
Abstract
Background
For the normal functioning of the patellofemoral joint (PF), the relationship between the patella and the trochlear groove must be compatible.
Purpose
To investigate the relationship between patellofemoral joint morphology (PFM) and patellar chondromalacia.
Material and Methods
Overall, 136 knees of patients aged 20–55 years examined between March 2020 and March 2021 were included in this study. In all patients, trochlear sulcus angle, trochlear sulcus depth, trochlear facet asymmetry, patella alta (Insall–Salvati [IS] index), and patellar facet asymmetry were measured. Of these cases, 66 knees with an abnormality detected in any of the measurements for PFM were included in the case group. Moreover, 70 knees with demonstrating normal PFM measurements were included in the control group.
Results
The incidence and grade of chondromalacia was higher in the case group than in the control group (P < 0.001). Between the patients with and without chondromalacia trochlear sulcus angle (mean = 138.25° ± 10.02° vs. 132.58° ± 7.24°; P = 0.001), IS index (mean = 1.25 ± 0.21 vs. 1.16 ± 0.15; P = 0.014), patellar facet asymmetry (mean = 0.77 ± 0.09 vs. 0.73 ± 0.12; P = 0.039), trochlear sulcus depth (mean = 5.39 ± 1.42 mm vs. 6.27 ± 1.04 mm; P < 0.001), and trochlear facet asymmetry (mean = 0.67 ± 0.11 vs. 0.71 ± 0.09; P = 0.023) measurements, there was a significant difference.
Conclusion
The presence of at least one of the measures indicating pathology in PFM is associated with the presence and severity of chondromalacia.
Introduction
For the normal functioning of the patellofemoral (PF) joint, the relationship between the patella and the trochlear groove must be compatible. Developmental or acquired pathologies in patellofemoral joint morphology (PFM) can cause various clinical outcomes, such as chondromalacia patella, PF instability, and PF pain syndrome (1). Femoral trochlear dysplasia is a geometric abnormality in the trochlear groove and groove depth that usually affects the cranial part of the joint (2) and may affect the PFM. Previous studies have reported that trochlear depth and sulcus angle measurements obtained using magnetic resonance imaging (MRI) are associated with trochlear dysplasia (2). The relationship of the patella—another component of the joint—with the femur and patellar-shaped abnormalities may also affect the relationship with the joint. There are conflicting data regarding the effects of shape abnormalities of the structures forming the PF joint on patellar chondromalacia in the relevant literature (1,3–5).
Previously, morphological features of the joint were attempted to be evaluated using direct radiography, but currently, MRI of the knee is more widely used because it allows the evaluation of both cartilage and anatomy (6,7). The sensitivity of MRI in detecting chondromalacia patella is 66% in the early stages, whereas it increases to 85%–100% in the advanced stages (8).
The aim of the present study was to investigate the effects of changes in PFM on the presence and severity of patellar chondromalacia.
Material and Methods
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Ethics Committee of our hospital (No. 2497).
Overall, 148 knees of patients aged 20–55 years who applied for any reason between March 2020 and March 2021 were included in the study. In contrast, 12 knees were excluded from the study owing to a history of surgery, inaccessibility of the images, and inability to obtain images in a moving and appropriate position. Thus, 136 knees were included in the study.
MRI was performed using a 1.5-T system (Avanto; Siemens Healthineers, Erlangen, Germany) in the supine position with the knee in full extension. Moreover, the following sequences were obtained: sagittal fast spin-echo T1-weighted (TRTE = 584/22 ms, matrix = 202 × 320, field of view [FOV] = 180 mm, slice thickness = 4 mm); sagittal fat-saturated proton-density (PD)-weighted (TR/TE = 2180/42 ms, matrix = 213 × 320, FOV = 180 mm, slice thickness = 4 mm); coronal fat-saturated PD-weighted (TR/TE = 3210/47, matrix = 207 × 320, FOV = 170 mm, slice thickness = 4 mm); and axial fat-saturated PD-weighted (TR/TE = 2930/39 ms, matrix = 170 × 256, FOV = 160 mm, slice thickness = 3.5 mm).
