
Abstract
Background
Computed tomography (CT)-guided percutaneous transthoracic core needle biopsy (PTNB) is typically performed at 120 kVp tube voltage. However, there is no study that has demonstrated diagnostic performance including ground-glass nodules and radiation dose reduction at lower tube voltage in large population.
Purpose
To retrospectively compare the diagnostic performance and radiation dose between 100 kVp and 120 kVp during CT-guided PTNB.
Material and Methods
This study included 393 PTNBs performed in 385 patients (Group I; 120 kVp) from March 2011 to September 2011 and 1368 PTNBs performed in 1318 patients (Group II; 100 kVp) from October 2011 to December 2013. The patients underwent CT-guided PTNB with the coaxial technique. Diagnostic performance, complication rate, and radiation dose were compared between two groups.
Results
Technical success was achieved in 391 of 393 PTNBs (99.5%) in Group I and in 1344 of 1368 PTNBs (98.2%) in Group II (P = 0.09). The diagnostic accuracies for pulmonary lesions were not significantly different between two groups (97.1% [362/373] versus 96.2% [1202/1249], P = 0.458). Complication rate showed no significant differences between two groups in terms of pneumothorax (19.7% [77/391] versus 19.4% [261/1344], P = 0.904) and hemoptysis (2.3% [9/391] versus 3.2% [43/1344], P = 0.360). Among patients who developed pneumothorax, three patients (3.9%, 3/77) in Group I and eight patients (3.1%, 8/261) in Group II required treatment with drainage catheter. Nobody needed further treatment for hemoptysis in the two groups. The mean radiation dose was 1.5 ± 1.9 mSv in Group I and 0.7 ± 0.3 mSv in Group II (P < 0.001).
Conclusion
The 100-kVp protocol for CT-guided PTNB showed significant benefit of radiation dose reduction while maintaining high diagnostic accuracy and safety.
Introduction
Computed tomography (CT)-guided percutaneous transthoracic core needle biopsy (PTNB) is a commonly performed, safe, and accurate method for the diagnosis of lung nodules and masses, with a high diagnostic yield of 95.0–98.4%, even for small pulmonary nodules (1–5). The use of PTNB has grown recently due to the increased detection of indeterminate nodules by low-dose CT (LDCT) screening (6) and the need for histological determination of genetic mutation status in order to use the targeted drugs of lung cancer (7,8). As a result, procedure-related radiation exposure by CT-guided biopsy has gained attention. Although CT-guided biopsy uses a smaller radiation dose than conventional diagnostic CT, patients who are diagnosed with malignancy by PTNB will usually undergo several CT scans for follow-up and may result in considerable radiation exposure. Furthermore, the study by Pearce et al. (9) reported that even a relatively low irradiation from medical imaging in childhood can result in a small but excess risk for cancer. Therefore, radiation exposure during a procedure should be kept as low as possible.
Currently, CT-guided PTNB is typically performed at 120 kVp tube voltage with a reported mean estimated effective dose in the range of 2.7–5.3 mSv (5,10). Given that PTNB utilizes CT only for guiding the needle tract to locate a pulmonary nodule, image quality is not required comparable to conventional chest CT. Therefore, we assumed that CT-guided PTNB with lower tube voltage (100 kVp) and routine tube current may be sufficient.
However, there are few studies that have examined radiation dose reduction using CT-guided PTNB at lower tube voltage. Two previous studies reported diagnostic performance and radiation dose reduction with ultra-low dose (ULD) CT protocol (100 kVp and 7.5 mAs). They reported significantly lower radiation doses (0.3 mSv and 2.3 mSv) compared with standard-dose CT protocol with 92.0% and 95.8% of procedure success rate, respectively (10,11). Recently, Chang et al. reported a 68.6% reduction in the radiation dose (mean effective dose = 2.5 mSv) and no significant difference in diagnostic accuracy relative to standard-dose CT, when they used LDCT-guided PTNB (100 kVp and fixed 50 mAs) (12).
