
Abstract
Objectives
To identify epidemiological determinants of the contact behaviour of children and their impact on parental employment, during school closures that took place over the course of the 2009 pandemic influenza (H1N1-2009) in Japan.
Methods
A retrospective survey was conducted in Japanese households between October 2009 and May 2010 by administration of a standardized questionnaire. Demographic and behavioural variables were explored, in association with the frequency with which children left the home and the risk of parents being absent from work during school closures.
Results
Data from 882 eligible households were analysed. A total of 181/882 (20.5%) of households reported that children left the home for nonessential reasons during school closures. No impact on parental working hours was reported by 742/882 (84.1%) of households. Univariate analyses showed that the frequency with which children left the home was dependent on age, extent of school closure and requirement for special childcare arrangements.
Conclusions
A greater understanding of age-dependent behaviours, during school closures as a consequence of a pandemic, is required. Consideration of a public policy to permit a paid leave of absence from work for parents during school closures may be beneficial; the cost-effectiveness of such a measure should be assessed in future.
Keywords
Introduction
School closure is a key component of public health interventions against an influenza pandemic. 1 Public health interventions are conventionally classified into pharmaceutical and nonpharmaceutical interventions. Nonpharmaceutical interventions are nonspecific but are applicable in a variety of settings, including school closures. It is important to put in place nonpharmaceutical interventions at the emergence of a pandemic, since vaccine production and distribution may take 4–6 months. Furthermore, the stock of antiviral agents tends to be limited by serious concerns over the spread of resistant strains. 1
School children are known to act as maintenance hosts of influenza, therefore the rationale for a school closure programme is to reduce contact and subsequent transmission within the school setting. 2 During the course of the 2009 pandemic, however, surveys reported that children had used the extra time that they gained from school closures to attend parties or prep-school lectures outside of the home.3,4 The behaviour of students during school closures is critical as it can influence the frequency of contacts among children, thereby diluting the effectiveness of the closure. Compensatory behaviour among school children has been referred to as the ‘compensation of contact’ and is recognized to be a key determinant of the success of school closure interventions. 5
While school closure continues to represent a nonpharmaceutical intervention against future pandemics, few published studies have examined the possible adverse effects of school closure programmes. The present study used data from a retrospective household survey to identify epidemiological determinants that influenced the behaviours of children and their parents, during the course of the H1N1-2009 pandemic in Japan. In particular, two specific outcomes were examined: children leaving the home during periods of school closure; disturbance to parental work as a result of such closures.
Subjects and methods
Study population
A retrospective survey of nonrandomly sampled households in Japan was conducted between 1 October 2009 and 31 May 2010. During the 2009 pandemic, household respondents for this survey were invited from a Japanese community of research monitors, established for the conduct of multiple original studies. 6 Formation of the community was by respondent-driven sampling, maintained by a commercial research company in Tokyo, Japan. 6 The size of the community changes with time, but never involves <10 000 monitors from different Japanese households. Households were included in the study if: (i) the size of the household (including the index case) was two or more; (ii) the household had at least one child aged between 4 and 17 years; (iii) the child experienced school closure or class suspension at least once between May 2009 and the time of enrolment.
Enrolment was based on area sampling across Japan, depending on the population size at each prefecture, and only one adult respondent was invited from a single household. The sampling was made by inviting two control households for each household that had at least one index case. Following area sampling, households with at least one symptomatic case were initially invited to participate in the survey; control households, regardless of geographical area, were subsequently identified. A symptomatic case was defined as: (i) a confirmed case of H1N1-2009 influenza, diagnosed by reverse transcription–polymerase chain reaction; (ii) a suspected case of H1N1-2009 influenza, based on rapid diagnostic testing; (iii) a case of influenza-like illness, characterized by objective or subjective fever and a cough or sore throat. Voluntary participation of households with at least one index case was invited, until the number of households in each region reached one-third of a predetermined maximum number that was proportional to the regional population size. Households were classified into four groups depending on the school year of the eldest child, as follows: kindergarten; primary school; junior high school; high school.