Measurements of the PFM were performed in all cases. The trochlear sulcus angle measurement was made in the axial plane from the widest level of the trochlea, and the angle between the medial and lateral facets was measured (Fig. 1). A trochlear sulcus angle of >150° was considered to indicate pathology (9).

Increased trochlear sulcus angle (165°) on axial proton density magnetic resonance image.
The depth of the trochlear sulcus was measured in the axial plane at the widest level of the trochlea, and the distance between the line passing through the highest points of the medial and lateral trochlear facets and the deepest point of the groove was measured. A depth of <3 mm was considered to indicate pathology (9).
In addition, trochlear facet asymmetry was measured at the widest plane of the trochlea in the axial plane. The deepest point of the trochlear groove was considered to be the border; the lengths of the medial facet and lateral facets were measured, and the ratio of the medial and lateral facets was obtained. A ratio of <0.4 was considered to indicate pathology (9).
The assessment of the patella alta was performed using the Insall–Salvati (IS) index from the section with the widest patellar length in the sagittal plane (Fig. 2). The IS index was measured by dividing the patellar length by the patellar tendon length. A ratio of >1.3 was considered to indicate pathology (9).

Increased IS ratio on sagittal proton density magnetic resonance image; patella alta (IS index = 1.5). IS, Insall–Salvati.
For patellar facet asymmetry measurement, the section with the widest view of the patella in the axial plane was used. The patellar apex was considered to be the border, and the lengths of the medial facet and lateral facets of patella were measured, and the ratio of the medial and lateral facets was obtained.
Of the included knees, 66 knees with abnormalities based on any of the measurements for PFM were included in the case group, and 70 knees with normal measurements were included in the control group.
