
Abstract
Background
Limited studies have investigated the accuracy of therapeutic decision-making using machine learning-based coronary computed tomography angiography (ML-CCTA) compared with CCTA.
Purpose
To investigate the performance of ML-CCTA for therapeutic decision compared with CCTA.
Material and Methods
The study population consisted of 322 consecutive patients with stable coronary artery disease. The SYNTAX score was calculated with an online calculator based on ML-CCTA results. Therapeutic decision-making was determined by ML-CCTA results and the ML-CCTA-based SYNTAX score. The therapeutic strategy and the appropriate revascularization procedure were selected using ML-CCTA, CCTA, and invasive coronary angiography (ICA) independently.
Results
The sensitivity, specificity, positive predictive value, negative predictive value, accuracy of ML-CCTA and CCTA for selecting revascularization candidates were 87.01%, 96.43%, 95.71%, 89.01%, 91.93%, and 85.71%, 87.50%, 86.27%, 86.98%, 86.65%, respectively, using ICA as the standard reference. The area under the receiver operating characteristic curve (AUC) of ML-CCTA for selecting revascularization candidates was significantly higher than CCTA (0.917 vs. 0.866, P = 0.016). Subgroup analysis showed the AUC of ML-CCTA for selecting percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG) candidates was significantly higher than CCTA (0.883 vs. 0.777, P < 0.001, 0.912 vs. 0.826, P = 0.003, respectively).
Conclusion
ML-CCTA could distinguish between patients who need revascularization and those who do not. In addition, ML-CCTA showed a slightly superior to CCTA in making an appropriate decision for patients and selecting a suitable revascularization strategy.
Keywords
Introduction
Coronary computed tomography angiography (CCTA) has been introduced as a reliable method for the first-line diagnostic test in patients with suspected or known coronary artery disease (CAD) in the outpatient, inpatient, or emergency department setting (1,2). Multiple studies have demonstrated that CCTA has a high diagnostic accuracy for obstructive CAD when using invasive coronary angiography (ICA) as a reference standard (3–5). In addition, the characteristics based on CCTA have been proven to be independent risk predictors of cardiovascular events (6).
According to the 2018 European Society of Cardiology/European Association for Cardio-Thoracic Surgery (ESC/EACTS) guidelines, it is critical to identify patients with obstructive CAD who are likely to benefit from myocardial revascularization (7). Yet, limited studies have investigated the accuracy (70%–89.8%) of therapeutic decision-making using CCTA compared with ICA (8–10). Recently, machine learning (ML) algorithms have been developed to both automate the processes and improve the diagnostic performance of cardiovascular imaging (11,12). Moreover, ML can assist doctors with increasing efficiency, reducing errors, and achieving objectives by providing streamlined, time-saving workflows in treatment decision-making (13). We have reported the clinical evaluation of an ML-based CCTA postprocessing and reporting system in patients with suspected CAD (14). The SYNTAX score has been widely advocated as an aided evaluation method in both the U.S and European revascularization guidelines for revascularization strategy (7,15). However, the performance of ML-based CCTA and SYNTAX for therapeutic decision-making requires further investigation. Thus, we sought to investigate the accuracy of ML-CCTA for selecting revascularization candidates compared with CCTA.
Material and Methods
The present study was approved by the local institutional review board and was conducted in compliance with the Health Insurance Portability and Accountability Act (HIPAA) of 1996.
Patients
CCTA and ICA examinations between July 2017 and July 2019 were retrospectively searched in the institution's Picture Archive and Communication System (PACS). Written informed consent was obtained from all participants. The study population consisted of patients with stable CAD with an interval of <30 days between CCTA and ICA were included (Fig. 1). General exclusion criteria were as follows: poor quality images; images that could not be recognized or analyzed by ML (scans affected by stair-step artifacts, respiratory motion artifacts, excessive image noise, or artifacts caused by arrhythmia); incomplete records; previously underwent percutaneous coronary intervention (PCI), coronary artery bypass graft (CABG), or other cardio surgery. Demographic and clinical information on cardiovascular risk factors, including age, sex, body mass index (BMI), symptoms, hypertension, diabetes mellitus (DM), chronic kidney disease (CKD), dyslipidemia, serum creatinine, urea nitrogen, EF, history of chronic obstructive pulmonary disease (COPD), and peripheral vascular disease (PVD), were collected from electronic medical records. History of COPD was defined as the long-term use of bronchodilators or steroids for lung disease. History of PVD was defined as exercise-related claudication or angiographic stenosis of >50% in the aorta or other arteries compared with that in the coronary arteries. Creatinine clearance calculated by using the Cockroft Gault formula was also acquired.
