
Abstract
Background
Bone strength is related to both mineral density (BMD) and the bone microstructure. However, only the assessment of BMD is available in clinical routine care today.
Purpose
To analyze and study the correlation of trabecular bone microstructure from the imaging data of a prototype Multitom Rax system, using micro-computed tomography (CT) data as the reference method (Skyscan 1176).
Material and Methods
Imaging data from 14 bone samples from the human radius were analyzed regarding six bone structure parameters, i.e. trabecular nodes, separation, spacing, and thickness as well as bone volume (BV/TV) and structural model index (SMI).
Results
All six structure parameters showed strong correlations to micro-CT with Spearman correlation coefficients in the range of 0.83–0.93. BV/TV and SMI had a correlation >0.90. Two of the parameters, namely, separation and number, had mean values in the same range as micro-CT. The other four were either over- or underestimated.
Conclusion
The strong correlation between micro-CT and the clinical imaging system, indicates the possibility for analyzing bone microstructure with potential to add value in fracture assessment using the studied device in a clinical workflow.
Introduction
Skeletal fractures often occur in patients with a bone mineral density (BMD) in the range of osteoporosis. Dual energy X-ray absorptiometry (DXA) is widely used in the diagnostics and research of osteoporosis and is regarded as the reference method (1,2). However, many low energy fractures take place in individuals with a normal or osteopenic skeleton (3). This may be related to the trabecular bone microstructure, which the two-dimensional (2D) technique of DXA is incapable of visualizing. Another known drawback of DXA is the elevation of areal BMD measurements that can be seen in patients due to vascular calcification and/or proliferations of the vertebrae (4,5). The use of conventional multi-slice computed tomography (MSCT) devices for volumetric measurements of BMD in the detection of osteoporosis has recently shown promising results (6,7). The bone structure as well as the BMD values are heavily affected in osteoporosis (8) and disconnections in the trabecular bone network have been shown to increase the risk of fractures in the vertebrae (9). It is also shown that the risk of fractures is independently correlated to deficits in bone density as well as in the bone structure (10). Therefore, clinical devices able to analyze bone microstructure may be important in osteoporosis imaging by adding additional parameters for assessing the future risk of fractures.
High-resolution peripheral quantitative CT (HR-pQCT) is a more recent diagnostic tool for the diagnostics and research of osteoporosis (11). With HR-pQCT imaging, it is possible to visualize the trabecular bone microstructure in the peripheral skeleton, such as the wrist and heel. HR-pQCT studies have shown that trabecular bone deficits are of great importance for fractures in young adult men (12). A drawback with HR-pQCT is that it is not possible to examine the hip or vertebrae, which are the body parts where most low energy fractures occur.
Patients arriving at the emergency department with the suspicion of a skeletal fracture are most often imaged by 2D imaging methods to diagnose fractures. If it was possible to image the bone microstructure and assess BMD, at the same time and preferably with the same device, a future fracture risk assessment could be calculated. In vitro studies have shown that trabecular bone microstructure can be visualized by conventional MSCT devices (13–15). The method is promising but often requires a high radiation dose, which makes it suboptimal for wider adoption. More research in this field is therefore needed.
A newly developed imaging device, the Multitom Robotic Advanced X-ray (RAX) (Siemens Healthineers GmbH, Forchheim, Germany), is a so-called twin robotic X-ray system. This device uses highly movable robotic arms for capturing images keeping the patient table static. Because of the movable robotic arms allowing the X-ray tube as well as the detector to rotate, there is no need to move the patient. This makes fracture examinations less painful and less time-consuming and useful in, for example, emergency orthopaedics. This device can be used as a conventional 2D X-ray system. The possibility of 3D imaging at the same device decreases the risk for delay in diagnostics, which may otherwise be a problem if the patient has to be examined with conventional CT as well. The possibility of free precision motion control all the way around the table allows examinations using cone-beam CT (CBCT) technique. The latter possibility enables various areas, including the hip and vertebrae, to be X-rayed in 3D and also makes it possible to examine patients with a 3D technique in a standing position.
