
Abstract
Background
Avascular osteonecrosis of the femoral head (AVN) often results in total hip arthroplasty (THA). The cause for increased THA revision rates among patients with AVN is not yet fully understood.
Purpose
To perform a comparative radiological analysis of implant integration between patients with AVN and osteoarthritis (OA).
Material and Methods
After a matched pair analysis of 58 patients, 30 received THA due to OA, 28 due to AVN. X-ray images were evaluated after one week (“baseline”) and on average 37.58 months postoperatively (“endline”). The prosthesis was grouped into 10 regions of interest (ROI): seven femoral and three acetabular. Incidence, width, and extent of “radiolucent lines” were measured within each zone.
Results
Between baseline and endline, width and extent progressed more noticeably in all femoral and acetabular zones among patients with AVN. In femoral ROI 1, the width increased in 40% of AVN cases compared to 6.7% of OA cases. For acetabular ROI 3, the width increased in 26.7% of AVN cases compared to no perceived changes in the OA group. No signs of prosthetic loosening were found in the AVN group.
Conclusion
The increase of width and extent of radiolucent lines over time in patients with AVN could be a sign of lack of osteointegration. However, prosthetic loosening in absence of clinical symptoms cannot be deduced from radiological findings after medium-term postoperative follow-up. Further long-term studies are required to monitor how radiolucent lines develop in respect to long-term implant loosening. Dependent on bone quality, individually adapted reaming and broaching of the implant site are recommended.
Keywords
Introduction
Osteonecrosis of the femoral head leads to progressive bone degeneration due to insufficient blood supply (1). Middle-aged men aged 30–50 years are affected four times as often as women. In most cases it manifests itself bilaterally, with an incidence of 30%–72% within two years (2). Typically, the anterolateral portion of the femoral head is affected due to its increased sensitivity to a lack of blood supply (3).
The prevalence of avascular osteonecrosis of the femoral head (AVN) is still unclear. In the United States, the number of patients experiencing AVN is in the range of 10,000–20,000 per year. Parameters that affect the choice of therapy are patient age, stage of the disease, localization and extent of the lesion, and the underlying cause of AVN (1). In the early stages, non-operative treatment is possible, although a final conclusion concerning the effectiveness of certain therapies in different stages has not yet been reached (4). Left untreated, AVN has been shown to be a progressive disease that may cause subchondral fractures within 2–3 years. At this point, joint-preserving therapy may no longer be a viable option (5).
Non-operative treatment options, indicated especially in the pre-collapse or early post-collapse stages, are reduction of weightbearing, medication, and physical therapy, generally employed until total hip arthroplasty (THA) is performed (5,6).
The most common surgical therapy in early stages of AVN is core decompression to achieve a reduction in pressure and stimulate reperfusion of the ischemic areas (7,8). Core decompression can be combined with a cancellous bone graft (9).
THA is the gold standard for late-stage AVN, mainly in cases of osteoporosis, secondary osteoarthritis, and elderly patients (7,10). Of all THAs, 5%–12% are performed due to AVN, with a mean patient age of 38 years (2,3). For patients with AVN, long-term survival rates of implants vary from 97% after a six-year follow-up to 87% after a nine-year follow-up, depending on the literature (11). The cause of varying implant survival rates in AVN and osteoarthritis (OA) is yet to be determined. Some authors describe no significant difference in survival rates, at least for a short-term period of observation (4,10,12), while others witnessed an increased revision rate for AVN patients up to 6.1% after 16 years, compared to 4.2% in an OA group (6,13,14). In the course of time, implant loosening became the primary cause for revision surgery (14). Young age, increased activity level, or poor bone quality accompanied by insufficient integration of the implant could play an important role. Due to our lack of understanding concerning the influence of AVN on implant integration, we sought radiological evidence hinting at early THA loosening in patients with AVN. Our hypothesis is that patients with AVN show more radiolucent lines in follow-up studies.
The main topics were as follows: (i) if there are any visible radiological changes at the implant surrounding the bone; (ii) if these can be quantified; and (iii) if these can be used as indicator for implant integration.
Therefore, radiological analysis was performed to assess the bone–implant interface area looking for radiolucent lines that show the retreat of bone around the implant. Furthermore, subsidence of the stem was measured.
Material and Methods
Between 2007 and 2013, a total of 4221 primary THAs were performed at the department of orthopedics at a university hospital.
In the same period, 255 patients with AVN were treated. Of them, 60 received THA. They were included in the present study. The remaining 195 patients initially received a joint-preserving operation (core decompression). Of them, 85 converted to a higher ARCO stage and received THA, while 110 patients maintained their native hip. All 195 cases were excluded from the present study according to the inclusion criteria “no prior joint-preserving surgery.” The abovementioned 60 cases served as study collective (32 men, 28 women; mean age = 63.24 years; age range = 23–87.7 years). They received a THA between 2007 and 2012 (Pinnacle, Corail; Depuy, Warsaw, IN, USA). Nine patients received a bilateral THA.