Although those studies demonstrated significant radiation dose reduction with the use of LDCT compared with standard dose CT protocol, it is difficult to apply the same protocol in routine clinical practice as the previous studies have been performed with relatively small populations (less than 100 patients). Furthermore, there are concerns regarding the detectability of ground-glass nodules (GGNs) using LDCT. Until now, there have been no studies regarding the diagnostic performance of CT-guided PTNB using low tube voltage (100 kVp) in large populations.
Therefore, the purpose of this study was to retrospectively determine and compare the diagnostic performance and radiation dose between low tube voltage (100 kVp) and conventional tube voltage (120 kVp) during CT-guided PTNB.
Material and Methods
This retrospective study was approved by our hospital’s institutional review board of Asan Medical Center and informed consent was waived.
Study population
Between March 2011 and September 2011, 393 consecutive CT-guided PTNBs using conventional tube voltage (120 kVp, Group I) were performed in 385 patients (mean age = 61.3 ± 9.2 years). There were 237 male patients (mean age = 62.9 years ± 11.3; age range = 19–86 years) and 148 female patients (mean age = 58.8 years ± 11.6; age range = 29–82 years). Between October 2011 and December 2013, 1368 CT-guided PTNBs using low tube voltage (100 kVp, Group II) were performed in 1318 patients (mean age = 62.9 ± 9.3 years). There were 782 male patients (mean age = 63.6 years ± 11.4; age range = 16–93 years) and 536 female patients (mean age = 61.9 years ± 11.4; age range = 33–94 years). The patients’ ages were normally distributed.
In Group I, CT-guided PTNBs were performed twice for the same pulmonary lesion in eight patients. In Group II, PTNBs were performed twice for the same pulmonary lesion in 37 patients and for different pulmonary lesion in 15 patients. In Group II, two patients underwent CT-guided PTNB twice for the same lesion and a third CT-guided PTNB for an additional lesion. In this study, repeat PTNBs were considered different initial cases of PTNB.
Of the 1761 CT-guided biopsy procedures in this study, 38 were included in the study population of a previous report (4). That study (4) dealt with the diagnostic outcomes of CT-guided aspiration and core biopsy for pulmonary nodules smaller than 1 cm, whereas our study focused on diagnostic performance and radiation dose reduction with the use of 100-kVp protocol for PTNB.
Biopsy procedure
All PTNBs were performed by ten attending chest imaging fellows who were under supervision, or by five chest radiologists with more than four years of experience with chest interventions. Each case was randomly assigned to one chest imaging fellow or experienced chest radiologist every month. Before the procedures, the operators reviewed the imaging examinations and planned the most effective needle pathway that would avoid bulla, emphysema, large proximal pulmonary vessels, airways, and fissures.
CT-guided PTNB procedures were performed with 64-MDCT (Somatom Definition AS; Siemens Healthcare, Erlangen, Germany). The parameters for Group I were 120 kVp, 25 mA reference, and 1.2 mm collimation with 1.5 mm or 3 mm axial slice thickness; the same parameters, except tube voltage (100 kVp), were used for Group II.
