
Abstract
Background
Chronic low back pain secondary to degenerative changes in the spine is a common cause of disability, and disc degeneration is one of the most frequent imaging findings. Intervertebral vacuum phenomenon (IVP) is usually observed in advanced degeneration. Recently, this phenomenon has gained interest due to a relatively new surgical technique called percutaneous discoplasty, aimed at treating low back pain secondary to degenerative disc disease in elderly patients.
Purpose
To analyze the prevalence and related factors of the vacuum phenomenon in adult patients.
Material and Methods
A retrospective cohort study was performed of patients who underwent abdominal computed tomography (CT) for non-spine-related reasons. Age, body mass index, smoking, and CT-based characteristics as presence of IVP, subchondral sclerosis, and facet joint degeneration at the lumbar spine from L1 to the sacrum were included in order to determine the prevalence of the vacuum phenomenon in this population and establish a relationship between this condition and patient demographics and other signs of spine degeneration, such as sclerosis and facet joint disease.
Results
A total of 238 patients were included in the study (114 men, 124 women; mean age = 75.6 ± 12.3 years. In total, 91 (38%) patients had at least one level of IVP; 59 (25%) patients exhibited subchondral sclerosis, and 235 (98%) facet joint degeneration. Among risk factors, age, smoking, and subchondral sclerosis were significantly associated with the presence of vacuum.
Conclusion
IVP was present in 38% of participants. Risk factors associated with vacuum were age, smoking, and subchondral sclerosis.
Keywords
Introduction
Low back pain is a common cause of disability and non-permanent incapacity in the world with a negative impact on patients’ quality of life and healthcare systems (1,2).
The prevalence of back pain among elderly patients is expected to increase due to the aging population and degenerative spinal conditions, such as de novo scoliosis, degenerative spondylolisthesis, and spinal stenosis (3,4).
Among degenerative changes in the spine, degenerative disc disease (5), facet joint osteoarthritis (6), and lumbar spinal stenosis are the most common anatomical findings (7). As the discs continue their degenerative process, some patients develop intervertebral vacuum phenomenon (IVP), a relatively common finding, especially with advanced degeneration (8). The role of the vacuum phenomenon as a potential cause of pain is controversial; while this imaging finding had only descriptive importance decades ago, new studies correlate the presence of IVP with intersomatic vertical instability and foraminal stenosis (9,10). In addition, this relatively new concept of IVP as a pain generator promoted the development of a new surgical treatment called percutaneous cement discoplasty (PCD), also known as percutaneous intervertebral-vacuum polymethylmethacrylate injection (PIPI), a minimally invasive procedure intended to fill the empty vacuum disc with polymethyl methacrylate (PMMA), acting as an intervertebral spacer providing vertical stability and indirect foraminal decompression to treat low back pain and radicular pain in elderly patients (11–16).
The prevalence of IVP has been studied in patients with low back pain. The primary aim of the present study was to analyze the tomographic prevalence of IVP along with other degenerative changes as facet joint degeneration (FJD) and subchondral sclerosis in patients who underwent CT in the emergency department (ED) of our institution for reasons unrelated to back pain. In addition, we analyzed the baseline factors that could influence the prevalence and severity of IVP and FJD such as age, sex, body mass index (BMI), and active smoking.
Material and Methods
A retrospective cohort study was performed of patients who underwent abdominal CT at our ED in our institution between March and May 2022. This study was first registered and approved by the protocol and investigation evaluation committee of our institution (CEPI); personal patient data were anonymized before the analysis.
We included patients aged >50 years who underwent an abdominal CT scan at our ED in our institution with no active low back pain nor radicular leg pain, and who had not received epidural/facet joint injections, or physical therapy for spine reasons in the last six months. A sample size calculation was performed with the Power and (The R Project for Statistical Computing, Vienna, Austria) Precision version 4 software before the data analysis; for an estimated IVP prevalence of 20% according to the previous literature, 180 patients were necessary. In order to obtain a major sample size power, the authors decided to include 238 patients.
Patients with a previous history of lumbar surgery, active infection or tumor in the spine, or lumbar trauma within the last year of consultation were excluded.
Baseline characteristics, such as age, sex, BMI, and active smoking, were recorded.
Tomographic measurements were performed at the lumbar spine from L1 to the sacrum on each patient using sagittal, coronal, and axial views.
