
Abstract
Objectives
To investigate (i) the relationship between the ratio of fresh gas flow to min volume (FGF/MV) and the ratio of the fraction of inspired sevoflurane to the delivered concentration of sevoflurane (FI/FD); (ii) to establish the saturation state of sevoflurane anaesthesia and factors affecting the volume of ejected sevoflurane through the nonrespiratory tract route (nVERT) during the saturation state.
Methods
Two studies were undertaken in patients with cancer, scheduled to undergo surgery. All patients received tracheal intubation and inhaled sevoflurane. In study 1, anaesthesia parameters were fixed, the initial FD of sevoflurane was 2.2% vol and the FGF/MV was set to 0.2, 0.3, 0.4 and 1.0 in groups A, B, C and D, respectively. In study 2, FGF = MV and the initial FD of sevoflurane was 2.2% vol, but the tidal volume (TV) was set to 6, 8 or 10 ml/kg in groups I, II and III, respectively.
Results
Study 1 (n = 60) showed a positive relationship between FI/FD and FGF/MV. In study 2 (n = 60), when TV was fixed, nVERT increased during the saturation state as FD increased; when FD was fixed, nVERT remained stable, despite increased TV.
Conclusions
FI/FD is positively associated with FGF/MV; nVERT is affected by FD but not TV.
Introduction
At the initiation of inhalation anaesthesia with sevoflurane, it is important to make the fraction of the end tidal sevoflurane (Fet) go up to (and stabilize at) the expected value as soon as possible, in order to get enough depth of anaesthesia 1 It is usual to set a high delivered concentration (FD) of volatiles, increase the fresh gas flow (FGF), min volume (MV) and inhalation time (determined by the ratio of inhalation time : exhalation time [I : E]), in order to achieve this aim. The first step is to increase the fraction of inspired (FI) sevoflurane. The gas with the concentration of FD coming from the volatilizer to the adapter (monitoring FI) that connects the tracheal catheter and corrugated tube is diluted by air in the circuit, and some of exhaled tidal volume (TV) takes part in the next inhaled TV. The main factors affecting FI include the velocity with which sevoflurane fills the circuit of the anaesthesia machine and how much of the exhaled TV is taken in with the next inhaled TV. 1 Therefore, with greater FGF and MV, sevoflurane fills the circuit rapidly, less exhaled TV is taken in with the next inhaled TV and FI reaches FD more quickly. 1
Low-flow anaesthesia has been used for several decades, although it requires a high FD and low or normal FGF at the beginning of anaesthesia.2,3 The most important problem of low-flow anaesthesia is that the monitoring parameters (including FI and Fet) are not very stable, so it is difficult to maintain a sufficient and stable fractional concentration of venous blood (Fv), and to achieve depth of anaesthesia rapidly. In my opinion, to make the Fet go up to (and stabilize at) the expected value as quickly as possible, FI must be initially made to go up rapidly, and to stabilize at a large value. Usually, a high FD can be set and FI is allowed to reach FD. Because sevoflurane is metabolized by the liver,4,5 eliminated by the kidneys,6,7 absorbed by blood, combined with plasma proteins and diffused into tissues and the environment, FI must be kept constant, and a certain amount of time is required for the fractional concentration of air sac (FA), arterial blood (Fa), tissue fluid (Ft), Fv and Fet to increase up to (and stabilize at) their maximum concentrations.
Although it has long been known that FI reaches FD faster with increased FGF, the relationship between FI/FD and FGF/MV for sevoflurane anaesthesia has not been addressed. Because patients of different body weights (which is used to determine MV) require different FGFs, it is important to understand the relationship between FI/FD and FGF/MV. Doing so allows anaesthesiologists to determine how to achieve a stable FI, Fet and depth of anaesthesia by setting some reasonable parameters on the anaesthesia machine at the beginning of anaesthesia induction. This current report describes two separate studies that: (i) investigated the relationship between FGF/MV and FI/FD; (ii) established the saturation state of sevoflurane anaesthesia and the factors affecting the volume of ejected sevoflurane through the nonrespiratory route (nVERT), during the saturation state, in patients with cancer who were scheduled to undergo surgery.