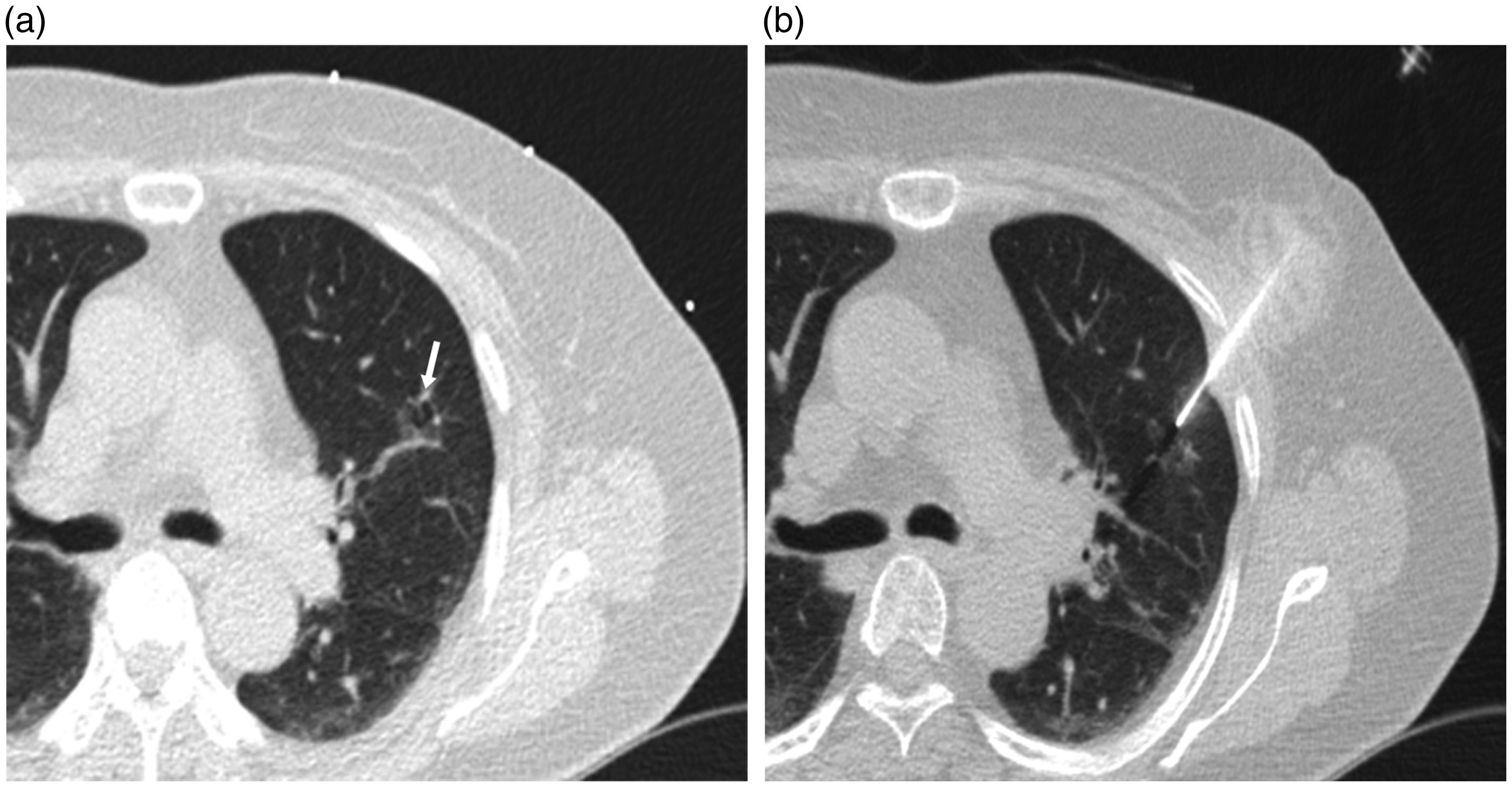
Patients were placed in a supine, prone, or lateral decubitus position depending on the location of the lesions. Localization was determined using a pre-procedural CT scan with a grid on the patients’ skin. Standard coaxial technique was performed using a 19-G coaxial introducer and a 20-G cutting needle (Pro-Mag 2.2, Manan Medical Products, Northbrook, IL, USA). After needle insertion, interval scans were acquired to assess the position of coaxial introducer. Final CT images were obtained to identify procedure-related complications (Fig. 1 & 2).
