
Abstract
Objectives
To investigate expression of pentraxin 3, long (PTX3) in patients with acute coronary syndrome (ACS) and its correlation with matrix metalloproteinase-9 (MMP-9) and C-reactive protein (CRP) levels.
Methods
Patients with ACS were randomly assigned to the ACS group (subdivided into unstable angina pectoris [UAP] and acute myocardial infarction [AMI]). Healthy participants and patients with stable angina pectoris (SAP) were enrolled as controls. Mononuclear cell PTX3 expression, and serum MMP-9 and CRP levels, were measured by enzyme-linked immunosorbent assay.
Results
The ACS group comprised 200 patients (80 in the UAP subgroup; 120 in the AMI subgroup). The control group comprised 130 participants (80 healthy volunteers and 50 patients with SAP). PTX3 expression was significantly higher in the ACS group compared with controls (3.64 ± 0.49 versus 1.85 ± 0.65 ng/ml), and significantly higher in the AMI compared with the UAP subgroup (5.44 ± 0.47 versus 3.39 ± 0.59 ng/ml). Serum MMP-9 and CRP levels were significantly higher in the ACS group compared with controls (48.55 ± 14.22 versus 23.14 ± 0.62 ng/ml; 4.88 ± 1.76 versus 1.26 ± 0.19 ng/ml, respectively), and significantly higher in the AMI compared with the UAP subgroup (58.13 ± 7.24 versus 31.77 ± 3.61 ng/ml; 5.80 ± 1.46 versus 3.27 ± 0.83 ng/ml, respectively). PTX3 expression, and MMP-9 and CRP levels in the SAP subgroup, were not significantly different from the healthy participants. PTX3 expression positively correlated with MMP-9 and CRP levels.
Conclusions
In patients with ACS, peripheral blood mononuclear cell PTX3 expression, and serum MMP-9 and CRP levels, were significantly enhanced compared with controls; in addition, PTX3 expression positively correlated with MMP-9 and CRP levels. PTX3 may be involved in ACS pathogenesis.
Keywords
Introduction
Despite great progress in pharmacotherapy and interventional treatment, acute coronary syndrome (ACS) remains a major factor associated with morbidity and mortality in the modern world. 1 Endothelial erosion and plaque rupture with a superimposed thrombus is thought to be the underlying pathophysiological process leading to ACS, which is driven by inflammatory processes initiated by other cardiovascular risk factors. 2 Research 3 has demonstrated that C-reactive protein (CRP) is a proinflammatory factor that is relevant to the pathogenesis of coronary heart disease and plays a crucial role with prognostic value in patients with ACS.
Pentraxin-related protein PTX3 is a long pentraxin with a molecular weight of 45–50 kDa, encoded by the pentraxin 3, long (PTX3) gene: 4 it is abundantly expressed in atherosclerotic plaques and cardiac myocytes. 5 The present study was designed to investigate expression levels of PTX3 in peripheral blood mononuclear cells (PBMC), and the relationship between PTX3 expression and the inflammatory markers, matrix metalloproteinase (MMP)-9 and CRP, that increase during systemic inflammation in patients with ACS.
Patients and methods
Study population
This observational case–control study included consecutive patients who were screened and admitted to the Department of Cardiology at the People’s Hospital of Sanya, Hainan, China, between March 2009 and April 2012 due to an initial diagnosis of ACS, patients with stable angina pectoris and healthy volunteers. Patients with ACS were assigned to the ACS group, which was further subdivided into an unstable angina pectoris (UAP) subgroup and acute myocardial infarction (AMI) subgroup. ACS was diagnosed by the presence of one of the following criteria: AMI, defined as either non-ST segment elevation (on electrocardiogram [ECG])-myocardial infarction when patients presented with typical chest pain and markers of myocardial necrosis (troponin I or creatine kinase release), or ST-elevation myocardial infarction when patients presented with ST elevations on ECG at the J-point in at least two contiguous leads (≥1.5 mm in female and ≥2 mm in male patients); UAP was defined as patients with clinical symptoms and new ECG changes, but no markers of myocardial necrosis. Exclusion criteria for the patient group comprised: chronic heart failure (New York Heart Association class IV); vasospastic angina; chronic renal failure (creatinine concentration >176.8 mmol/l); metabolic or inflammatory disease; anaemia; thyrotoxicosis; therapy with steroids, immunosuppressive agents; nonsteroidal antiinflammatory drugs (excluding low-dose aspirin).
During the study period, healthy volunteers were recruited from the local population in Haikou, China, and patients with stable angina pectoris (SAP) also treated at the Department of Cardiology at the People’s Hospital of Sanya were enrolled to serve as the control group. Healthy volunteers were excluded if coronary angiography showed significant luminal narrowing. SAP was defined as patients with medically controlled stable angina who required elective percutaneous coronary intervention or coronary artery bypass graft surgery, long-term (>6 months’) stable effort angina and a positive exercise test.
The study protocol was approved by the Ethics Committee of the People's Hospital of Sanya, Hainan, China, and written informed consent was obtained from all participants.