Patients and methods
Study design
This current report presents the findings from two separate studies that were undertaken in two separate groups of patients, herein called study 1 and study 2. Procedures used in each study are described separately.
Study procedures
Study 1
This randomized prospective study included consecutive patients with breast cancer or thyroid gland tumours, scheduled to undergo surgery under combined intravenous and inhalation anaesthesia at the Department of Anaesthesiology, Cancer Hospital, Shanghai Medical College, Fudan University, Shanghai, China, between January 2009 and December 2010. The patients were divided randomly using a computer-generated randomization schedule into four groups (groups A, B, C and D). All patients were categorized as American Society of Anesthesiologists (ASA) physical status 1.
Ethical approval was provided by the Ethics Committee of Fudan University (clinical trial registration number: 3521-2009; Cancer Hospital, Shanghai Medical College, Fudan University) and written informed consent was obtained from all study participants.
A Dräger Fabius Tiro® (Dräger, Shanghai Branch, Shanghai, China) anaesthesia machine with Baxter sevoflurane (Baxter, Shanghai Branch, Shanghai, China) and a Dräger vaporizer (Vapor 2000; Dräger) were used for mechanical ventilation. A GE S/5 monitor (Baxter) was used to monitor FI and Fet in the tracheal catheter adapter. After anaesthesia was induced with midazolam (0.04 – 0.06 mg/kg), propofol (1.5 mg/kg), fentanyl (2 – 3 µg/kg) and norcuron (100 µg/kg), all patients were tracheally intubated and inhaled sevoflurane (2.2–2.6% vol; equivalent of 1.3–1.5 minimum alveolar concentration [MAC]) was administered, to maintain the depth of general anaesthesia. The TV was set to 500 ml (8 ml/kg), I : E = 1 : 1.5 and the respiration rate (RR) was set to 10 breaths per min (BPM). FD was initially set to 2.2% vol. The FGF/MV of groups A, B, C and D were set to 0.2 (1.0 l/min), 0.3 (1.5 l/min), 0.4 (2.0 l/min) and 1.0 (5.0 l//min), respectively. FI was recorded 1–10 min after the beginning of mechanical ventilation.
For group D, when Fet had reached the maximum and was stable at that value for >5 min, the times at which FI reached FD and Fet reached its maximum were recorded. FD was subsequently increased to 2.6% vol and then to 3.4% vol, and the times at which FI reached FD and Fet reached its maximum (for >5 min) were recorded. After the research procedures were completed and Fet was sufficient (1.3–1.5 MAC), the surgeons were permitted to begin the operation.
Study 2
This randomized prospective study included consecutive patients with breast cancer or thyroid gland tumours who were scheduled to undergo surgery under combined intravenous and inhalation anaesthesia at the Department of Anaesthesiology, Cancer Hospital, between January 2009 and December 2010. The patients were divided randomly using a computer-generated randomization schedule into three groups (groups I, II and III). All patients were categorized as ASA physical status 1.
Ethical approval was provided by the Ethics Committee of Fudan University (clinical trial registration number: 3521-2009; Cancer Hospital, Shanghai Medical College, Fudan University) and written informed consent was obtained from all study participants.
A Dräger Fabius Tiro® (Dräger) anaesthesia machine with Baxter sevoflurane (Baxter) and a Dräger vaporizer (Vapor 2000; Dräger) were employed for mechanical ventilation. A GE S/5 monitor (Baxter) was used to monitor FI and Fet in the tracheal catheter adapter. After anaesthesia was induced with midazolam (0.04 – 0.06 mg/kg), propofol (1.5 mg/kg), fentanyl (2 – 3 µg/kg) and norcuron (100 µg/kg), all patients underwent tracheal intubation and inhaled sevoflurane (dose adjusted based on study protocol) to maintain the depth of general anaesthesia. The TV was set as 6 ml/kg (group I), 8 ml/kg (group II) and 10 ml/kg (group III). Other parameters were: I : E = 1 : 1.5, RR = 10 BPM, FGF = MV and FD was initially set to 2.2% vol. When Fet had reached its maximum and had stabilized for >5 min, FI, Fet and the difference between FI and Fet (ΔF; FI − Fet) were recorded. FD was then increased to 2.6% vol and then 3.4% vol, and FI, Fet and ΔF were recorded when Fet had reached its maximum and had stabilized for >5 min. ΔF during the saturation state while inhaling different FDs was compared among the three groups. After the research procedures had been completed and Fet was sufficient, the surgeons were permitted to begin the operation.