CT-guided biopsy using 100 kVp for GGN. (a) Pre-procedural CT at 100 kVp clearly demonstrates a 10-mm pure GGN (arrow) in the right lower lobe of a 52-year-old woman. (b) Although a metallic artifact due to the coaxial needle, biopsy was successfully performed without complications. The GGN was confirmed as invasive adenocarcinoma on both biopsy and surgical resection. CT-guided biopsy using 120 kVp for GGN. (a) Pre-procedural CT at 120 kVp shows a 17 mm GGN (arrow) with bubble lucency in the left upper lobe of a 72-year-old woman. (b) Minimal metallic artifact caused by the coaxial needle and biopsy gun was seen. Biopsy was successfully conducted without complications. The GGN was confirmed as invasive adenocarcinoma on both biopsy and surgical resection.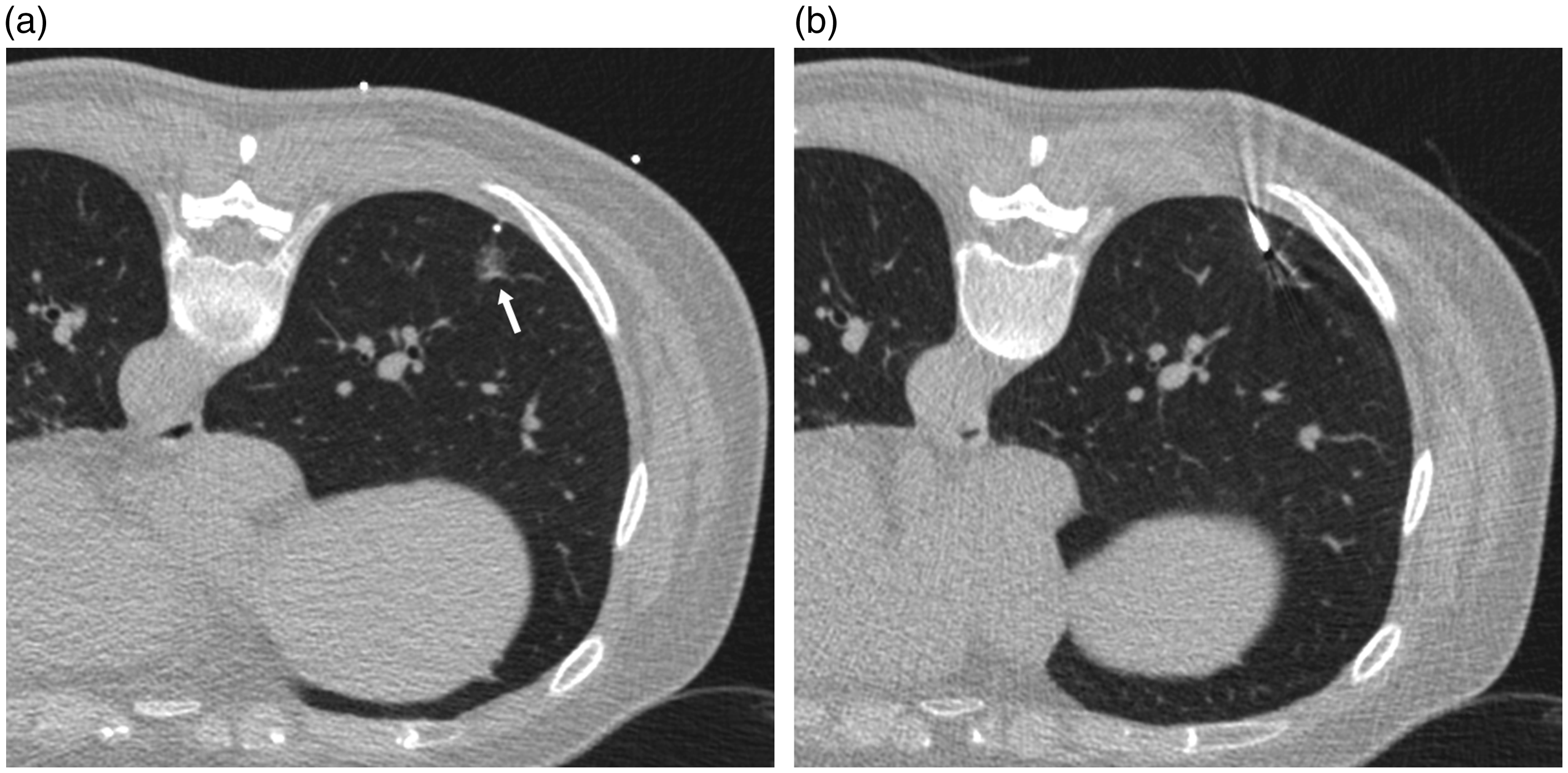
Data collection
The patients’ demographics (age, sex), characteristics of target lesions (lesion size, lesion location, depth from the pleura along the planned needle tract, and lesion type), and procedure-related variables (patient position, number of pleural passage, and number of tissue sampling) were recorded. The procedure time was defined as the time interval between the initial planning CT scan and the final CT scan. The radiation dose and dose-length product (DLP) were obtained from the value in the dose report. The effective dose was calculated from the product of DLP and conversion factors (0.017 mSv mGy−1 cm−1) (13). The development of pneumothorax was evaluated by the final CT scan or by follow-up radiography within two days. The occurrence of hemoptysis and air embolism was also recorded by operators based on patients’ symptoms and medical records. For evaluation of complication rate and radiation dose, cases determined as technical failure were excluded.