The evaluation of chondromalacia was performed using axial fat-suppressed proton density images. The International Cartilage Repair Society classification was used (10) for the analysis, and grades 1–2 chondromalacia were considered to be mild, whereas grades 3–4 chondromalacia were considered to be severe (Fig. 3). Among patients with ≥1 cartilage damage, the most serious damage was evaluated.
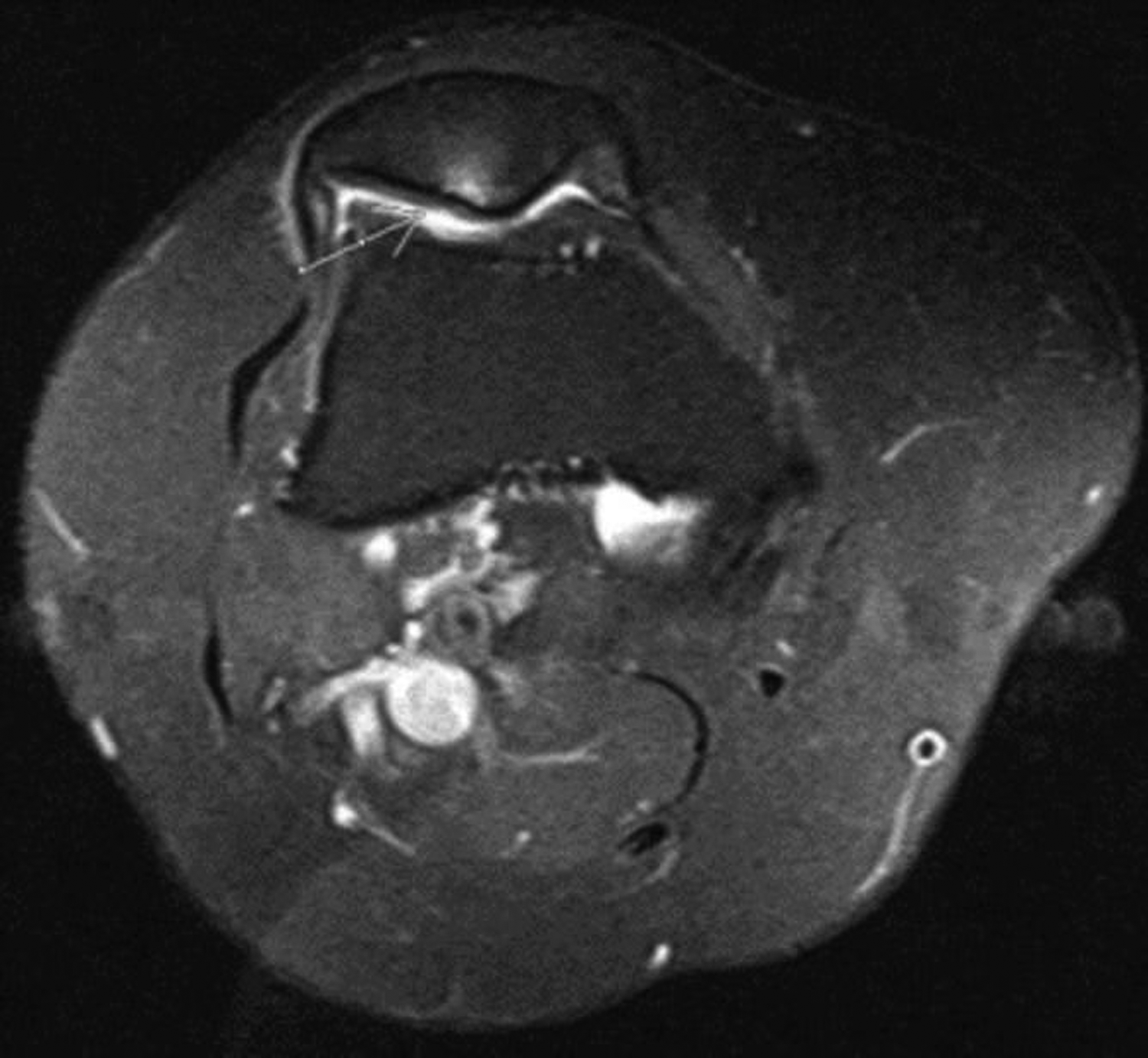
Grade 3 chondromalacia in the retropatellar cartilage (white arrow).
The presence, severity, and localization of chondromalacia (medial/lateral) were investigated between the case (with abnormal morphological measurements) and control (with normal measurements) groups.
Notably, the distributions of PFM measurements and the used threshold values were analyzed by classifying the patients into the groups of those with and without chondromalacia, regardless of the PFM measurements.
In the descriptive statistical analysis, mean, standard deviation (SD), median, and interquartile range (IQR) values were used for continuous data, and the number and percentage values were used for categorical data. The Shapiro–Wilk test was used to examine the conformity of the data in the normal distribution. During the comparison of continuous data between the case and control groups, the independent samples t-test was used for normally distributed data, and the Mann–Whitney U test was used for non-normally distributed data. Moreover, the one-way analysis of variance was used for comparisons between different grades of chondromalacia. The Tukey's test was used to determine which group or groups the difference originated from. The chi-square and Fisher's exact tests were used for between-group comparisons (cross tables) of nominal variables. Factors affecting the presence of chondromalacia were analyzed using multivariate logistic regression analysis. SPSS version 20 (IBM Corp., Armonk, NY, USA) program was used for the statistical evaluations, and a P value of <0.05 was considered statistically significant.
