
Abstract
Background
Bridging treatment with intravenous thrombolysis (IVT) before endovascular thrombectomy (EVT) in acute ischemic stroke is applied under the assumption of benefits for patients with large vessel occlusion (LVO). However, the benefit of this additional step has not yet been proven.
Purpose
To compare procedural parameters (procedural time, number of attempts), complications, and clinical outcome in patients receiving EVT vs. patients with bridging treatment.
Material and Methods
In this prospective study all patients had acute anterior cerebral circulation occlusion and were treated with EVT. All patients were selected for treatment based on clinical criteria, multimodal computed tomography (CT) imaging. Eighty-four patients were treated with bridging IVT followed by EVT; 62 patients were treated with EVT only.
Results
Bridging therapy did not influence endovascular procedure time (P = 0.71) or number of attempts needed (P = 0.63). Bleeding from any site was more common in the bridging group (27, 32%) vs. the EVT group (12, 19%) (P = 0.09). Functional independence modified Rankin Scale after 90 days was slightly higher in the bridging group (44%) vs. the EVT group (42%) (P = 0.14). Mortality did not differ significantly at 90 days: 17% in the bridging group vs. 21% in EVT alone (P = 0.57). Both treatment methods showed high recanalization rates: 94% in the bridging group and 89% for EVT alone.
Conclusion
Bridging treatment in LVO did not show benefits or elevated risks of complications in comparison to EVT only. The bridging group did not show significantly better neurological outcome or significant impact on procedural parameters vs. EVT alone.
Introduction
Several randomized controlled trials (RCT), including EXTEND-IA, MR CLEAN, SWIFT- PRIME, and ESCAPE, were published in 2015 and provided strong evidence of improved outcome for patients who were treated with endovascular thrombectomy (EVT) vs. intravenous thrombolysis (IVT) alone (1–3). Some of these studies included bridging treatment of patients with IVT but did not compare the patients with bridging to EVT alone (2,4). Therefore, the effectiveness of bridging therapy compared with EVT alone for large vessel occlusion (LVO) strokes is still questionable (5). Guidelines currently recommend the use of IVT if treatment can be started within 4.5 h and if there are no contraindications (5,6). Potential risks of IVT are an increased risk of intracerebral hemorrhage (ICH) or other bleeding complications (7,8). IVT is contraindicated: after the 4.5-h time window; for patients with current use of anticoagulants with international normalization ratio (INR) > 1.7 or partial thromboplastin (PTT) > 15 s; wake up stroke; surgery or ICH in the last three months. Administration of IVT can delay the start of EVT for some patients, especially in centers where patients can be transferred quickly to EVT (9).
A couple of recent single-center retrospective studies have already shown tendencies that IVT before EVT might have very limited or even no effect on potential outcome in patients with LVO strokes compared to EVT alone (7,10–12).
IVT is applied before EVT under the assumption of shortening thrombectomy procedural time and reduced number of attempts of catheterization with a stent-retriever or aspiration system. Furthermore, it is assumed that IVT would favor the dissolution of residual thrombotic material after mechanical thrombectomy (9). Thrombolysis might be more effective in cases of cardio-embolic stroke compared to atherothrombotic etiology stroke and IVT can be started quickly, especially for patients who are transferred from another hospital (7). Moreover, there is no clarity if bridging therapy increases the number of symptomatic ICH (7).
The aim of this study was to compare bridging therapy with EVT (IVT followed by EVT) with EVT alone in patients with proximal vessel occlusion, using procedural parameters, complication rate, and late neurological outcome after 90 days as the markers of process and outcome.
Material and Methods
This prospective single-center study evaluated 157 acute stroke patients who were admitted between February 2014 and January 2017 and eligible for endovascular treatment. The study was approved by the local ethics committee. Verbal informed consent was obtained from all individuals or from legally authorized representatives before the study.
All patients received multimodal computed tomography (CT) imaging including non-contrast CT, CT angiography of intra- and extracranial blood vessels, and CT perfusion (CTP). Imaging equipment used were GE LightSpeed VCT 64 scanner and AW CT Perfusion 4D post-processing software (13,14) (GE Healthcare, USA). CTP was performed for tissue viability assessment and for differentiation of “core” area describing irreversible cerebral ischemia or necrosis from “penumbra” showed as hypoperfused brain tissue, also called tissue at risk (13). The key inclusion criterion was a large artery occlusion in anterior circulation (ICA and MCA [M1 segment] or both vessels [tandem occlusion]) suitable for EVT and other perfusion-imaging based parameters. Patients were eligible for EVT if National Institutes of Health Stroke Score (NIHSS) score was ≥ 5.