Assessment of diagnostic accuracy
Technical success was defined as the accurate localization of the coaxial introducer tip within the target lesion on CT scan and the presence of pathologic results. Operators visually determined the adequacy of the obtained specimen because an on-site cytopathologist was not available at our institution. Cases with malignancy and atypical cells in the pathology results were considered as true-positives, whereas those with specific benign diagnoses, such as hamartoma or tuberculosis, were considered as true-negatives. Cases that had non-specific benign findings, such as chronic inflammation or non-neoplastic lung parenchyma, were considered as true-negatives when the follow-up imaging showed more than 20% decrease in diameter or no interval change in size for more than two years; we considered the result as indeterminate if the non-specific benign findings did not meet these criteria (2). Non-specific benign findings on the pathology report that were otherwise diagnosed as malignant by surgical pathology or repeat biopsy were considered false-negatives. Technical failure and indeterminate results were excluded for the assessment of PTNB diagnostic accuracy.
The sensitivity, specificity, and accuracy for the diagnosis of malignant lesions were defined using the following equations: sensitivity = (number of malignant lesions – number of false-negative lesions)/number of malignant lesions; specificity = (number of benign lesions – number of false-positive lesions)/number of benign lesions; and diagnostic accuracy = (number of total lesions – number of false-negative or false-positive lesions)/number of total lesions.