The presence of the vacuum phenomenon was recorded. To analyze severity, positive IVP was classified as minimal, partial, and total vacuum phenomenon according to the classification by Camino-Willhuber et al. (17) (Fig. 1). In this regard, a minimal vacuum phenomenon is considered if the vacuum/disc ratio is <1, partial vacuum is considered if the vacuum/disc ratio is approximately 1, and total vacuum is considered if the vacuum/disc ratio is >1. The presence of subchondral sclerosis was also taken from this classification, which defined subchondral sclerosis as the presence of increased radiodensity with at least one-third of the vertebral body adjacent to the level analyzed.
FJD was classified according to the classification by Weishaupt et al. (18). Grade 0 was defined as a normal facet joint space with 2–4 mm of regular facet surface, grade 1 was defined as a narrowing of the facet joint (<2 mm) with small osteophytes, grade 2 was defined as the presence of moderate osteophytes and facet joint hypertrophy, and grade 3 was defined as a severe narrowing of the facet joint with large osteophytes and/or the presence of bony erosion and/or subchondral cyst. Measurements were performed before the tomographic analysis by three assessors (SV, LC, and EM), who received an online training session explaining the classifications with case-based examples and all questions/concerns were resolved. In addition, the inter-observer reliability of those measurements was assessed with a Kappa coefficient (k) value of 0.81 (95% confidence interval [CI] = 0.28–1.27).
The primary aim of the present study was to evaluate the proportion of IVP in patients who underwent a CT scan for reasons not related to back pain. For this outcome, we calculated the proportion of the event (IVP) related to the total number of CT scans; the 95% CI was calculated with the exact binomial distribution
As a secondary aim, we evaluated the relationship between the presence or absence of IVP and the patients' demographics, such as age, sex, BMI, and smoking. In this regard, we performed a multivariate analysis of risk factors.
Outcomes were analyzed utilizing univariate analysis based upon baseline demographics and radiological variables. Comparisons were performed using chi-square tests, Fisher's exact tests, or Student t-tests. Results from regression analyses have been reported as adjusted odds ratio (OR) with their respective 95% CIs and P values. A P value <0.05 was considered significant. All statistical analyses were conducted using SPSS version 17 (SPSS, Chicago, IL, USA).
Results
Baseline characteristics
A total of 238 patients (114 men, 124 women; mean age = 75.6 ± 12.3 years; mean BMI = 25 ± 5.6 kg/m2) were finally included in the study. Table 1 illustrates baseline characteristics. Overall, 1190 levels were analyzed (five levels in 238 patients).
Baseline characteristics.
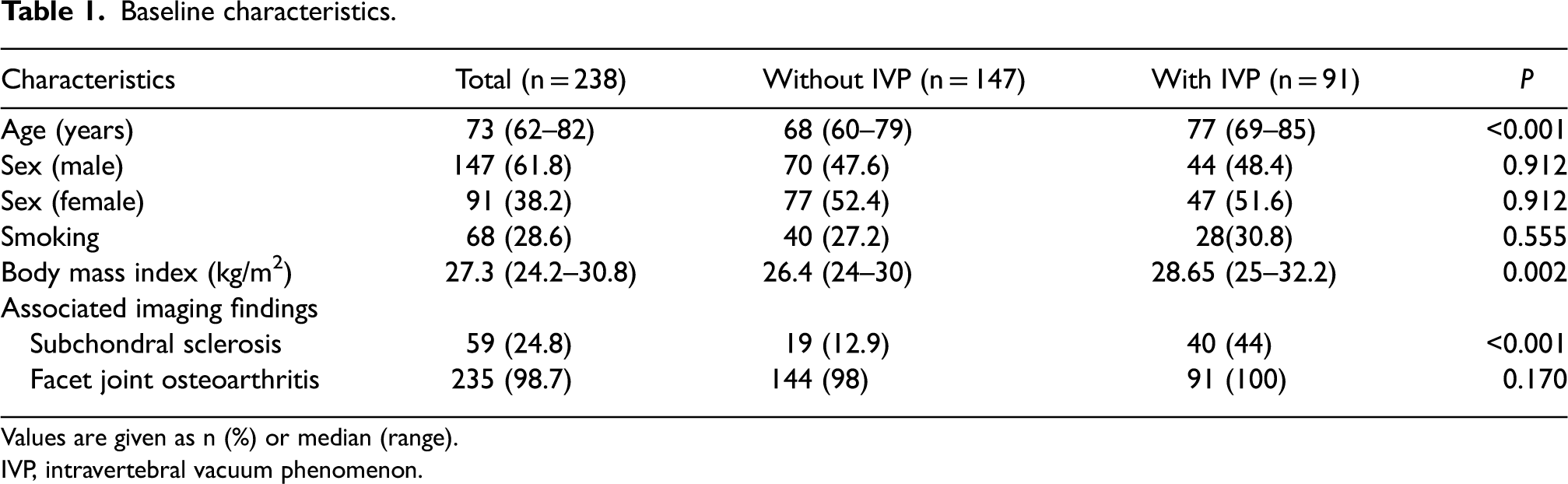
Values are given as n (%) or median (range).
