
Abstract
Objectives
To assess nasal cycle, nasal mucosal pH and mucociliary clearance time in patients with Parkinson’s disease and healthy control subjects.
Methods
Patients with idiopathic Parkinson’s disease and healthy control subjects were recruited. Presence of the nasal cycle, nasal mucosa pH and mucociliary clearance time were investigated in all participants.
Results
The study included 27 patients and 24 control subjects. The nasal cycle was present in significantly fewer patients than controls. Nasal pH and mucociliary clearance time were significantly higher in patients than in controls.
Conclusions
Parkinson’s disease is associated with alterations in nasal cycle, nasal mucosa pH and mucociliary clearance time. Measurements of these nasal parameters may be useful for the early diagnosis of autonomic and olfactory dysfunction in Parkinson’s disease.
Introduction
The motor symptoms of Parkinson’s disease are well recognized. Around 62% of patients with Parkinson’s disease experience nonmotor symptoms, with autonomic nervous dysfunction in particular being responsible for substantial disability and effects on health-related quality of life.1–3 Nonmotor symptoms can appear at any stage of Parkinson’s disease.4,5 Symptoms including olfactory dysfunction, REM sleep behaviour disorder, constipation and depression can occur before a diagnosis has been made, and may therefore be useful for determining those patients at risk of developing Parkinson’s disease.1,2,4,5
The nasal cycle is the spontaneously repeating series of reciprocal vasomotor changes that occur within the nasal mucosa, in order to moisturize and warm respiratory air;6–8 this cycle is regulated by the autonomic nervous system. Unilateral sympathetic activity causes vasoconstriction and decongestion in one nostril, whereas simultaneous parasympathetic activity causes vasodilatation and congestion in the other. 9 Both nostrils are therefore able to be congested alternately without any change to total nasal resistance. The ideal nasal cycle involves identical periods with similar airflow and volume changes in each nostril, with the left and right sides of the nose being 180° out of phase with one another. 10 The duration of the nasal cycle varies between 30 min and 6 h, and is present in 13–80% of adults, 8 although this frequency decreases with advancing age, due to mucosal atrophy. 11
Ciliary activity in the respiratory tract depends on temperature, pH, osmotic pressure, infections, surgery, and genetic and iatrogenic factors. 12 Abnormal ciliary function may be caused by chronic sepsis of the upper or lower airways, resulting in serious respiratory tract infections in sensitive patients (such as those with Parkinson’s disease or chronic obstructive pulmonary disease).13–15 The ability of respiratory mucosal surfaces to remove foreign particles and to keep these surfaces moist and fresh depends on both effective ciliary activity and regular regeneration of airway fluids, 16 together known as mucociliary activity. Mucociliary clearance can be assessed by measuring the elimination time of inhaled aerosols 17 or by the saccharin test. 18
The aim of the present study was to assess the nasal cycle, nasal mucosal pH and mucociliary clearance time in patients with Parkinson’s disease and healthy control subjects.
Patients and methods
Study population
The study recruited patients with idiopathic Parkinson’s disease attending the neurology clinic of Ataturk University Faculty of Medicine, between April 2008 and October 2009. Diagnosis of Parkinson’s disease was confirmed by ≥3 years of clinical observation, clinically significant improvement in symptoms with levodopa treatment and absence of demonstrable atrophy of the brain stem or cerebellum on magnetic resonance imaging. Disease severity was assessed using the Hoehn–Yahr modified staging scale 19 and the motor section III of the Unified Parkinson's Disease Rating Scale. 20 Patients with lower or upper respiratory tract infections or chronic obstructive pulmonary disease were excluded from the study. Age- and sex-matched control subjects were recruited from healthy people attending the neurology clinic of Ataturk University Faculty of Medicine for routine screening. All patients and control subjects underwent a physical examination including ear, nose and throat examination, and medical history.
The study was approved by the Human Ethics Committee of the Faculty of Medicine, Ataturk University. All participants provided written informed consent.
Nasal cycle
Nasal airway resistance was assessed in all participants using a Rhino 4000 rhinomanomer (Homoth Medical Electronics, Hamburg, Germany) at a pressure of 150 Pa. Resistance was measured at 20-min intervals for 6 h, without the use of decongestants and with the participant in a seated position at constant room temperature and humidity.