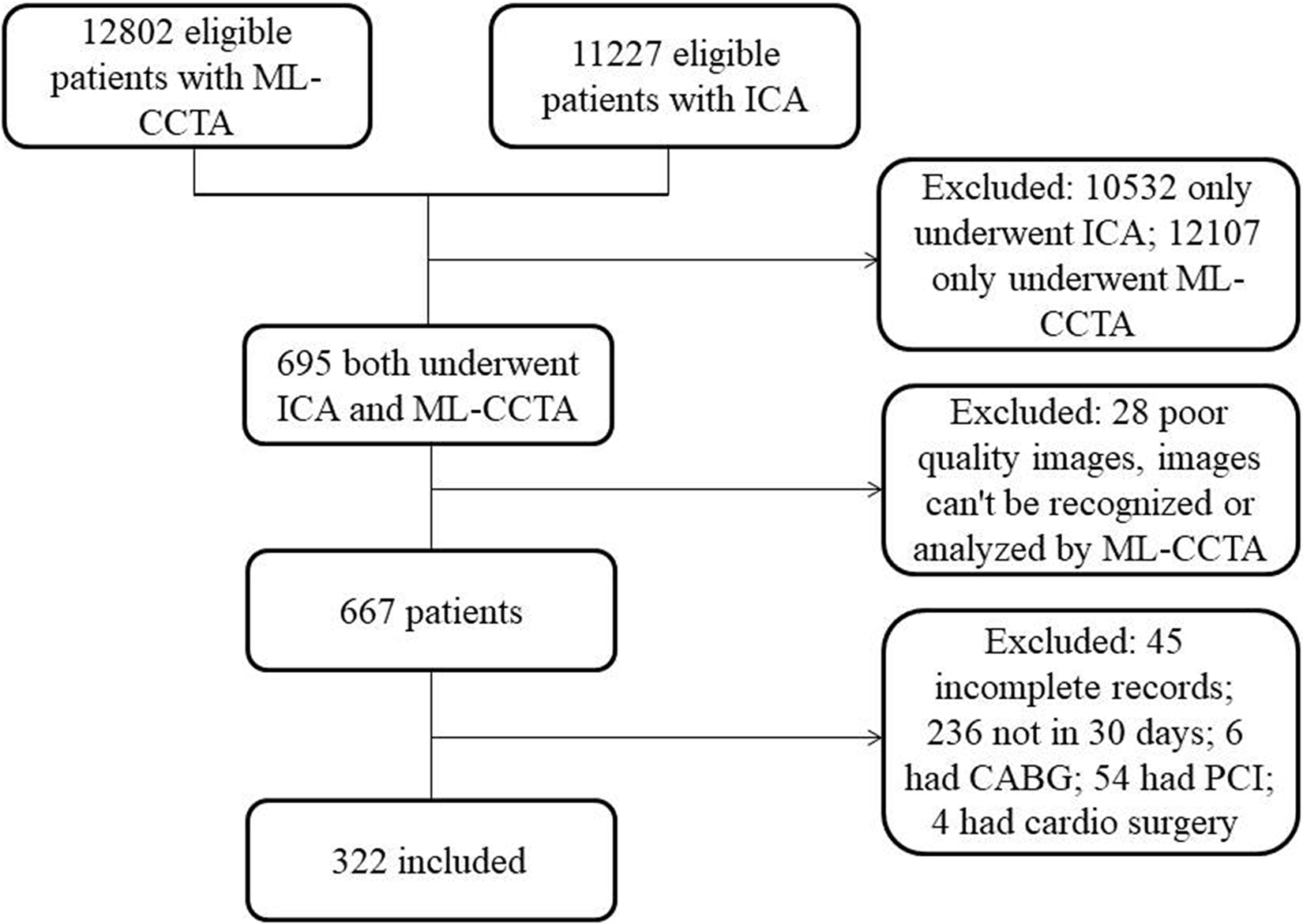
Flow diagram showed the study population. CABG, coronary artery bypass graft; CAD, coronary artery disease; CCTA, coronary computed tomography angiography; ICA, invasive coronary angiography; ML-CCTA, machine learning-based CCTA; PCI, percutaneous coronary intervention.
Criteria for revascularization
We established eligibility criteria for revascularization according to the 2018 ESC/EACTS guidelines (7). Revascularization therapeutic decision-making (PCI or CABG) for the patients with stable CAD was based on the level of evidence and the strength of recommendation. We considered the higher class of recommendation and level of evidence was the better revascularization therapeutic decision in this study. For example, CABG (I B) was the better revascularization therapeutic decision for a two-vessel CAD patient with proximal left anterior descending coronary artery (LAD) stenosis rather than PCI (I C). If the class of recommendation and level of evidence were both the same for CABG and PCI, either type would be the revascularization therapeutic decision. Based on these considerations, the therapeutic recommendation decision for the type of revascularization in patients with stable CAD is shown in Table 1. The SYNTAX score was an anatomical complexity of coronary lesions scoring system to evaluate the extent of CAD (16). The SYNTAX score was calculated by online calculator (www.syntaxscore.com/calculator/start.htm; version 2.28).
Therapeutic recommendation decision for the type of revascularization in patients with stable CAD.
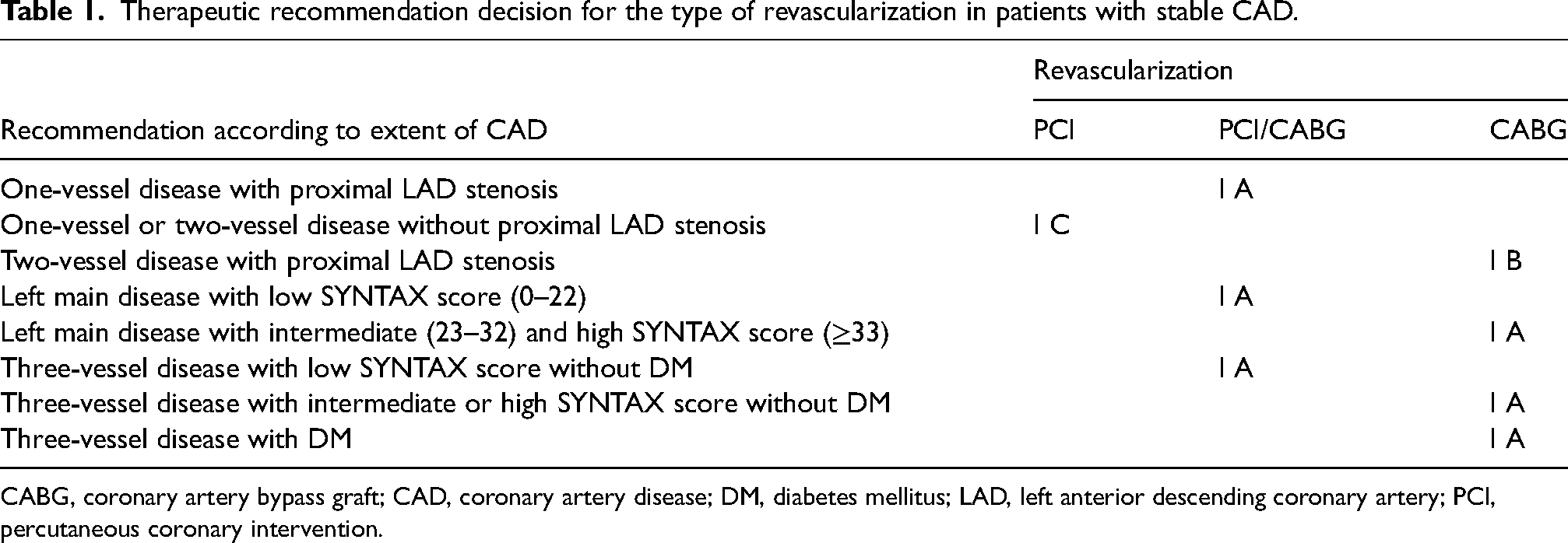
CABG, coronary artery bypass graft; CAD, coronary artery disease; DM, diabetes mellitus; LAD, left anterior descending coronary artery; PCI, percutaneous coronary intervention.
