine intravenously with venous occlusion followed by injection with microemulsion propofol for anaesthesia induction.
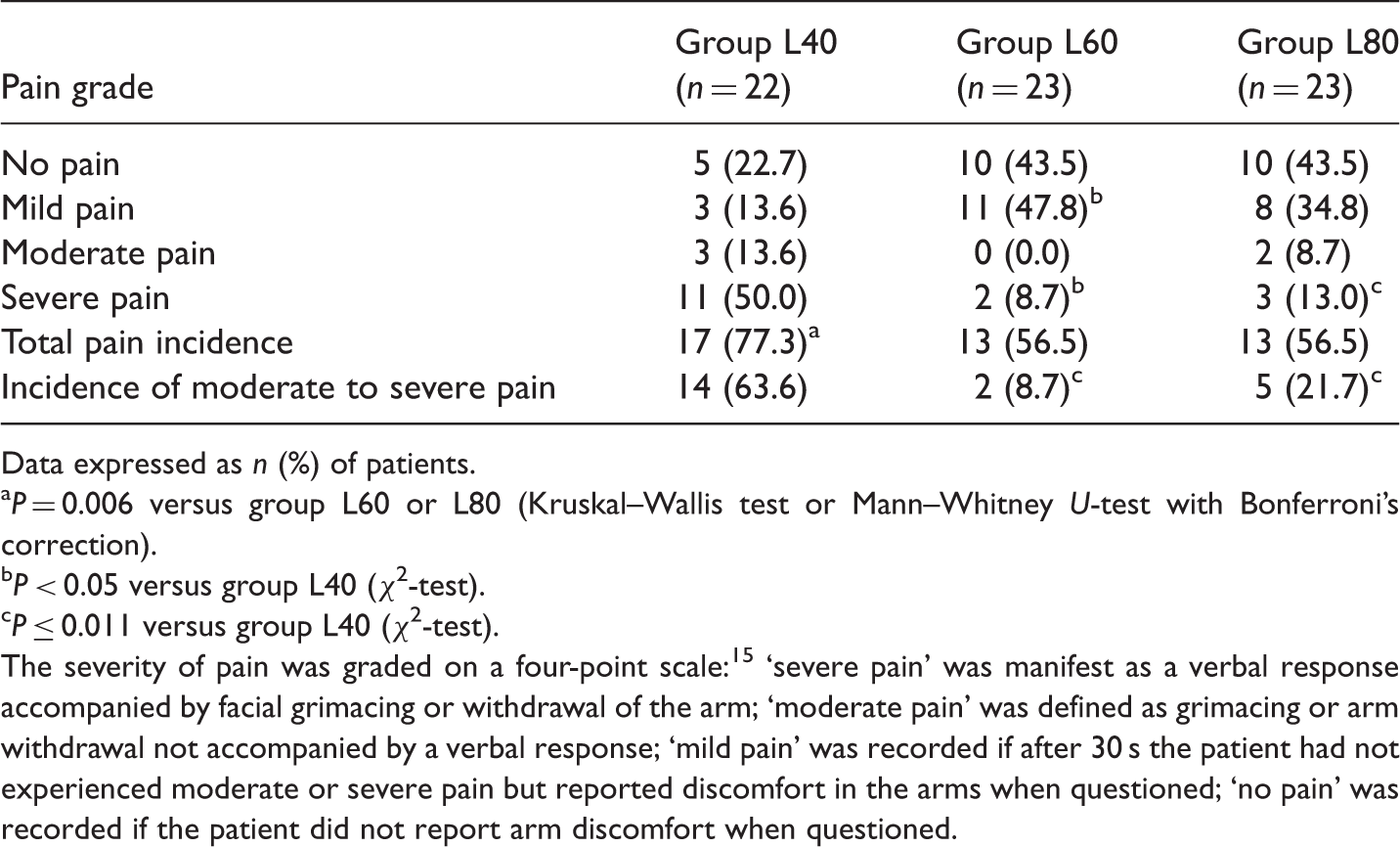
Data expressed as n (%) of patients.
P = 0.006 versus group L60 or L80 (Kruskal–Wallis test or Mann–Whitney U-test with Bonferroni’s correction).
P < 0.05 versus group L40 (χ2-test).
P ≤ 0.011 versus group L40 (χ2-test).
The severity of pain was graded on a four-point scale: 15 ‘severe pain’ was manifest as a verbal response accompanied by facial grimacing or withdrawal of the arm; ‘moderate pain’ was defined as grimacing or arm withdrawal not accompanied by a verbal response; ‘mild pain’ was recorded if after 30 s the patient had not experienced moderate or severe pain but reported discomfort in the arms when questioned; ‘no pain’ was recorded if the patient did not report arm discomfort when questioned.