IVP, intravertebral vacuum phenomenon.
Vacuum phenomenon, prevalence, and severity
The presence of IVP in at least one of the levels analyzed was observed in 91 (38%) patients. IVP was more common at L4-L5 followed by L5-S1 levels. Regarding the per-level analysis, the severity classification showed a higher prevalence of minimal vacuum, followed by partial and total IVP (Table 2). Subchondral sclerosis was observed in 59 (25%) patients. The most common level was L5-S1 (n = 38, 16%), followed by L1-L2 (n = 14, 6%), L4-L5 (n = 12, 5%), L3-L4 (n = 11, 4.5%) and L2-L3 (n = 10, 4%).
Vacuum phenomenon distribution according to level and severity.
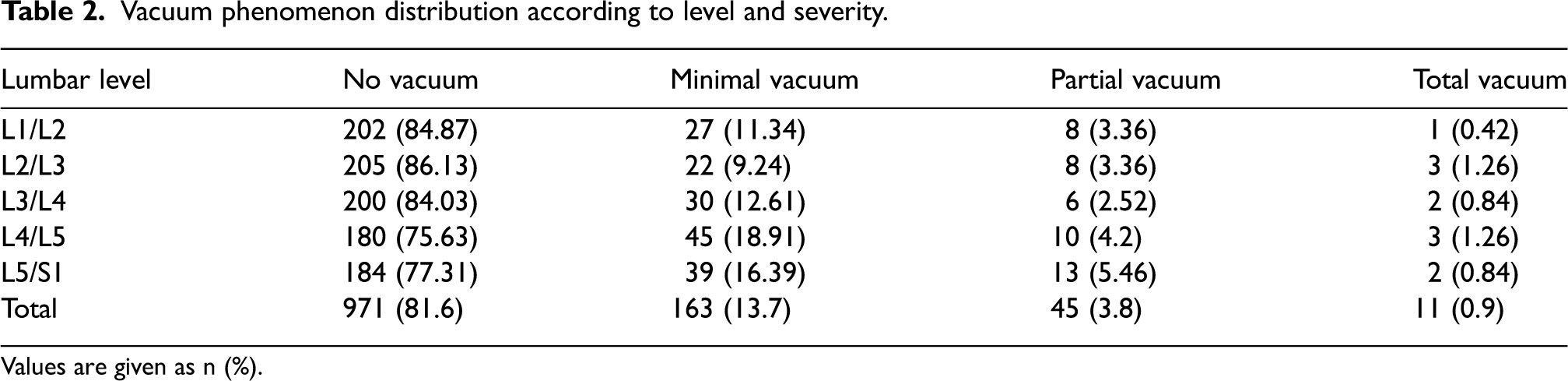
Values are given as n (%).
Facet joint osteoarthritis, prevalence, and severity
Of 238 patients, 235 (98%) exhibited some degree of FJD; the most common level of FJD was at L5-S1 followed by L4-L5 levels. The majority of FJD were considered mild, followed by moderate and severe changes (Table 3).
Facet joint prevalence and severity according to level.