CCTA and ML-CCTA studies
Multidetector-row CT imaging was performed with a dual-source CT scanner (Somatom Definition, Siemens Medical Solutions, Forchheim, Germany) and a 256-slice CT scanner (Brilliance iCT; Philips Healthcare, Best, the Netherlands) which has been reported previously (17,18). Heart rate control (HR ≥65 beats/min) was performed with beta-blockers before the scan. For contrast enhancement, 60–80 mL of iopromide (370 mgI/mL, Bayer Schering Pharma, Leverkusen, Germany) followed by 30–40 mL of pure saline with a flow rate of 4–5 mL/s. The scan will automatically commence during an inspiratory breath hold of 8–14 s after a delay of 2 s when the density in the region of interest (descending aorta) rises to a preset value (100 HU).
CCTA images were sent to one of the two workstations for postprocessing: Intelligence space portal (Version 6.0.4, Philips Medical Systems, Best, the Netherlands) and SyngoVIA (Siemens Medical Solutions, Forchheim, Germany). The postprocessing includes transaxial 2D image stacks, multiplanar reformations (MPR), maximum intensity projections (MIP), curved multiplanar reformations (cMPR), and volume rendering technique (VRT) reconstructions according to the JCCT guideline (19). Three radiologists (blinded to the patients’ history, ML-CCTA and ICA results, the dataset split up between them) with 5 (YD), 10 (SCZ), and 16 (JWX) years of experience in cardiac CT evaluated the CCTA images (Fig. 2). The coronary arteries with a diameter ≥2 mm were evaluated for luminal narrowing. The standardized Coronary Artery Disease-Reporting and Data System (CAD-RADS) classification was reported in our recent researches (14,18,20).
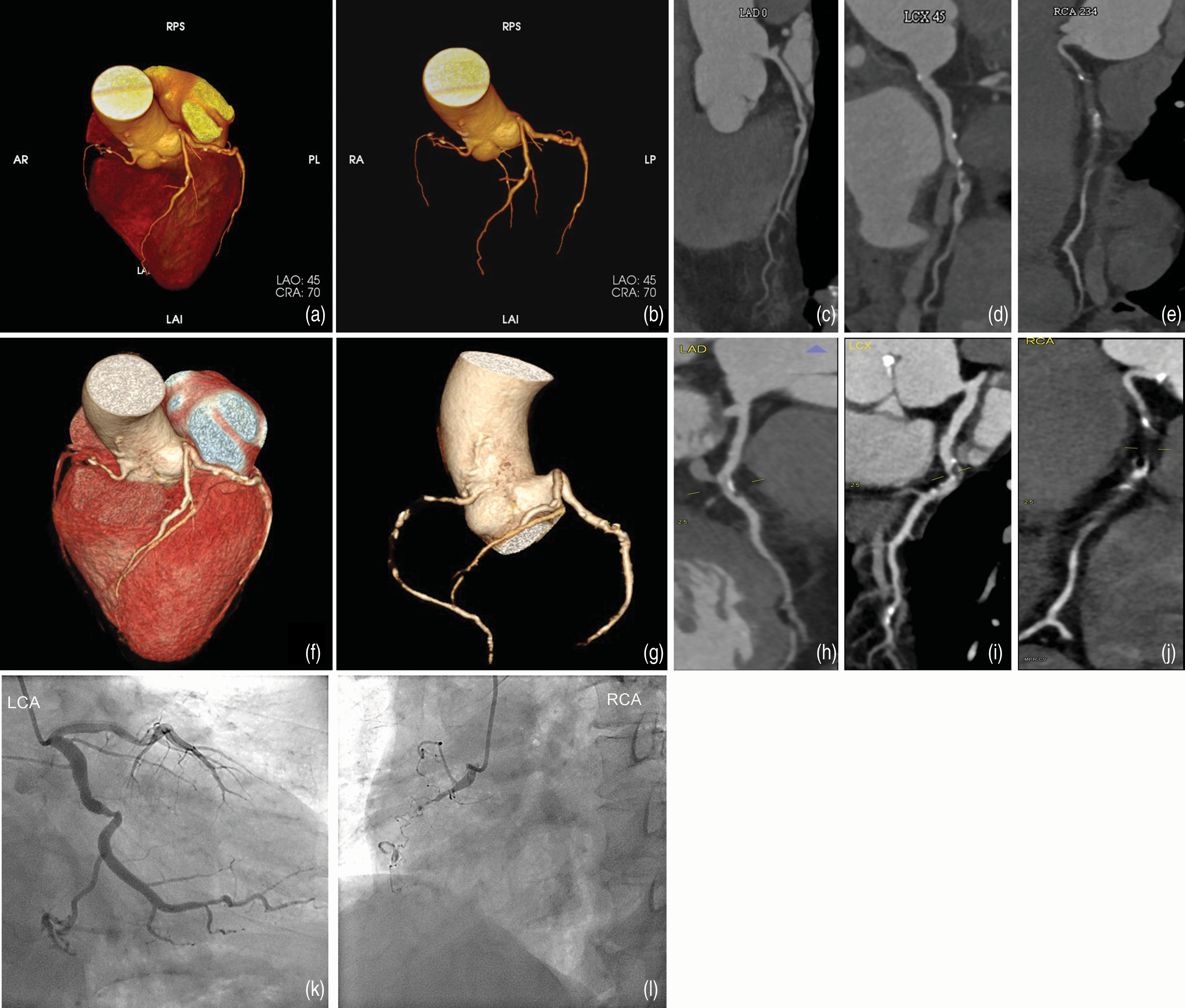
(a–e) Lesions showed in ML-CCTA, multidetector-row CCTA, and ICA. ML-CCTA showed mild stenosis in LAD (7 segments), severe stenosis in LCX (11 segments), and occlusion in RCA (2 segments). (f–j) Multidetector-row CCTA showed the same pictures and these coronary lesions were confirmed on (k, l) ICA. CCTA, coronary computed tomography angiography; ICA, invasive coronary angiography; LAD, left anterior descending coronary artery; LCX, left circumflex coronary artery; ML-CCTA, machine learning-based CCTA; RCA, right coronary artery.
ML-CCTA calculations were performed by one radiologist (ZFH) using a software prototype (CoronaryDoc, version 1.5, Shukun Technology, Beijing, China), which has been described previously (14,18,21). The software is based on an artificial intelligence ML platform for standardized postprocessing and structured reporting using CCTA data (Supplementary Figures 1–3).
