
Abstract
Objectives
A prospective, randomized, double-blind study using bispectral index values to objectively quantify the sedative effect of high spinal anaesthesia in patients stratified according to age, and to determine whether sedative drugs are associated with additional adverse respiratory and haemodynamic effects in older patients.
Methods
Patients who were electively scheduled for lower limb or abdominal surgery were recruited and allocated into one of three groups according to their age and whether midazolam and fentanyl were used: younger (20–40 years); and older (61–80 years) with or without midazolam and fentanyl intravenous infusion.
Results
The study recruited a total of 90 patients (n = 30 per group). Intraoperative bispectral index values were significantly lower than preoperative values in all groups. Patients in the older age group had significantly lower intraoperative bispectral index values than younger patients. Older patients were significantly more likely to experience respiratory depression (arterial oxyhaemoglobin saturation <90%) than younger patients.
Conclusions
The sedative effect of high spinal anaesthesia is greater in older patients than in younger patients, with an increase in respiratory instability.
Introduction
Sedation induces a comfortable and relaxed state in patients undergoing local or regional anaesthesia. It also serves to lessen anxiety by limiting awareness of unpleasant procedures, while maintaining cardiovascular stability and sufficient alertness for an adequate response to physical or verbal stimulation.1,2 Anaesthetists are responsible for maintaining adequate sedation while avoiding complications such as respiratory depression, bradycardia and changes in blood pressure.
Spinal anaesthesia is known to have a sedative effect,3–5 with high spinal anaesthesia often associated with decreased alertness. The likelihood and degree of drowsiness increase as the spinal block level rises: a phenomenon that has several possible explanations.6–8 The extent of spinal anaesthesia has been shown to influence the depth of sedation, assessed via bispectral index (BIS). 6 BIS quantifies the hypnotic state during sedation and anaesthesia, and is based on continuous noninvasive electroencephalography.9,10
Ageing is associated with many physiological changes, but the consequence of age on the sedative effects of high spinal anaesthesia has not been thoroughly investigated. Studies examining the degree of sedation provided by additive intravenous drugs in patients undergoing spinal anaesthesia either had small cohorts or used subjective evaluation methods.7,8 To our knowledge, there have been no studies regarding the use of midazolam or fentanyl in high spinal anaesthesia, despite the frequent clinical use of these medications.
The aim of the present study was to objectively quantify the sedative, respiratory and haemodynamic effects of high spinal anaesthesia in patients stratified according to age. In addition, we investigated whether midazolam and fentanyl were associated with additional adverse effects in older patients during high spinal anaesthesia.
Subjects and methods
Study population
This prospective, randomized, double-blind study recruited patients aged 21–40 or 61–80 years, with American Society of Anesthesiologists physical status I or II, 11 scheduled to undergo elective lower limb or abdominal surgery using high spinal anaesthesia at Kangwon National University Hospital, Chuncheon, Republic of Korea between August 2011 and August 2012. Exclusion criteria were: use of any opioid or sedative medication in the week prior to surgery; history of alcohol or drug abuse; history of any psychiatric or neurological abnormality; refusal of spinal anaesthesia.
Patients were stratified into two groups according to age: younger (group Y; aged 20–40 years); older (aged 61–80 years). Patients in the older group were allocated to one of two equally-sized groups using a randomization table: those receiving no additional medication (group O); those receiving 2 mg midazolam and 50 µg fentanyl intravenous injection (group OMF). Medical personnel involved in patient care and evaluation, and all study participants, were blinded to group randomization in the older group and to the age-related criteria for group assignment.
The study was designed using Consolidated Standards of Reporting Trials guidelines, 12 and was conducted according to Good Clinical Practice guidelines and the Declaration of Helsinki.13,14 The institutional review board of Kangwon National University Hospital, School of Medicine, Kangwon National University (Chuncheon, Republic of Korea) approved the protocol. All participants provided written informed consent.