The differences in nVERT during the saturation states were calculated and compared among the three groups inhaling different FDs, based on the following formula: nVERT = (FI − Fet) × MV if the dead space (consisting of anatomical and endotracheal catheter dead space) was not considered.
Statistical analyses
All data were presented as mean ± SD. All statistical analyses were performed using the SPSS® statistical software package, version 16.0 (SPSS Inc., Chicago, IL, USA) for Windows®. In study 1, univariate analysis of variance was used to analyse changes in FI/FD while FGF/MV = 0.2, 0.3, 0.4 and 1.0 at the same timepoints from 1–4 min (the duration that it took for FI/FD = 1 at an FGF/MV = 1.0) and while FGF/MV = 0.2, 0.3 and 0.4 at the same timepoints from 1–10 min. Semilogarithmic transformation was used to change half-parabola lines into straight lines and the slopes of the four new straight lines (S1.0, S0.4, S0.3, S0.2) were compared using coefficient of regression. A P-value <0.05 was considered statistically significant.
In study 2, analysis of variance (ANOVA) for repeated measures was used to analyse changes over time. ANOVA was also used to analyse changes in FI in the three study groups, and different FIs within a group. The ΔFI during the saturation state, while patients were inhaling different FDs, was compared among the three groups. Differences in nVERT during the saturation states were also calculated and compared among the three groups, while inhaling different FDs.
Results
Study 1
General demographic characteristics of patients scheduled to undergo surgery, randomized to one of four treatment groups in study 1 (n = 60).

Data presented as mean ± SD.
There were no significant differences in age, body weight or sex among the four groups.
The FI/FD at 0–10 min of the four treatment groups are shown in Table 2 and Figure 1. When FGF/MV was low (0.2) or high (0.3, 0.4), FI did not reach FD within 10 min. As shown in Table 2, the FI/FD at 1–4 min of FGF/MV = 1.0 (group D) was significantly higher than when FGF/MV = 0.4, 0.3 or 0.2 (P < 0.05, all comparisons). The FI/FD at 1–10 min of FGF/MV = 0.4 was significantly higher than when FGF/MV = 0.2 or 0.3 (P < 0.05, all comparisons). The FI/FD at 3–10 min of FGF/MV = 0.3 was significantly higher than when FGF/MV = 0.2 (P < 0.05, all comparisons). As shown in Figure 1, all four curves were half-parabolas and semilogarithmic transformation was used to change them into straight lines. The slopes of the straight lines were then compared. There were significant differences between S1.0 compared with S0.4 (P = 0.045), S0.3 (P = 0.037) and S0.2 (P = 0.011), and between S0.2 and S0.4 (P = 0.032), thereby demonstrating indirectly that there was a positive relationship between FI/FD and FGF/MV.