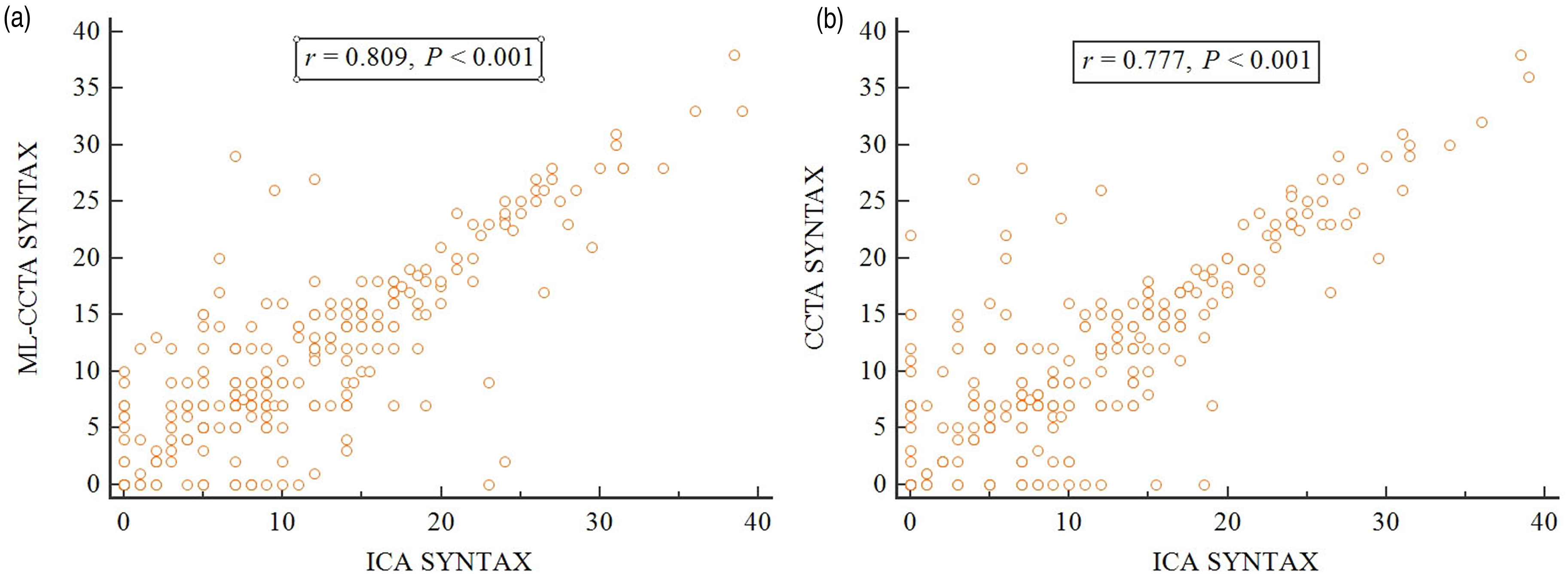
Correlation between SYNTAX scores. (a) Correlation between the ML-CCTA-based SYNTAX score and the ICA-based SYNTAX score. (b) Correlation between the CCTA-based SYNTAX score and the ICA-based SYNTAX score. CCTA, coronary computed tomography angiography; ICA, invasive coronary angiography; ML-CCTA, machine learning-based CCTA; SYNTAX, The Synergy between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery.
Invasive coronary angiography
ICA was performed according to standard practice by a group of experienced interventional cardiologists. Coronary stenosis was evaluated by visual estimation (stenosis ≥50%, XW was blinded to the patients’ history, CCTA and ML-CCTA results) and the decision of whether or not to proceed with revascularization and which revascularization to perform were based on invasive angiographic assessment and the ICA-based SYNTAX score.
Therapeutic decision-making
Standardized postprocessing and structured reporting including CAD-RADS using CCTA data was created based on the ML algorithm. The SYNTAX score was calculated with an online calculator based on ML-CCTA results. Therapeutic decision-making was determined by a team with experienced cardiologists based on the ML-CCTA results and ML-CCTA-based SYNTAX score. Then, another team was asked to determine the treatment strategy based on the CCTA results and CCTA-based SYNTAX score, which was blinded to the treatment strategy of ML-CCTA. The treatment strategy was recorded as coronary revascularization (PCI or CABG) and/or optimal medical treatment for ML-CCTA, CCTA, and ICA, respectively.
Statistical analysis
Continuous variables were presented as mean ± SD. Categorical variables were presented as percentages or absolute values. We used either the chi-square test or Fisher's exact test, as appropriate, for categorical variables and one-way ANOVA test for continuous variables. The correlation between the SYNTAX scores calculated from ML-CCTA, CCTA, and ICA was analyzed using Spearman’s correlation coefficient. Designed as a diagnostic test, the performance of ML-based CCTA for selecting revascularization candidates was determined as sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy. P < 0.05 was considered as statistically significant. All statistical analysis was performed using SPSS version 18 (SPSS, Inc., Chicago, IL, USA) and MedCalc Statistical Software version16.8.4.0 (Ostend, Belgium).
Results
The study population included 190 men and 132 women (mean age = 63.8 years; age range = 35–87 years). The baseline characteristics of the study patients were summarized in Table 2. There was no significant difference among the patients who fulfilled CABG surgery criteria based on CCTA, ML-CCTA, or ICA. In addition, there was no significant difference among the patients who fulfilled PCI criteria based on CCTA, ML-CCTA, or ICA.
Basic characteristics of the study patients.