Statistical analysis
All data were expressed as mean ± standard deviation. For continuous variables, the normality of distribution was assessed using the Kolmogorov–Smirnov test. The comparison of continuous data between the two different protocols was performed with an independent sample t-test. Chi-square test or Fisher’s exact test was used for the comparison of categorical data. A P value of less than 0.05 was considered statistically significant. The statistical package SPSS version 18.0 (SPSS Inc., Chicago, IL, USA) was used.
Results
Baseline characteristics
Technical success was achieved in 391 of 393 PTNBs (99.5%) in Group I and in 1344 of 1368 PTNBs (98.2%) in Group II (P = 0.09). The causes of technical failure in both groups consisted of uncontrolled breathing (n = 21), development of pneumothorax during the procedure (n = 3), and failure of needle localization into the target lesions (n = 2).
Demographics and baseline characteristics between CT-guided percutaneous transthoracic core needle biopsy using 120 kVp and 100 kVp.
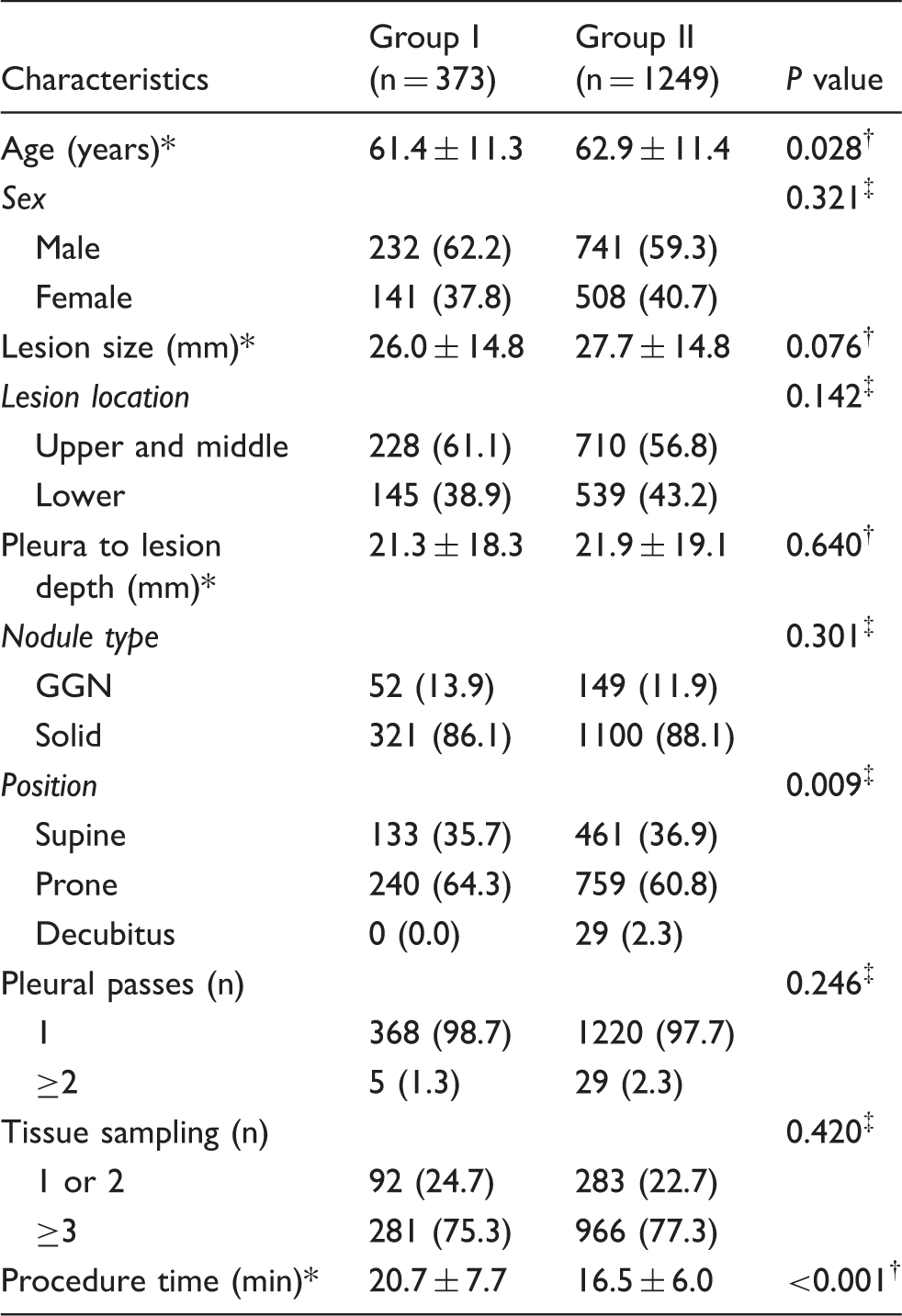
Unless otherwise indicated, data are numbers of procedures, with percentages in parentheses. All data were normally distributed.
Data are mean ± standard deviation.
Independent sample test.
Pearson’s chi-squared test.
Diagnostic accuracy
Final pathologic diagnoses in each group.