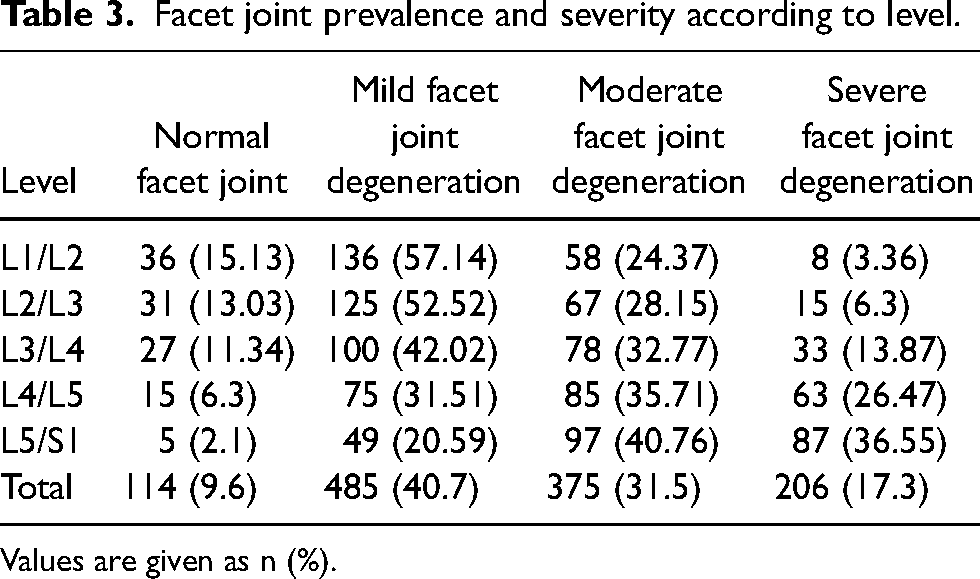
Values are given as n (%).
Multivariate analysis of risk factor for vacuum phenomenon
A multivariate analysis was conducted of risk factors associated with the presence of vacuum phenomenon; the presence of IVP was significantly correlated with age, smoking, obesity, and subchondral sclerosis (Table 4).
Multivariate analysis of risk factors for vacuum phenomenon.
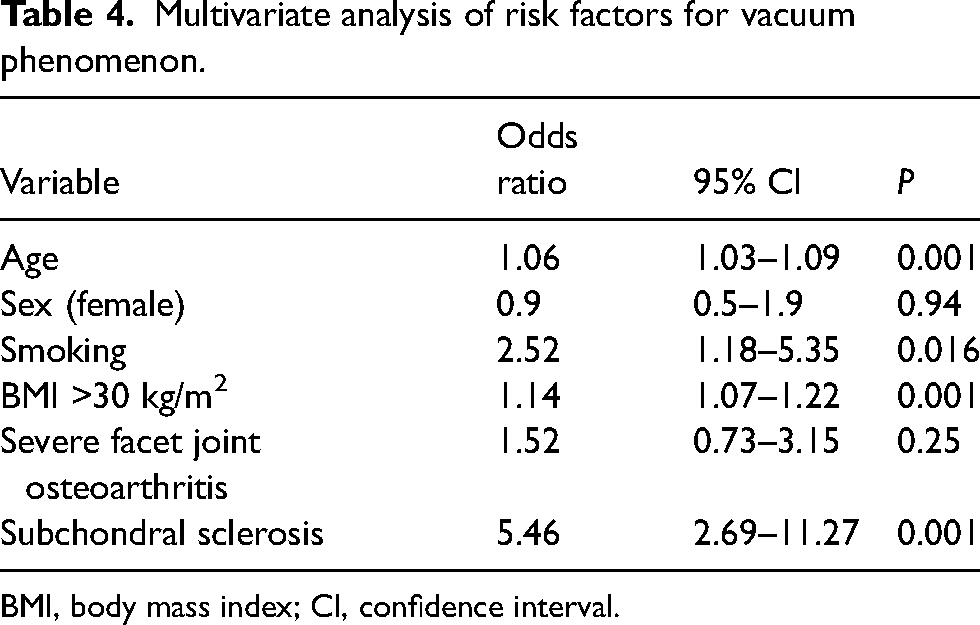
BMI, body mass index; CI, confidence interval.
Discussion
The prevalence of degenerative changes in the lumbar spine increases over time. In the present study, we found a tomographic prevalence of IVP of 38%, with 24% of subchondral sclerosis and 98% of FJD among patients who underwent CT for non-spine-related reasons. It is well known that the presence of degenerative changes per se does not completely explain the cause of pain. Different studies found a high prevalence of degenerative changes, or spinal stenosis in asymptomatic populations. Kanna et al. observed a prevalence of vacuum of 47% in 721 patients, with L5-sacrum as the most frequent level involved. The authors also observed a multilevel vacuum prevalence of 12.5% (19).