Anaesthesia
No premedication was administered, due to sedative and cardiovascular system effects. Routine physiological monitoring included noninvasive arterial blood pressure, heart rate and arterial oxyhaemoglobin saturation (SpO2), as well as electrocardiogram examination. Continuous BIS monitoring was planned with high spinal anaesthesia at a level above T6. Before administering spinal anaesthesia, BIS electrodes (Aspect Medical Systems, Norwood, MA, USA) were placed on the frontotemporal regions of the cranium, as recommended by the manufacturer, and were connected to an electroencephalogram monitor (A-3000, version 2.1, Aspect Medical Systems) for BIS measurement. The smoothing rate was set at 15 s. To reduce electrode impedance, the skin over the forehead was cleaned with an alcohol-impregnated skin wipe. The BIS monitor waveform, signal quality and other interferences were observed continuously by one of the investigators (D.H.) to ensure accurate measurements. BIS was observed once per min for 5 min in the operating room before anaesthesia and the mean value was recorded as the baseline for each patient. BIS was observed continuously during the first 60 min of anaesthesia and recorded once per min. The operating room was warmed, to prevent increased electromyogram activity resulting from the patient shivering. All patients were provided with earplugs to block noise, and breathed normal room air.
Patients were moved into the lateral decubitus position. Subarachnoid puncture was performed with a 25-gauge Sprotte needle (Tae Chang Industrial Co. Ltd., Chung-Nam, Republic of Korea) at the lumbar 3–4 or 4–5 space, using the paramedian approach, and 0.5% hyperbaric bupivacaine (AstraZeneca, Osaka, Japan) was injected into the subarachnoid space (15 mg bupivacaine in group Y; 12 mg in groups O/OMF). Patients were moved to a supine position immediately after injection. The effect of spinal anaesthesia is known to appear 15–20 min after administration,5,6 and the dermatomal level of sensory blockade was assessed using an ice-cold alcohol-immersed sponge 15 min (the starting point of sensory blockade) and 60 min (the endpoint of BIS measurement) after injection. Patients with sensory block levels of T6 and above were defined as having high spinal anaesthesia. Patients in the OMF group received 2 mg midazolam and 50 µg fentanyl intravenous injection 20 min after spinal anaesthesia. Patients with inadequate spinal anaesthesia and those with uncontrollable anxiety were excluded from analysis.
Study definitions
Blood pressure was recorded every 3 min for 60 min, and mean blood pressure was calculated as (2 × systolic blood pressure + diastolic blood pressure)/3. Hypotension was defined as a decrease of >20% in mean blood pressure from baseline, and was treated with 5 mg ephedrine bolus. Bradycardia was defined as a heart rate of <60 beats per min (bpm), and was treated with 0.5 mg atropine. Respiratory depression (SpO2 <90%) was treated with 100% oxygen, administered by face mask via the anaesthesia machine.
Statistical analyses
Sample size was calculated on the basis of a pilot study that had five patients in each group. The primary outcome for power analysis was the lowest intraoperative BIS value. A priori power assessment was performed to detect any difference of ≥10 in BIS. Using a desired power of 0.8 and an α-level of 0.05, and in view of the fact that some participants might drop out, it was determined that 30 patients should be enrolled in each group. Data from the patients in the pilot study were incorporated into the present study.
Data were presented as mean ± SD. Between-group comparisons of demographic data were made using one-way analysis of variance (ANOVA). BIS data were analysed by repeated ANOVA for serial comparisons and ANOVA for within- and between-group differences, followed by Scheffe’s test to adjust significance levels. Haemodynamic and respiratory data were analysed by the χ2-test. A P-value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS® software, version 19.0 (IBM Corporation, Somers, NY, USA) for Windows®.
Results
Demographic and clinical characteristics of patients undergoing elective abdominal or lower limb surgery, included in a study to evaluate the sedative effects of high spinal anaesthesia, stratified according to age and sedative use (n = 85.

Data presented as mean ± SD or n (%) of patients.
Group Y, aged 20–40 years; Group O, aged 61–80 years; Group OMF, aged 61–80 years receiving midazolam 2 mg and 50 µg fentanyl intravenous infusion.
P < 0.05; one-way analysis of variance followed by Scheffe’s post hoc test.
Pre- and intraoperative bispectral index (BIS) parameters in patients undergoing elective abdominal or lower limb surgery under high spinal anaesthesia, stratified according to age and sedative use (n = 85.

Data presented as mean ± SD or n (%) of patients.
Group Y, aged 20–40 years; Group O, aged 61–80 years; Group OMF, aged 61–80 years receiving midazolam 2 mg and 50 µg fentanyl intravenous infusion.
P < 0.05 versus preoperative value; bP < 0.05 versus group Y; one-way analysis of variance followed by Scheffe’s post hoc test.
Haemodynamic and respiratory complications observed in patients undergoing elective abdominal or lower limb surgery under high spinal anaesthesia, stratified according to age and sedative use (n = 85.