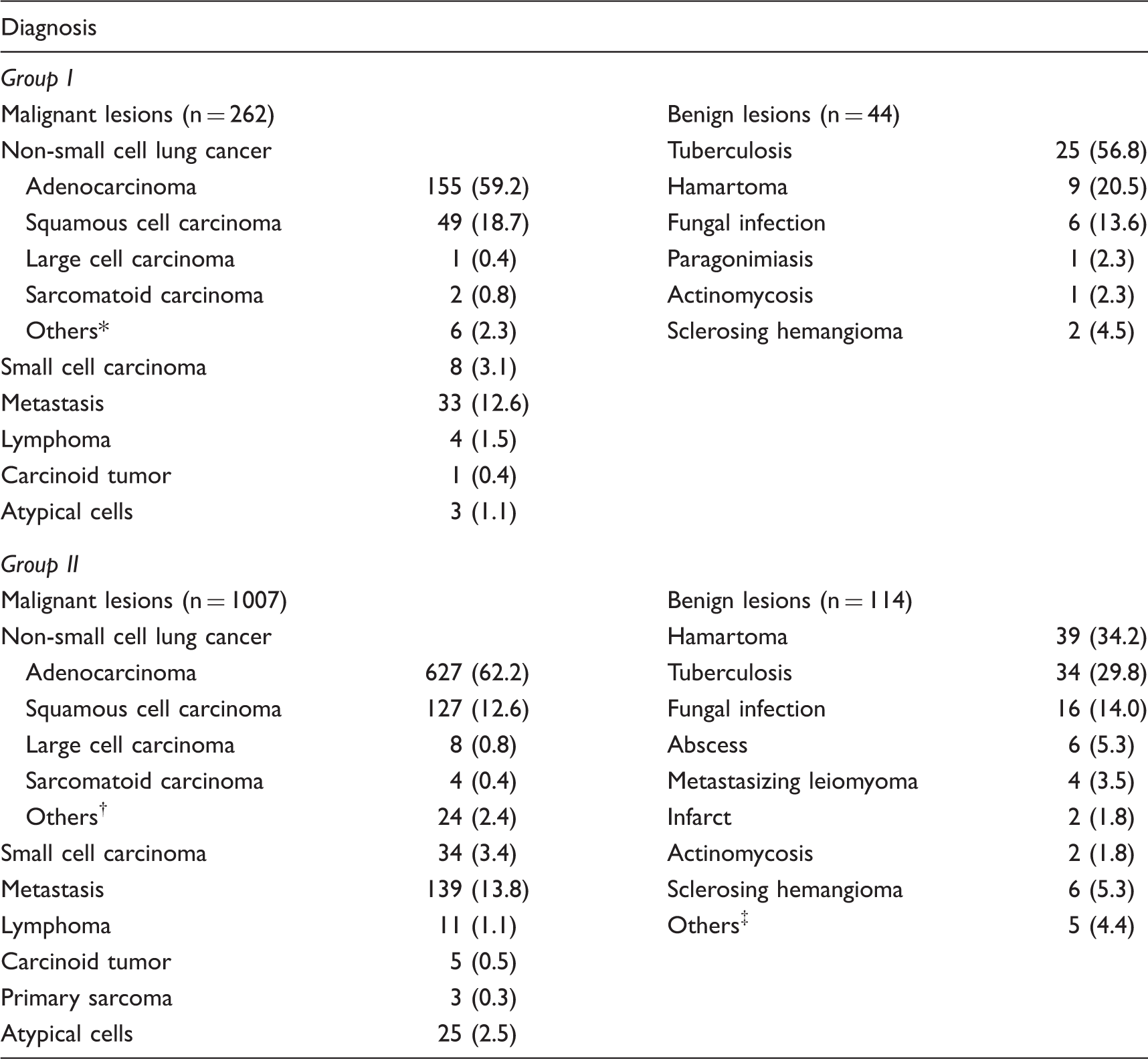
Data are numbers of lesions with percentages in parentheses.
Adenosquamous (n = 3) and unspecified non-small-cell lung cancer (n = 3).
Adenosquamous (n = 7) and unspecified non-small-cell lung cancer (n = 17).
Parasite infection (n = 1), Langerhans cell histiocytosis (n = 2), vascular malformation (n = 1), and amyloidosis (n = 1).
In Group II, 1007 of the 1344 lesions that were technically successful by PTNB were confirmed to be malignant by surgery (n = 827) or by the specific malignant biopsy results (n = 180). A total of 242 benign lesions were diagnosed by biopsy (n = 114) or follow-up (n = 128). The remaining 95 (7.1%) were indeterminate lesions. Of the 1007 malignant lesions, 47 were false-negative. The sensitivity, specificity, and accuracy of the diagnosis of malignant lesions in Group II were 95.3% (960/1007), 100% (242/242), and 96.2% (1202/1249), respectively.
Comparison of the radiation dose and outcome between 120-kVp and 100-kVp CT-guided percutaneous transthoracic core needle biopsy.