Exclusion criteria were imaging based on CT and CTP based: ASPECTS score on CTP maps of irreversible cerebral ischemia – necrosis < 5 (range = 0–10, with 1 point for each ischemic region and lower numbers indicating less viable tissue); absent (malignant) collaterals on CT angiography or stroke in the posterior circulation; and wake up stroke (15,16). Patients lost to follow-up were also excluded (n = 11; six in the bridging group and five in the EVT group).
Finally, 146 patients were included in this study: 84 (57.5%) received bridging treatment (IVT followed by EVT); and 62 (42.5%) patients received only EVT. All patients included in the study were from one hospital.
Bridging therapy
IVT was initiated immediately for all patients after the multidisciplinary evaluation, including multimodal CT assessment and evaluation of any possible contraindication, e.g. INR > 1.7 or PTT > 15 s, wake up stroke, surgery or ICH during last three months. All patients in the bridging group received a full dose (0.9 mg/kg) of recombinant tissue plasminogen activator (17). IVT was completed for some patients during the EVT procedure to avoid delaying the initiation of endovascular treatment. The bridging therapy patients received IVT within 4.5 h from onset of symptoms (5). All EVT groin punctures were performed within 6 h and full thrombectomy within 8 h of symptom onset. EVT without bridging treatment was applied if the patient had contraindications for IVT or based on doctor’s preference and equipment availability.
Endovascular thrombectomy
EVT was performed using a combination of aspiration and stent-retriever techniques. An aspiration device was used to extract the clot. A retriever device resembling a stent attached to a guide wire was used to remove resistant clots (18,19). EVT was available 24 h for all acute stroke patients with initiated or contraindicated thrombolysis with eligible clinical and imaging criteria (neurological status, tissue viability on perfusion, accessible anatomy on angiography).
Anesthesia was adapted to the individual situation. Of patients, 94% received local anesthesia or sedation; general anesthesia was administered only for patients with low Glasgow Coma Scale (< 8) and with respiratory failure (5,20).
All the patients received follow-up by non-enhanced brain CT scan 24 h after treatment. All the procedural and imaging parameters corresponded to the European Recommendations on Organization of Interventional Care in Acute Stroke (EROICAS) (5).
The NIHSS was used to analyze neurological deficit with a range of 0 (no deficit) to 42 (fatal outcome). Modified Rankin Scale (mRS) was applied for functional neurological assessment on admission and at discharge from hospital and 90 days after the treatment via phone interview. Two or fewer points on the mRS describes functional independence (21). Symptomatic and asymptomatic ICH and mortality rate were analyzed in both groups. Local hematoma at the catheter insertion site was not counted as any bleeding.
Revascularization was evaluated using the Thrombolysis in Cerebral Infarction (TICI) scale. The scale ranges from 0 (no perfusion) to 3 (complete reperfusion). Successful revascularization was considered as a TICI score of 2 b–3 (22).
Time from femoral arterial access to full recanalization on digital subtraction angiography and the number of stent-retriever attempts to obtain recanalization were recorded.
Statistical analysis
Data were analyzed using Microsoft Excel and SPSS software version 20. Linear data were tested for normality using Shapiro–Wilcoxon and Kolmogorov–Smirnov tests. If the P value was < 0.05, the data were not considered to be normally distributed. Median and interquartile range were used for linear data characteristics. The Mann–Whitney test was used to compare median data in thrombectomy and bridging groups. Fisher’s exact test was used for bivariate associations. A P value <0.05 was considered statistically significant. We used odds ratio (OR) in binary logistic regression to analyze risk of hemorrhage and to compare proportion of good functional outcome (mRS = 0–2).
Results
Baseline patient characteristics.
