
Abstract
Objective
This institutional anaesthetic practice evaluation compared patient safety with respect to residual neuromuscular blockade (NMB) at the time of tracheal extubation in patients undergoing high-risk eye surgery.
Methods
Two muscle relaxation regimens were compared: rocuronium administered via intravenous (i.v.) bolus dosing combined with reversal through sugammadex at end of surgery (group R/S; 17 patients); mivacurium administered via continuous i.v. infusion without antagonization (group M; 22 patients). Train-of-four (TOF) monitoring determined the depth of NMB.
Results
The TOF ratio at the time of tracheal extubation was greater in group R/S (median 1.03) than in group M (median 0.62). Time from end of surgery to tracheal extubation was not significantly different. The surgeons were 100% satisfied with the working conditions provided under both relaxation regimens.
Conclusions
Residual postoperative curarization at the time of extubation was frequently observed in group M, whereas there was complete recovery in group R/S. Reversal of NMB by sugammadex provides an additional safety dimension to patient care and should thus be considered especially for those at risk of airway complications or aspiration, in addition to frail patients.
Introduction
High-risk eye surgery includes keratoplasties and pars plana vitrectomies (PPV). Keratoplasty, which is also known as corneal graft transplantation, entails the allografting of a full- or partial-thickness graft. This procedure is primarily performed to improve or restore visual acuity. 1 A PPV involves the removal of the vitreous humour in order to attend to a number of different retinal pathologies, e.g. retinal detachment or neovascular proliferation. 2 Aided by specially designed ophthalmological microscopes, a very delicate and precise procedure can achieve successful treatment of an otherwise potentially progressive loss of sight.2,3 In 2011, there were 5193 keratoplasties and 64 450 PPVs performed in German hospitals. 4
There are several indispensible anaesthesia-related requirements when aiming for maximum surgical success and patient safety with these interventions. In particular, avoiding involuntary movements, coughing and positional changes of the bulbus during surgery are prerequisites for a good outcome. 5 Either regional or general anaesthesia can be used. 6 In general anaesthesia, either a laryngeal mask or a tracheal tube may be used. 5 Tracheal intubation is preferred in patients at heightened risk of surgery-related sequelae or in those with high American Society of Anesthesiologists (ASA) physical status scores, such as patients with severe heart disease or respiratory disease. 7 In our department, if tracheal intubation is performed for keratoplasty and PPV, the current standard includes the continuous application of the nondepolarizing muscle relaxant mivacurium (throughout the operation) to establish an adductor pollicis train-of-four (TOF) count between 0 and 1. 8 Due to its short-term action, mivacurium provides flexible control over the neuromuscular block (NMB) combined with short spontaneous recovery and is therefore particularly suitable for continuous i.v. application, although prolonged action may be observed in patients suffering from pseudocholinesterase deficiency. 9 Another way to guarantee a motionless bulbus and/or patient is the acceleromyography-guided application of rocuronium, along with the reversal of curarization shortly before tracheal extubation, by means of sugammadex.10–12 Sugammadex is a modified γ-cyclodextrin and exerts its effect by forming tight complexes at a 1 : 1 ratio with steroidal neuromuscular blocking drugs (preferably rocuronium, and to a lesser extent vecuronium and pancuronium), thereby reversing the NMB within ∼2 min of its application. What has prevented most clinicians from using sugammadex more generously or for a wider range of indications, such as the one presented in this article, is primarily its high price.13,14
After uneventful movements were reported in two patients undergoing eye surgery, 15 we set up an institutional anaesthetic practice evaluation in order to compare these two strategies for muscle relaxation in daily routine high-risk eye surgery. A practice evaluation, rather than a randomized controlled trial, was chosen, since a strict study protocol (which would be required for a trial) would not allow the detection of differences in everyday practice. The primary outcome measure of our evaluation was the TOF ratio at tracheal extubation.
Patients and methods
Patients
Patients scheduled for either keratoplasty or PPV at the Department of Ophthalmology, Charité – Universitätsmedizin Berlin, Berlin, Germany, between February 2011 and April 2011, were enrolled sequentially into this study to evaluate the two muscle relaxation regimens in the setting of an observational cohort study. The only exclusion criteria were known allergies to any of the drugs applied and any form of neuromuscular deficiency.