The aim of the present in vitro study was to analyze trabecular bone microstructure and study the correlation of these structure measures from imaging data of a prototype Multitom Rax system, using micro-CT (Skyscan 1176) data as the reference method.
Material and Methods
Material
This was an in vitro study on 14 cadaver biopsies from the distal part of the human radius, the forearm. The specimens were donated for medical research according to the ethical guidelines from University of California, San Francisco. The specimens have previously been analyzed and these results have been published elsewhere (16–18). All specimens are almost cubic, with sides of about 12–15 mm, and they all have slabs of cortical bone. The cortical bone slabs were used for orientation purposes during the imaging and analyses processes. The specimens have been chemically defatted before being stored individually, in numbered test tubes filled with water (Fig. 1). At imaging, each test tube was placed in the center of a 100-mm-diameter paraffin cylinder. The paraffin was used to mimic human soft tissue.
One of the bone specimens, individually stored and numbered in a test tube filled with water. The slice of cortical bone is marked in black.
Imaging
The imaging data were acquired using two devices, namely
A micro-computed tomography (micro-CT) scanner, the Skyscan 1176 (Bruker micro-CT, Kontich, Belgium). These images were acquired using a tube voltage of 65 kV and a tube current of 385 μA and through a 360° rotation at a rotation step of 0.3° at 1100 ms per projection, frame averaging of four images and a total exposure time of approximately 2 h. The reconstruction algorithm was a filtered back-projection (FBP) using a Hamming filter and the volume was reconstructed with 8.67 µm voxels. A twin robotic X-ray scanner, Multitom Rax (Siemens Healthineers GmbH, Forchheim, Germany) using the CBCT technique. The radiation field used in this study is cone-shaped with a diameter of 16 cm. The detector is an a-Si with a CsI scintillator and a size of 42 × 42.5 cm. The pixel size of the flat panel detector is 0.148 mm and when using the high-resolution mode, the spatial resolution is 3.2 lp/mm at 2% MTF. The imaging protocol was at a tube voltage of 80 kV and a tube current of 1538 mAs (at 304 projection images) with a scan time of 12 s at one single rotation and a field of view (FOV) of 16 cm. The radiation dose measured as CTDI was 33.6–35.1 mGy. The DLP was in the range of 535–562 mGycm. Each detector element is 0.148 mm. Voxels at an isotropic resolution of 80 μm were reconstructed in the scanner software. The reconstruction algorithm was a FBP (FDK algorithm, Feldkamp, Davis, Kress) and the reconstruction kernel was VF11. The system used was a prototype device with pre-production software.
The data from the micro-CT were regarded as the reference. Data from the Multitom Rax were manually registered to match the volumes of interest from the micro-CT. This was performed in two steps in MeVisLab (MeVis Medical Solutions AG, Bremen, Germany) and resulted in cubes consisting only of trabecular bones with sides of approximately 8 mm (Fig. 2).