Results
There was no significant difference in the age and sex of the patients in the case group and those in the control group (P > 0.05). Notably, chondromalacia was detected in 78.8% and 44.3% of patients in the case and control groups, respectively (P < 0.001). Moreover, the grade of chondromalacia was higher in the case group than in the control group (P < 0.001). PFM measurements of the case and control groups are presented in Table 1, and the distribution of the threshold values used in PFM values is shown in Table 2. Furthermore, the trochlear facet asymmetry measurement was not <0.4 in any patient in the case group, but it was significantly lower in the case group (Tables 1 and 2). There was no significant difference in the localization of chondromalacia between the case and control groups (P > 0.05).
Comparison of PFM measurements between the case and control groups.
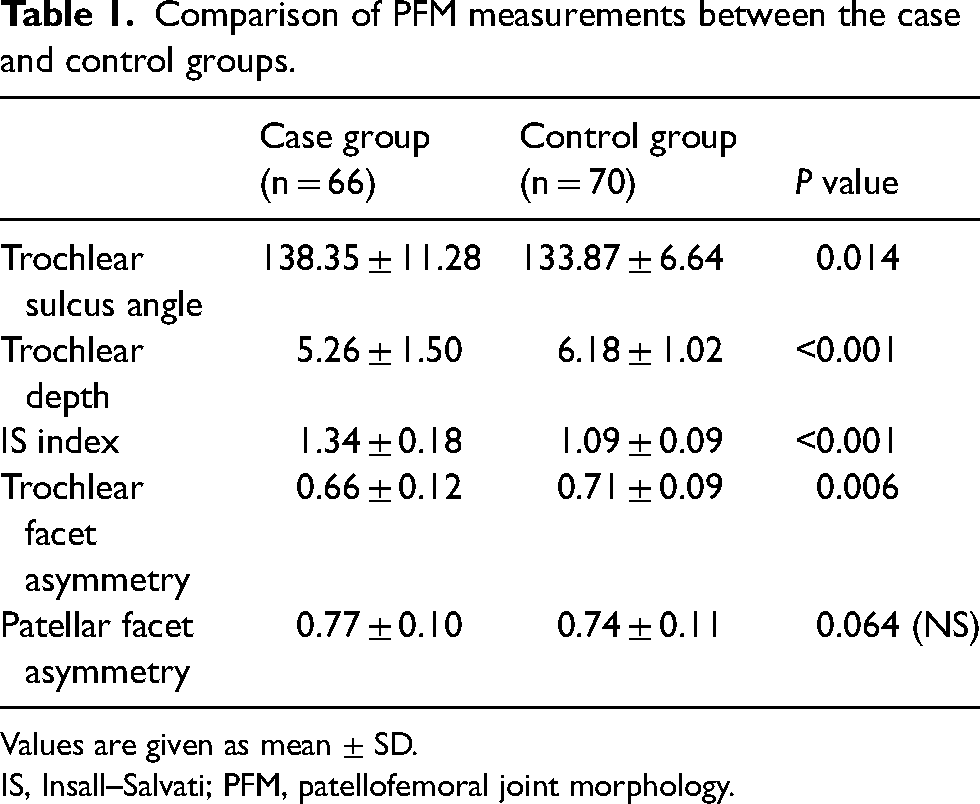
Values are given as mean ± SD.
IS, Insall–Salvati; PFM, patellofemoral joint morphology.
Distribution of PFM threshold values among patients in the case and control groups.