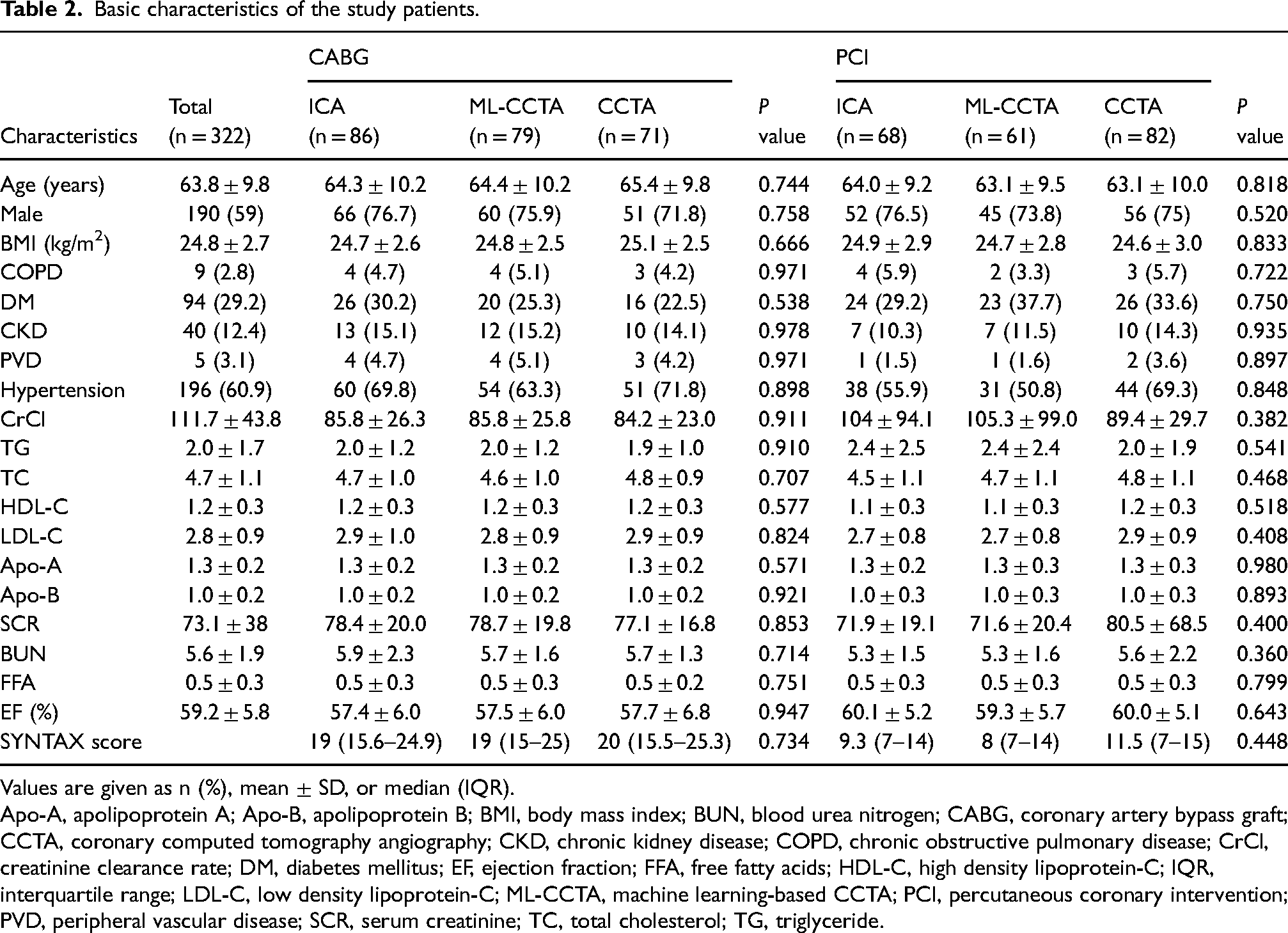
Values are given as n (%), mean ± SD, or median (IQR).
Apo-A, apolipoprotein A; Apo-B, apolipoprotein B; BMI, body mass index; BUN, blood urea nitrogen; CABG, coronary artery bypass graft; CCTA, coronary computed tomography angiography; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CrCl, creatinine clearance rate; DM, diabetes mellitus; EF, ejection fraction; FFA, free fatty acids; HDL-C, high density lipoprotein-C; IQR, interquartile range; LDL-C, low density lipoprotein-C; ML-CCTA, machine learning-based CCTA; PCI, percutaneous coronary intervention; PVD, peripheral vascular disease; SCR, serum creatinine; TC, total cholesterol; TG, triglyceride.
Correlation of SYNTAX score and CAD-RADS classification
There was a strong correlation between the ML-CCTA-based SYNTAX score and the ICA-based SYNTAX score (Spearman’s correlation coefficient, r = 0.809; P < 0.001) (Fig. 3a). Similarly, a strong correlation was found between the CCTA-based SYNTAX score and the ICA-based SYNTAX score (Spearman’s correlation coefficient, r = 0.777; P < 0.001) (Fig. 3b) (Supplementary Figure 4). In addition, we also found a strong correlation between the ML-CCTA-based CAD-RADS classification and CCTA-based CAD-RADS classification (intraclass correlation coefficient = 0.879; P < 0.001) (Supplementary Table 1).
Diagnostic accuracy of ML-CCTA and CCTA for selecting revascularization candidates
A total of 154 patients fulfilled the revascularization criteria using ICA as standard diagnostic tool, 140 patients met the criteria using ML-CCTA, and 153 patients met the criteria using CCTA. The sensitivity, specificity, PPV and NPV, and accuracy of ML-CCTA for selecting revascularization candidates were 87.01%, 96.43%, 95.71%, 89.01%, and 91.93% respectively. The sensitivity, specificity, PPV and NPV, and accuracy of CCTA for selecting revascularization candidates were 85.71%, 87.50%, 86.27%, 86.98%, and 86.65%, respectively. The area under the receiver operating characteristic (ROC) curve (AUC) of ML-CCTA for selecting revascularization candidates was significantly higher than CCTA (0.917, 95% confidence interval [CI] = 0.882–0.945 vs. 0.866, 95% CI = 0.824–0.901; P = 0.016) (Fig. 4). The data were summarized in Table 3. The clinical workup would be changed in 10.1% (17/169) of patients from optimal medical treatment to revascularization and 19.6% (30/153) of patients from revascularization to optimal medical treatment if they only used ML-CCTA when compared with CCTA. As a result, it would slightly underestimate the number of patients who need revascularization compared to CCTA.