Information to anaesthesiologists
One day prior to surgery, operating timetables were screened for applicable surgeries. The anaesthesiologist in charge was informed shortly before an applicable patient arrived in the operating theatre. He or she was given an information sheet and a verbal explanation saying that the two regimens of muscle relaxation would be evaluated, but without detail. According to our standard anaesthesia protocol, total intravenous (i.v.) anaesthesia with propofol and remifentanil was used for both regimens (see next section). For curarization, the anaesthetist had two options: to use mivacurium for tracheal intubation followed by a continuous i.v. mivacurium infusion during surgery (group M); to use rocuronium for tracheal intubation followed by repeated bolus injections afterwards and to reverse the effect of rocuronium with sugammadex at the end of surgery (group R/S). No specific target was given to the anaesthetist as to what the TOF ratio should be at the time of tracheal extubation, or what other criteria should be fulfilled before extubation.
Anaesthesia and perioperative care
All patients were premedicated with oral midazolam 3.75–7.5 mg ∼45 min before the operation began. Routine monitoring (electrocardiogram, noninvasive blood pressure recording, pulse oximetry and capnometry) was applied. End-tidal CO2 concentration was kept at 35–45 mmHg.
For total i.v. anaesthesia, after opioid preloading with remifentanil at a rate of 0.15–0.2 µg·kg−1·min−1 for 3–5 min, general anaesthesia was induced by bolus injection of propofol 2.0 mg·kg−1. Anaesthesia was then maintained with propofol 5–7 mg·kg−1·h−1 and remifentanil 0.1–0.3 µg·kg−1·min−1 continuously. Depth of anaesthesia was assessed by bispectral index scale monitoring (Covidien, Mansfield, MA, USA). During surgery, the propofol infusion rate was adjusted to target a bispectral index scale between 40 and 60. Towards the end of the operation, when the surgeon announced a remaining operating time of 5–10 min, propofol and remifentanil were discontinued or infusion rates were reduced.
The following variables were noted on a separate evaluation sheet with the help of a medical student (D.G.) involved in this project: exact time of the end of surgery; inspiratory tidal volume and respiratory rate shortly before tracheal extubation; the time and individual TOF ratio at tracheal extubation; results of clinical tests at 2 min after tracheal extubation (i.e. lifting head for > 5 s for muscle strength; sticking out tongue and giving own name for cognitive function). TOF monitoring was terminated after tracheal extubation. Pulse oximetry was continued during transport of the patient to the recovery room. Time between tracheal extubation and arrival in the recovery room, as well as time spent in recovery, was documented. In the recovery room, all patients were monitored for clinical signs of residual paralysis as at 2 min after extubation, as well as for the development of delirium (nursing delirium score, with a score ≥ 2 predicting delirium), pain (numerical rating scale: 0, no pain; 1, worst possible pain) and postoperative nausea and vomiting, in accordance with our standards. 16
For postoperative analgesia, i.v. piritramid, administered in 1.5 mg fractions until pain was relieved, was used either alone or with metamizol (i.v. 2 g) or paracetamol (i.v. 1 g).
Curarization
Before tracheal intubation, patients in group M received an i.v. bolus of 0.2–0.25 mg·kg−1 mivacurium. After recurrence of T1 (the first of the four TOF count twitches), mivacurium was continuously infused at a rate of 3–15 µg·kg−1 min−1 to keep the depth of curarization between 0 and 1 twitches until wound closure.
Patients in group R/S received an i.v. bolus of 0.45–0.6 mg·kg−1 rocuronium before tracheal intubation and ∼0.15 µg·kg−1 (i.e. ∼25% of the initial dose) after recurrence of T1. Sugammadex was i.v. injected 1–2 min before tracheal extubation at a bolus dose of 2–4 mg·kg−1 for reversal of NMB, if the TOF count was 0–1.