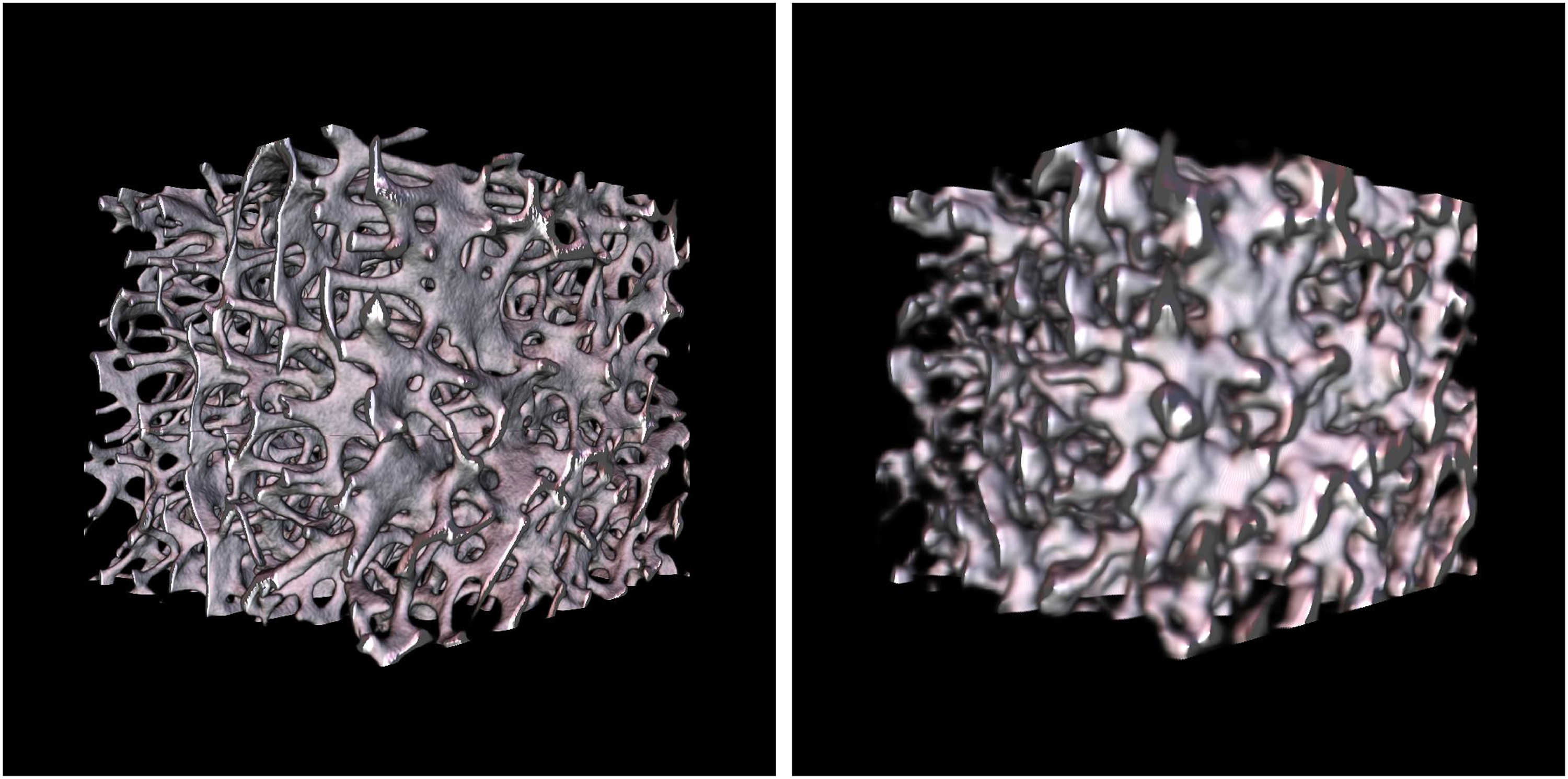
Trabecular bone cubes, from the same bone specimen as in Fig. 1, which were used for the microstructure analyses. Left: a bone cube from segmented micro-CT data. Right: a bone cube from segmented Multitom Rax data. CT, computed tomography.
Image processing
For the Multitom Rax, the segmentation method used to segment bone from other tissues, was the automated 3D region growing algorithm (ARG) (19). This method has been used for the segmentation of imaging data from other clinical CT devices and is described in more detail in previous studies (20). The segmentation of the micro-CT data is easier to perform due to the high contrast-to-noise ratio (CNR) compared to the clinical scanner (Fig. 3). The high CNR of the micro-CT data makes it possible to use the single threshold, intensity-based Otsu-method with a specific threshold for each specimen as described in the paper by Otsu (21).