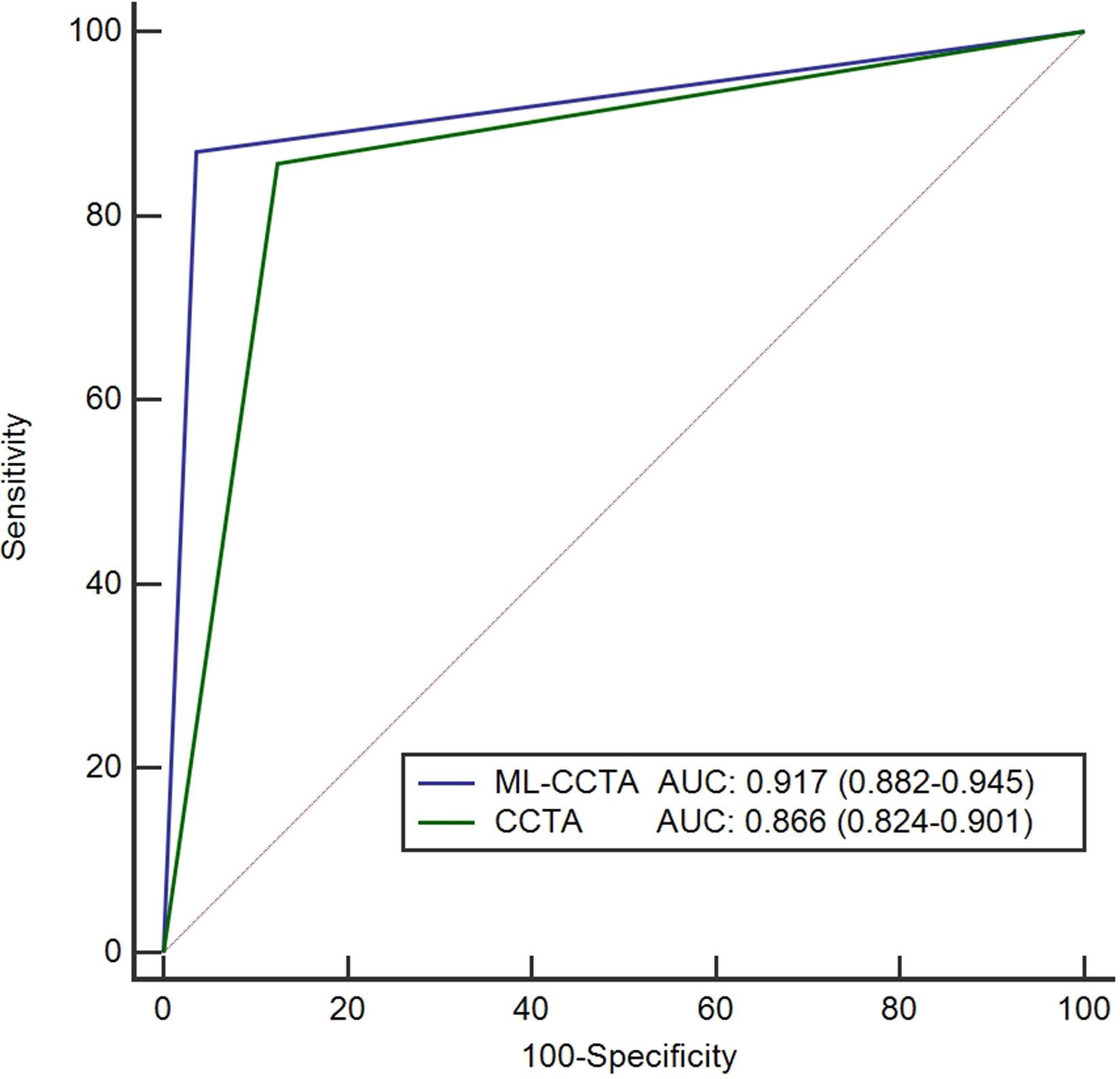
ROC curves for selecting revascularization candidates. AUC, area under curve; CCTA, coronary computed tomography angiography; ML-CCTA, machine learning-based CCTA; ROC, receiver operating characteristic.
Diagnostic accuracy of CCTA and ML-based CCTA for selecting revascularization candidates.

AUC, area under the curve; CCTA, coronary computed tomography angiography; FN, false negative; FP, false positive; ML, machine learning; ML-CCTA, machine learning-based coronary computed tomography angiography; NPV, negative predictive value; PPV, positive predictive value; TN, true negative; TP, true positive.
Diagnostic accuracy of ML-CCTA and CCTA for selecting the method of revascularization with candidates
Table 4 shows the diagnostic accuracy of the two procedures for selecting the method of revascularization with candidates. A total of 68 patients fulfilled the PCI criteria using ICA as a standard diagnostic tool, 61 patients met the criteria using ML-CCTA, and 82 patients met the criteria using CCTA. The sensitivity, specificity, PPV and NPV, and accuracy of ML-CCTA for selecting PCI candidates were 79.41%, 97.24%, 88.52%, 94.64%, and 93.48%, respectively. The sensitivity, specificity, PPV and NPV, and accuracy of CCTA for selecting PCI candidates were 69.12%, 86.22%, 57.32%, 91.25%, and 82.61%, respectively. The AUC of ML-CCTA for selecting PCI candidates was significantly higher than CCTA (0.883, 95% CI = 0.843–0.916 vs. 0.777, 95% CI = 0.727–0.821; P < 0.001) (Fig. 5a).
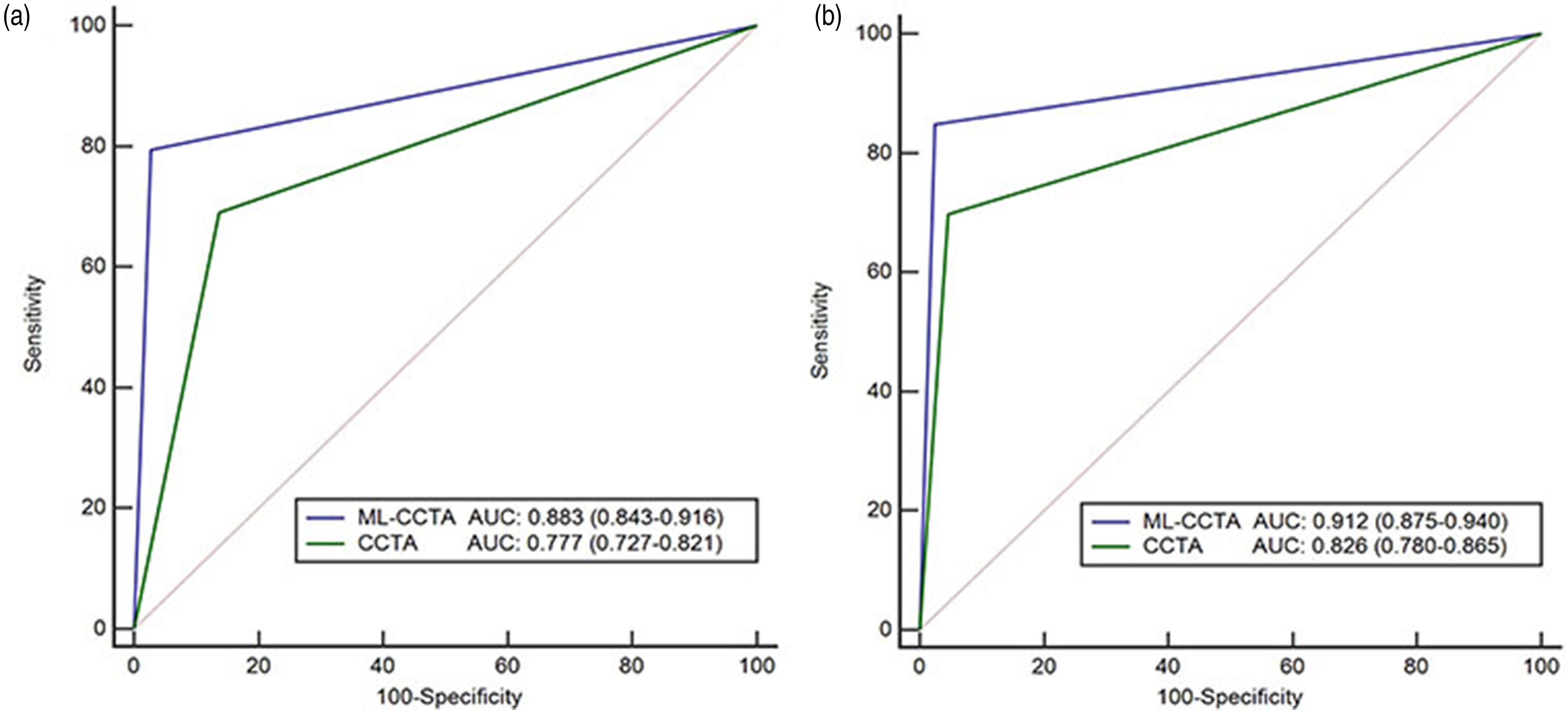
ROC curves for selecting method of revascularization with candidates. (a) ROC curves for selecting PCI candidates. (b) ROC curves for selecting CABG candidates. AUC, area under curve; CCTA, coronary computed tomography angiography; ML-CCTA, machine learning-based CCTA; ROC, receiver operating characteristic.