Changes in the ratio of the fraction of inspired sevoflurane (FI) to the delivered concentration (FD) of sevoflurane at 1–10 min after mechanical ventilation commenced, following increases in the ratio of the fresh gas flow (FGF) to min volume (MV), in patients scheduled to undergo surgery and randomized to one of four treatment groups in study 1 (n = 60). FGF/MV of groups A, B, C and D was set to 0.2 (1.0 l/min), 0.3 (1.5 l/min), 0.4 (2.0 l/min) and 1.0 (5.0 l/min), respectively. Statistically significant findings are shown on Table 2 and described in the text. The ratio of the fraction of inspired sevoflurane (FI) to the delivered concentration (FD) of sevoflurane at 1–10 min after mechanical ventilation commenced in patients scheduled to undergo surgery, randomized to one of four treatment groups in study 1 (n = 60). Data presented as mean ± SD. P < 0.05 compared with FGF/MV = 0.2 at the same timepoint (1–10 min); univariate analysis of variance (ANOVA). P < 0.05 compared with different FGF/MV (0.3, 0.2) at the same timepoint (1–10 min); univariate ANOVA. P < 0.05 compared with different FGF/MV (0.4, 0.3, 0.2) at the same time-point (1, 2, 3, 4 min); univariate ANOVA. When FGF/MV was 1.0, FI = FD within 5 min, but when FGF/MV was low (0.2) or high (0.3, 0.4), FI did not reach FD within 10 min. FGF, fresh gas flow; MV, min volume.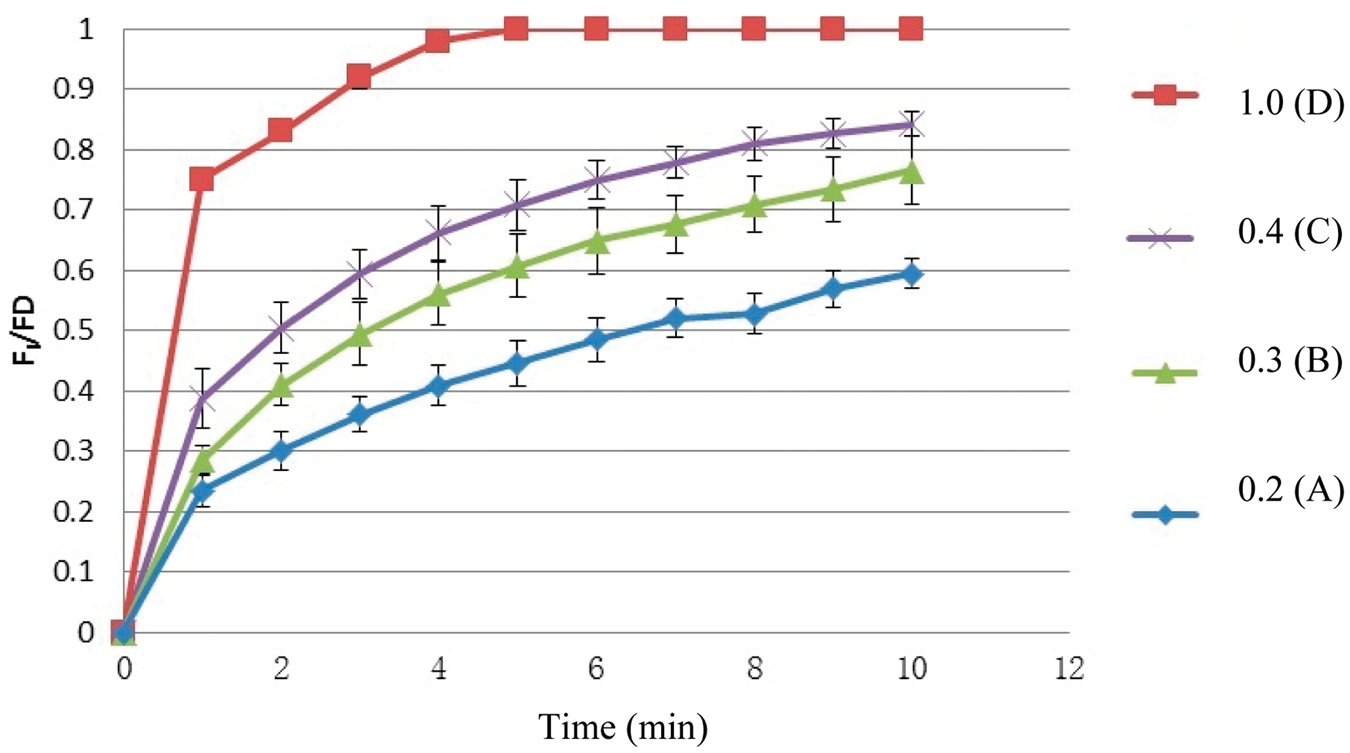

Time taken to reach the state where the fraction of inspired sevoflurane (FI) was equal to the delivered concentration (FD) of sevoflurane (FI = FD) and the time taken to reach maximum fraction of end tidal sevoflurane (Fet) in patients scheduled to undergo surgery who were randomized to group D (fresh flow gas/min volume = 1.0 [5.0 l/min]) in study 1 (n = 15).