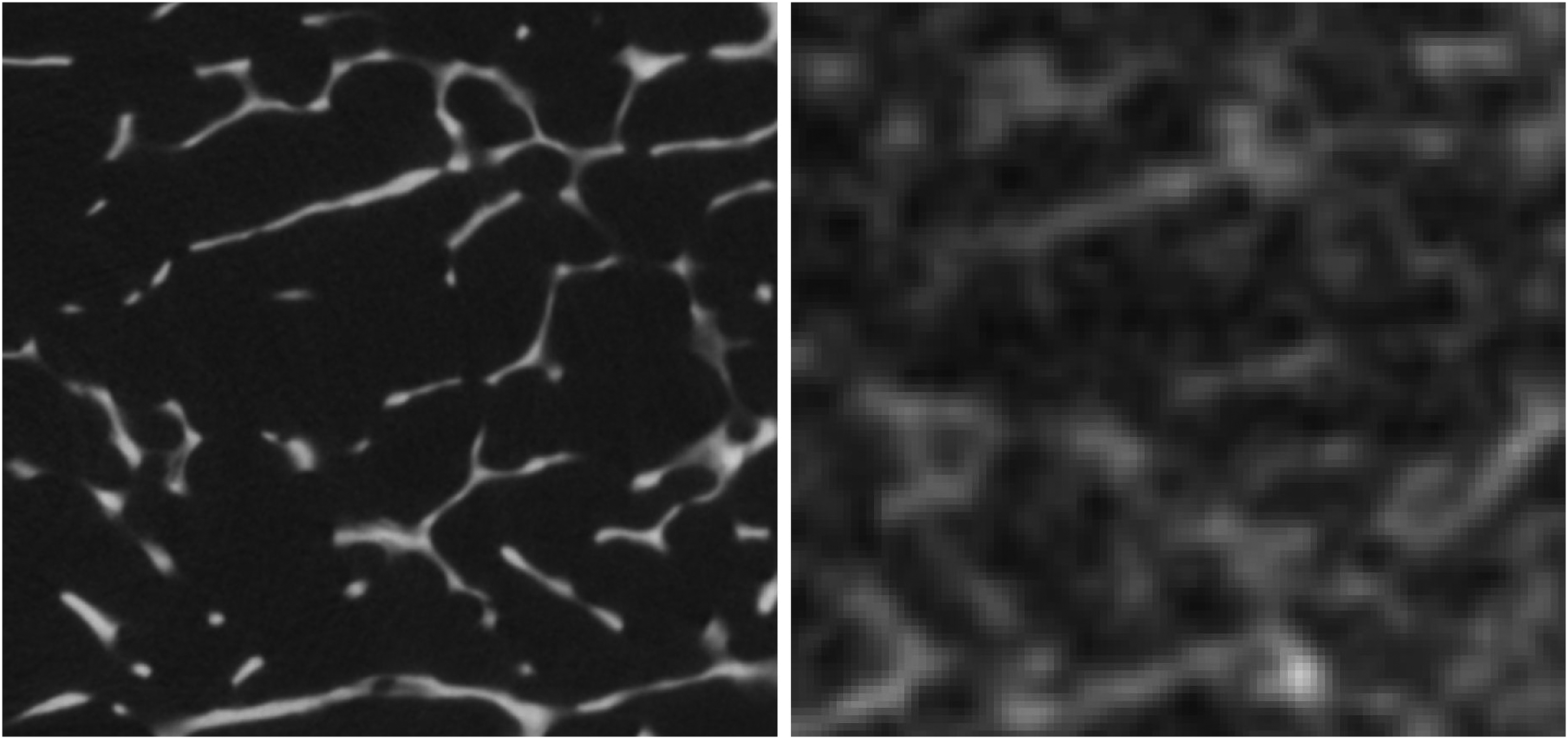
Raw image slices, with a Skyscan micro-CT slice (left) and a Multitom Rax slice (right). Demonstrating the difference in CNR between the two raw image datasets. The images also show how the trabecular thickness is impacted from the partial volume effect. CNR, contrast-to-noise ratio; CT, computed tomography.