Neuromuscular monitoring
For neuromuscular monitoring, the TOF Watch SX (Organon, Oss, The Netherlands) was used. For this, the right arm of the patient was placed on the operating table’s arm board, in slight supination. The four ulnar fingers were immobilized with the provided hand adaptor (Organon), then fixed to the arm board with tape. After preparation of the skin with propyl alcohol, two ECG electrodes were put over the ulnar nerve at the wrist ∼5 cm apart, the negative electrode distal to the positive one. The acceleration transducer was placed over the volar aspect of the distal phalanx of the thumb. Palmar skin temperature was measured and kept at > 32℃. The i.v. line was placed into the same arm. Muscle relaxation monitoring (acceleromyography) was started after induction of anaesthesia but before the administration of the muscle relaxant, with two or three on-demand 2 Hz TOF stimulations. Calibration (CAL2 mode) was then started to determine the individual supramaximal threshold and to calibrate the transducer sensitivity at 10% above the threshold up to 60 mA. Thereafter, repetitive TOF stimulations were performed for 2 min. If a stable control response could be detected (< 5% variation), mivacurium or rocuronium was administered and the individual normalized 0.9 TOF ratio was calculated (i.e. if the TOF ratio was 1.05 before curarization, the appropriate TOF ratio at the time of extubation would then have to be at least 1.05 × 0.9 = 0.95). This procedure was necessary because the TOF Watch SX does not automatically correct the TOF ratio with respect to the TOF ratio measured prior to NMB if it deviates from 100%. Normalization helps to detect postoperative residual curarization more reliably. 10 The decision to terminate the application of either relaxant, in addition to the decision to perform tracheal extubation, was at the discretion of the anaesthetist, guided by TOF and/or clinical signs.
Surgeon questionnaire
After the operation, the anaesthetist gave a questionnaire to the surgeon, asking about the incidence and severity of general or bulbar movements and intraoperative coughing, as well as establishing the surgeon’s overall satisfaction with the conditions provided.
Endpoints
The primary outcome measure was the degree of recovery from NMB, as indicated by the TOF ratio of the adductor pollicis muscle at the time of tracheal extubation. Secondary outcome measures were the time period from the end of surgery to tracheal extubation and the surgeon’s opinion of the surgical conditions with the two curarization regimens.
Ethical approval
Ethical approval to analyse and publish the data from this institutional anaesthetic practice evaluation was provided by the Ethics Committee I at the Charité – Universitätsmedizin Berlin (Chairperson Prof. R. Morgenstern) on 1 November 2011 (EA 1/205/11). Informed consent was waived because this was an observational institutional anaesthetic practice evaluation without any intervention. It reflected daily routine and reported data from a completely anonymized data set.
Statistical analyses
Continuous data were described as mean and standard deviation (SD); categorical data were presented as number and percentage, median and interquartile range (IQR) or 95% confidence interval (CI). After exploratory analysis of primary and secondary end points (including checks for normality), the clinical effect variables were tested using the nonparametric Mann–Whitney U-test for comparisons between independent groups. After having found a significant difference between the two regimens in terms of the TOF ratio at tracheal extubation, a power calculation was performed, resulting in a power of 98% for group sizes of 17 each, and α = 5% (two-sided). Frequencies were compared using Fisher’s Exact test. P-values ≤ 0.05 were considered statistically significant. All tests were conducted for exploratory data analysis, therefore no adjustments for multiple testing were made. Data analysis was performed using IBM SPSS® statistical software, version 20 (SPSS Inc., Chicago, IL, USA).
Results
Baseline characteristics of patients undergoing high-risk eye surgery, where muscle relaxation regimens with either mivacurium (group M) or or rocuronium/sugammadex (group R/S) were evaluated.

Data presented as mean ± SD, n (%) or n.
ASA, American Society of Anesthesiology; BMI, body mass index; M, mivacurium; R/S, rocuronium/sugammadex.
No statistically significant differences were observed (P ≥ 0.05; Mann–Whitney U-test and Fisher’s exact test).