The OA cohort included 135 patients (64 men, 71 women; mean age = 62.69 years; age range = 50–75 years) (Fig. 1). They received a THA between 2011 and 2013.
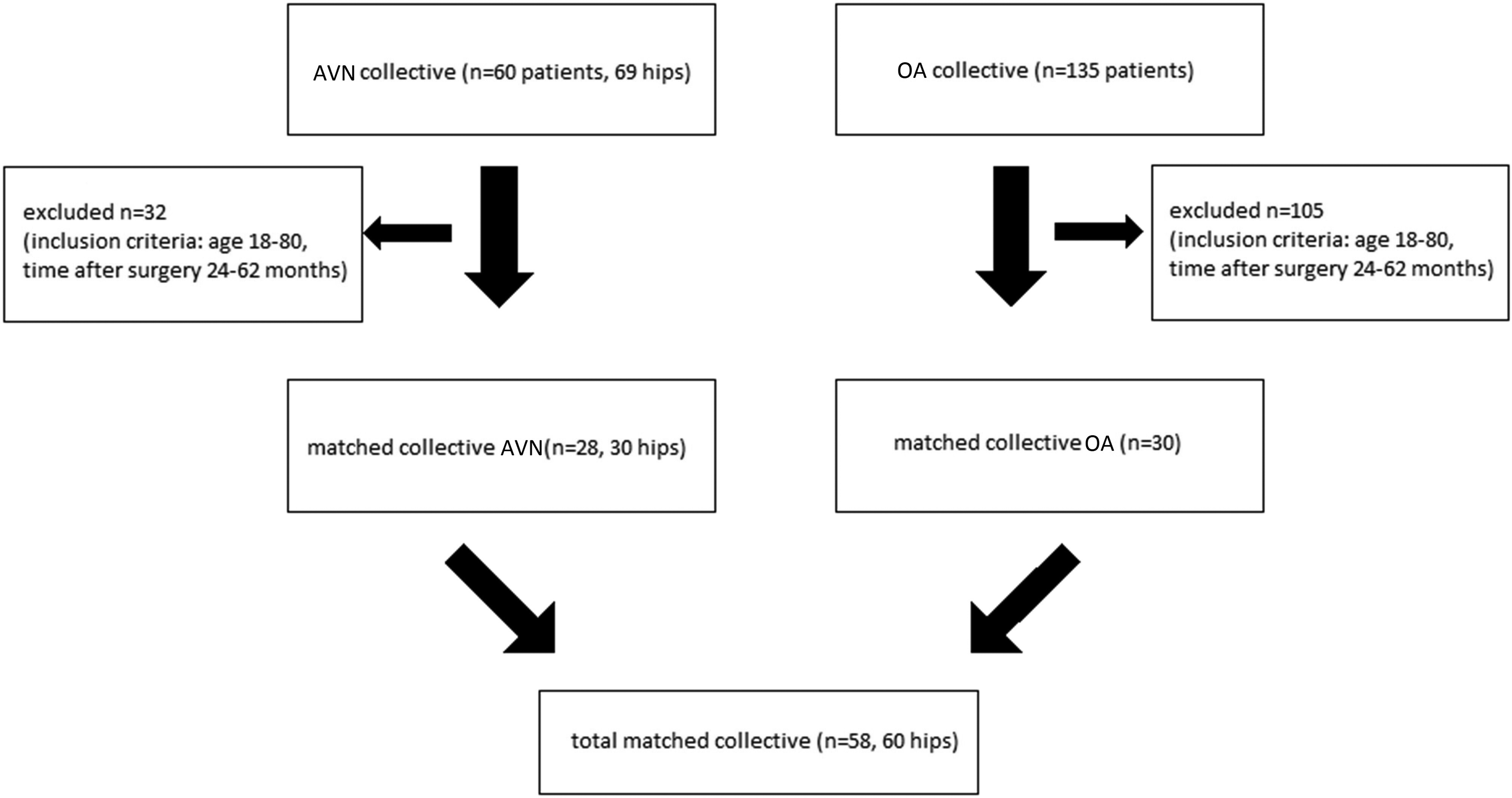
Consort diagram: matching of patient collective avascular osteonecrosis of the femoral head and osteoarthritis.
Individuals were matched according to age, sex, elapsed time after surgery, and body mass index (BMI). Due to the different range of age in our two collectives, we excluded some cases of AVN for an equitable matched pairing process. Different bone quality in different age classes made correct matching inevitable to prevent an incomparability bias.
The 30 matched pairs included 28 men and 32 women (mean age = 63.88 years; age range = 50–80 years) at the time of the procedure.
In total, we included 58 patients after the matched-pair analysis. A total of 30 individuals received a unilateral THA due to OA and 28 due to AVN, two of them bilaterally (Fig. 1).