Isolation of mononuclear cells from whole blood
Peripheral venous blood (10 ml) samples were collected into heparinized tubes from patients admitted with ACS ≥6 h after onset of chest pain, or on admission or at time of clinic visit for patients with SAP and healthy volunteers. The blood was diluted with sterile 0.01 M phosphate-buffered saline (PBS, pH 7.4) in a 1 : 1 ratio at room temperature. The suspension (20 ml) was then carefully layered onto 7 ml Ficoll-Biocoll separating solution (TBD, Tianjin, China) in a tube, according to the manufacturer’s instructions, and density gradient centrifugation was performed at 200
Blood sampling and laboratory analyses
Venous blood samples (10 ml) were drawn from all study participants into sterile tubes at the same timepoint described for isolation of PBMC. The collected blood samples were allowed to stand for ≤2 h at room temperature then centrifuged at 300
Blood lipid levels were determined in all samples using an immune turbidimetric method. 7 Triglyceride (TG), serum total cholesterol (TC) and high density lipoprotein-cholesterol (HDL-C) levels were measured in each of the serum samples. Low density lipoprotein-cholesterol (LDL-C) levels were calculated using the Friedwald’s formula. 8
Statistical analyses
Data were presented as mean ± SD. Between-group differences were analysed using Student’s t-test. Spearman’s rank correlation coefficient was used to analyse the correlation between PTX3, CRP, and MMP-9, since data were not normally distributed. Statistical analyses were performed with the SPSS® statistical software package, version 13.0 (SPSS, Inc., Chicago, IL) for Windows®. A P-value <0.05 was considered statistically significant.
Results
Baseline clinical and laboratory characteristics in 200 patients with acute coronary syndrome (ACS), subdivided into patients with acute myocardial infarction (AMI) and unstable angina pectoris (UAP) and 130 controls, subdivided into patients with stable angina pectoris (SAP) and healthy volunteers.
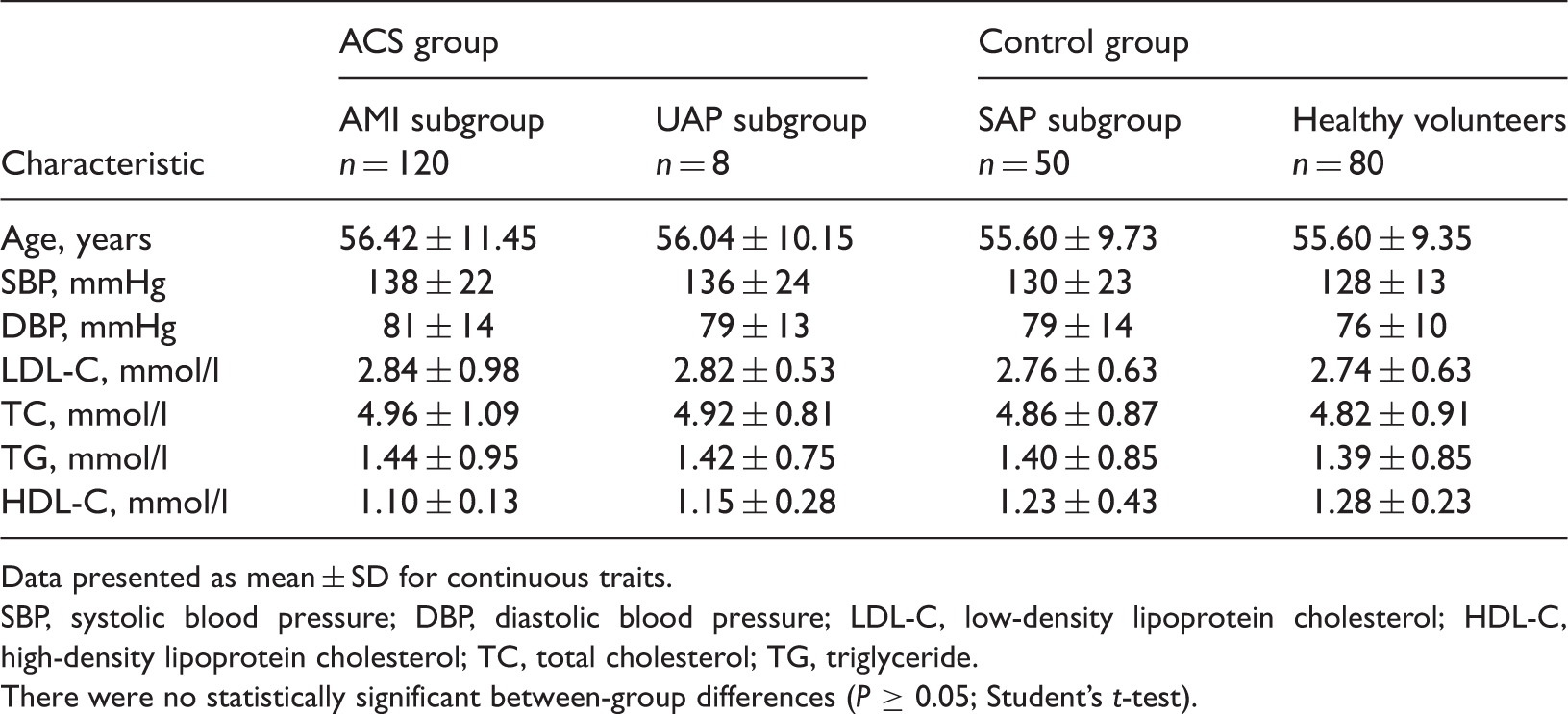
Data presented as mean ± SD for continuous traits.
