
Abstract
Objectives
To investigate the relationship between serum plasma pregnancy-associated plasma protein A (PAPP-A) and coronary plaque characteristics, and their prognostic value for coronary no-reflow after percutaneous coronary intervention (PCI).
Methods
Patients with unstable angina undergoing PCI were divided into a normal reflow group and a no-reflow group after stent deployment. Coronary blood flow was measured angiographically; plaque components were detected by virtual histology intravascular ultrasound. Serum PAPP-A and high-sensitivity C-reactive protein (hsCRP) were measured before PCI. Cardiac troponin T (cTnT) was measured before and 24 h after PCI.
Results
A total of 166 patients with unstable angina undergoing PCI were included: normal reflow group (n = 145) and no-reflow group (n = 21), after stent deployment. Baseline coronary blood flow was similar in the two groups. The no-reflow group had plaques with less-fibrotic tissue and a larger necrotic core, more thin-cap fibroatheromas and plaque ruptures, and higher serum PAPP-A, hsCRP and post-PCI cTnT levels than the normal reflow group. Serum PAPP-A was correlated negatively with plaque fibrotic area and positively with necrotic core area.
Conclusion
High serum PAPP-A and plaque lesions with a large necrotic core are associated with the no-reflow phenomenon after PCI, in patients with unstable angina.
Keywords
Introduction
The phenomenon of coronary no-reflow after percutaneous coronary intervention (PCI) is associated with a poor prognosis.1,2 Appropriate use of distal protection devices can prevent coronary no-reflow after PCI, so prediction before PCI of which lesions are at high risk of no-reflow is of great importance. Studies have shown that lesion morphology and plaque characteristics, detected by integrated backscatter intravascular ultrasound (IB-IVUS) and virtual histology intravascular ultrasound (VH-IVUS), are closely related to no-reflow after PCI.3,4 However, most of these studies were performed in patients with acute myocardial infarction and it is still unclear whether lesion characteristics are predictive of no-reflow after PCI, in patients with unstable angina pectoris.
Pregnancy-associated plasma protein A (PAPP-A) is a member of the metzincin superfamily of metalloproteinases that was originally identified in the serum of pregnant women. 5 It has been demonstrated that PAPP-A is abundantly expressed in both eroded and ruptured atherosclerotic plaques, but is only minimally expressed in stable plaques. 6 In patients with non-ST-elevation acute coronary syndrome, circulating PAPP-A levels were shown to predict medium-term PCI outcomes. 7 However, it is unclear whether PAPP-A levels are related to plaque characteristics and the prediction of no-reflow after PCI, in patients with unstable angina.
The aim of this study was to investigate the relationship between plasma PAPP-A levels and atherosclerotic plaque characteristics, determined using VH-IVUS, and to assess their prognostic value for coronary no-reflow after PCI.
Patients and methods
Patients
Patients with unstable angina pectoris and a single, native, de novo coronary lesion with stenosis >70% on coronary angiography were recruited sequentially from the Department of Cardiology, First Affiliated Hospital, Zhengzhou University, Zhengzhou, China, between September 2010 and November 2011. Exclusion criteria were: ST-segment elevation acute myocardial infarction; the need for multivessel or multilesion PCI; a prior PCI procedure; pre-PCI cardiac troponin T (cTnT) elevation >0.08 ng/ml; treatment with atheroablative or distal protection devices; congestive heart failure; renal insufficiency with a baseline serum creatinine level of >133 µmol/l.
The study protocol was approved by the Medical Ethics Committee of Zhengzhou University, Zhengzhou, China. The procedures used were in accordance with the ethical standards of the Medical Ethics Committee of Zhengzhou University and the Helsinki Declaration of 1975 (as revised in 1983). Written informed consent was obtained from all study participants.
Coronary angiography and VH-IVUS
In all patients, coronary angiography was performed using a 5 F Judkins-type catheter via a radial approach. An intravenous bolus injection of 100 IU/kg heparin was given prior to the procedure. A 200 µg intracoronary dose of isosorbide dinitrate was given after the catheter was inserted but before coronary angiography was performed, and a second 200 µg intracoronary dose was given after the IVUS catheter was advanced distal to the lesion and before it was pulled back.
After completion of diagnostic coronary angiography and before any intervention, all patients were evaluated using VH-IVUS. A phased-array, 20 MHz, 3.2 F IVUS catheter (Eagle Eye®, Volcano, Rancho Cordova, CA, USA) was carefully advanced distal to the lesion. It was then pulled back automatically from the distal position at 0.5 mm/s. During pullback, greyscale IVUS was performed with manual infusion of contrast medium and a colour-coded map was constructed using a VH-IVUS data recorder (In-Vision Gold, Volcano); data were stored on DVD for analysis.