Within the matched collective, two anteroposterior (AP) view X-rays of each patient were evaluated: one week postoperatively (baseline) and a mean of 37.58 months postoperatively (endline, range = 24–62 months). The X-rays were evaluated with special digital imaging software (mediCAD, HECTEC, Altdorf, DE, USA). Every X-ray was scaled to the head of the implant (32-mm caliper) as reference.
Implants were divided into regions of interest (ROI): seven zones at the femoral shaft classified by Gruen et al. (15) and three zones within the acetabular region according to DeLee and Charnley (16). Radiolucent lines were measured within these defined zones. Radiolucent lines are lucencies detected along the implant–bone interface on X-ray imaging according to Katzer and Löhr (17).
The radiolucent line at the implant stem (Fig. 2) was defined as follows: according to its width (i.e. the distance from implant to bone): 0 = no radiolucent line, 1 = <1 mm, 2 = 1–2 mm according to Salvati et al. (18); and according to its extent (i.e. along the implant): 0 = no radiolucent line, 1 = <50% of the zone, 2 ≥50% according to Roche et al. (19).
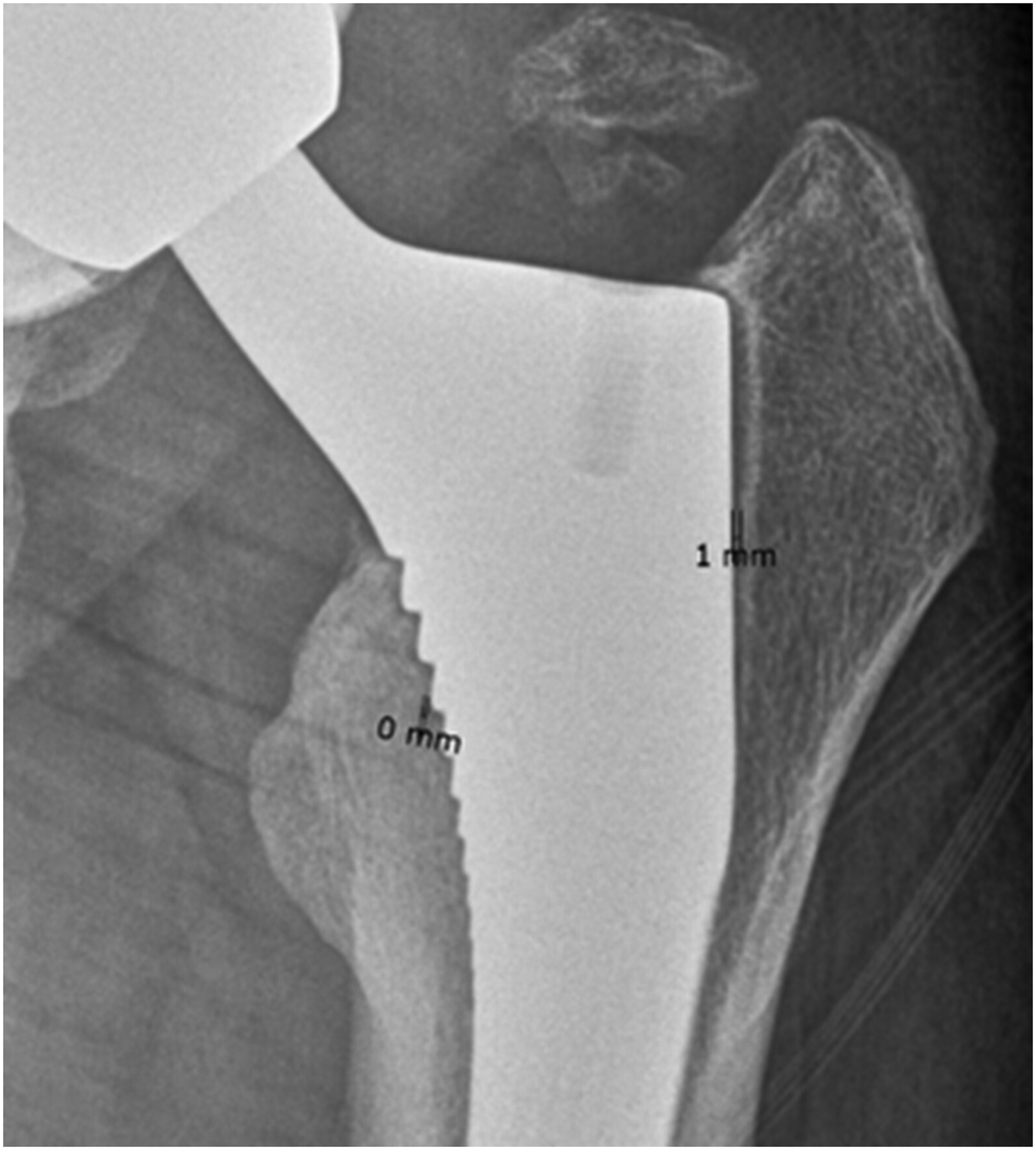
Measuring of the width of the radiolucent line at the stem; program shows a precision up to 1 mm (i.e. 0 ≤ 1 mm in the measurements).