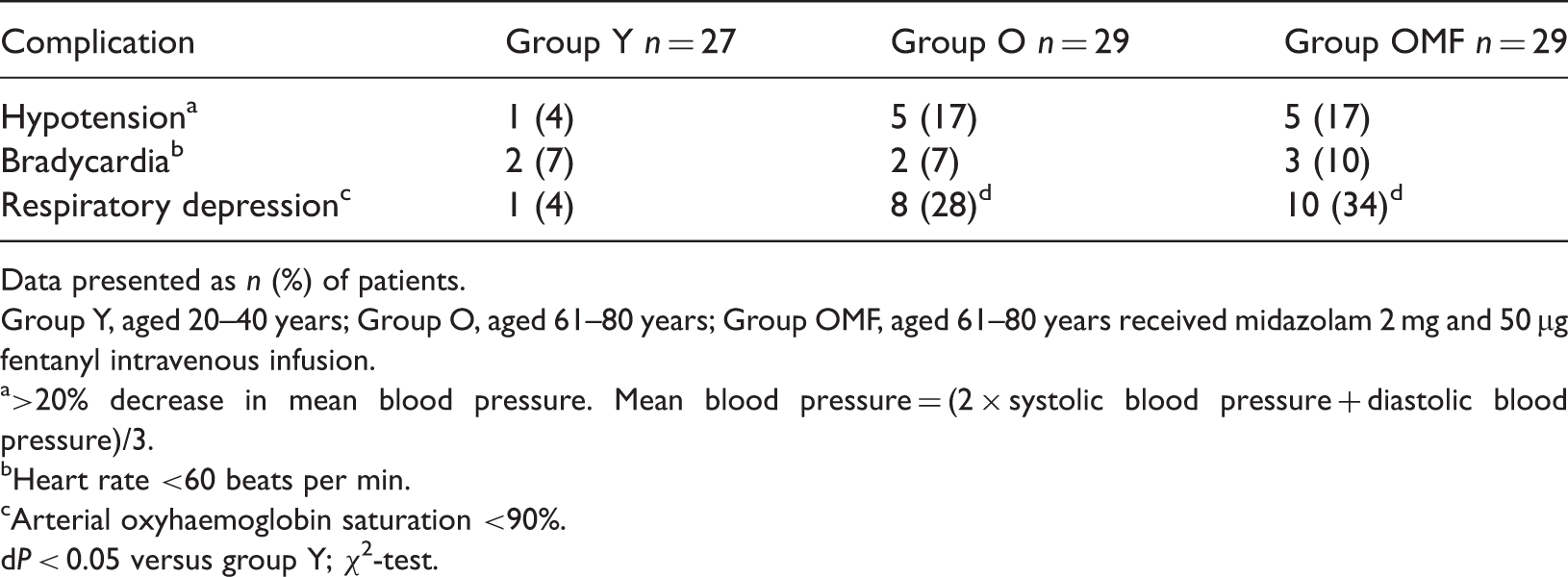
Data presented as n (%) of patients.
Group Y, aged 20–40 years; Group O, aged 61–80 years; Group OMF, aged 61–80 years received midazolam 2 mg and 50 µg fentanyl intravenous infusion.
>20% decrease in mean blood pressure. Mean blood pressure = (2 × systolic blood pressure + diastolic blood pressure)/3.
Heart rate <60 beats per min.
Arterial oxyhaemoglobin saturation <90%.
P < 0.05 versus group Y; χ2-test.
Discussion
Spinal anaesthesia resulted in significant decreases in BIS, compared with preoperative levels in all patient groups, in the present study. The lowest intraoperative BIS values were significantly lower in older patients (with or without midazolam and fentanyl administration) than in younger patients. In addition, older patients were significantly more likely to exhibit respiratory depression during anaesthesia.