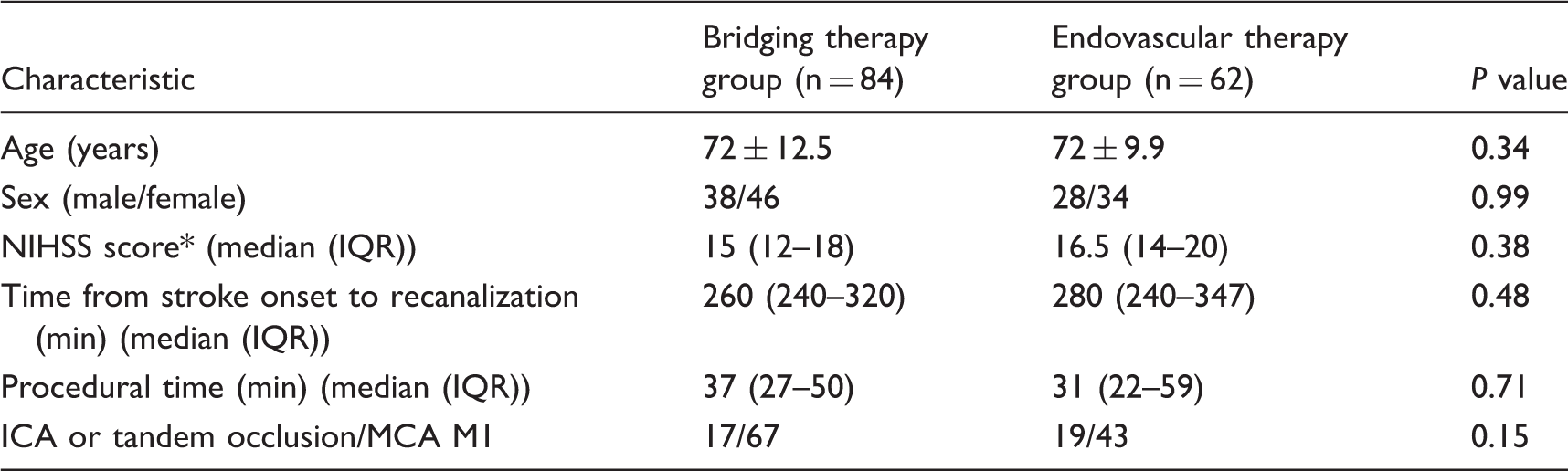
National Institutes of Health Stroke Scale, ranging from 0 (normal) to 42 (fatal outcome): 0 = no stroke symptoms; 1–4 = minor stroke; 5–15 = moderate stroke; 16–20 = moderate to severe stroke; 21–42 = severe stroke (25).
ICA, internal carotid artery; MCA M1, middle cerebral artery M1 segment; IQR, interquartile range.
The long-term results at 90 days showed that mRS was 0–2 in 37 patients from the bridging group (44%) and in 26 patients from the EVT group (42%; P = 0.14) with an OR of 0.48 (95% CI = 0.216–1.070). Median mRS at 90 days after bridging treatment was 3.0 (range = 1–5), while median mRS at 90 days after EVT was 3.0 (range = 2–5; P = 0.7), with no statistical significant difference. The patients’ functional outcome is shown in Fig. 1.
Distribution of the mRS scores 90 days after the treatment within EVT and bridging groups. The numbers in the boxes represents the absolute numbers of patients. MRS range of 0 to 6: 0 = no symptoms; 1 = no clinically significant