
Abstract
Objective
To determine the accuracy of the Faecal Occult Blood–Transferrin test (FOB–T; Certest Biotec, San Mateo de Gállego, Spain) for detection of blood in nasogastric aspirate, and its emergency diagnostic value for upper gastrointestinal bleeding (UGIB).
Methods
Nasogastric aspirate was collected from patients with haematemesis on admission to hospital. Haemoglobin was quantified on admission and after 12 h. FOB–T test was used to assess each nasogastric aspirate sample for the presence of haemoglobin and transferrin.
Results
Of 64 patients included in the study, 28 (43.8%) were hospitalized for UGIB based on physical examination, haemoglobin level. 24 were confirmed with endoscopy findings. Four were excluded from study due to lack of endoscopic confirmation. The remaining 36 patients had no clinical evidence of UGIB. FOB–T test findings were positive in 26/60 patients, including all 24 patients with UGIB. The FOB–T test had sensitivity 100%, specificity 94.4%, positive predictive value 92.3% and negative predictive value 100% for UGIB.
Conclusions
A negative FOB–T test may be sufficient to exclude the possibility of UGIB without other diagnostic tests.
Keywords
Introduction
Upper gastrointestinal bleeding (UGIB) is a life-threatening condition with an annual incidence ranging between 48 and 149 cases per 100 000 adults, resulting in high costs to public health systems.1–3 Acute UGIB is the most common gastroenterological emergency, 2 but diagnosis in the emergency department can be time consuming, and many patients admitted with haematemesis do not have UGIB. Prompt, accurate diagnosis is important, 4 because delays can result in unnecessary or incomplete treatment. 1 Standard diagnostic tools for UGIB include nasogastric tube aspiration, digital rectal examination, faecal occult blood test, repeated haemoglobin counts and endoscopic evaluation. 4
The Gastroocult® (Beckman Coulter, Pasadena, CA, USA) test is a rapid diagnostic tool with high sensitivity for detecting blood in gastric aspirates; its use reduces the incidence of undiagnosed UGIB. The high false-positive rate of this test (∼5%) leads to unnecessary treatment and limits its use in clinical decision-making, however.5,6 The Faecal Occult Blood–Transferrin test (FOB–T; Certest Biotec, San Mateo de Gállego, Spain) is a one-step, chromatographic immunoassay for the qualitative determination of haemoglobin and transferrin in stool samples. The present study evaluated the accuracy of the FOB–T test for the detection of blood in nasogastric aspirates, and the negative predictive value of the test for excluding UGIB.
Patients and methods
Study population
The study recruited consecutive adult patients (aged >18 years) with haematemesis admitted to the Department of Emergency Medicine, Haydarpasa Numune Training and Research Hospital, Istanbul, Turkey, between June 2012 and December 2012. Patients with liver disease, those using anticoagulants or antiplatelet drugs, and pregnant or breastfeeding women were excluded. Standard diagnostic tools for UGIB were undertaken, including nasogastric tube aspiration, digital rectal examination, faecal occult blood test, haemoglobin count (on admission and after 12 h) and endoscopic evaluation. Patients with clear clinical evidence of haematesis and melena in physical examination were diagnosed with UGIB. Patient medical records were reviewed for endoscopy results.
This study was conducted with the approval of the Ethical Committee of the Haydarpasa Numune Training and Research Hospital, and all patients provided written informed consent.
FOB–T test
Nasogastric aspirates were collected via a 16-Fr PVC Levin catheter, on hospital admission. All samples were tested immediately by a technician who was blinded to the patients’ condition. The FOB–T test was performed according to the manufacturer’s protocol. The test has sensitivity of 10 ng/ml and 4 ng/ml for human haemoglobin and transferrin, respectively.
Statistical analyses
Data were presented as mean ± SD or n (%). Nonparametric data were compared using Mann Whitney-U test. Categorical data were compared using χ2-test. The specificity, sensitivity, positive predictive value and negative predictive value of FOB–T test were determined. Data were analysed using NCSS and PASS software (NCSS LLC, Kaysville, UT, USA). P-values < 0.05 were considered statistically significant.
Results
The study included 64 patients with hematemesis (37 male/27 female; mean age 55.19 ± 20.7 years; age range 22–90 years
Some patients had multiple endoscopic findings and the aetiology of UGIB was antral ulceration (n = 3 [12.5%]), duodenal ulceration (n = 2 [8.3%]), antral gastritis (n = 14 [58.3%]), bulbus ulceration (n = 6 [25%]).
Haemoglobin levels and haematocrit in patients with haematemesis, stratified by nasogastric aspirate Faecal Occult Blood–Transferrin (FOB–T; Certest Biotec, San Mateo de Gállego, Spain) test results.