Offline analyses of the greyscale and VH-IVUS data were performed using s5™ Imaging System software (Volcano) by two experienced IVUS investigators, according to standards set by the American College of Cardiology.8,9 In the VH-IVUS images, plaque components were colour-coded as white (dense calcium), red (necrotic core), light green (fibrofatty) or dark green (fibrotic tissue). The area of each type of tissue expressed as a percentage of the total plaque area was calculated. The numbers of thin-cap fibroatheromas and ruptured plaques were recorded. Thin-cap fibroatheroma was defined as a lesion with ≥40% plaque burden, a confluent necrotic core (>10%) in direct contact with the lumen (no evidence of a fibrous cap) and a minor amount of calcium (<10%) present in three consecutive VH-IVUS cross-sectional frames. Plaque rupture was defined as ulceration or fissuring of a plaque, with a tear detected in the fibrous cap.
PCI procedure
All patients received 300 mg aspirin and 300 mg clopidogrel, orally, before PCI and 100 mg/day aspirin and 75 mg/day clopidogrel, orally, following the procedure. Anticoagulation treatment with subcutaneous enoxaparin sodium at a dose of 1 mg/kg every 12 h was initiated when the patient was admitted to the ward and was continued until 72 h after the PCI procedure. PCI was performed through the radial artery. Predilation of the target lesion with a balloon was usually performed before stenting. After stent deployment, postdilation was performed in each patient.
Coronary flow analysis
Coronary angiograms were analysed using standard methodology. Angiographic coronary blood flow was assessed at baseline and after stent deployment, according to the Thrombolysis in Myocardial Infarction (TIMI) flow grade10,11 and the Corrected TIMI Frame Count (CTFC).12,13 No-reflow was defined as a post-PCI TIMI flow grade of 0, 1 or 2 in the absence of mechanical obstruction. 14 Normal reflow was defined as TIMI flow grade 3. On this basis, patients were divided into a no-reflow group and a normal reflow group.
Laboratory assessments
Fasting blood samples were obtained from each patient on the day of diagnostic coronary angiography for the measurement of PAPP-A, high-sensitivity C-reactive protein (hsCRP) and cTnT. Further blood samples (not fasting samples) were taken 24 h after the PCI procedure, for a second measurement of cTnT. All blood samples were centrifuged immediately at 3000 rpm for 10 min, at room temperature ‘(Thermo Scientific™ MicroCL 17, Thermo Fisher Scientific, Waltham, MA,USA), and the serum was aliquoted and stored at −80 ℃ until analysed.
Serum PAPP-A levels were measured using an ultrasensitive enzyme-linked immunosorbent assay (ELISA) kit (IBL International, Hamburg, Germany), according to the manufacturer’s instructions, on an Evolis™ automated ELISA processor (Bio-Rad Laboratories, Hercules, CA, USA). This kit is specific for PAPP-A and its measurement range is 0–100 mIU/l. A highly sensitive latex particle-enhanced immunoturbidimetric assay (Kamiya Biomedical, Seattle, WA, USA) was used, according to the manufacturer’s instructions, to quantify hsCRP. cTnT levels were determined using a chemiluminescent immunoenzymatic assay (Beijing Tigsun Diagnostics, Beijing, China) according to the manufacturer’s instructions; the upper normal cut-off value suggested by the manufacturer is 0.04 ng/ml.
Statistical analyses
Data for categorical variables were presented as frequencies and were compared using the χ2-test or Fisher’s exact test (if there was an expected cell value <5). Data for continuous variables were presented as the mean ± SD; Student’s t-test was used to compare data between the two groups. Correlations between continuous variables were analysed using Pearson’s correlation coefficient method. A P-value of <0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS® software, version 15.0 (SPSS Inc., Chicago, IL, USA).
Results
Baseline clinical characteristics for patients with unstable angina, undergoing percutaneous coronary intervention, divided according to reflow outcome.