disability; 2 = slight disability but can live without assistance; 3 = moderate disability; 4 = moderately severe disability (unable to walk unassisted); 5 = severe disability; and 6 = death. Patients with a score of 0, 1, or 2 are rated as functionally independent.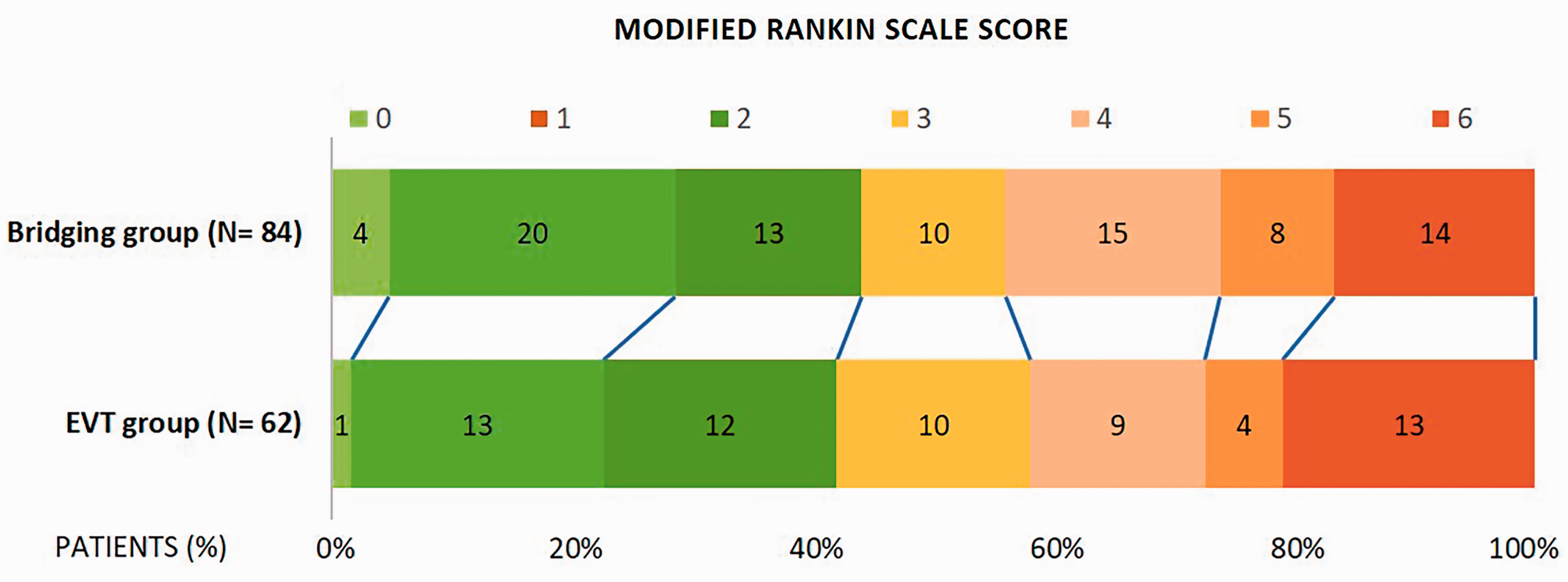
Mortality at 90 days was 17% in the bridging group (n = 14) and 21% in the EVT group (n = 13), with no significant difference (P = 0.57). The number of symptomatic ICHs was equal in both groups: 10 (12%) in the bridging group vs. 6 (10%) in the EVT group (P = 0.79).
The tendency for a higher asymptomatic bleeding risk in the bridging group (17 [20%]) compared to the EVT group (6 [10%]) was of no statistical significance (P = 0.1). Similarly, the numbers of any bleeding in the bridging treatment group were of no significant difference to the EVT group (27 [32%] vs. 12 [19%]; P = 0.09, OR = 0.5, 95% CI = 0.221–1.062).
Clinical outcome.
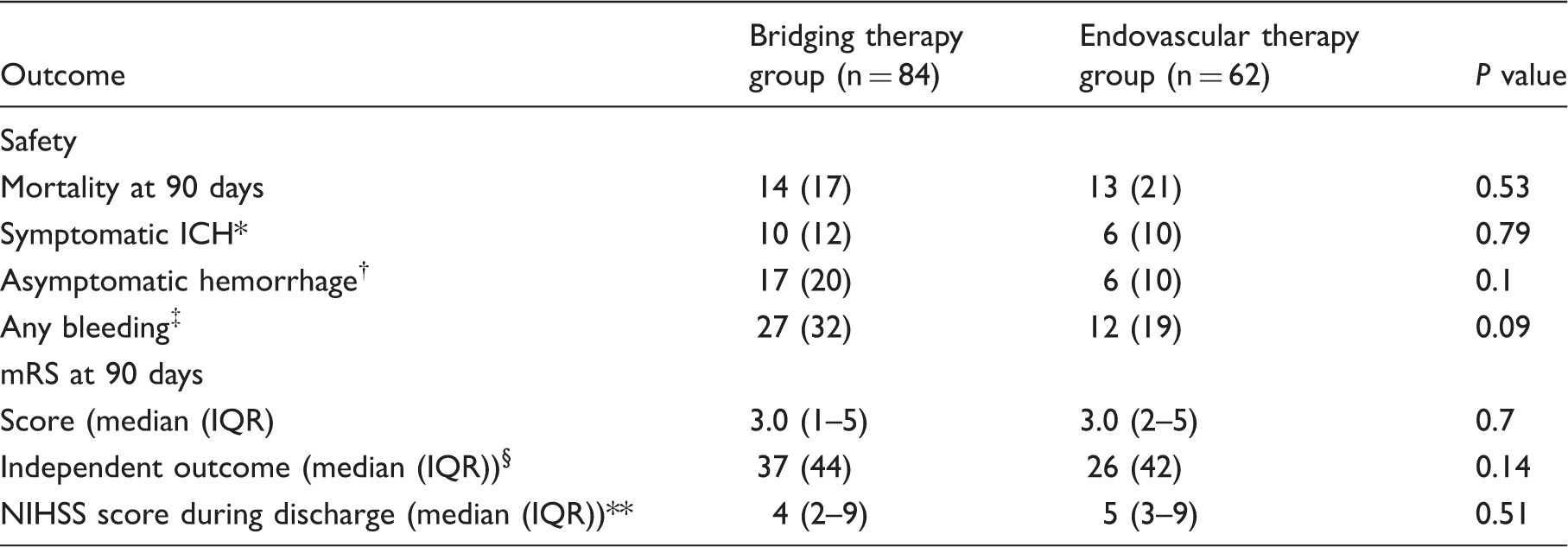
Values are n (%) unless otherwise stated.