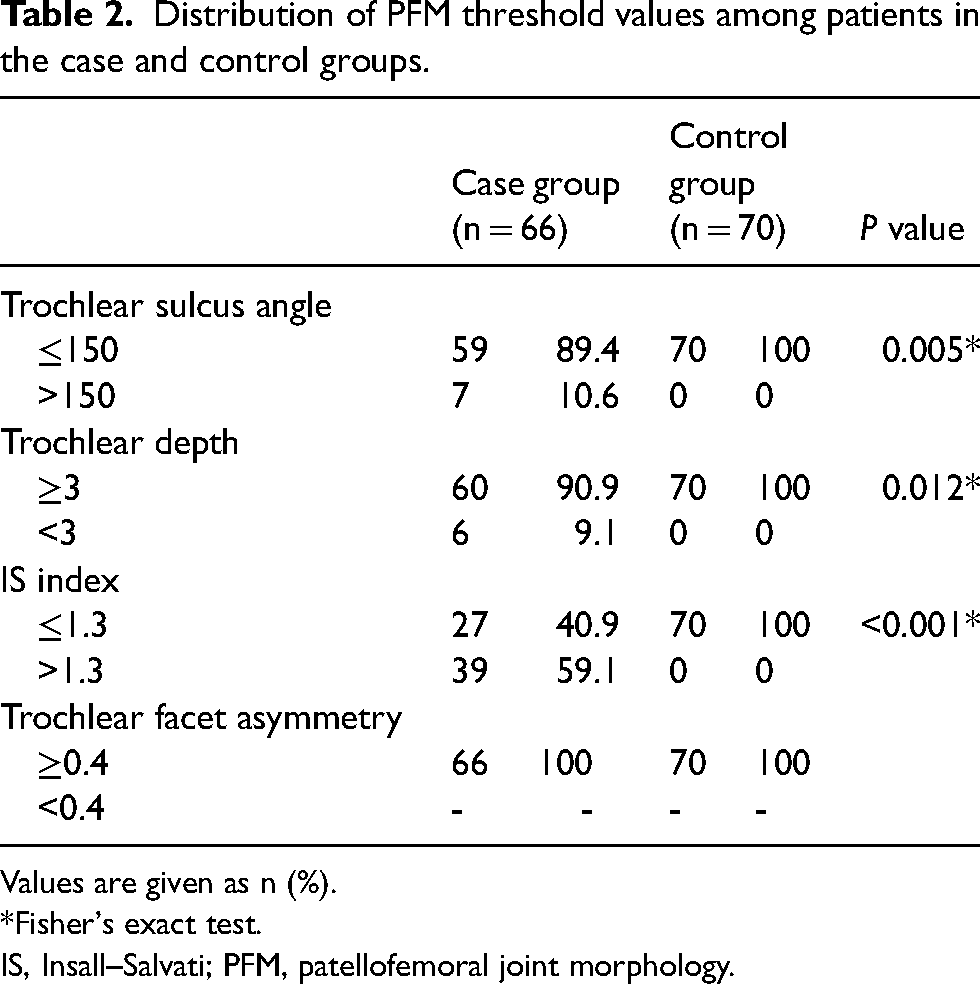
Values are given as n (%).
*Fisher's exact test.
IS, Insall–Salvati; PFM, patellofemoral joint morphology.
Regarding the comparison of the patients with and without chondromalacia, the age of patients was significantly higher in the group with chondromalacia than in the group without chondromalacia (42.80 ± 10.97 vs. 35.89 ± 8.42 years; P < 0.001). The PFM measurements of patients with and without chondromalacia are summarized in Table 3. Regarding the analysis of threshold value distributions used in PFM measurements of patients with and without chondromalacia, we found that the ratio of trochlear sulcus angle >150° (P < 0.05) and IS index >1.3 (P < 0.001) was higher in the group with chondromalacia than in the group without chondromalacia, but no significant difference was found in terms of the rate of trochlear depth being <3 mm (P > 0.05).
Comparison of PFM measurements between patients with and without chondromalacia.