Regarding the factors associated with the presence of vacuum, we found that aging, smoking, obesity, and subchondral sclerosis were significantly associated with the presence of IVP at the lumbar spine.
Increased population age is a well-known factor for disc degeneration (20). Regarding the vacuum phenomenon, Kanna et al. observed that patients with the vacuum phenomenon were older than those without the vacuum phenomenon in a series of 721 patients (19). In addition, similar to our study, the authors found no association between vacuum and sex.
Obesity has been shown to increase the risk of disc degeneration (21,22). However, no clear relationship between IVP and obesity has been reported in the literature despite the fact that prevalence of vacuum increases in advanced degeneration and that both disc degeneration and obesity are linked. This is the first study to analyze and demonstrate a significant association between IVP and obesity.
Smoking has been associated with disc degeneration in different studies (23,24). Elmasry et al. observed that the nicotine present in cigarettes downregulates both the proliferation rate and the amount of glycosaminoglycan biosynthesis of disc cells. Moreover, it causes a vascular network constriction that provides the vascular supply to the disc, reducing the exchange of nutrients and anabolic agents from the blood vessels to the disc cells (25). Similar to obesity, our study showed a significant association between the presence of the vacuum phenomenon and smoking. The role of smoking in the development of the vacuum is not clear but could be related to the endplate degeneration that affects the transfer of nutrients and metabolites, as proposed by Li et al. (26). This mechanism also contributes to other imaging findings, such as Modic changes on magnetic resonance imaging (27); however, in our study we only analyzed CT-based changes.
The association between disc degenerative changes and other radiological findings, such as sclerosis, osteophytes, and facet degeneration, has been previously reported. Pye et al. observed a strong correlation between osteophytes and endplate sclerosis in 585 patients with a mean age of 65 years (28).
Lv et al. found an association between facet joint osteoarthritis and disc degeneration (29). However, it is unclear whether these degenerative changes occur independently, due to age-related changes or because of a direct causative mechanism (30). To our knowledge, this is the first study to analyze the association between IVP, subchondral sclerosis, and facet joint osteoarthritis. In this regard, we found a significant association with subchondral sclerosis. These results can be explained by the fact that increased stress in the end plate surface due to advanced degeneration might increase the reactive sclerotic response (31).
The role of the vacuum phenomenon as a cause of low back pain is unclear. While in the past decades this imaging finding had only a descriptive nature, more recent evidence suggests that IVP can be associated with low back pain. Some studies suggest an association between low back pain and movement in patients with the vacuum phenomenon. Morishita et al. (9) observed that patients with the vacuum phenomenon had more pain when standing up and rolling over than patients without the vacuum phenomenon. These findings suggest a role of vacuum phenomenon with movement related to the low back . Physical activity could also play a role in advanced disc degeneration and, therefore, increase the rate of IVP. Suri et al. (32) found an association between physical activity and facet joint degeneration with facet joint vacuum; however, an association with IVP has not been demonstrated.
The use of relatively new therapeutic interventions in patients with IVP have raised the focus on this imaging finding. In this regard, some studies found an improvement in low back pain after filling the IVP with PMMA, providing a spacer stabilizing effect (11–15). In addition, some authors found an improvement of radicular pain due to indirect foraminal decompression due to the PMMA effect (16,33).
Other authors argued that the presence of IVP per se does not completely explain the mechanism for back pain. Yamada et al. (14) states that type 1 Modic change should be considered along with the vacuum phenomenon to be the cause of back pain. In their series, patients with low back pain, vacuum, and type-1 Modic changes are the best indication for percutaneous cement discoplasty.
Besides these recent studies, identifying the cause of back pain is challenging, Low back pain can originate from disc inflammation, facet joints, muscle spasm, tumors, and infections among other causes. Moreover, the source of pain can come from different levels at the lumbar spine, making the diagnosis more difficult, especially in multilevel degeneration observed in elderly patients.