Symptomatic intracerebral hemorrhage (ICH) was defined as a large parenchymal hematoma (> 30% blood of stroke volume with mass effect and increase of 4 points or more in the NIHSS score).
Asymptomatic hemorrhage was defined as a hemorrhagic imbibition with no mass effect and no increase in NIHSS score.
Any bleeding was a summary of both symptomatic and asymptomatic hemorrhage count.
Independent outcome mRS 0–2.
Median NIHSS score during discharge excluded dead patients.
Characteristics of the endovascular procedure.
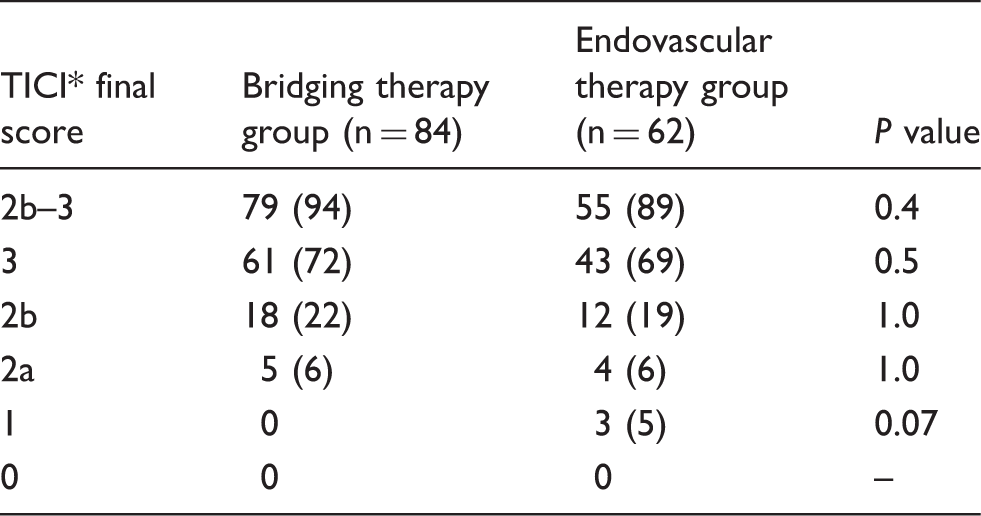
Values are n (%).
Thrombolysis in cerebral infarction (TICI) grading system for endovascular revascularization evaluation: 0 = no perfusion; 1 = penetration with minimal perfusion; 2a = partial perfusion, less than two-thirds of entire vascular territory is visualized; 2b = complete filling of all the expected territory is visualized but the filling is slower than normal; 3 = complete perfusion (26).
Recanalization was achieved by one pass in >50% of cases within both groups: 61% in the EVT group and 54% in the bridging group. There was no statistically significant difference between distribution of thrombectomy attempts within both groups, P = 0.63. The results are shown in Fig. 2.