SBP, systolic blood pressure; DBP, diastolic blood pressure; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TC, total cholesterol; TG, triglyceride.
There were no statistically significant between-group differences (P ≥ 0.05; Student’s t-test).
Comparison of serum matrix metalloproteinase (MMP)-9 and C-reactive protein (CRP) levels, and mononuclear cell PTX-3 levels, between different subgroups of 200 patients with acute coronary syndrome (ACS), subdivided into patients with acute myocardial infarction (AMI) and unstable angina pectoris (UAP), and 130 controls subdivided into patients with stable angina pectoris (SAP) and healthy volunteers.

Data presented as mean ± SD.
Statistically significant difference compared with UAP subgroup (P < 0.01; Student’s t-test).
Statistically significant difference compared with healthy volunteers (P < 0.05; Student’s t-test).
The PBMC PTX-3 levels positively correlated with serum CRP and MMP-9 levels (r = 0.836, P < 0.01; r = 0.894, P < 0.01, respectively).
Discussion
Inflammation has been shown to play an important role in atherogenesis. 9 Inflammation that occurs in the coronary plaques is the main cause of inflammation that leads to ACS, through rupture and erosion of the tissues. 10 Monocytes are known to be important in the key stages of ACS, 11 during which their synthesis of the proinflammatory molecules, such as interleukin-6, tumour necrosis factor-α and CRP, is promoted. Pentraxin-related protein PTX-3 is one of the long pentraxins and, like CRP, is produced and released in the liver as an acute-phase response to proinflammatory cytokines, and also from within the unstable atherosclerotic plaque.12,13 During the process of atherogenesis, PTX3 is found to be expressed in human vascular smooth muscle cells via atherogenic lipoproteins, 14 and is thought to upregulate tissue factor expression in human endothelial cells 15 and activated monocytes, 16 and to occur extensively in advanced atherosclerotic plaques. The present study showed that PBMC PTX-3 levels were significantly increased in patients with ACS compared with the controls. Within-group analysis of the controls showed that expression of PTX3 in the SAP subgroup was not significantly different from that in healthy volunteers. These results indicate that PBMC expression of PTX-3 may contribute to the pathophysiology of ACS.
Epidemiological studies have shown that CRP, one of the short pentraxins, has a key role and worldwide use as a diagnostic biomarker in ischaemic heart diseases, and that increased serum CRP levels in ACS are considered to be a nonspecific response to myocardial injury.17–19 Similar to previous research, the present study showed serum CRP levels to be increased in patients with ACS, and to increase as the seriousness of cardiovascular disease increased from stable angina pectoris to acute myocardial infarction. PBMC expression of PTX3 positively correlated with serum CRP levels in the present study, supporting the hypothesis that pentraxin-related protein PTX3 may play a direct role in promoting the inflammatory component of atherosclerosis in the development of ACS.
Matrix metallopeptidase 9 is expressed in atherosclerotic plaques and is thought to induce degradation of extracellular matrix proteins, leading to rupture of the fibrous cap of the atherosclerotic plaque which predisposes an individual to coronary thrombus formation, ultimately leading to ACS.20–23 MMP9 can also be induced in response to cytokines implicated in a variety of inflammatory processes that play a key role in stability and plaque rupture.4,24,25 These cytokines display a degradative action on several components of the extracellular matrix, thus actively participating in weakening of the fibrous cap and plaque instability.15,26 In the present study, levels of MMP-9 were significantly higher in patients with ACS than control subjects. Therefore, MMP-9 may serve as a marker of plaque instability in ACS.
During atherosclerosis, macrophages and T cells infiltrate the blood vessel wall, triggered by endothelial dysfunction. The findings of the present study showed that PBMC expression of PTX3 positively correlated with serum levels of MMP-9, suggesting that pentraxin-related protein PTX3 may be involved in the pathogenesis of ACS, and may be related to atherosclerotic plaque instability.
In conclusion, PTX3 was expressed in PBMC in patients with ACS and non-ACS controls. Expression of PTX3 was found to be higher in the ACS group compared with controls and positively correlated with serum MMP-9 and CRP levels, which were also increased in patients with ACS compared with controls. These results suggest that PTX3 expression may be involved in the pathogenesis of ACS.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This work was financially supported by Science and Technology Cooperation Projects of Sanya (2011YD100).