Mucociliary clearance time
Mucociliary clearance time was assessed using the saccharin test, 18 performed at room temperature with the participant seated and with his/her head in an upright position. The participant was asked to clear their nasal secretions, then a 1-mm diameter saccharin tablet was placed into one nasal cavity, 1 cm posterior to the anterior border of the medial surface of the inferior turbinate. Participants were instructed to maintain their initial position, were not allowed to breathe deeply, talk, cough, sneeze or sniff, and were instructed to swallow as infrequently as possible. The time taken until tasting a sweet flavour in the mouth (to the nearest 30 s) was recorded as the clearance time. The mean normal saccharin clearance time is 9–25 min with >25 min considered abnormal. 18
Nasal mucosal pH
The pH of nasal mucosa was determined using colour-fixed pH indicator sticks (Macherey–Nagel, Düren, Germany) applied 1 cm along the medial aspect of the inferior turbinate and 1 cm along the posterior of the maxillary spine, on both sides of the nasal septum. All readings were taken at the same time of day and were repeated twice at 5-min intervals, the mean value was then recorded.
Statistical analyses
Categorical variables were presented as percentages and continuous variables as mean ± SD. The relationship between nasal parameters and age, sex and duration of disease or medication was studied. Between-group comparisons were made using the paired sample t-test for normally distributed variables and Wilcoxon signed-rank test for non-normally distributed variables. Statistical analyses were performed using SPSS® software, version 15.0 (SPSS Inc., Chicago, IL, USA) for Windows®. A P-value <0.05 was considered statistically significant.
Results
Demographic and clinical characteristics of patients with idiopathic Parkinson’s disease, included in a study investigating the relationship between olfactory dysfunction and Parkinson’s disease severit.
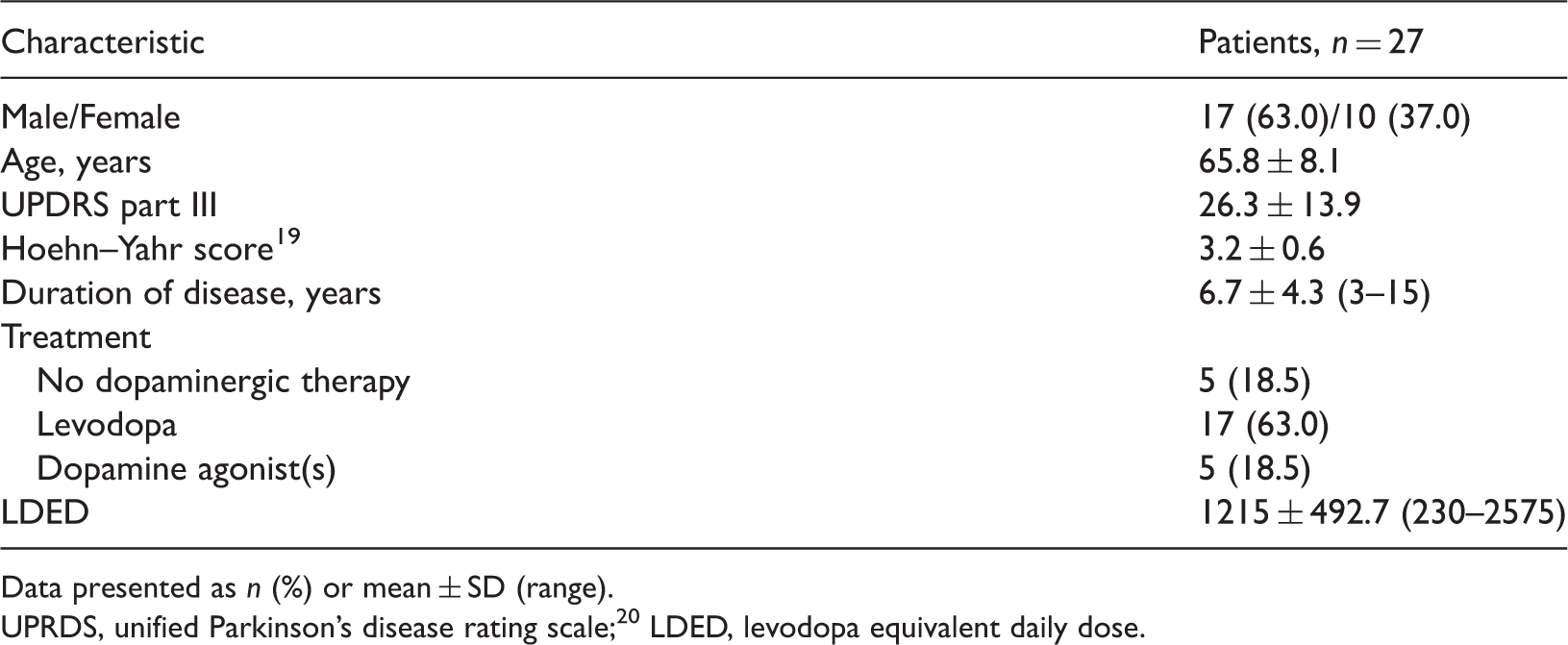
Data presented as n (%) or mean ± SD (range).