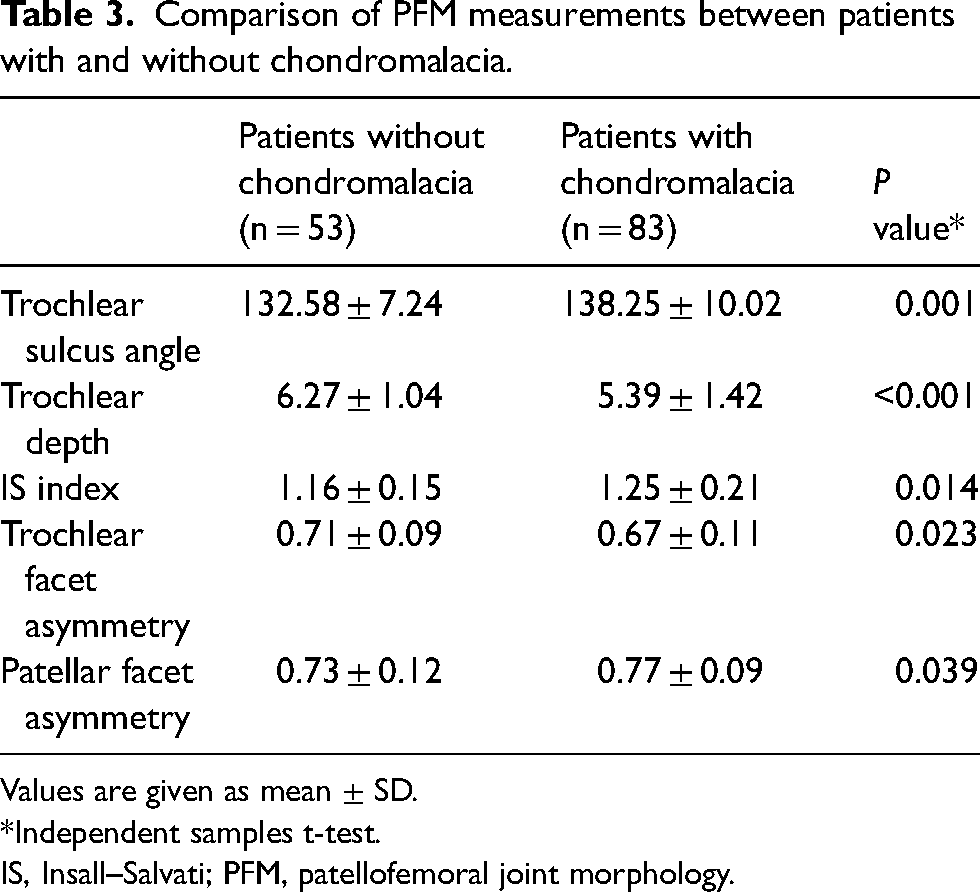
Values are given as mean ± SD.
*Independent samples t-test.
IS, Insall–Salvati; PFM, patellofemoral joint morphology.
Female sex was more common among patients with advanced chondromalacia (P < 0.05). PFM measurement distributions of participants according to chondromalacia grade are shown in Table 4. When the distribution of the threshold values used according to the grade of chondromalacia was analyzed, the rate of trochlear sulcus angle >150° and trochlear depth <3 mm was higher in patients with severe chondromalacia. However, there was no significant difference in the rate of IS index >1.3. Moreover, no significant difference was found between the patients with early-stage chondromalacia and the patients without chondromalacia in terms of the threshold values used for trochlear sulcus angle and trochlear depth.
PFM measurement distributions among patients with chondromalacia of grades 0, 1–2, and 3–4.