The in-house developed ARG-based segmentation code is written in MATLAB (Mathworks, Natick, MA, USA) using the method described previously (22,23). Thinning and skeletonizing the bone structure enables analysis of bone structure parameters in 3D. Six different parameters were calculated, which are described below.
Tb.Nd is the number of trabecular intersections of the skeletonized structure (nodes) per volume Tb.Sp (mm) is the trabecular separation, i.e. the space between the edges of the trabecular microstructure Tb.N (1/mm) is the number of trabeculae Tb.Th (mm) is the trabecular thickness BV/TV (%) is the trabecular bone volume fraction in the analyzed volume (bone volume/total volume) SMI is the structural model index and is a way to represents the proportion of rods and plates in the volume
Statistical methods
Statistical analysis was carried out using SPSS Statistics version 28 (IBM Corp., Armonk, NY, USA). Results of the microstructure parameters are given as mean values with standard deviations. The data from the micro-CT were compared to the data from the Multitom Rax using Spearman’s correlation with 95% confidence interval and with Wilcoxon signed rank test with 25%–75% percentiles.
Results
As shown in Table 1, there were significant correlations between the Multitom Rax and micro-CT regarding all bone microstructure parameters analyzed. All six segmented structures showed a Spearman’s correlation of 0.83 or stronger. The BV/TV and SMI had correlations >0.90.
Comparison of trabecular scores derived from micro-CT and Mutlitom Rax.
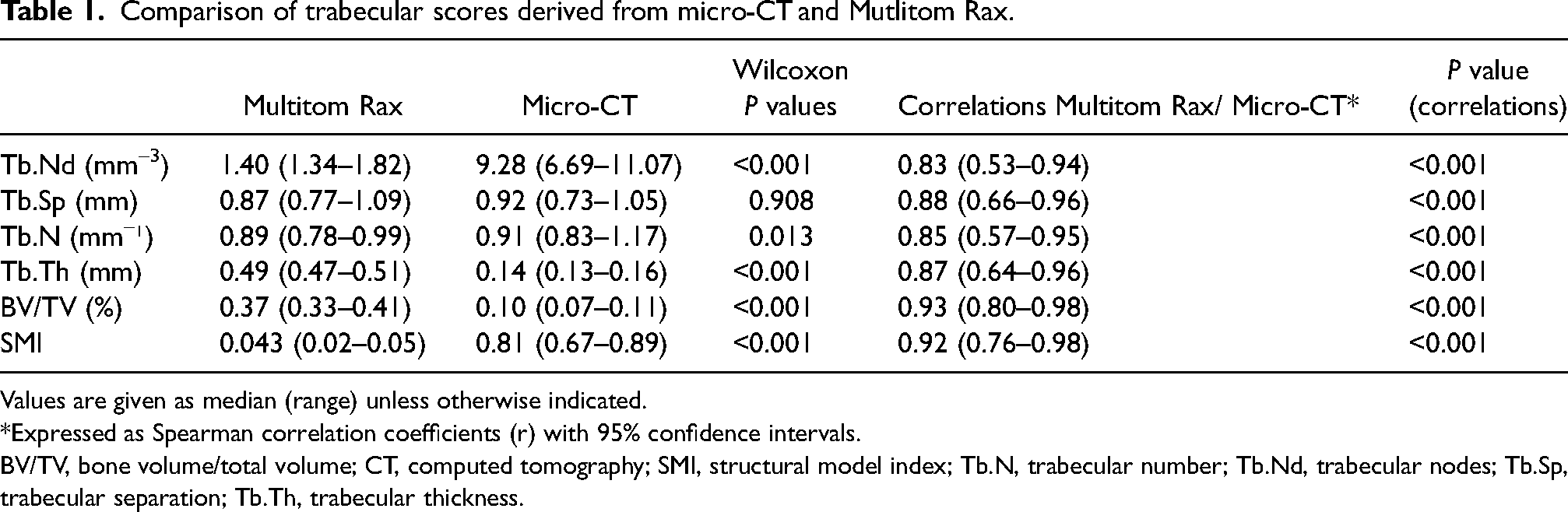
Values are given as median (range) unless otherwise indicated.