Respondents were fully aware that enrolment in the study was voluntary and that they could withdraw from participation at any time. For each household, adult respondents were informed of how the data would be used and were assured of the confidentiality of their responses. Written informed consent was obtained from all adult respondents. Approval of the study protocol by a human ethics committee was not required, as the survey did not involve prevention or treatment in individual subjects and recorded existing information anonymously. Respondents received remuneration, based on the commercial research company’s points system: each research monitor is granted a fixed point on completion of each single questionnaire; following completion of multiple questionnaire surveys, the accrued points can be exchanged for a gift card or shopping voucher. The survey was conducted in real time during the course of the pandemic (to minimize recall bias) and was completed by the end of May 2010.
Household survey questionnaire
A standardized questionnaire was electronically distributed to collect information on the behaviour of children and their parents during school closures. The questionnaire focused on two epidemiological outcomes: (i) the child leaving the home during the school closure; (ii) parental absenteeism from work (including a full day of absence or a reduction in working hours) to take care of the children. The contents of the questionnaire adhered to previously published surveys,4,5,7,8 but also stratified subjects by the eldest child’s school year and their history of infection during the school closure. Some open-ended questions were also included.
Respondents provided the following information: the school year; age and sex of the child; onset of illness (if any) during the school closure period; household size; household income; highest educational level in the household; parental perspectives on the appropriateness of the school closure; degree of preparedness for school closures/class suspension; details of how the school closure affected their own employment and daily routine; the need for special childcare arrangements due to the closure; whether the child went out of the home during the school closure period (and for what reason). All questions regarding the child were provided for the eldest child in the household only. Households were also described according to the absence of at least one parent who could care for a child during school closure; such households were those in which: (i) both the husband and wife regularly worked; (ii) one parent was a full-time worker and the other was a part-time worker; (iii) there was only one parent.
Statistical analyses
Descriptive statistics for demographic, behavioural and epidemiological characteristics of respondents and their children were summarized. In addition, two outcome variables were prespecified: (i) children leaving the home during the school closure; (ii) disturbance to parental employment as a result of the closure. Both outcomes were handled as dichotomous, and potential interactions with other dichotomous or ordinary variables were explored. Due to difficulties in explicitly addressing confounding factors, and because the primary aim of the analysis was to identify probable characteristic factors of the outcomes, only univariate associations were examined using Fisher’s exact test or the χ2-test. The level of statistical significance was set at α = 0.05. All statistical data were analysed using JMP statistical software, version 9.0.0 (SAS Institute, Cary, NC, USA).
Results
Demographic data from 882 Japanese households affected by school closures during the H1N1-2009 influenza pandemic.