The present study has some limitations. First, this is a retrospective monocentric prevalence analysis. Our findings constitute a sample from a much bigger population so the results may not extrapolate to the entire population. Second, this descriptive study does not analyze clinical aspects such as the presence of low back pain or other factors such as physical activity. This correlation would be interesting to better understand the role of the vacuum and other degenerative changes in the presence of back pain; however, it is difficult to identify pain generators in patients with degenerative changes. Another limitation concerns smoking and BMI variables, which are gathered from the electronic records; they are updated annually from the primary care visit. Due to the retrospective nature of the study, this can be inaccurate. Besides the above-mentioned limitations, to our knowledge, this is the first study that assesses a detailed prevalence of the vacuum phenomenon as well as its severity and correlates these findings with other degenerative changes, such as facet joint osteoarthritis and baseline characteristics.
In conclusion, the prevalence of IVP in patients who underwent CT at the ED in our institution was 38%. Increasing age, obesity, smoking, and subchondral sclerosis were significantly associated with the presence of IVP.
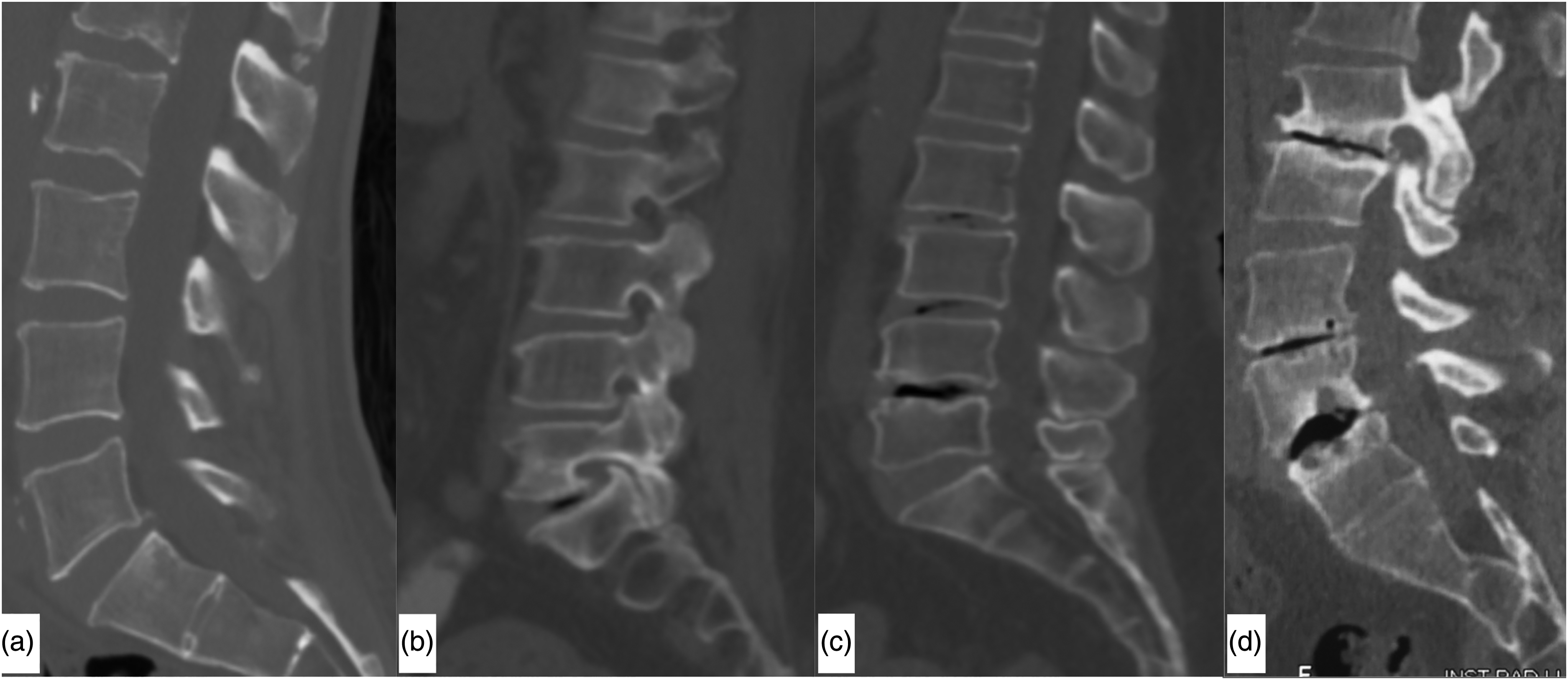
The four stages of the vacuum classification in computed tomography scans obtained from this study: (a) no vacuum; (b) minimal vacuum; (c) partial vacuum; (d) total vacuum.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article