We co-operated with three eye surgeons (two consultants and the head of the department). A total of 39 patients (30 PPVs and nine keratoplasties) were evaluated (Table 1). Anaesthesia was performed by 11 anaesthesiologists (nine staff anaesthesiologists and two anaesthetists in training, in their penultimate or last year).
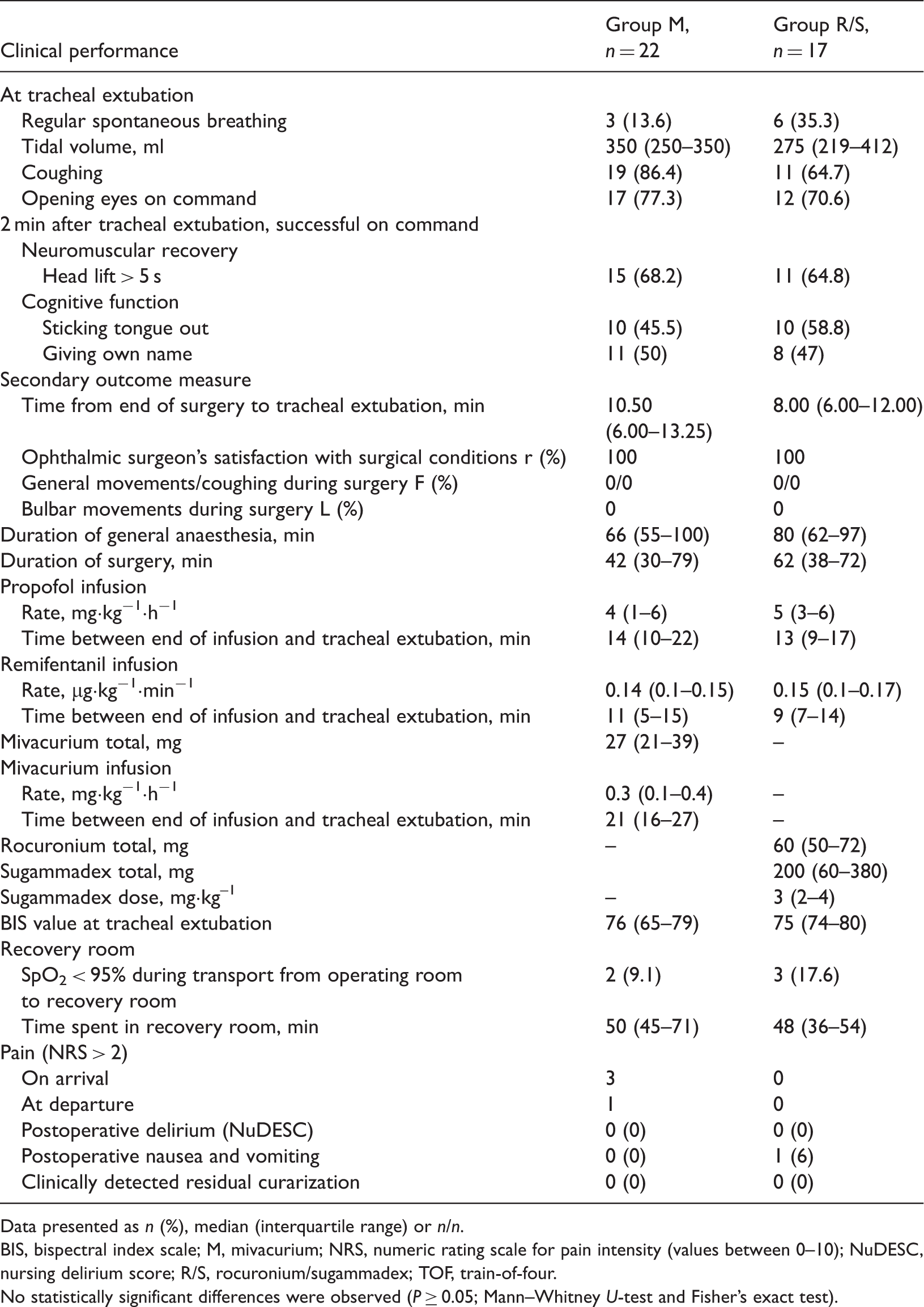
At the time of tracheal extubation, a significantly greater TOF ratio was found in group R/S compared with group M (P < 0.0001; Figure 1). At the time of extubation, all patients were breathing regularly or had started to cough (Table 2). In both groups, clinical signs did not reliably reflect neuromuscular recovery 2 min after extubation (Table 2). The time to tracheal extubation did not differ between groups. The surgeons were completely satisfied with the surgical working conditions during both regimens (Table 2). No significant differences with respect to time spent in the recovery room, postoperative nausea and/or vomiting, postoperative pain or postoperative delirium were found. None of the patients presented with clinical signs of residual curarization in the recovery room (Table 2).