Diagnostic accuracy of CCTA and ML-based CCTA for selecting method of revascularization with candidates.
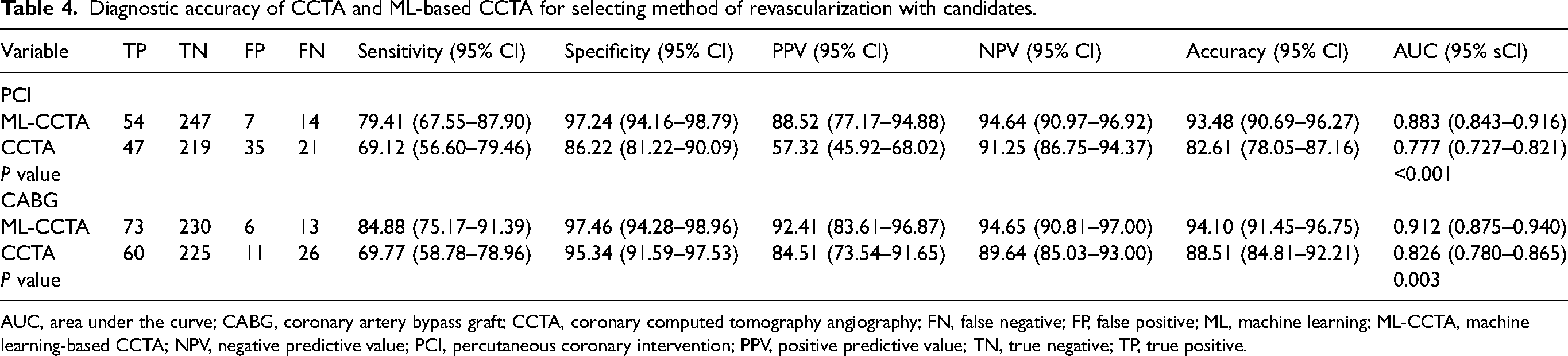
AUC, area under the curve; CABG, coronary artery bypass graft; CCTA, coronary computed tomography angiography; FN, false negative; FP, false positive; ML, machine learning; ML-CCTA, machine learning-based CCTA; NPV, negative predictive value; PCI, percutaneous coronary intervention; PPV, positive predictive value; TN, true negative; TP, true positive.
In total, 86 patients fulfilled the CABG surgery criteria using ICA as a standard diagnostic tool, 79 patients met the criteria using ML-CCTA, and 71 patients met the criteria using CCTA. The sensitivity, specificity, PPV and NPV, and accuracy of ML-CCTA for selecting CABG candidates were 84.88%, 97.46%, 92.41%, 94.65%, and 94.10%, respectively. The sensitivity, specificity, PPV and NPV, and accuracy of CCTA for selecting CABG candidates were 69.77%, 95.34%, 84.51%, 89.64%, and 88.51%, respectively. The AUC of ML-CCTA for selecting CABG candidates was significantly higher than CCTA (0.912, 95% CI = 0.875–0.940 vs. 0.826, 95% CI = 0.780–0.865; P = 0.003) (Fig. 5b).
Treatment with follow-up
In addition to the accuracy investigation, we further followed the real treatment of the included patients to provide more details for the outcome of the patients. During the follow-up (mean = 4.6 months; range = 0–16 months), 15 of the 322 patients underwent CABG surgery, 122 underwent PCI, and 185 received optimal medical treatment. However, there are significant differences between treatment decisions based on ML-CCTA, CCTA, or ICA and real treatment (Supplementary Table 2).
Discussion
The present study demonstrated that ML-based CCTA could distinguish between patients who need revascularization and those who do not. In addition, ML-based CCTA showed a better performance than CCTA in making an appropriate decision for patients and selecting a suitable revascularization strategy following the 2018 ESC/EACTS Guidelines on myocardial revascularization.
Previous studies showed that CCTA-based CABG candidate selection exhibited high diagnostic accuracy with a sensitivity of 83.3%–96.5%, specificity of 90.9%–97.3%, PPV of 88.3%–93.8%, and NPV of 90.7%–98.6% (10,22–24). The specificity, NPV, and accuracy of CCTA- or ML-CCTA-based CABG candidate selection in the present study were comparable to those of previous studies. However, the sensitivity and PPV of CCTA were relatively low. This may have been partly because of the different CABG surgery guidelines used (ACC/AHA 2004 guideline update for coronary artery bypass graft surgery, 2011 ACCF/AHA CABG surgery guidelines, and 2014 ESC/EACTS guidelines). CABG surgery selection criteria in the 2018 ESC/EACTS guidelines we used had some changes: three-vessel CAD with diabetes mellitus was recommended for CABG surgery. Moreover, two-vessel disease with proximal LAD stenosis was also recommended for CABG surgery in the present study. The results of the present study demonstrated that ML-CCTA performed more accurately in identifying patients with or without the need for revascularization compared to CCTA, using ICA as the reference standard.