The radiolucent line at the cup of the implant (Fig. 3) was measured similarly; however, the width was defined differently: width (i.e. the distance from implant to bone): 0 = no radiolucent line, 1 ≤1 mm, 2 = >1 mm, 3 = >2 mm according to Udomkiat et al. (19); and its extent analog to the implant stem.
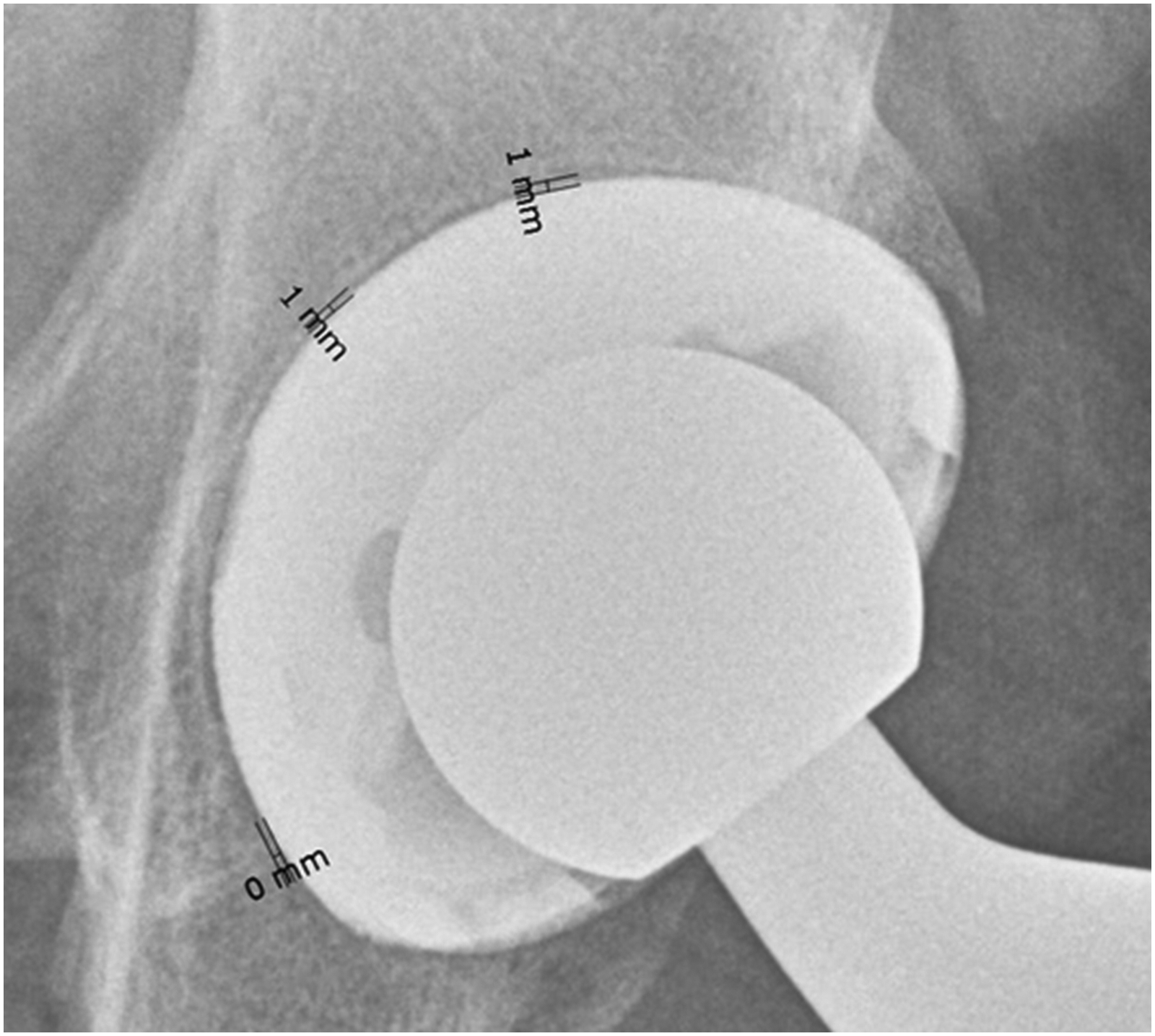
Measuring the width of the radiolucent line at the cup.
The statistical analysis was performed with SPSS Statistics version 23 (IBM Corp., Armonk, NY, USA). For the comparison of metrical data (such as BMI) between both groups, the two-sample t-test was used. The analysis of radiologic measurements of the radiolucent lines was carried out by applying the Mann–Whitney U-test for the comparison of the two groups and the Wilcoxon signed-rank test for comparison throughout time.