Proportions of patients who had train-of-four (TOF) ratios ≥ 0.9 (not normalized) at the time of extubation treated with mivacurium (group M, five of 22) or rocuronium/sugammadex (group R/S, 17/17). Median (interquartile range) given in the boxes. *P < 0.001. Clinical performance at tracheal extubation and 2 min after tracheal extubation, and intra- and post-operative variables, in patients undergoing high-risk eye surgery, where muscle relaxation regimens with either mivacurium (group M) or or rocuronium/sugammadex (group R/S) were evaluated. Data presented as n (%), median (interquartile range) or n/n. BIS, bispectral index scale; M, mivacurium; NRS, numeric rating scale for pain intensity (values between 0–10); NuDESC, nursing delirium score; R/S, rocuronium/sugammadex; TOF, train-of-four. No statistically significant differences were observed (P ≥ 0.05; Mann–Whitney U-test and Fisher’s exact test).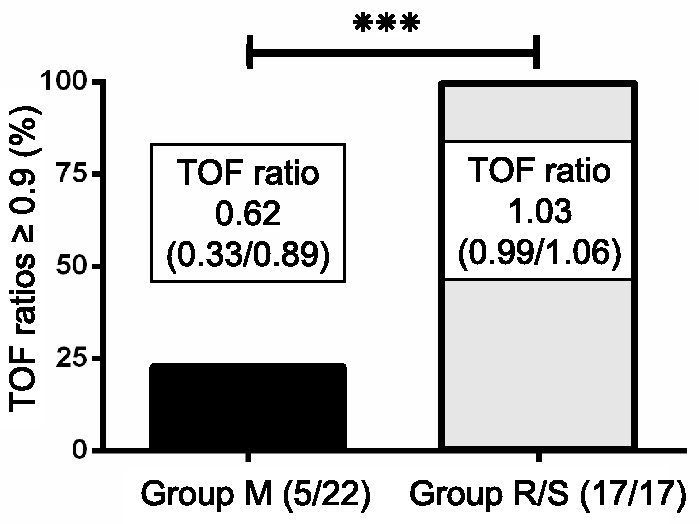
Discussion
In this institutional anaesthetic practice evaluation, no specific target (e.g. TOF ratio ≥ 0.9) was given and the decision when to extubate was left to the discretion of the anaesthetist. Under these circumstances, the main finding of our study was that the TOF ratios in the M group at the time of tracheal extubation revealed considerable residual curarization, while there was no residual curarization in the R/S group. Thus, in a setting like ours, the safety profile appears to be substantially improved when using the rocuronium/sugammadex regimen.
Unlike the TOF ratio, the clinical criteria did not reliably reflect residual curarization in our study. This is in line with findings of Murphy et al., 17 who also demonstrated the insensitivity of clinical criteria for determining the appropriate timepoint for tracheal extubation in gynaecology and general surgery patients. In the study by Murphy et al., the mean TOF ratio at tracheal extubation was 0.67 ± 0.2 (58% had a TOF ratio < 0.7 and 88% had a TOF ratio < 0.9), 17 very similar to our present findings.