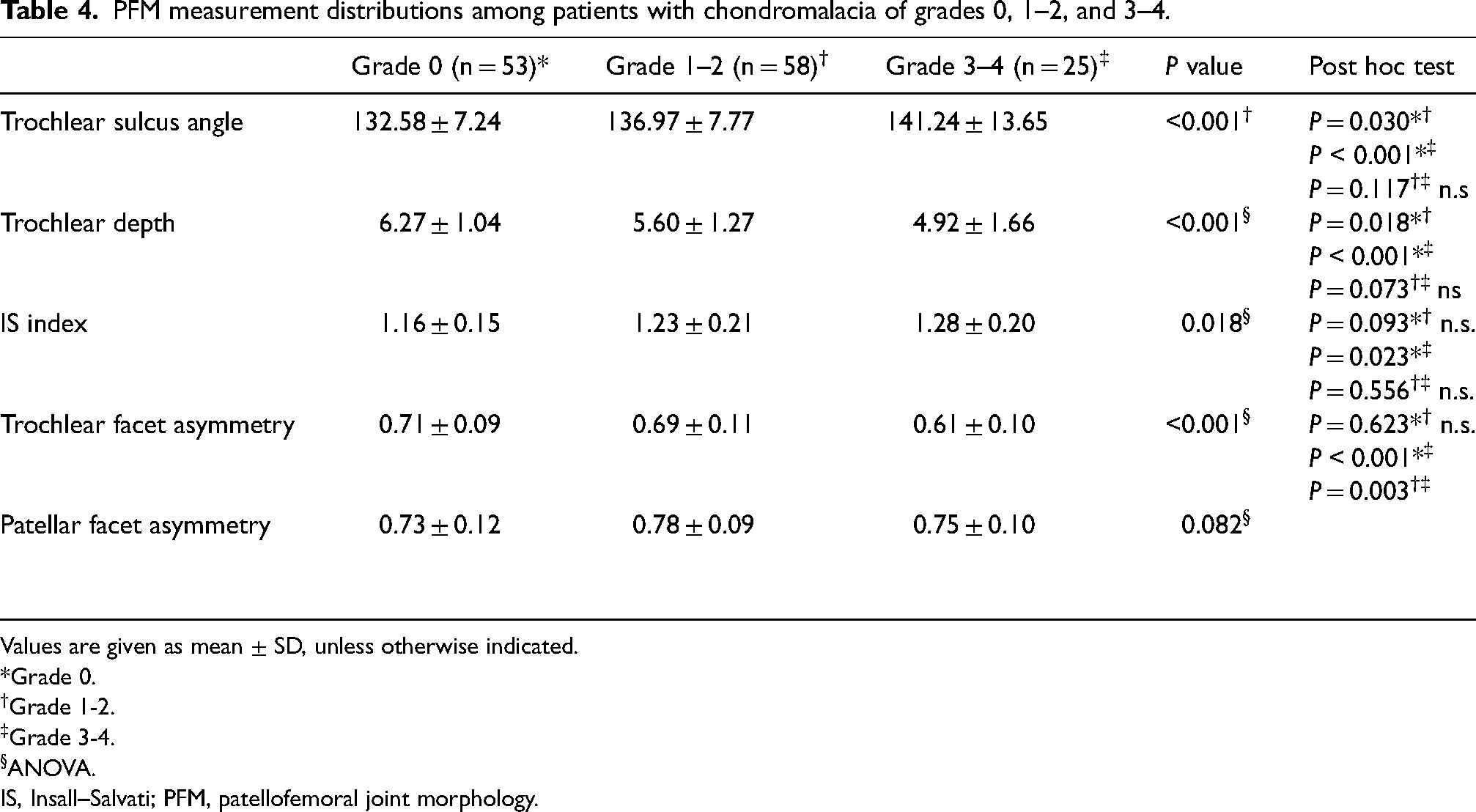
Values are given as mean ± SD, unless otherwise indicated.
*Grade 0.
Grade 1-2.
Grade 3-4.
ANOVA.
IS, Insall–Salvati; PFM, patellofemoral joint morphology.
Discussion
Disruption of the PFM relationship can cause joint instability, patellar chondromalacia, and ultimately PF osteoarthritis (6). In the present study, chondromalacia patella was found to be more frequent and severe in the group with an abnormality based on at least one of the PFM measurements. Regarding the comparison between patients with and without chondromalacia, the trochlear sulcus angle, IS index, and patellar facet asymmetry measurements were statistically significantly higher, whereas the trochlear sulcus depth and trochlear facet asymmetry measurements were statistically significantly lower in the group with chondromalacia. In addition, our study results revealed that the effects of patellar and femoral morphological abnormalities on the severity of chondromalacia were varying.