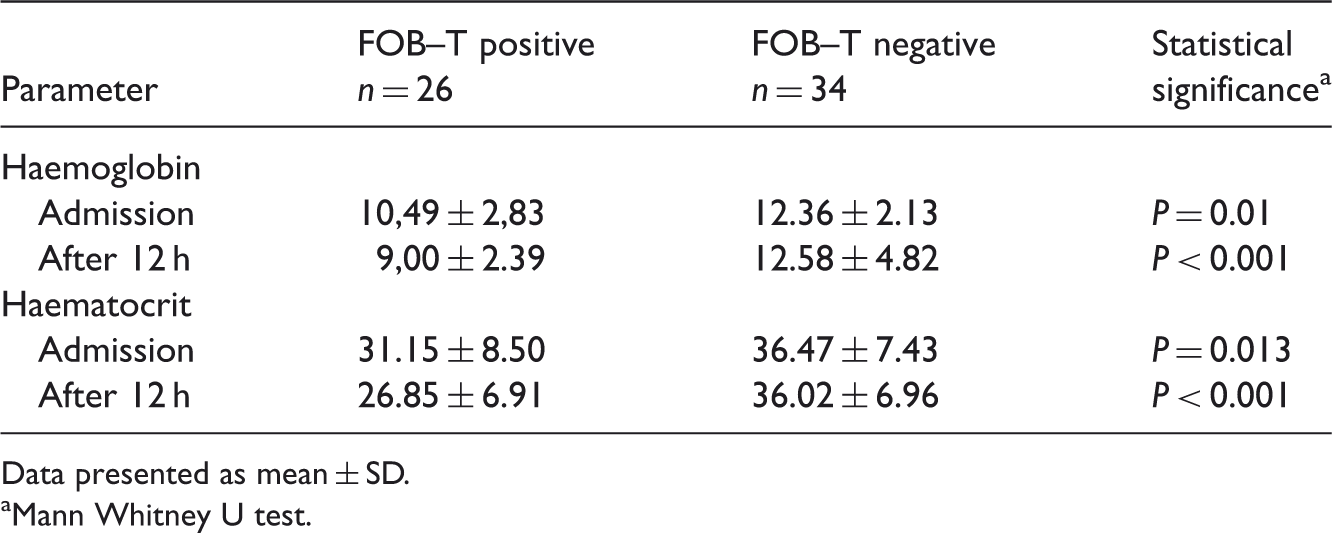
Data presented as mean ± SD.
Mann Whitney U test.
All 24 patients with clinically diagnosed UGIB also had positive FOB–T test findings (sensitivity 100%). Two of 60 patients (3.3%) without clinical evidence of UGIB had positive FOB–T results; both of these patients experienced difficulties during insertion of the nasogastric tube. The remaining patients without UGIB had negative FOB–T findings (34/60). The FOB–T test had specificity 94.4%, positive predictive value 92.3% and negative predictive value 100%. There were no significant differences between traditional diagnostic methods and FOB–T in the rate of UGIB diagnosis (24/60 versus 26/60 patients).
Discussion
Diagnosis of upper gastrointestinal haemorrhage in the emergency room is difficult in the absence of overt gastrointestinal bleeding, 7 but prompt, accurate diagnosis is vital in order to avoid unnecessary or incomplete treatment. 1 Each day, a tertiary hospital emergency room typically admits several patients with haematemesis or melena3,8 many of whom do not have UGIB.
Using traditional diagnostic methods, only 40% of the patients in the current study were found to have UGIB. Diagnosis is dependent on the physician’s assessment, including close observation and an emergency gastroenterology consultation, both of which increase costs. There is a need for an inexpensive, reliable, simple diagnostic test that can accurately exclude UGIB.
The Blatchford 9 and Rockall 10 risk-scoring systems focus on rebleeding and mortality prediction. Both the Blatchford and pre-endoscopy Rockall scores evaluate clinical and laboratory data, and the complete Rockall score uses endoscopic data to predict rebleeding or mortality.4,9,10 Although these scoring systems play an important role in the management of UGIB they are not designed as diagnostic tools. Faecal occult blood tests for the diagnosis of UGIB are limited by low specificity and sensitivity for detecting haemoglobin and transferrin. Such tests are also affected by proteolytic haemoglobin degradation, enterobacteria-related loss of haemoglobin antigenicity, faecal hydration and various drugs. 11
The Gastroocult® test has been shown to be sensitive for the detection of haemoglobin in nasogastric aspirate, but may lead to unnecessary evaluation and treatment of patients who have false-positive results.8,12–14 The FOB–T test used in the present study was capable of excluding the possibility of UGIB, with a negative predictive value of 100%. Additionally, patients with positive FOB–T findings had significantly lower initial haemoglobin levels and a significant decrease in follow-up haemoglobin levels than those who had negative findings. FOB–T testing of nasogastric aspirate may be the procedure of choice for the initial evaluation of suspected UGIB. The two false-positive results observed in the present study suggest that the FOB–T test have similar limitations to Gastroocult®. Complicated nasogastric tube insertions may lead to nasopharyngeal occult bleeding, and result in false-positive results in these patients. The physician should therefore further evaluate any patients with positive test results. The sensitivity, specificity, and positive and negative predictive values of FOB–T in the present study are similar to those reported for Gastroocult® (95%, 82%, 77% and 96%, respectively). 15 The current study was not designed to compare the FOB–T and Gastroocult® tests, and further studies are required to determine which of these tests is more accurate and clinically useful. Other faecal occult blood tests may have similar negative predictive value to the FOB–T test and should be evaluated in a similar manner before use.
The current study had several limitations, including the small number of patients. In addition, these findings should be confirmed in patients with variceal bleeding, and in those treated with anticoagulants or antiplatelet drugs.
In conclusion, findings of the present study suggest that a negative FOB–T test may be sufficient to exclude the possibility of UGIB without other diagnostic tests.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.