Thrombectomy attempts compared within direct EVT and bridging therapy groups. Recanalization was achieved in >50% of cases by first thrombectomy attempt with no statistically significant difference within both the EVT and bridging therapy groups (P = 0.64).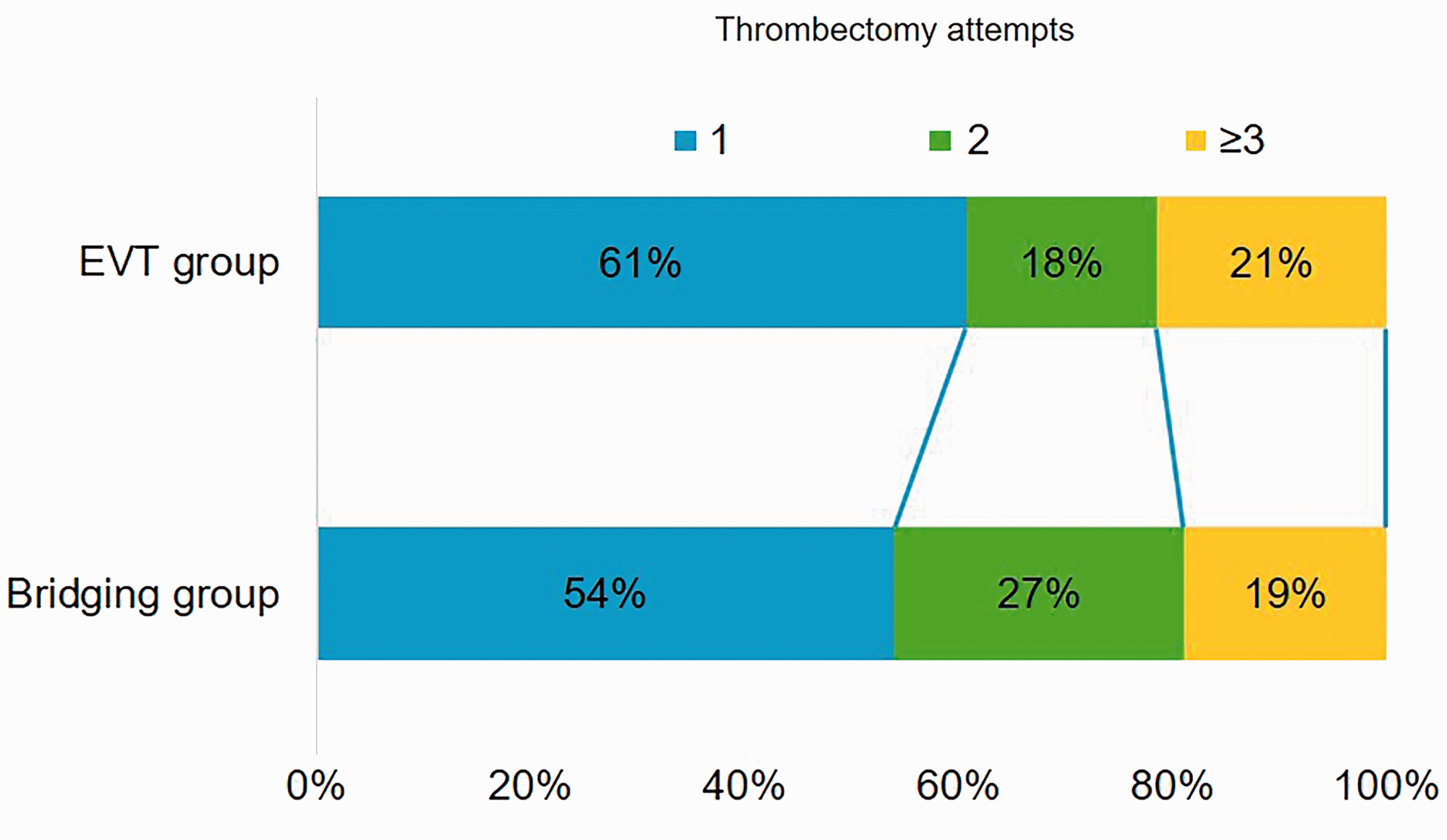
Discussion
This study showed that the bridging treatment is a safe and effective method, but it did not show a significantly better recanalization rate or functional outcome. Also, procedural time and number of attempts did not differ between EVT alone and bridging group.
EROICAS guidelines still recommend IVT for all patients, but EVT as a first-line treatment method should be used for patients with LVO stroke in the anterior circulation if patient has contraindications for IVT. Although, there are several benefits of IVT use in bridging before the application of EVT, concerns about haemorrhage rate may occur (5).
IVT is applied before EVT under the assumption of shorter thrombectomy procedural time and a reduced number of attempts of catheterization with a stent-retriever or aspiration and to induce thrombolysis in the clot. Furthermore, the beneficial effects of IVT on the dissolution of residual thrombotic material after mechanical thrombectomy are still discussed (9).