Data presented as mean ± SD.
Study 2
General demographic characteristics of patients scheduled to undergo surgery, randomized to one of three treatment groups in study 2 (n = 60).

Data presented as mean ± SD.
There were no significant differences in age, body weight or sex among the three groups.
The difference (ΔF; %vol) between the fraction of inspired sevoflurane (FI) and the maximum fraction of end tidal sevoflurane (Fet) during the saturation state in patients scheduled to undergo surgery, randomized to one of three treatment groups in study 2 (n = 60), when inhaling different delivered concentrations (FD) of sevoflurane.

Data presented as mean ± SD.
P < 0.05 compared with 2.2% vol at the same tidal volume; analysis of variance for repeated measures.
P < 0.05 compared with group I at the same inhalation FD; analysis of variance for repeated measures.
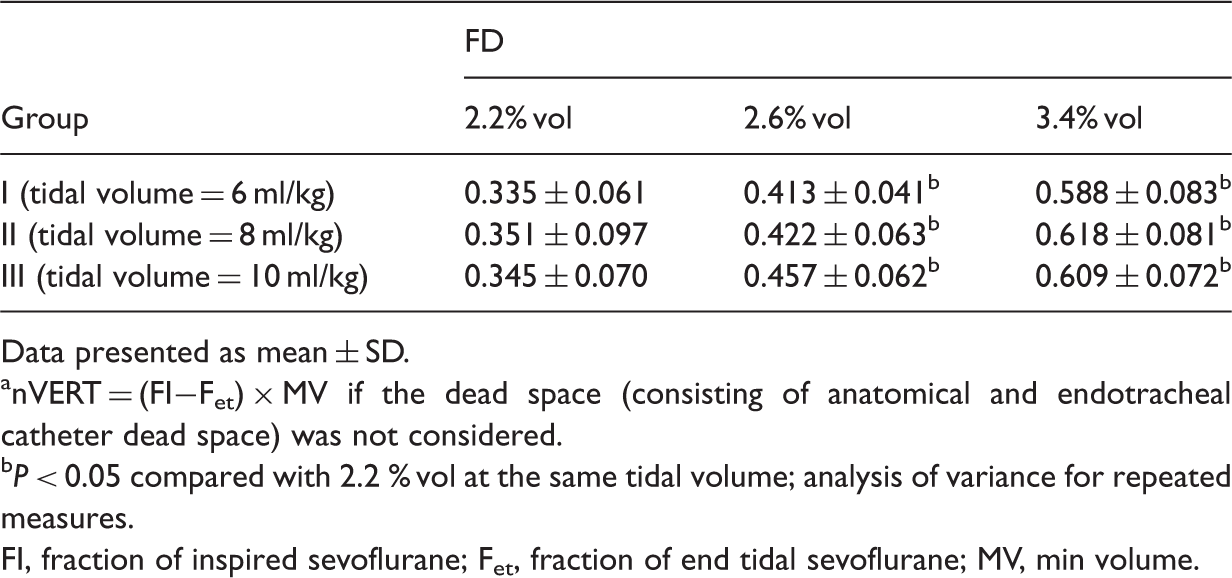
Volume of ejected sevoflurane through the nonrespiratory tract route (nVERT) a during the saturation state in patients scheduled to undergo surgery, were randomized to one of three treatment groups in study 2 (n = 60) when inhaling different delivered concentrations (FD) of sevoflurane.
Data presented as mean ± SD.
nVERT = (FI−Fet) × MV if the dead space (consisting of anatomical and endotracheal catheter dead space) was not considered.
P < 0.05 compared with 2.2 % vol at the same tidal volume; analysis of variance for repeated measures.
FI, fraction of inspired sevoflurane; Fet, fraction of end tidal sevoflurane; MV, min volume.