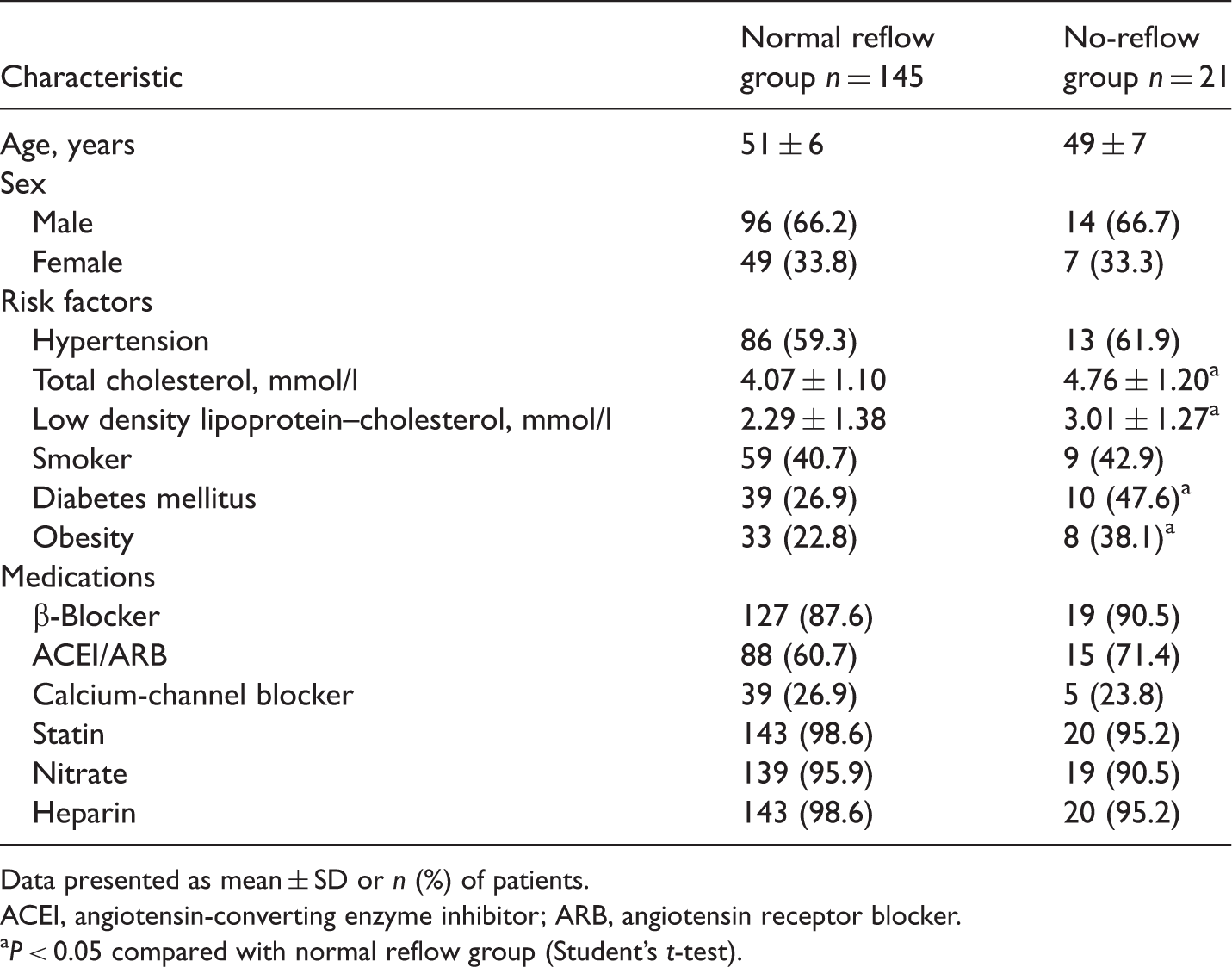
Data presented as mean ± SD or n (%) of patients.
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker.
P < 0.05 compared with normal reflow group (Student’s t-test).
Serum pregnancy-associated plasma protein A (PAPP-A), high-sensitivity C-reactive protein (hsCRP) and cardiac troponin T (cTnT) levels in patients with unstable angina undergoing percutaneous coronary intervention (PCI), divided according to reflow outcome.

P < 0.05 compared with normal reflow group (Student’s t-test).
Angiographic data from patients with unstable angina undergoing percutaneous coronary intervention (PCI), divided according to reflow outcome.

Data presented as mean ± SD or n (%) of patients.
Only side branches with a diameter >1.5 mm were analysed.
TIMI, Thrombolysis in Myocardial Infarction; CTFC, Corrected TIMI Frame Count.
P < 0.05 compared with normal reflow group (Student’s t-test).
Side branches were crossed in 13.8% of normal reflow patients and 14.3% in no-reflow patients, but this difference was not statistically significant.
Characteristics of coronary plaques, as seen on virtual-histology intravascular ultrasound in patients with unstable angina undergoing percutaneous coronary intervention (PCI), divided according to reflow outcome.

Data presented as mean ± SD or n (%) of patients.
P < 0.05 compared with normal reflow group (Student’s t-test).
Correlations between serum PAPP-A levels and plaque characteristics are shown in Figures 1 and 2. Serum PAPP-A was negatively correlated with plaque fibrotic area (Figure 1; P < 0.001) and was positively correlated with necrotic core area (Figure 2; P < 0.001).