The significantly greater TOF ratio in group R/S compared with group M at the time of extubation implies that 77.3% (17/22) of the patients in group M were extubated, even though the TOF ratio still suggested residual curarization (12 with TOF ratio < 0.7 and five with TOF ratio 0.7–0.89), whereas all patients (17/17) in group R/S had a TOF ratio > 0.92 (P < 0.0001). If the TOF ratios were normalized according to the TOF ratios measured directly before the initial curarization – which were 1.06 (IQR 1.04–1.09) in group M and 1.02 (IQR 0.99–1.07) in group R/S (P = 0.073) – the TOF ratios at tracheal extubation would have had to reach 0.96 (IQR 0.93–0.98) in group M and 0.92 (IQR 0.89–0.97) in group R/S (P = 0.329). If these stricter values of the normalized 0.9 TOF ratio had been applied, only 18% (four of 22) of the patients in group M would have reached or exceeded a normalized TOF ratio of 0.9 at tracheal extubation, versus 100% (17/17) of those in group R/S (P < 0.0001).
Our study included patients with applicable eye surgeries with no further selection criteria or randomization. Anaesthesia was to be performed as total i.v. anaesthesia, according to our clinical standard for intraocular surgery. 8 Within this setting, the anaesthetists were free to use either one of the two relaxation regimens. Also according to our standards, the intraoperative depth of muscle relaxation had to be kept at 0 or 1 twitches, but no target TOF ratio was given at which tracheal extubation had to be performed. This allows us to present data of muscle relaxation practice in eye surgery that are not influenced by a study protocol and do thus reflect ‘true’ daily practice.
Muscle relaxation measurements are not regularly performed throughout Europe. According to a survey in the UK, 62% of anaesthesiologists do not use nerve stimulators at all and 90% do not use an objective (quantitative) form of monitoring of NMB. 18 Studies show that in Denmark and Germany, only 43 and 28% of anaesthetists, respectively, routinely monitor NMB.19,20 But even if relaxation monitoring is established, postoperative residual curarization at the time of tracheal extubation may still be encountered, as was impressively demonstrated in group M of this study.
Postoperative residual curarization is associated with an elevated incidence of morbidity and mortality. 21 It confronts the anaesthetist with high-risk situations, such as: reduced respiratory muscle strength and inability of the patient to clear secretions from the upper airway; reduced pharyngeal muscle strength with the risk of upper airway obstruction and silent aspiration;22–24 reduced hypoxic ventilatory response.25–27 Insufficient respiratory function, with a consequent increase in paCO2, may also lead to an increase in intraocular pressure and hence endanger surgical outcome. Not least of all, the subjectively felt degree of paralysis constitutes a substantial contributor to postoperative emotional stress and may endanger patients, especially those with multiple morbidities, who are frequently encountered among ophthalmology patients. 28 Therefore, the benefits of using objective NMB monitoring to minimize and/or prevent postoperative residual curarization are beyond doubt.29–33
In view of the consequences just described, it is relevant to consider the reasons for disregarding the muscle relaxation monitor readings at the time of tracheal extubation. Some of the anaesthesiologists involved in this study might have regarded the old benchmark TOF ratio of 0.7, which was established in the mid-1970s, 34 as sufficient. However, a TOF ratio ≥ 0.9 is now recommended before tracheal extubation.35,36 Others may have thought that no visible or palpable fade in the TOF response indicates sufficient neuromuscular recovery, not knowing that fade can only reliably be felt at TOF ratios < 0.4, and that the failure rate to detect fade by tactile and visual evaluation at TOF ratios between 0.41 and 0.70 lies somewhere between 40 and 80%. 37 However, since nine of the 11 participating anaesthetists were staff anaesthesiologists with several years of experience in anaesthesia for ophthalmic surgery, we regard a lack of experience with either the surgical procedures or general anaesthesiological requirements as being highly unlikely. Some of our anaesthetists obviously performed early extubation, to prevent the patient from coughing because the tube was no longer tolerated. For this, they were relying on clinical signs (such as respiratory function), but most of all they were relying on their personal experience to call the patient fit for tracheal extubation, disregarding the exact degree of neuromuscular recovery (TOF ratio) displayed on the muscle relaxation monitor, as long as four seemingly equally strong twitches were visible or palpable.