*Expressed as Spearman correlation coefficients (r) with 95% confidence intervals.
BV/TV, bone volume/total volume; CT, computed tomography; SMI, structural model index; Tb.N, trabecular number; Tb.Nd, trabecular nodes; Tb.Sp, trabecular separation; Tb.Th, trabecular thickness.
Regarding the median values of the bone parameters, the Tb.Sp and Tb.N had mean values in the same range as the micro-CT, in the range of 91%–101% of these values Tb.Nd and SMI were strongly underestimated and had values of 17% and 4% compared to the micro-CT. On the other hand, the Tb.Th and BV/TV were overestimated by approximately 220%–382%. All parameters except Tb.Sp (P = 0.908) were statistically significantly different from the micro-CT (Table 1 and Fig. 4).
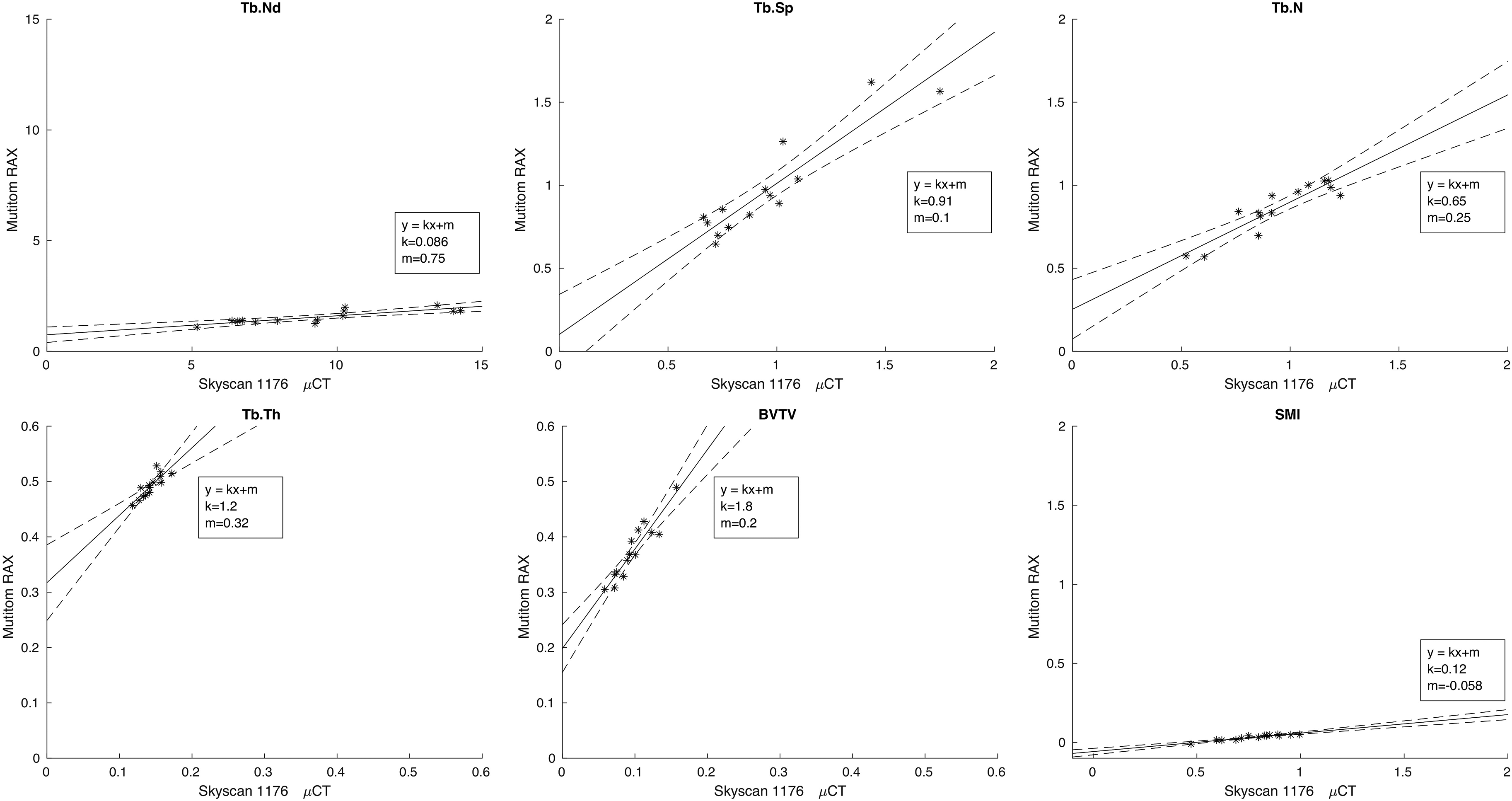
Scatter plot diagram with the six bone microstructure parameters. The y-axis shows the Multitom Rax values and the x-axis shows the Skyscan micro-CT values. The two dotted lines in the scatter plots represent the 95% confidence intervals. CT, computed tomography.
Discussion
In the present study where the CBCT technique in the Multitom Rax was used, there were strong correlations to micro-CT for all studied bone structure parameters with correlation coefficients in the range of 0.83–0.93. Two of the six parameters had correlations of >0.90.
As the trabecular bone microstructure is known to be of great importance for the strength of skeletal body parts (9), it would be of great interest if X-ray devices used in clinical practice could be used for such analyses.
Currently, HR-pQCT is often regarded as the method of choice for bone structure analysis in clinical use and studies (10,24). In a previous study, the segmentation method used in this study was applied on data from an HR-pQCT device. The results were encouraging and demonstrated strong correlations to data derived from micro-CT (20).