The present study was conducted after authorization by the Institutional Ethical Board of a medical university. It has been performed in accordance with the ethical standards in the 1964 Declaration of Helsinki and has been carried out in accordance with regulations of the US Health Insurance Portability and Accountability Act (HIPAA). Written informed consent for participation in this investigation was obtained from all patients.
Results
Differences in radiolucent lines measured one week after surgery (baseline) were significant in the femoral zones ROI 1 (P = 0000) and ROI 7 (P = 0000) regarding both width and extent (Table 1). The OA group displayed a higher number, increased width, and more extensive radiolucent lines in both zones. All patients with OA showed a radiolucent line of <1 mm in zone ROI 1, whereas 46.7% of the patients with AVN showed no radiolucent line at all within that zone. In zone ROI 7, all patients with OA showed a radiolucent line <1 mm, whereas 40% of patients with AVN showed no radiolucent line within that zone. No significant difference was found for the remaining zones (ROI 2–6) (Fig. 4).
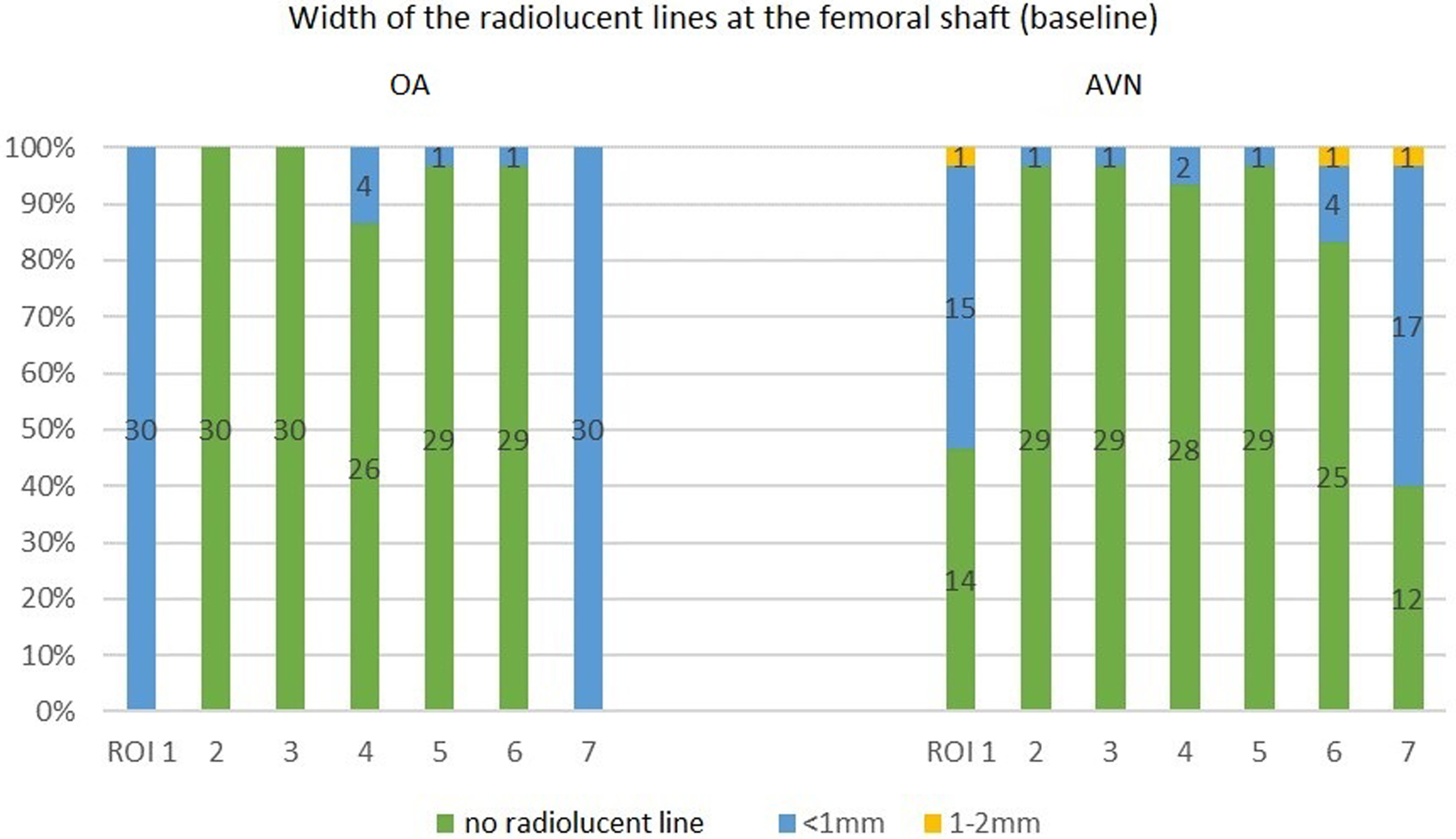
Width of radiolucent lines one week postoperatively (baseline) in the femoral zones ROI 1–7.