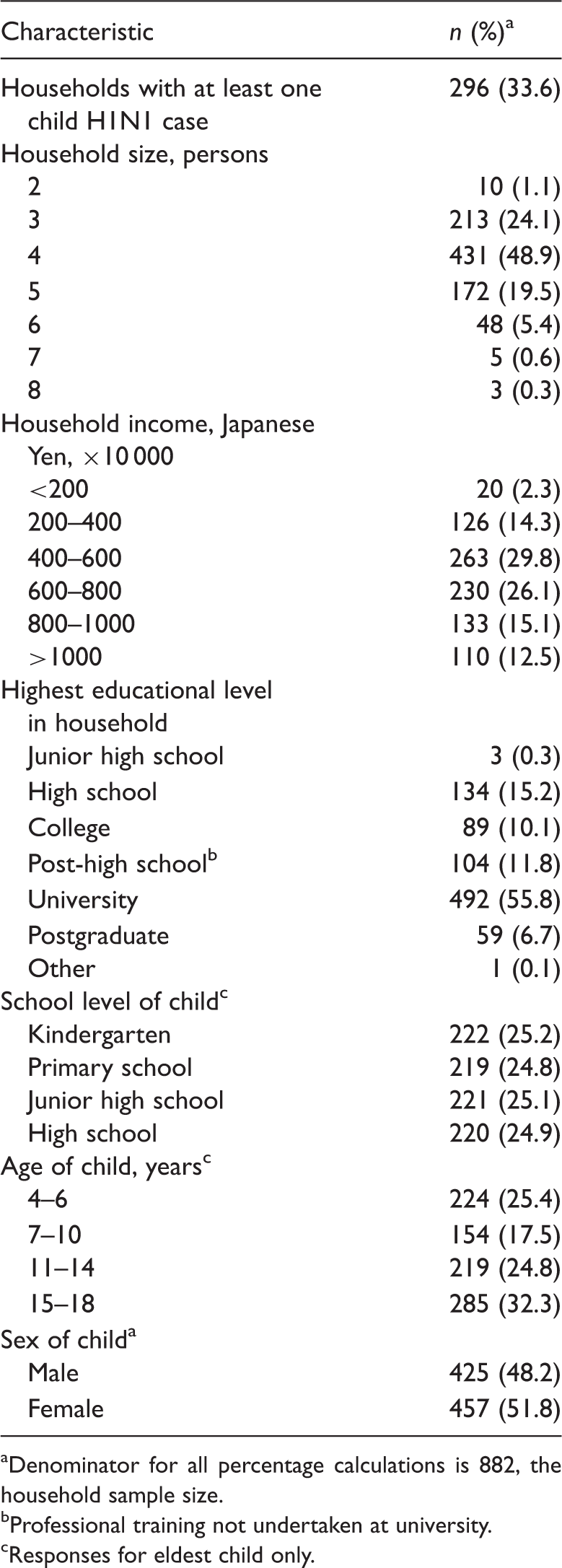
Denominator for all percentage calculations is 882, the household sample size.
Professional training not undertaken at university.
Responses for eldest child only.
Behaviour of children from 882 Japanese households in relation to staying at home or engaging in outside activities during school closures, as a response to the influenza H1N1-2009 pandemic.
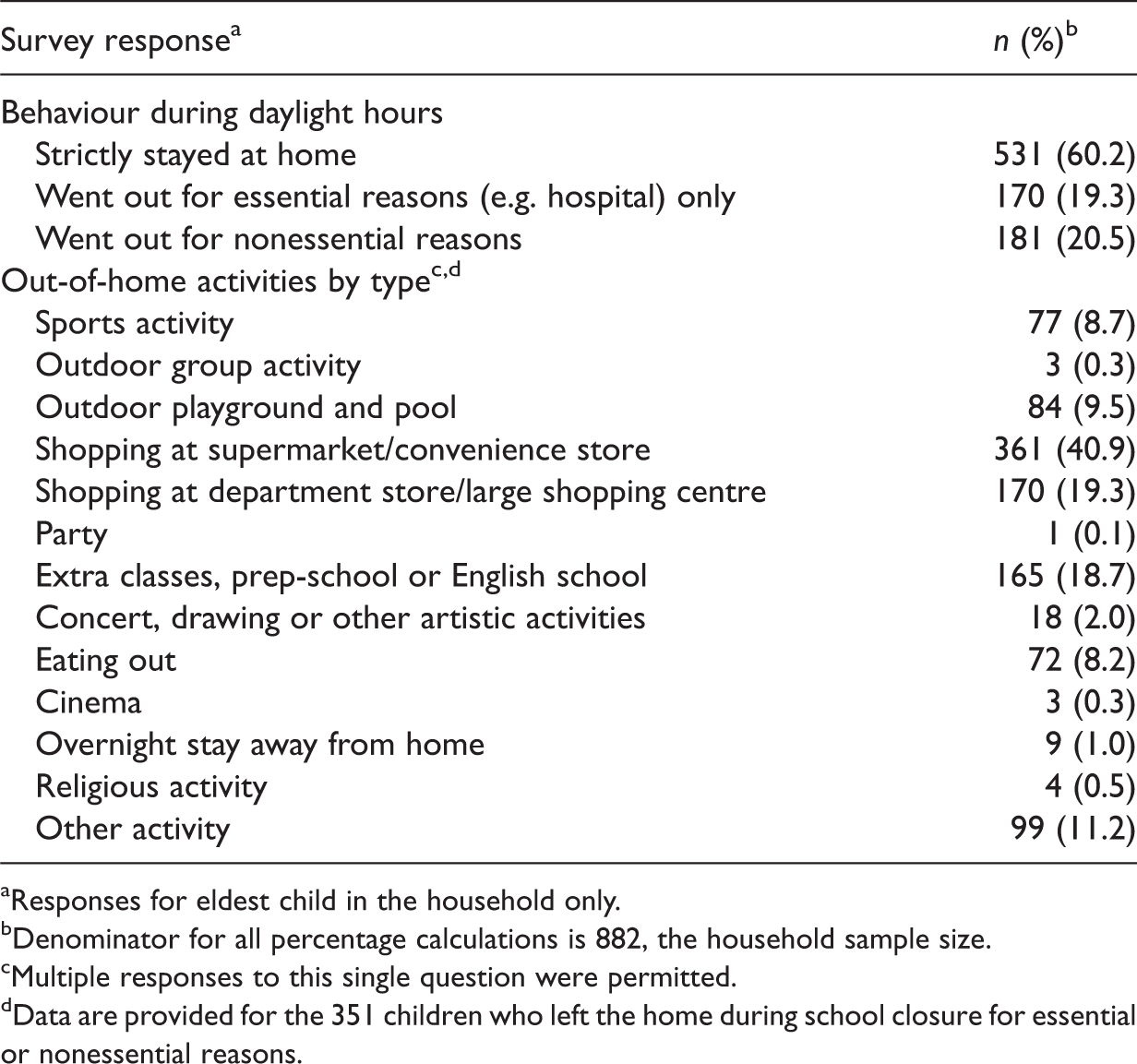
Responses for eldest child in the household only.
Denominator for all percentage calculations is 882, the household sample size.
Multiple responses to this single question were permitted.
Data are provided for the 351 children who left the home during school closure for essential or nonessential reasons.
Parental attitudes and impact on parental employment in 882 Japanese households affected by school closures as a consequence of the influenza H1N1-2009 pandemic in Japan.
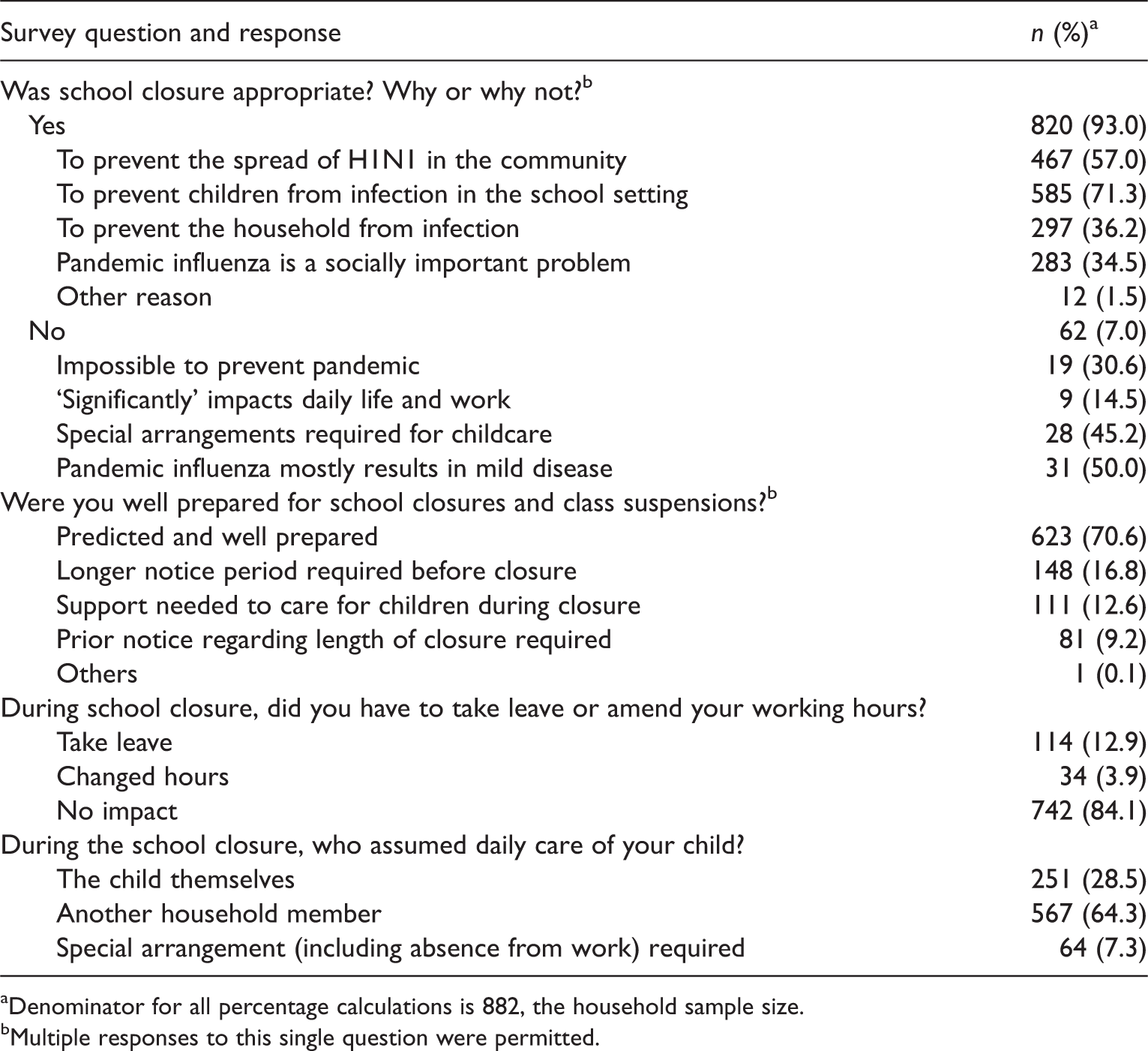
Denominator for all percentage calculations is 882, the household sample size.
Multiple responses to this single question were permitted.
Univariate analyses demonstrated that the sex of the child, household educational level, household income and household size were not associated with the likelihood of the child leaving the home during school closure, or of parents having to take a leave of absence from work in order to care for their child. The extent of the school closure was significantly associated with the frequency of children leaving the home: closure of the entire school, closure of a single grade or single class suspension were associated with 47.8% (75/157), 32.2% (64/199) and 40.3% (212/526) of children leaving the home, respectively (P = 0.01). Younger children were more likely to leave the home during the