Another device available in clinical practice is dental CBCT. Studies have described strong correlations regarding bone microstructure between micro-CT and CBCT (17,25). Such CBCT devices are, however, not applicable for the imaging of central body parts and only some devices can be used outside the facial skeleton, due to the fact that most of the devices are designed for patients in a sitting and/or standing position. Studies of the mandible have shown that fractures of other sites in the human body can be predicted by mandible bone structure (26). One drawback is that CBCT devices do not display Hounsfield values. The study showing the potential of density measurements as well as microarchitecture assessments of the distal radius, with CBCT devices, is encouraging (27).
Since Multitom Rax uses the CBCT technique for 3D volume examinations, this scanner has the same kind of limitations as dental CBCT devices. Although the voxels are smaller (80 µm) compared to MSCT devices (200 µm), the resolution close to the thickness of a bone trabeculae will result in partial volume effects. The strong underestimation of SMI measured by Multitom Rax (0.04) compared to the reference method of micro-CT (0.81) can be assumed to be related to the partial volume effect, which will increase the number of plates compared to the number of rods. This partial volume effect can also explain the overestimation of the bone volume and trabecular thickness.
The present study has some limitations. Although the correlations between micro-CT and Multitom Rax were strong, all parameters but Tb.Sp significantly differed in magnitude from micro-CT. Tb.N also had values in nearly the same range as micro-CT, but these values did significantly differ from the micro-CT (P = 0.013). This counterintuitive result is likely related to the blooming artefacts of the bony structures that increase the trabecular thickness for the Multitom RAX data. This affects the low attenuation part between the trabeculae, which then decreases. The algorithm fails in separating the trabeculae, which can be seen in Fig. 4, where Multitom Rax for most of the specimens produces a lower Tb.N compared to micro-CT. When looking at the number of trabecular separations detected, this is not as affected. All other structure parameters were either over- or underestimated.