Inclusion of patients into our study was based on radiological selection criteria in CT (perfusion ASPECTS score, perfusion parameters, collateral blood flow). The study analyzed the potential outcomes between both groups (EVT vs. bridging); the patient selection and procedural parameters were more detailed compared to other previous retrospective studies about the effects of bridging therapy, especially including procedural time, success, and number of attempts (7,23).
Regarding the benefits for the EVT procedure, an earlier study by Leker et al. (24) showed that patients who received IVT needed fewer attempts during the EVT, while our study showed that recanalization was achieved by the first pass in > 50% of cases within both groups without statistically significant difference. Also, the median procedural time did not differ between the groups. Other previous retrospective studies by Morvay et al. (7) and Sallustio et al. (25) did not analyze the influence of bridging treatment on procedural parameters. It can only be speculated that a further analysis of thrombus structure, such as atherosclerotic or of cardio-embolic origin, might contribute to predict the benefit of IVT before EVT. Further investigation on this aspect in designated RCTs are warranted.
The median time from stroke onset to recanalization was similar between both groups in our study. This is mainly attributed to the fact that in our treatment algorithm we do EVT without waiting for the clinical effects of bridging with IVT. This has to be taken into account compared to the study of Kass-Hout et al. (23), where time to treatment was significantly longer in the bridging group.
Previous meta-analyses and retrospective studies of mechanical thrombectomy show that EVT using the latest-generation stent-retrieval devices has high recanalization and low complication rates (26,27). Consistent with these data, our study showed high recanalization rates of up to 90% with state-of-the-art stent-retrieval devices. Slightly higher recanalization rates of 9% in the bridging therapy group vs. 89% in the EVT group were of no statistically significant difference. However, how far this minimal and not statistically significant effect could be attributed to synergetic effects of IVT and EVT with dissolving of small thrombi after the EVT procedure remains a subject for discussion.
A recently published hypothesis and proved data of IVT suggest a maximum operating peak up to 2 h after administration that could have contributed to the improved technical success rate (9).
How far other aspects, such as patient individual vessel anatomy and thrombus etiology, may have contributed to the recanalization rate remains unclear (28).
Regarding complications, rates of symptomatic ICH were not different in the bridging and EVT groups; however, there was a tendency for a higher asymptomatic bleeding risk in the bridging group, but without statistical significance (P = 0.09).
Finally, regarding clinical outcome, our results showed that patients who received IVT before EVT did not have significantly better neurological outcomes at dismissal or better late functional outcomes. This is consistent with previous single-center studies by Morvay et al. (7) and Kass-Hout et al. (23) where results also did not show better neurological or functional benefits of bridging. The study by Morvay et al. (7) randomized 40 patients between groups without contraindication for IVT and results did not show a higher benefit of IVT before EVT. Recent metaanalysis by Mistry et al. (29) on this topic including 13 retrospective studies unexpectedly showed significantly higher benefit from bridging treatment with better mRS score and lower mortality.
Despite slightly better results for technical success and later clinical outcome, IVT should still be considered as a treatment option in the established time window before EVT (30). In particular, in the hospitals where initiation of mechanical thrombectomy can be significantly delayed for any reason, this should be considered as a valuable option.
This study had some limitations: patient randomization; the prospective design; selecting patients for treatment with thrombolysis or directly with EVT. These decisions were determined by different factors: including contraindications for thrombolysis, doctors' preference and equipment availability. How far this introduced a selection bias and affected the outcomes can be only speculated. Further studies would require a dedicated multicenter RCT.
Despite the limitations of this study, we believe that bridging therapy may be particularly beneficial if there is a risk of significant delay of starting EVT due to logistic reasons. Unless further evidence of bridging therapy has been proven by dedicated RCT, current guidelines or practice should be applied.
zIn conclusion, the bridging therapy group did show slightly, but not significantly, higher recanalization and lower mortality rates with better neurological outcomes compared to EVT alone. The trade-off was a tendency to a higher risk of any hemorrhage in the bridging therapy group, but no significantly higher risk for symptomatic ICH. No significant impact on procedural time and number of attempts during EVT procedure was observed between the bridging therapy group and EVT alone.
Footnotes
Acknowledgments
We would like to thank Dr. H. Kidikas and Dr. A. Veiss for their assistance and contribution in patient selection and medical support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.