closure, with 53.2% (118/222) of kindergarten pupils, 42.5% (93/219) of primary school pupils, 30.3% (67/221) of junior high school pupils and 33.2% (73/220) of high-school pupils reporting that they left the house at least once (P < 0.01). Primary school pupils were most likely to leave the home to visit a supermarket or convenience store, followed by high school pupils (P = 0.05 for the association between school category and shopping). Junior high school pupils and primary school pupils were more likely to leave the home to attend extracurricular studies (including prep-school and English school) compared with pupils in other school categories (P = 0.02).
Parents in households with a child attending kindergarten or primary school tended to be absent from work more frequently than parents with older children; absence from work was observed in 17.1% (38/222), 20.6% (45/219), 15.4% (34/221), and 10.5% (23/220) of households with a kindergarten, primary school, junior high school or high-school pupil, respectively (P = 0.03). The risk of a parent missing work was significantly greater in those households where at least one parent could not assume childcare responsibilities; 28.7% (109/380) of parents in such households reported missing work compared with 6.2% (31/502) of parents in other households (odds ratio [OR] 6.1 [95% confidence interval [CI] 4.0, 9.4], P < 0.01). Parental absence from work was also significantly associated with the requirement for special childcare arrangements; parents in 44/64 (68.8%) of households that needed to make special childcare arrangements were forced to take a leave of absence from work, compared with 29/251 (11.6%) and 67/567 (11.8%) of households with independent children, or with at least one other household member who could take care of the child, respectively (P < 0.01).