UPRDS, unified Parkinson’s disease rating scale; 20 LDED, levodopa equivalent daily dose.
Presence of nasal cycle and mucociliary clearance time, and nasal mucosal pH, in patients with idiopathic Parkinson’s disease and healthy control subject.

Data presented as n (%) or mean ± SD.
P < 0.05, **P < 0.01 vs controls; paired sample t-test.
Discussion
Nonmotor symptoms are observed in the majority of patients with Parkinson’s disease, and include autonomic dysfunction and olfactory dysfunction. These symptoms are a result of the pathological involvement of the neurological system outside the non-nigrostriatal dopaminergic system. 21 Choking can cause aspiration pneumonia (silent aspiration) in patients with Parkinson’s disease, even in the absence of airway irritation. 22 Nasal dysfunction (increased pH and mucociliary clearance time) such as that seen in the present study may be caused by upper or lower respiratory tract infections, or silent aspiration.
Mucociliary clearance time was prolonged and nasal mucosal pH levels were increased in patients with Parkinson’s disease compared with control subjects, in the present study. In addition, the nasal cycle was present in significantly fewer patients than controls. The physiological mechanisms underlying this cycle remain unclear, but the sympathetic nerves that supply the nose are regulated by the hypothalamic and vasomotor areas of the brainstem. 23 The reduced presence of the nasal cycle in patients with Parkinson’s disease observed in the present study suggests that the mechanism controlled by the sympathetic system can exhibit autonomic dysfunction or hypofunction. In normal subjects, airflow through nasal passages is usually asymmetrical, which is often explained as being due to the nasal cycle. The majority of individuals are completely unaware of any changes in nasal airflow because the total resistance to airflow remains relatively constant, due to the reciprocal relationship between the nasal passages. 24 It has been suggested that the nasal cycle may not always be detectable (due to minor variations that are irregular in timing) or not reciprocal between the two sides of the nose.24,25 It is therefore important to define the characteristics of nasal cycle fluctuation and to distinguish them from pathological conditions, especially in clinical practice. The nasal parameters examined in the present study may be useful for determining olfactory dysfunction.
Mucociliary clearance is a key defence mechanism in the upper and lower airways, the impairment of which (both acquired and genetically determined) predisposes an individual to chronic infection of the nose, paranasal sinuses and respiratory tract. 26 The present finding–that mucociliary clearance time is prolonged in patients with Parkinson’s disease–is in accordance with the increased predisposition to lower respiratory infections found in these people, compared with healthy individuals. 27
An intact nasal epithelium is essential for pH maintenance of nasal secretions, with more-alkaline secretions produced when the epithelium is damaged by infective or allergic rhinitis. 28 Nasal pH was significantly more alkaline in patients than in controls, in the present study.
The present study had several limitations. First, the nasal cycle is not detectable in all individuals, and other nasal parameters vary with age.29,30 In addition, these findings may carry more weight if compared with those from patients with other age-related diseases, such as dementia.
In conclusion, the present data indicate alterations in nasal cycle, increased nasal mucosal pH and prolonged mucociliary clearance time in people with Parkinson’s disease. Measurements of these nasal parameters may be useful for the early diagnosis of autonomic and olfactory dysfunction in Parkinson’s disease. The therapeutic value of these nasal parameters in Parkinson’s disease is worthy of further investigation.
Footnotes
Declaration of conflicting interest
The Authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.