Measurement of radiolucent lines one week postoperatively (baseline) in femoral zones ROI 1–7 according to Gruen et al.
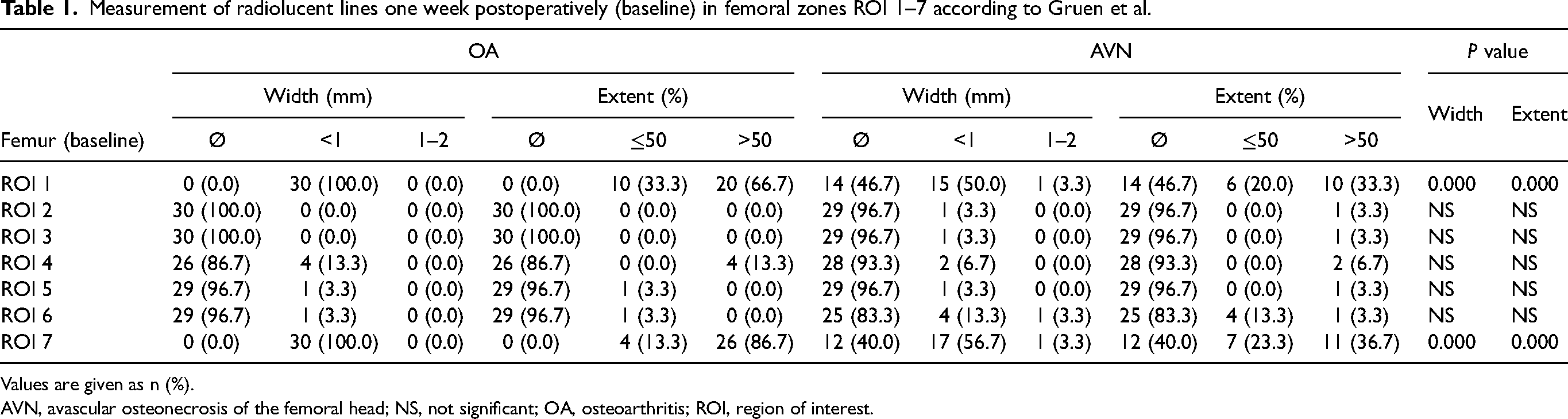
Values are given as n (%).
AVN, avascular osteonecrosis of the femoral head; NS, not significant; OA, osteoarthritis; ROI, region of interest.
At baseline, all acetabular zones (ROI 1–3) showed a significant difference between patients with OA and those with AVN. A higher number of radiolucent lines were found in the OA group compared to the AVN group (Table 2).
Measurement of radiolucent lines one week postoperatively (baseline) in acetabular zones ROI 1–3 according to DeLee and Charnley (16).

Values are given as n (%).
AVN, avascular osteonecrosis of the femoral head; NS, not significant; OA, osteoarthritis; ROI, region of interest.
At endline (a mean of 37.58 months postoperatively), the measurement of radiolucent lines showed significant differences in femoral zone ROI 1, regarding extent, as well as in femoral zone ROI 7, regarding width and extent. No significant difference was found among the remaining zones.
A significant difference was seen in the acetabular zones ROI 1 and 2 (only regarding the extent of radiolucent lines). At the endline, more radiolucent lines were visible in the OA group.
Over the course of time (during the time between baseline and endline), the radiolucent lines in the femoral zone ROI 1 got wider in 12 (40%) patients with AVN, while the radiolucent lines only widened in 2 (6.7%) patients with OA. This difference was significant (Fig. 5).