Recently, Tesche et al. (25) reported the use of a machine learning algorithm-based CT-FFR value to assess the functional significance of CAD and make the therapeutic decision. They showed excellent performance (sensitivity of 97%, specificity of 100%, PPV of 100%, NPV of 97%, and accuracy of 99%) of ML-based CT-FFR with CCTA in determining the appropriate treatment strategy. However, the use of FFR or CT-FFR remains limited in China, France, and the United States (26–28). In China, FFR measurement costs an extra 10,000 Yuan and financial support is still lacking (26). Moreover, as the only clinical and commercial CT-derived FFR evaluation product that has been proved by the FDA, HeartFlow FFRCT requires transmission of CT datasets to its offsite core laboratory, which requires 8 h for processing and analysis and costs up to $1500 without any guarantee of reimbursement (29). In addition, the requisite offsite handling of sensitive and confidential patient information and associated medical conditions is a highly delicate issue involving IT security, potential for data abuse, etc. (30).
ML has been increasingly applied across the diagnostic and prognostic applications of CAD (31–34). However, most of those previous studies did not consider decisions regarding the selection of a treatment strategy. The principal focus of our study was to compare our ML-CCTA-based decision-making with CCTA-based decision-making. We found that the ML-CCTA-based program was superior to the CCTA-based method for both appropriateness of revascularization and determining the treatment strategy when considering ICA as the reference standard.
The prognostic value of the SYNTAX score has been extensively discussed. However, the low intra- and inter-observer reproducibility of the SYNTAX score has been clearly reported (35). ML assistance could result in higher inter-observer reproducibility (36). The correlation between ML-CCTA-based SYNTAX score and ICA-based SYNTAX score was strong, and slightly higher than that between CCTA-based SYNTAX score and ICA-based SYNTAX score in the present study and previous studies (23,37,38). To the best of our knowledge, the present study is the first to analyze the value of ML-CCTA-based SYNTAX score for selecting revascularization strategy candidates who underwent diagnostic imaging.
CAD-RADS can now provide guidance on clinical decision-making through non-invasive imaging and may play an important role in the bridge between test abnormalities and optimal patient care. The recent multinational CONFIRM study suggested that incorporating CAD-RADS into CCTA reports might provide a novel opportunity to promote evidence-based care after CCTA (39). A strong correlation was shown between the ML-CCTA-based CAD-RADS classification and CCTA-based CAD-RADS classification in the present study. In addition, the CAD-RADS scoring system based on ML was faster, more objective, and repeatable in determining CAD-RADS grades by measuring stenosis degree compared to manual measurement. A previous study demonstrated that a structured reporting platform with automated calculation of the CAD-RADS score might improve data quality and support the standardization of clinical decision-making (40). However, this reporting platform automatically determined the CAD-RADS category that should be based on the data provided by the readers, although that remained hidden to the readers.
The present study has some limitations. First, revascularization candidates who were selected on the basis of ICA, ML-CCTA, or CCTA did not reflect real revascularization data according to the results of the follow-up. Setting up which decision is the right one would be more challenging but would actually provide the value of the decision made by comparison with patient outcomes. Some patients who fulfilled the revascularization criteria underwent optimal medical treatment instead of revascularization, possibly because of the patient's or physician's preference, cost, co-morbidity issues, or other clinical considerations, such as the burden of ischemia. In addition, the functional information of the coronary artery is needed in decision-making for the revascularization strategy. Multidisciplinary decision-making in a Heart Team is needed to analyze and interpret the available diagnostic evidence, determine the need for myocardial revascularization, and assess the relative short- and long-term safety and efficacy of the percutaneous and surgical options (7). Second, we did not include patients with stents, grafts, or other cardio surgeries. Third, hemodynamic evaluation was not performed in the present study and the long-term prognostic value of ML-CCTA-based decision-making remains to be further investigated. Forth, two different teams made the decisions for CCTA and ML-CCTA, respectively, without taking into account the inter-reader variability. Finally, in this study, only patients with CCTA referred for ICA were included, meaning that they had an abnormal CCTA or other characteristics that increases the a priori risk of CAD requiring revascularization. This does not represent the general population who undergo CCTA in whom the a priori risk of revascularization is lower. To properly evaluate the accuracy of ML-CCTA, all patients who underwent CCTA should be included. Therefore, the current numbers will be biased.
In conclusion, ML-CCTA could distinguish between patients who need revascularization and those who do not. In addition, ML-CCTA was slightly superior to CCTA in making an appropriate decision for patients and selecting a suitable revascularization strategy.
Supplemental Material
sj-docx-1-acr-10.1177_02841851231158730 - Supplemental material for Performance of machine learning-based coronary computed tomography angiography for selecting revascularization candidates
Supplemental material, sj-docx-1-acr-10.1177_02841851231158730 for Performance of machine learning-based coronary computed tomography angiography for selecting revascularization candidates by Zengfa Huang, Yi Ding, Yang Yang, Shengchao Zhao, Shutong Zhang, Jianwei Xiao, Chengyu Ding, Ning Guo, Zuoqin Li, Shiguang Zhou, Guijuan Cao and Xiang Wang in Acta Radiologica
Supplemental Material
sj-docx-2-acr-10.1177_02841851231158730 - Supplemental material for Performance of machine learning-based coronary computed tomography angiography for selecting revascularization candidates
Supplemental material, sj-docx-2-acr-10.1177_02841851231158730 for Performance of machine learning-based coronary computed tomography angiography for selecting revascularization candidates by Zengfa Huang, Yi Ding, Yang Yang, Shengchao Zhao, Shutong Zhang, Jianwei Xiao, Chengyu Ding, Ning Guo, Zuoqin Li, Shiguang Zhou, Guijuan Cao and Xiang Wang in Acta Radiologica
Supplemental Material
sj-docx-3-acr-10.1177_02841851231158730 - Supplemental material for Performance of machine learning-based coronary computed tomography angiography for selecting revascularization candidates
Supplemental material, sj-docx-3-acr-10.1177_02841851231158730 for Performance of machine learning-based coronary computed tomography angiography for selecting revascularization candidates by Zengfa Huang, Yi Ding, Yang Yang, Shengchao Zhao, Shutong Zhang, Jianwei Xiao, Chengyu Ding, Ning Guo, Zuoqin Li, Shiguang Zhou, Guijuan Cao and Xiang Wang in Acta Radiologica
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Scientific Research Project of the Wuhan Municipal Health Commission (WX2019B02 and WX20D49).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.