Discussion
The depth of sevoflurane inhalation anaesthesia is related to the fractional concentration in brain tissue (Fb), which is reflected by Fv and Fet. 1 It is important to determine how to acquire a sufficient depth of general anaesthesia rapidly, by increasing Fet to the expected value. The first step is to increase FI, because FA, Fa, Ft, Fv and Fet will increase quickly only if FI is increased. The increase in FI/FD is related to MV, FGF/MV, inhalation time (determined by I : E), RR, the properties of the gaseous anaesthetic agents, the state of the patient’s respiratory and cardiovascular systems, 8 the patient’s body temperature and the atmospheric pressure.
In this current study, when the volume control mode of a semiclosed anaesthesia machine for mechanical ventilation was used, FI = FD × FGF/BR × TV + Fet(TV − FGF/BR)/TV = Fet + (FD − Fet)FGF/MV. Based on this formula, it is clear that FI is always less than FD, because Fet is always less than FD. Additionally, FI will approach FD as FGF/MV and time increase. When FGF = MV, FI will go up to (and stabilize at) FD because the exhaled TV is not part of the next inhaled TV after the circuit is filled with the FD of sevoflurane gas, provided that the atmospheric pressure and the temperature difference between the patient’s body and the operating room are all constant. All of the inhaled sevoflurane is equal to the sum of the volume that is dissolved in blood 9 and tissue fluid, bound with proteins in plasma and tissue fluid, metabolized by the liver, ejected by the kidneys,10,11 shed through blood loss and dispersed through the raw operating surface and skin. Once FI is equal to FD and stable, FA, Fa and Ft will be stable when the volume of sevoflurane ejected through the nonrespiratory tract route (i.e. nVERT) approaches its maximum. Then, Fet will reach its maximum and sevoflurane will reach a saturation state. If FD is increased, a new saturation state will be reached, several min later.
The results of study 1 showed that FI did not reach FD within 10 min when FGF was set at 1.0 l/min (FGF/MV = 0.2), 1.5 l/min (FGF/MV = 0.3) or 2.0 l/min (FGF/MV = 0.4), but there was a significant relationship between FI/FD and FGF/MV. Increases in FI/FD were significantly related to increases in FGF/MV. With higher FGF/MV, FI/FD increased faster and FI reached FD sooner. When FGF = MV, FI increased to 2.2% vol (FD) in a mean ± SD of 250.1 ± 32.9 s and Fet achieved and stabilized at its maximum in a mean ± SD of 483.1 ± 43.6 s. A new saturation state was achieved within 3 min when FD was subsequently increased. When FGF = MV, the exhaled TV is almost completely excluded from taking part in the next inhaled TV. Therefore, FI depends on the speed with which sevoflurane gas fills the circuit at the initiation of anaesthesia. In group D in study 1, the time it took FI to reach FD was actually the time it took the sevoflurane gas to fill the circuit of the anaesthesia machine with an FGF of 5.0 l/min. When FGF > MV, redundant sevoflurane gas will not enter the circuit and will be eliminated as end gas.
At the initiation of sevoflurane anaesthesia, increases in Fet are determined by FI, I:E, MV (TV × RR), FGF/MV, and so on. If the anaesthesiologist wants to achieve a sufficient depth of general anaesthesia as quickly as possible, a greater MV can be set, letting FGF = MV. This will cause the FD of sevoflurane gas to fill the circuit of the anaesthesia machine rapidly, prevent the exhaled TV from taking part in the next inhaled TV, make FI rapidly increase and stabilize at FD and produce a longer inhalation time, in order to ensure that sevoflurane is absorbed more and exhaled less. Once a saturation state is reached at the desired FD, a sufficient and stable depth of anaesthesia will be achieved.