Sedation is related to the spread of spinal sensory block.6,15 Patients who are administered high spinal anaesthesia occasionally fall asleep, and this type of drowsiness increases in intensity with increasing levels of spinal blockade.8,15 Patients undergoing high spinal anaesthesia became sedated in the present study. The degree of sedation resulting from spinal anaesthesia may have important clinical implications. General anaesthesia frequently occurs in elderly patients during sedation and spinal anaesthesia. 16 It has been reported that major anaesthetic mishaps occur during spinal anaesthesia, with some patients becoming sedated to the extent that they are unable to respond to verbal commands. 17 BIS monitoring has been used to minimize the complications that may occur during sedation and to evaluate the level of sedation using objective measures (instead of conventional, subjective measures such as the modified observer’s assessment of alertness and sedation).3,9,18,19
The BIS is a widely used quantitative parameter for evaluating anaesthesia and sedation levels, and provides the level of sedation as a constant readout after analysis of single-channel EEG findings. BIS values are as follows: 95–100, awake; 70–95, light to moderate sedation; 60–70, deep sedation with low probability of explicit recall; 40–60, general anaesthesia with low probability of consciousness; <40, deep hypnotic state.10,20 The present study used BIS to examine the sedative effects of high spinal anaesthesia in patients stratified according to age, and found significantly lower intraoperative BIS levels in older patients than in younger patients. Other research reported that age-related decreases in BIS in patients undergoing midazolam induced sedation, but this study did not include patients undergoing high spinal anaesthesia. 21 Studies have indicated the mean lowest intraoperative BIS values to be 83–87 in young patients,22,23 which is consistent with the findings of the present study (in which younger patients had a mean lowest BIS of 85). High spinal anaesthesia has been associated with decreased intraoperative BIS compared with preoperative values in older patients. 4 The mean lowest intraoperative BIS was less than the preoperative value across both age groups, in the present study.
Patients remain concerned regarding the anxiety, discomfort and stress associated with being awake during surgery. Sedation with propofol, midazolam or remifentanil has become a popular method to reduce fear and stress, and to make patients feel comfortable,2,9 in particular during surgery under spinal anaesthesia.8,9 Individual variability in drug–dose response results in some patients becoming more deeply sedated than expected, leading to serious complications including apnoea and hypoxia.16,17 Patients under high spinal anaesthesia, particularly older individuals, are more sensitive to sedative drugs. 8 Studies have indicated that elderly patients under spinal anaesthesia can become sedated even when no sedative drugs are administered.4,5 Respiratory depression was significantly more common in older patients in the present study, but the use of midazolam and fentanyl was not associated with an increased risk of adverse effects compared with high spinal anaesthesia alone.
Others have reported decreased blood pressure and stroke volume during high spinal anaesthesia in elderly patients. 4 Although hypotension was observed in one patient (4%) in group Y, five patients (17%) in group O and five patients (17%) patients in group OMF in the present study, there were no statistically significant between-group differences in the incidence of hypotension.
The present study had several limitations. First, there is debate about the accuracy of BIS,3,4 and there is no gold standard for the clinical assessment of sedation depth. This lack of a standard makes it difficult to definitively evaluate the accuracy and specificity of the BIS algorithm in the operating room. The present study therefore focused on the objective change in BIS values, avoiding the use of subjective evaluations of sedation levels. Others have shown temporal correlations between BIS and conventional sedation measures,24,25 suggesting that BIS monitoring is useful for evaluating sedation.4,24 Both the depth of sedation and BIS values have been shown to correlate with the level of spinal block.6,15
Secondly, BIS is sensitive to internal or external patient circumstances and can be affected by abrupt arousal, movement, coughing or noise in patients with light or no additional sedation.26,27 Attempts were made to minimize the effect of the surrounding environment on BIS values by warming the operating room (to prevent an increase in electromyogram activity due to shivering) and by blocking noise with ear plugs. It is, however, not possible to state that patients were totally free from the effects of environmental factors. Numerical sedation scales, including the Observer’s Assessment of Alertness/Sedation, Ramsey Scale, Sedation–Agitation Scale and Motor Activity Assessment Scale,2,3,28 exhibit large variability, but bispectral analysis improves the predictive power of simple spectral analysis in distinguishing sedation levels.24,25 Thirdly, the type of surgery may affect BIS values. In order to minimize this, all patients enrolled in the present study were electively scheduled for lower limb or abdominal surgery, and all surgeries were performed in the supine position. These operations did not use noisy instruments and did not involve body movement during the period of BIS measurement.
In conclusion, we found that high spinal anaesthesia significantly decreases BIS compared with preoperative BIS values, and that the sedative effect is greater in older patients (aged 61–80 years) than in younger patients (20–40 years). Older patients were more likely to experience respiratory depression during high spinal anaesthesia, but the use of midazolam and fentanyl did not cause additional adverse effects in such patients. These findings suggest that patients undergoing high spinal anaesthesia must be carefully evaluated according to their age, as well as their respiratory and haemodynamic status. The administration of small amounts of sedatives in older patients during high spinal anaesthesia does not have any additional impact on their status.
Footnotes
Declaration of conflicting interest
The Authors declare that there are no conflicts of interest
Funding
This study was supported by a 2011 research grant from Kangwon National University, Republic of Korea.