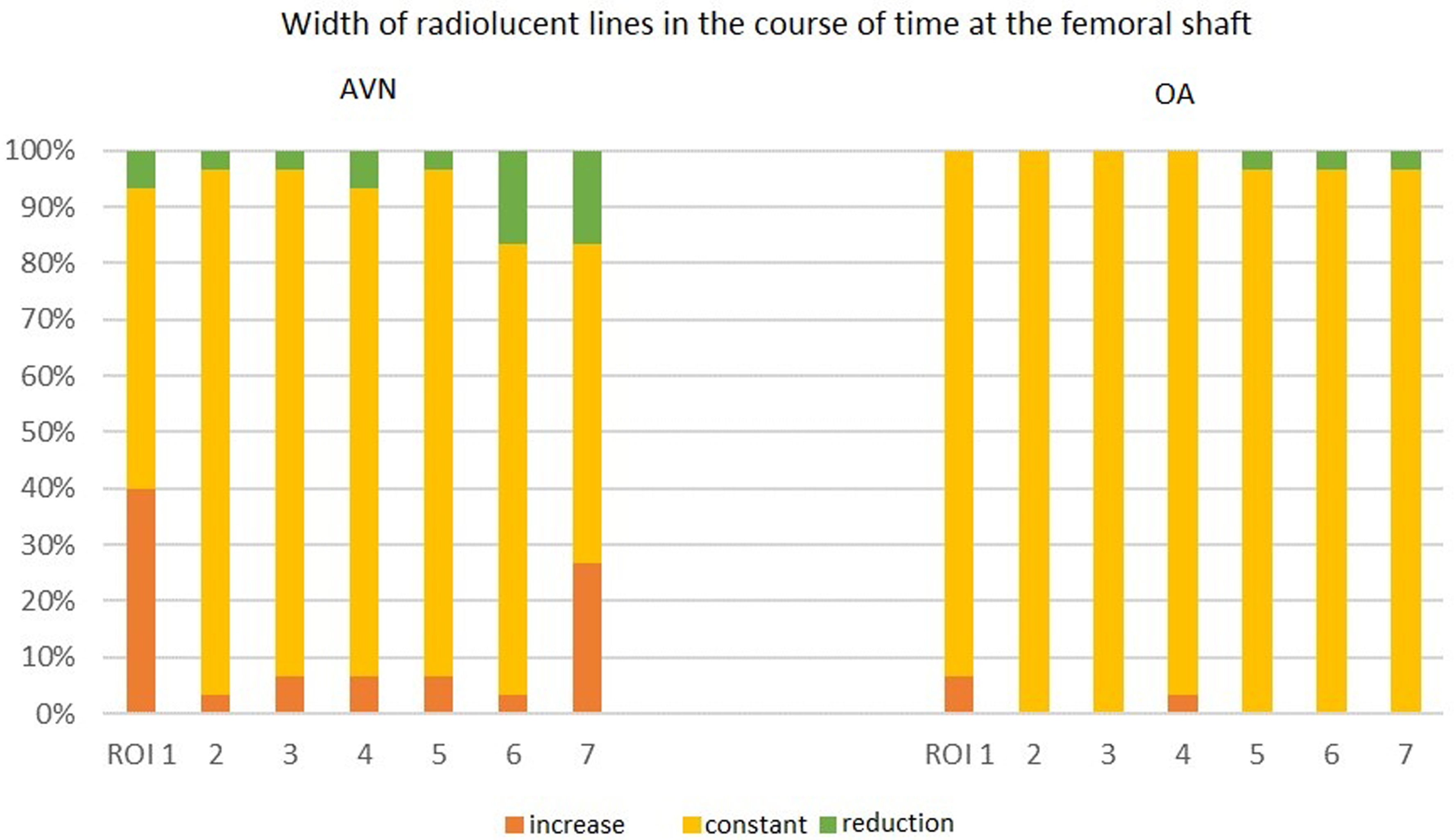
Width of radiolucent lines over time (baseline–endline) at the femoral shaft in the seven femoral zones according to Gruen et al. (ROI 1–7) in relation to the number of patients in comparison to both collectives in %.
In the acetabular zone ROI 3, the radiolucent lines widened in 8 (36.7%) patients with AVN– in contrast to none within the OA group. Simultaneously, the extent of the radiolucent line in zone ROI 3 increased in 14 (46.7%) patients with AVN compared to 3 (10%) patients with OA. This also presented a significant difference (Table 3).
Course of radiolucent lines between baseline and endline in acetabular zones ROI 1–3 according to DeLee and Charnley (16).

Values are given as n (%).
AVN, avascular osteonecrosis of the femoral head; NS, not significant; OA, osteoarthritis; ROI, region of interest.
In general, the widening and increasing extent of radiolucent lines occurred in all femoral and acetabular zones within the AVN group. No implant loosening was found in the AVN group at the endline, however. All prosthesis components remained in place without the need for revision surgery.
Discussion
The aim of the present study was to analyze whether radiological signs of THA loosening, in this case “radiolucent lines,” vary in incidence, width, and extent among matched AVN and OA groups. Indeed, we found significant differences regarding the occurrence and progression of radiolucent lines over time after THA.
According to Engh et al., more extensive radiolucent lines (>50% extension in one zone), also referred to as “reactive lines” or “loosening lines,” are one of the major indicators for poor osteointegration of the implant (20). Katzer et al. stated that progressive loosening lines or loosening lines exceeding 2 mm two years after THA bear an increased risk of revision surgery up to 50% (17).
In our study, at baseline, significantly more radiolucent lines were found in patients with OA in femoral zones ROI 1 and 7 (the metaphyseal zones), as well as in acetabular zones ROI 1–3 (the lateral and medial third of the cup). These radiolucent lines were significantly wider and more extensive in the X-rays of patients with OA than in patients with AVN. A possible explanation is the increased amount of sclerotic bone at the subchondral acetabular surface and endofemorally in patients with OA. The studies by Craiovan et al. showed significantly lower levels of bone density for patients with AVN in DXA measurements in femoral zones ROI 1 and 7, as well as in acetabular zones ROI 2 and 3 comparing a group of patients with AVN to patients with OA (21,22). Consequently, we can assume that due to a reduced bone density in patients with AVN, the austerity of bone is lower, and therefore less wide and less extended radiolucent lines occur in this group. Hence, reaming and broaching to prepare the implant site should be adapted individually to bone quality regarding the stem implant type (rather meta-diaphyseal stabilized than only metaphyseal).