Correlation between percentage of fibrotic area in coronary plaques and serum pregnancy-associated plasma protein A (PAPP-1) levels in patients with unstable angina, undergoing percutaneous coronary intervention. Correlation between percentage of necrotic core area in coronary plaques and serum pregnancy-associated plasma protein A (PAPP-1) levels in patients with unstable angina, undergoing percutaneous coronary intervention.

Discussion
The relationship between PAPP-A and coronary plaque stability has attracted much attention. Studies have demonstrated that patients with hyperechoic or isoechoic carotid plaques have significantly higher PAPP-A levels than those with hypoechoic carotid lesions. 15 The prognostic value of serum PAPP-A has been studied in patients with coronary artery disease. It was reported that the PAPP-A level is associated with inflammation, and may be used to detect plaque instability and rupture before an increase in cTnT is detectable. 16 PAPP-A has also been shown to be independently associated with recurrent cardiovascular events in patients with non-ST-segment elevation acute coronary syndrome 17 and seems to be valuable in predicting outcome in patients admitted with high-risk acute coronary syndromes. 18 However, discrepant results have been reported in relation to PAPP-A elevation. In patients with acute coronary syndrome, serum PAPP-A elevation seemed to be caused by heparin-induced release of PAPP-A from the arterial wall, not by excretion from vulnerable plaques. 19 This suggests that PAPP-A cannot be used as a marker for vulnerable atherosclerotic plaques. Wittfooth et al. 20 confirmed that heparin-induced PAPP-A elevation can be seen in various patients and should be taken into account when PAPP-A is studied as a biomarker. In the present study, patients in both groups received the same dose of low molecular weight heparin, but the serum PAPP-A level was significantly higher in the no-reflow group than in the normal reflow group, and was negatively correlated with the percentage of fibrotic tissue and positively correlated with the percentage of necrotic area in the coronary plaques. This indicates that, in patients with unstable angina, PAPP-A may be a biomarker of plaque instability. The reasons for discrepant results concerning PAPP-A levels in coronary plaque instability should be further explored.
A 2011 study reported a convincing result regarding the relationship between serum PAPP-A and no-reflow after PCI: in patients with acute coronary syndrome and stable coronary heart disease, multivariate logistic regression analysis showed that serum PAPP-A was an independent predictor of the no-reflow phenomenon and a useful biomarker for stratifying high-risk coronary no-reflow patients after PCI. 21 However, the mechanism underlying this relationship is not yet clear.
Since many studies have found that PAPP-A is related to plaque instability, the present study investigated the relationships between PAPP-A, plaque components and no-reflow in patients with unstable angina pectoris. It is thought that plaque characteristics may be predictive of no-reflow after PCI. In one study, attenuated plaque identified by greyscale IVUS in acute coronary syndrome patients was associated with higher C-reactive protein levels, more severe and complex lesion morphology, reduced coronary blood flow before PCI and (particularly) no-reflow after PCI. 22 The HORIZONS-AMI trial 23 further confirmed the value of attenuated plaques in predicting transient deterioration in coronary flow and/or no-reflow during PCI. Plaque rupture, which is another common sign of plaque instability, has been found to be closely related to no-reflow in patients with ST-segment elevation myocardial infarction.24,25 In addition, the fibrofatty volume detected by VH-IVUS and lipid-rich plaque assessed by IB-IVUS have been reported to be important predictors of coronary no-reflow after PCI,4,14 while others have shown that only the percentage of necrotic core and thin-cap fibroatheroma were predictive of no-reflow after PCI. 26 These discrepancies may be attributable to the different patient populations, as some studies were performed in patients with acute myocardial infarction, while others included both patients with acute myocardial infarction and those with unstable angina.
The relationship between plaque morphology and no-reflow in patients with unstable angina pectoris is not yet clear. The present study in 166 patients with unstable angina showed that those who experienced no-reflow after PCI had coronary plaques with a lower fibrotic tissue area and higher necrotic core area, and higher rates of plaque rupture and thin-cap fibroatheroma.
In conclusion, the present study demonstrated that patients with unstable angina with the no-reflow phenomenon had higher serum PAPP-A levels, plaques with a higher percentage of necrotic area and a lower percentage of fibrotic tissue, and more thin-cap fibroatheromas and ruptured plaques, compared with unstable angina patients with normal reflow after PCI. Using these predictive parameters, protective measures (such as intensive use of glycoprotein IIb/IIIa inhibitors and high doses of antiplatelet agents), as well as the use of optimal stent implantation and distal protective devices to reduce distal embolization and the no-reflow phenomenon after stent deployment, can be considered in patients with unstable angina, who also have a high serum PAPP-A level and lesions with a large necrotic core.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.