Proportionately fewer children left the home in households that believed school closure was an appropriate response to the pandemic, compared with those households that felt the closure was inappropriate (318/820 (38.8%) versus 33/62 (53.2%), P = 0.03). Children were more likely to leave the home in households where special childcare arrangements were required during school closure, compared with households in which the children were independent and able to take care of themselves (34/64 (53.1%) versus 90/251 (35.9%), P = 0.04). The infection status of children was not a significant predictor of their behaviour to leave the home, but was a significant predictor of parental absence from work (P < 0.01); parents had to miss work in 80/296 (27.0%) of households with an infected child, compared with 61/586 (10.4%) of households in which children were not infected (OR 3.1 [95% CI 2.2, 4.5]).
Discussion
The present study investigated the contact behaviour of children and parental employment behaviour during school closures as a consequence of the pandemic influenza (H1N1-2009) in Japan. A large proportion of children (79.5%) spent the closure days at home (Table 2), only leaving the house for essential reasons; most households (84.1%) reported that parents did not miss any work days or change their working hours in order to care for their children (Table 3). These data are consistent with similar surveys in the USA.4,9 The present study also identified that younger children and more extensive school closures were significantly associated with a higher frequency of children leaving the home during such closures. Parental belief in the appropriateness of the closure, and children being able to care for themselves during the closure, were significantly associated with a lower rate of going-out behaviour. The risk of parents having to take a leave of absence from work was positively associated with the infection status of the child, younger age of the child and the absence in the household of at least one parent who could assume childcare responsibilities. Parents were less likely to be absent from work if the household included independent children who could care for themselves during the closure.
Data from this epidemiological study suggest that, in order to ensure the feasibility and maximize the effectiveness of school closure programmes, it is vital to limit unnecessary contacts among children during this time; appropriate measures are required to achieve this. The present study demonstrated that contact was more likely with younger children (attending kindergarten or primary school) during the closure. Similarly, the age-dependency in psychological response (e.g. risk perception and willingness to accept intervention) to the pandemic has been observed among adults. 10 Depending on age or school category, children left the home for different reasons and, as such, the corresponding optimal countermeasures are also likely to be age-dependent.11,12 Moreover, measures to improve the acceptance of school closure among parents should be implemented, since it is important that there is a proper understanding of why contact among children should be restricted. Taken together, data from the present survey suggest that a substantial effort regarding risk communication should be undertaken in advance of the next pandemic. It is important for parents that the impact of school closures on their own employment is minimal and it is likely their acceptance of closures is directly related to this. The present study demonstrated that the age of the child, the independence of the child and the absence of one parent in the household who could assume childcare responsibilities were probable determinants of the risk of parental absenteeism. Addressing these points requires public support to change and improve the working environment for parents of children affected by school closures. A government policy to permit paid leave during school closures may, for example, be worth considering under these circumstances, and the cost-effectiveness of such a policy should be explored in future.
There were some limitations to the present study. First, the participants were derived from a convenient sampling procedure rather than from a random selection, meaning that a potential selection bias could not fully be avoided. Secondly, it was not possible to avoid recall bias since the survey involved several months of recall. Finally, although the results may be useful to inform policymaking in general, they can only be directly applied to a Japanese population. In the case of other populations with different cultural, ethnic and geographical backgrounds, household responses to school closures may be very different compared with those reported by the present survey.
In conclusion, the present study identified that a large proportion of children affected by school closures in response to the influenza H1N1-2009 pandemic in Japan stayed at home or went out for essential reasons only during the prescribed closure. Furthermore, the majority of parents reported little or no impact on their working hours as a consequence of the closure. The frequency with which children left the home was age dependent, suggesting that there is a requirement for a more detailed understanding of age-dependent behaviours under these circumstances and for the optimal countermeasures to prevent child contact during a pandemic. A public policy to permit a leave of absence from work during periods of school closure could be a valuable option to parents and the potential effectiveness of such a measure should be assessed in future.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
Hiroshi Nishiura received funding support from the JST Agency PRESTO programme. This work also received financial support from the Harvard Centre for Communicable Disease Dynamics of the National Institute of General Medical Sciences (grant no. U54 GM088558). The funding bodies were not involved in the collection, analysis or interpretation of the data, the writing of the manuscript or the decision to submit for publication.