Although no significant difference in favour of group R/S could be noted for the time passing between the end of surgery and the time to tracheal extubation, we postulate that this may have been different if the anaesthesiologist had waited until a TOF ratio of ≥ 0.9 in group M had been reached. Due to the fast recovery time, which appears to be independent of the duration of the continuous mivacurium infusion, anticholinesterases to antagonize mivacurium have not been recommended. 38 Admittedly, the general onset of action of neostigmine in a dose of 0.04–0.07 µg·kg−1 is ≤ 1 min, but its peak effect does not occur for another 9 min. 39 In the double-blind, placebo-controlled study by Jahr et al., 40 the time to tracheal extubation after a mivacurium infusion was reduced by only 3.6 ± 3.3 min after edrophonium/atropine administration. Ting et al. 41 showed a reduction in recovery times from NMB after edrophonium/atropine, but the patients in this double-blind, placebo-controlled investigation could not be extubated faster than those without antagonization. The muscarinic side-effects of anticholinesterases include bradycardia and prolongation of the QT interval, 42 bronchoconstriction, 43 increased salivation, 44 miosis 44 and increased intestinal tone; 44 whether the incidence of postoperative nausea and vomiting increases after application of anticholinesterases remains controversial.40,45,46 In the context of eye surgery, postoperative nausea and vomiting constitutes an even more unwanted event, since a rise in intraocular pressure can be highly detrimental to the surgical outcome. Consequently, following intraocular surgery, we do not find the use of anticholinesterases after mivacurium infusions justified, since only minimal time loss is to be expected when simply waiting for spontaneous neuromuscular recovery.
For the National Health Service in the UK, a health technology assessment of the cost-effectiveness of sugammadex for reversal of moderate blockade came to the conclusion that ∼20 min of recovery time in the operating room would have to be saved to render sugammadex cost-effective, 14 not considering the possible monetary benefits of avoiding postoperative residual curarization-induced complications. In comparison, provided that one 200 mg vial of sugammadex is sufficient for reversal (depending on the individual patient’s body weight), in our institution, time in the operating room would need to be reduced by 6.7 min to recover the costs of sugammadex (fixed costs: €15/min in the operating room versus €100 for 200 mg sugammadex). Thus, the cost-effectiveness of sugammadex seems to be highly dependent on the setting in which it is administered (e.g. the hospital, the patient and whether it is administered in the operating room or the recovery room).
There was no randomization with respect to which of the two relaxation regimens was performed by the anaesthetist in our study, and there was therefore no blinding. We do not regard this aspect of study design as a limitation; instead we think this is an indispensable prerequisite for any practice evaluation to obtain valid results. Nonetheless, there may have been some bias because the anaesthetists involved all had thorough experience in the field and knew that anaesthetic practice was being evaluated. Therefore, the results may actually represent a best-case scenario, as routine muscle relaxation monitoring without supervision may be conducted even more insufficiently (or possibly omitted completely).
In conclusion, an educational programme, focused on the use of neuromuscular monitoring and the clinical implications of different TOF ratios for patient safety, seems to be urgently needed. Performing extubation safely is certainly possible when using mivacurium but usually requires a longer period from the end of the operation until extubation, as in the present study, to allow full neuromuscular recovery or requires the use of anticholinesterases. We would not promote the latter option for intraocular surgery, especially when using the (usually) short-acting mivacurium. Therefore, in patients at risk of airway complications or aspiration, in addition to frail patients, muscle relaxation with rocuronium should be considered. The action of rocuronium can be reversed swiftly by sugammadex if necessary, assuring complete reconstitution of neuromuscular function and consequently avoiding complications such as silent aspiration or pneumonia.
Footnotes
Acknowledgements
We thank Kathrin Scholtz for her assistance in preparing the documents for the Ethics Committee and Erika Schulte, MD for her assistance with the statistical analysis included in this paper. Both are affiliated to the Department of Anesthesiology and Intensive Care Medicine, Charité – Universitätsmedizin Berlin, Berlin, Germany.
Declaration of conflicting interest
Willehad Boemke has received payments for lectures from MSD Sharp & Dohme, Haar, Germany. Claudia Spies has received grants from MSD Sharp and Dohme, Haar, Germany. The other authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.