Discussion
The present study demonstrated that pretreatment with 60 mg or 80 mg lidocaine with venous occlusion significantly reduced the incidence and severity of pain following injection of microemulsion propofol compared with 40 mg lidocaine. No significant difference was observed in intensity or incidence of pain between patients in group L60 and patients in group L80. This finding implies that 60 mg lidocaine may be the optimal dose for reducing pain following injection of microemulsion propofol.
Microemulsion propofol was developed as an alternative to lipid emulsion propofol, which is associated with problems such as pulmonary embolism,16,17 bacterial infection,18,19 hypertriglyceridaemia and pancreatitis.8,20 The first microemulsion propofol formulation was composed of 1% propofol, 8% PEG 660 hydroxystearate (Solutol® HS 15; BASF, Seoul, Korea) and 5% tetrahydrofurfuryl alcohol polyethylene glycol ether (Glycofurol; Roche, Basel, Switzerland), and demonstrated effects bioequivalent to lipid emulsion propofol. 2 As a consequence of toxicities such as drug eruption, urticaria, fever and dizziness, increased total bilirubin and lactate dehydrogenase, and chest discomfort, microemulsion propofol has been reformulated and now comprises 1% propofol, 10% purified PP188 and 0.7% PEG 660 hydroxystearate. 3 This formulation was as effective as lipid emulsion propofol and showed similar pharmacokinetics. 4 The free propofol concentration in the aqueous phase of the reformulated microemulsion propofol is, however, five times greater than that of the original formulation, 21 meaning it has an increased potential to produce frequent and severe pain on injection.22,23 Pain on injection is one of the major drawbacks of microemulsion propofol 9 and it is important that methods to decrease injection pain in the clinical setting are available. Published research has demonstrated that 81.9% of patients experienced moderate to severe injection pain after microemulsion propofol administration, with an average visual analogue scale score (VAS; 0 mm, no pain, 100 mm, worst pain imaginable) of 72 mm. 4 In another study, the incidence of injection pain (defined as VAS > 30 mm) following microemulsion propofol administration was reported to be 69.7% with a median VAS score of 59 mm. 9
Among the various methods proposed to decrease injection pain, lidocaine pretreatment with venous occlusion is one of the most effective.10,11 Pretreatment with 40 mg or 0.5 mg/kg lidocaine with venous occlusion of the upper limb is recommended for alleviating injection pain associated with lipid emulsion propofol administration.10,12 Using this strategy, the overall incidence of pain on lipid emulsion propofol injection has been reported to range from 8% to 42%, while the incidence of moderate to severe pain ranges from 2% to 16%.12,24–28 In the present study, the overall incidence of injection pain following microemulsion propofol administration in patients in group L40 was 77.3% and the incidence of moderate to severe injection pain was 63.6%, which is comparable to previous data. 13 These findings suggest that pretreatment with 40 mg lidocaine in the clinical setting is insufficient to prevent injection pain following microemulsion propofol. The present study also evaluated 60 mg and 80 mg lidocaine pretreatment. These doses were selected after consideration of the established range of lidocaine doses used in the treatment or prophylaxis of ventricular arrhythmias 29 and by excluding patients weighing <55 kg such that the maximum dose of lidocaine used in the present study was <1.5 mg/kg.
Potential mechanisms of injection pain following propofol have been proposed, including triggering of the local kallikrein–kinin cascade, 30 stimulation by direct contact between aqueous phase propofol and free nerve endings in the inner venous wall, 30 or the pH and concentration of propofol.22,31 The exact mechanism by which lidocaine reduces propofol-induced pain remains unclear. It is possible that lidocaine pretreatment in the present study may have induced bradykinin generation associated with activation of the plasma kallikrein–kinin system. Previous studies have, however, reported no evidence that the generation of bradykinin through activation of the plasma kallikrein–kinin system was associated with propofol-induced pain. 9 Venous occlusion, as employed in the present study, may have blocked the nerve fibres that are responsible for transmission of pain resulting from direct irritation of the inner blood vessel walls by propofol. This direct anaesthetic effect of lidocaine is achieved when the dose is adequate and sufficient time for the drug to work is allowed: in previously published studies, higher doses of lidocaine have generally been more effective than lower doses, 32 although it has been reported in a systematic review of the literature that there is no obvious dose–response relationship within the dose range of 20–100 mg lidocaine. 10 The results of the present study demonstrate that a lidocaine dose of at least 60 mg with venous occlusion is required to reduce injection pain following microemulsion propofol. Microemulsion propofol was still found to cause moderate to severe pain, even after pretreatment with 60 mg or 80 mg lidocaine. This is probably because microemulsion propofol and lidocaine do not exert their effects on the same pain pathway, because there was an insufficient time interval between lidocaine administration and release of the tourniquet, or insufficient pressure was generated by venous occlusion.
In conclusion, the present study demonstrated that prior administration of 60 mg or 80 mg of lidocaine with venous occlusion was more effective for reducing pain following injection of microemulsion propofol than 40 mg lidocaine. No further reductions in the incidence or severity of pain were observed with 80 mg lidocaine compared with the 60 mg dose.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.