The depth of sevoflurane anaesthesia is relevant to Ft of the brain. Ft is determined by Fb, FI, FA, FD, MV, the state of patient’s circulatory system, properties of the gaseous anaesthetic agents, body temperature, and so on. At the initiation of anaesthesia, FI should be made to reach FD, and Fet should go up to (and stabilize) at its maximum as soon as possible. Usually a high FD and a low flow of fresh oxygen are set, to achieve this objective. However, the most significant limitation of low-flow anaesthesia is that the monitoring parameters, including FI and Fet, are not stable. If the anaesthesiologist uses the volume control mode of a semiclosed anaesthesia machine for ventilation, FI = Fet(TV − FGF/RR)/TV + FD × FGF/RR × TV = Fet + (FD − Fet)FGF/MV, therefore, when FGF = MV, FI = FD. FI will go up to and stabilize at FD after the circuit of the anaesthesia machine is filled with the inhaled gas, several min after the beginning of mechanical ventilation. Then, FA, Fb and Fet will increase to the highest possible value in the shortest time, which may represent a saturation state at that FD. When FD is increased, a new saturation state of sevoflurane anaesthesia will be achieved, several min later.
The results of study 2 showed that ΔF during the saturation state increases as FD increases, if MV is fixed. This may be because Ft increases after FD, FI and Fb increase. Therefore, the diffusion of sevoflurane from tissues to the environment must be accelerated, because the volume ejected by the liver and kidneys is definite. ΔF decreases gradually as MV increases, if FD is fixed. This may be because FI, FA, Fb and Ft are all stable during the saturation state, and the diffusion of sevoflurane from the tissues to the environment is invariable. Though increasing MV can augment the inhaled volume of sevoflurane, the exhaled volume is also increased as Fet and MV are increased. Therefore, nVERT increases as FD increases when MV is fixed, but is not subject to change when MV changes but FD is fixed.
The inhaled volume (IV) equals the volume of ejected sevoflurane through the respiratory tract (VERT) + nVERT. During the saturation state, both IV and VERT are stable, so nVERT is also stable. Among the factors that can affect nVERT, the amount of sevoflurane physically dissolved in blood and tissue fluid is invariable, because FI, FA and Fa are constant, the volume of sevoflurane bound to plasma proteins, metabolized in the liver and ejected by the kidneys cannot grow infinitely, and the volume in blood loss is lessened. Changes in the volume of diffusion from tissues to the environment may be important for changes in nVERT. As the partial pressure of sevoflurane increases in tissue fluid, the velocity of diffusion through the skin and the surgical wound site also increases. Therefore, it is likely that the most important factor affecting nVERT is FD, which determines FA, Fa, Ft, Fv and Fet during the saturation state of sevoflurane anaesthesia.
The results of study 2 suggest that a saturation state of sevoflurane may exist when ΔF is between 0.3–0.5% vol, if the settings are FGF = MV and TV = 8 ml/kg. The clinical significance of this research is that the expected Fet + 0.3–0.5% vol is the FD that should be set. For example, if the anaesthesiologist expects Fet = 2.0% vol, then he/she should set FD = 2.4% vol, FGF = MV and TV = 8 ml/kg. Fet will go up to and stabilize at 2.0% vol, several min after mechanically ventilating in volume control mode.
In addition, study 2 demonstrated that the nVERT of sevoflurane during the saturation state of the study participants was 0.30–0.35 ml/kg per min (gas). When inhaling 2.6% vol sevoflurane and MV = FGF (RR = 10 BPM, TV = 8 ml/kg), the nVERT of sevoflurane/total inhaled sevoflurane was 15–16%.
In conclusion, the results of study 1 demonstrate that the FI/FD of sevoflurane is positively related to FGF/MV. With higher set FGF/MV, FI/FD increases faster and FI reaches FD sooner. When FGF = MV, a saturation state is established, so that FI reaches FD (2.2% vol) in 250.1 s and Fet reaches (and stabilizes at) its maximum in 483.1 s. A new saturation state is likewise reached within several min when FD is increased. Study 2 demonstrates that ΔF during the saturation state is relevant to MV and FD. When FD is fixed, ΔF decreases gradually, as MV increases. ΔF increases as FD increases, when MV is fixed. nVERT during the saturation state is relevant to FD and increases as FD increases, but nVERT is not dependent on changes in MV. After the saturation state is achieved, it is possible to determine whether low FGF can be used to reduce the consumption of sevoflurane.
Footnotes
Declaration of conflicting interest
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.