Khalily and Whiteside discovered an increased number of radiolucent lines two years postoperatively in a group of patients who ultimately underwent revision surgery, compared to a group that required no revision surgery, using an uncemented Ortholoc femoral component (23). Comparable to our study, the femur was grouped into the respective zones according to Gruen et al. (15), also describing a significant difference in the occurrence of radiolucent lines in the revision group compared to the non-revision group in femoral zones ROI 1 and 7. Our study produced similar results for ROIs 1 and 7. The radiolucent lines increased over three years.
Our analysis is the first to compare patients with OA to those with AVN. However, all patients who showed an increase in the length and width of radiolucent lines at the endline demonstrated no indication for revision arthroplasty. In terms of estimating the risk of revision surgery when observing a progression of radiolucent lines, accuracy lies at approximately 50% according to literature (17), as though for our study that assumption can only be hypothetical.
Udomkiat et al. were able to show that a new appearance of a radiolucent line two years postoperatively, or a progression of an existing radiolucent line, is one of the most important predictive factors for the loosening of a hemispheric porous-coated cementless cup. In addition, radiolucent lines in all three acetabular zones, as well as a single radiolucent line >2 mm, provides an indication for the possible need for revision arthroplasty (19). A correlation between different patient collectives, such as AVN and OA as performed in our study, was not implemented.
We found significant differences in the development and progression of radiolucent lines between patients with OA and those with AVN within femoral zone ROI 1, as well as acetabular zone ROI 3. These are the zones with the largest proportion of cancellous bone. In femoral zone ROI 1, a widening of the radiolucent line was shown in 33% of patients with AVN compared to only 13% in patients with OA (P = 0,013). Within the acetabular zone, radiolucent lines also widened more often in patients with AVN compared to those with OA. In addition, there was an increased extension of radiolucent lines in patients with AVN. We used a hydroxyapatite coated stem (Corail; Depuy, Warsaw, IN, USA) in our study. It is designed for meta-diaphyseal osseous incorporation, proximal load application, and distal load transmission to the bone (24). This specific type of incorporation explains our results: the proximal femoral zones ROIs 1 and 7, according to Gruen et al., produced the highest number of radiolucent lines in both the OA and AVN groups. These results could possibly vary with different designs of stem incorporation, e.g. short stems, which incorporate metaphyseally (24,25). Further studies analyzing the development and progression of radiolucent lines utilizing different implant designs are required.
Bergh et al. found an increased risk for revision arthroplasty in patients with AVN (14). However, it is unclear whether AVN has a negative impact on survivorship of THA or if shorter survival rates are associated with younger age and the accompanying higher activity levels of patients.
The present study has some limitations. First is the relatively low number of cases as a result of performing a matching analysis in order to achieve an accurate comparison. To obtain the lowest possible bias for the comparability of bone quality and THA integration, each patient was directly compared with a patient from the other group. On the one hand, various bias such as age, sex, and BMI were removed. On the other hand, this reduced the number of patients in the two groups. It would be preferable for future studies to include larger patient collectives. Our selected patient collective only included clinically consolidated THAs without any need for revision surgery. It would also be interesting to observe the formation and development of radiolucent lines in a patient collective that has undergone THA revision surgery. A study design with a longer follow-up period is necessary to rule out any contingencies in terms of increased revision rates. Another limitation of our study is due to the fact that only a single implant design was evaluated. We do not have any information on stem implants that solely anchor at the metaphyseal aspect. Hence, with the available data we cannot provide a prediction for implant survival of short stems.
In conclusion, patients with AVN display radiolucent lines that exhibit a lower incidence, and reduced width and extent at baseline due to the presence of lower bone density within the femoral and acetabular regions. At the final follow-up (endpoint) we found radiolucent lines in patients with AVN to have progressed more frequently with regard to width and extent compared to those of patients with OA. This could be indicative of lack of osteointegration or proximal femoral loosening in terms of metaphyseal stem integration in the AVN group, possibly hinting at a higher revision rate for patients with AVN in the future. However, one cannot assume a loosening implant solely on the grounds of the presence of radiological signs and the absence of clinical symptoms within a medium-term postoperative period. Further studies, including well-designed long-term (10–15 years) prospective studies, are needed to identify how the development of radiolucent lines are associated with implant survival and implant loosening in our two groups. Considering a medium-term observational period, the Corail stem, with its meta-diaphyseal anchoring capability, appears to offer stable integration results in patients with AVN. Supported by the data and results of our research, we conclude that when performing THA in patients with AVN, good results can be achieved with a meta-diaphyseal stem anchoring system.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.