Over- or underestimations compared to micro-CT have been shown for other clinical devices in earlier publications, both from our study group as well as from others (16,25). This may be overcome if the grade of over- or underestimation is known. But one must keep in mind that other factors such as bone mass and/or grade of osteoporosis of the patient may impact such calculations. If the purpose of the examinations is to monitor changes in the bone structure for specific individuals over time and using the same device, the risk for misinterpretations may decrease. Another drawback is the relatively low number of samples. The samples, however, show differences in the structure, and when scanned with micro-CT the BV/TV was in the range of 6%–16% and the number of trabecular nodes were in the range of 5.2–14.2 per mm³.
The method used in the present study is not yet commercially available and the actual system and software with possibilities for reconstruction with smaller voxels was a prototype at the research center of the company. The high-resolution mode of Multitom Rax, used for the specimens in this study, is currently possible for imaging of the upper extremities such as the elbow and wrist. According to the manufacturer, the CTDI was 18.9 mGy and DLP was 307.9 mGy.cm, estimated with a 16-cm-diameter cylindrical PMMA phantom when imaging an elbow and wrist based on the methods described in Fransson and Tingberg (28).
At our radiology department, an examination of the wrist in a conventional CT scanner for a diagnosis of fracture corresponds to a size-specific dose estimate: SSDE of 8.4 mGy when CTDIvol was 2.8 mGy with a 32-cm-diameter cylindrical PMMA phantom for a wrist with an effective diameter of 59 mm (AP 52 mm, LAT 67 mm) using AAPM report 204 (29). At such examinations, it is not possible to evaluate bone microstructure. The dose in air in the center of rotation in a dental CBCT for bone microstructure imaging of a human wrist was estimated at 19.9 mGy with a CTDI of 6.3 mGy corresponding to an air kerma-area product of 716 mGy.cm² with a 36 cm2 X-ray beam area (6 × 6 cm2).These dose indices were the same as when using these imaging parameters in our previous studies (85 kV, 5 mA, FOV = 6 cm, imaging time = 17s) (17). The small voxel sizes needed for bone microstructure imaging results in radiation doses above conventional MSCT and CBCT diagnostic fracture imaging of the extremities (30). In our study, 1538 mAs has been used to test the limits of the system. The resulting CTDIvol of 18.9 mGy is in the same range as the measured dose of 23.7 mGy, in the study imaging the knee using the validated method of HR-pQCT (31). Analyzing the bone microstructure of the hip and spine would be of great interest because these fractures are more fatal. Unfortunately, at the moment, this is not possible due to limitations of the system as well as the high radiation dose needed. When the imaging is conducted with a cone-shaped beam and focused to the less radio-sensitive adult body parts, such as the extremities, this may not even be a problem. Research on more specimens as well as future clinical studies are needed to evaluate and optimize the protocol for such bone structure analyses.
The strong correlations regarding the studied bone structure parameters show the potential for future bone microstructure and osteoporosis research using this type of imaging device.
In conclusion, image data of radial human bone biopsies showed strong to very strong correlations in bone microstructure parameters when scanned with the Multitom Rax system and compared with imaging data from micro-CT. The information of microstructure might be obtained by the CBCT function in a Multitom Rax in a clinical workflow, possibly adding value in fracture assessment. Although, over- as well as underestimations of the bone parameters must be taken into account.
Footnotes
Acknowledgements
We thank Professor Sharmila Majumdar at the University of California, San Francisco, and Torkel Brismar at the Karolinska University Hospital for providing the bone specimens; Britt-Marie Andersson at the University of Uppsala for the micro-CT scans; and the staff at Siemens Healthineers, Forchheim for the opportunity to use the Multitom Rax device.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the ALF Grants, Region Östergötland, Sweden (grant no. RÖ-936170).