In the present study, chondromalacia patella was observed more frequently in the group with a pathological result in at least one of the PFM measurements. When we compared the groups with and without chondromalacia, a statistically significant difference was found in all measurements. In contrast to our results, in a study by Endo et al., no correlation was found between the IS index and trochlear depth measurements and the presence of chondromalacia (11). Moreover, no correlation was found between the trochlear sulcus angle and presence of patellar chondromalacia in a study by Yang et al. (12), and there was no correlation between the IS index and the presence of patellar chondromalacia in a study by Tabary et al. (13). However, similar to our results, some studies in the literature reported that the trochlear sulcus angle increases and the sulcus depth decreases in patients with patellar chondromalacia. In a study by Duran et al. involving women with advanced chondromalacia, trochlear morphological measurements and chondromalacia patella were found to be correlated (3). Similarly, other studies investigating the relationship between PFM measurements and chondromalacia reported that the trochlear depth was lower and the trochlear sulcus angle and IS index were higher in the patellar chondromalacia group (4,14). In another study evaluating chondromalacia with cartilage mapping, a relationship between early cartilage damage and trochlear morphological measurements was reported (15).
In the relevant literature, there are limited data regarding the relationship of trochlear and patellar facet asymmetry with chondromalacia patella. In the present study, the value of <0.4 was used as the threshold for trochlear facet asymmetry measurements, but the trochlear facet ratio was not below the threshold value in any patient. However, there was a statistically significant difference in the medial/lateral facet ratio between the case and control groups. The rate of trochlear facet asymmetry was lower and that of patellar facet asymmetry was higher in patients with chondromalacia than in those without chondromalacia. However, in a recent study, contrary to our results, no relationship was found between trochlear facet asymmetry and patellar cartilage defect (16). Moreover, in a study by Resorlu et al., no relationship was found between patellar facet asymmetry and chondromalacia patella (17). We believe that incompatibility due to the asymmetry of opposing articular surfaces may impact cartilage damage, and the fact that results in the literature differ from those of our study may be attributable to the different measurement methods, sex, and age distribution. More extensive anatomical studies on this topic can explain this situation.
In the present study, the factors affecting the stage of chondromalacia were trochlear morphological measurements, whereas there was no significant relationship between the IS index and patellar facet asymmetry. In a study investigating the chondromalacia stage and PFM morphology, it was reported that trochlear morphological measurements were associated with chondromalacia patella, but no significant correlation was found with the IS index (5). Similarly, Ali et al. revealed that trochlear morphological measurements were associated with severe chondromalacia, but no correlation was found between patellar measurements and chondromalacia stage (1). In a study examining chondromalacia patellar and joint morphological measurements in patients with anterior knee pain, in contrast to our results, no significant correlation was found between trochlear measurements and chondromalacia stage in addition to patellar morphological measurements (18). In another study, it was found that the trochlear sulcus angle and trochlear depth as well as female sex were associated with the stage of chondromalacia (4). In the present study, there was no significant difference in sex distribution between the case and control groups, but female sex was more common among patients with advanced stage chondromalacia.
The presents study has some limitations. First, due to the retrospective design of the study, body mass index, clinical, and examination findings were unknown. Hence obesity etc. the effect of clinical conditions on chondromalacia could not be evaluated. Another limitation was MRI was used in the evaluation of chondromalacia, and the arthroscopy results of the cases were not evaluated. A case evaluated as normal using MRI may be diagnosed as early-stage chondromalacia in arthroscopy.
In conclusion, the presence of at least one of the PFM measurements indicating pathology is associated with the presence and severity of chondromalacia. Our results revealed that the rate of manifesting pathological trochlear sulcus angle and trochlear sulcus depth is higher among patients with severe chondromalacia than among those with early-stage chondromalacia. However, there was no significant difference in the rate of having a pathological IS index between patients with mild and severe chondromalacia.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.