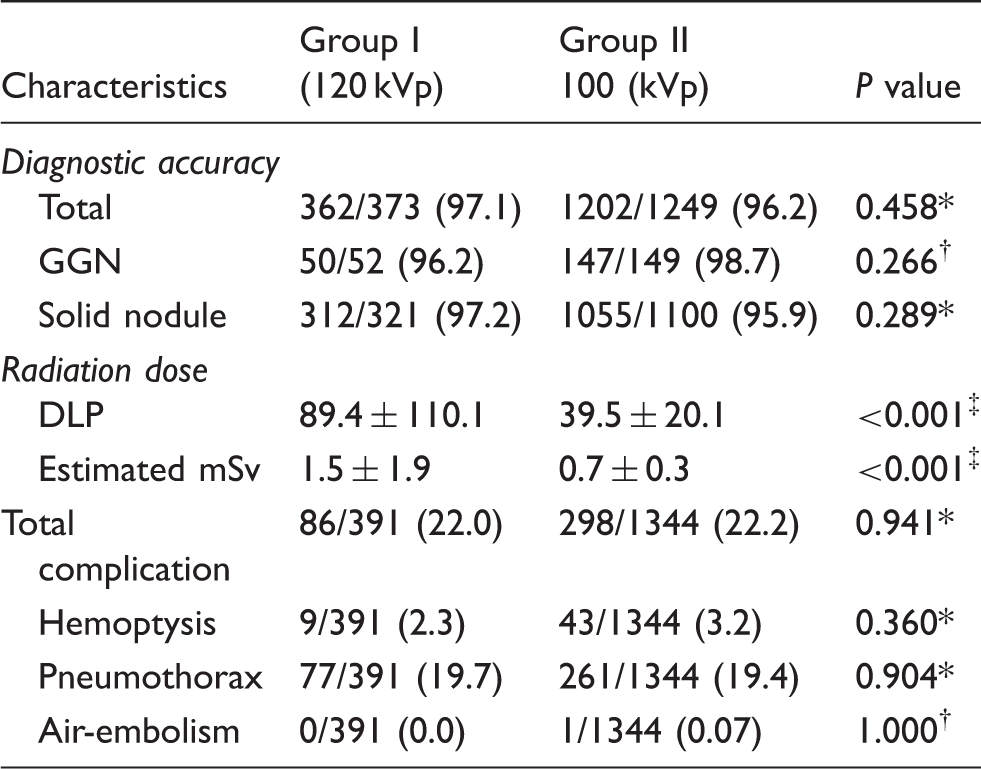
Unless otherwise indicated, data are numbers of procedures, with percentages in parentheses. All data were normally distributed.
Pearson’s chi-squared test.
Fisher’s exact test.
Independent sample t-test.
Complications
Pneumothorax occurred in 19.7% (77/391) and 19.4% (261/1344) of patients in Group I and Group II, respectively. Hemoptysis occurred in 2.3% (9/391) and 3.2% (43/1344) of patients in Group I and Group II, respectively. The overall and individual frequency of the complications did not differ significantly between the two groups (overall: P = 0.941; pneumothorax: P = 0.904; hemoptysis: P = 0.360).
Of the 77 cases of pneumothorax in Group I, three patients (3.9%, 3/77) required drainage catheter insertion and two patients (2.6%, 2/77) were treated with air aspiration during the procedure. Of the 261 cases of pneumothorax in Group II, eight patients (3.1%, 8/261) needed treatment with drainage catheter insertion. Bronchial artery embolization was not required in patients who developed hemoptysis. In Group II, air embolism was detected in one patient (0.07%, 1/1344) who had symptoms of dizziness and drowsiness (Fig. 3). The patient was discharged without sequelae of symptoms. There was no mortality in our study.
Symptomatic air-embolism after CT-guided biopsy. (a) A 23-mm irregular solid nodule (arrow) in the left lower lobe of a 60-year-old man is shown on CT. (b) The coaxial needle was localized precisely within the nodule. Three tissue samplings were performed. (c) On post-procedural CT, parenchymal hemorrhage and pneumothorax were detected. Immediately after the last CT scan, he complained of dizziness and drowsiness. His blood pressure dropped to 67/50 mmHg. Emergency measures were taken and he fully recovered without sequelae. (d) A retrospective review of post-procedural CT revealed air bubbles (arrow) in the left ventricle and we considered that the event may be related to air embolism. The nodule was confirmed as squamous cell carcinoma.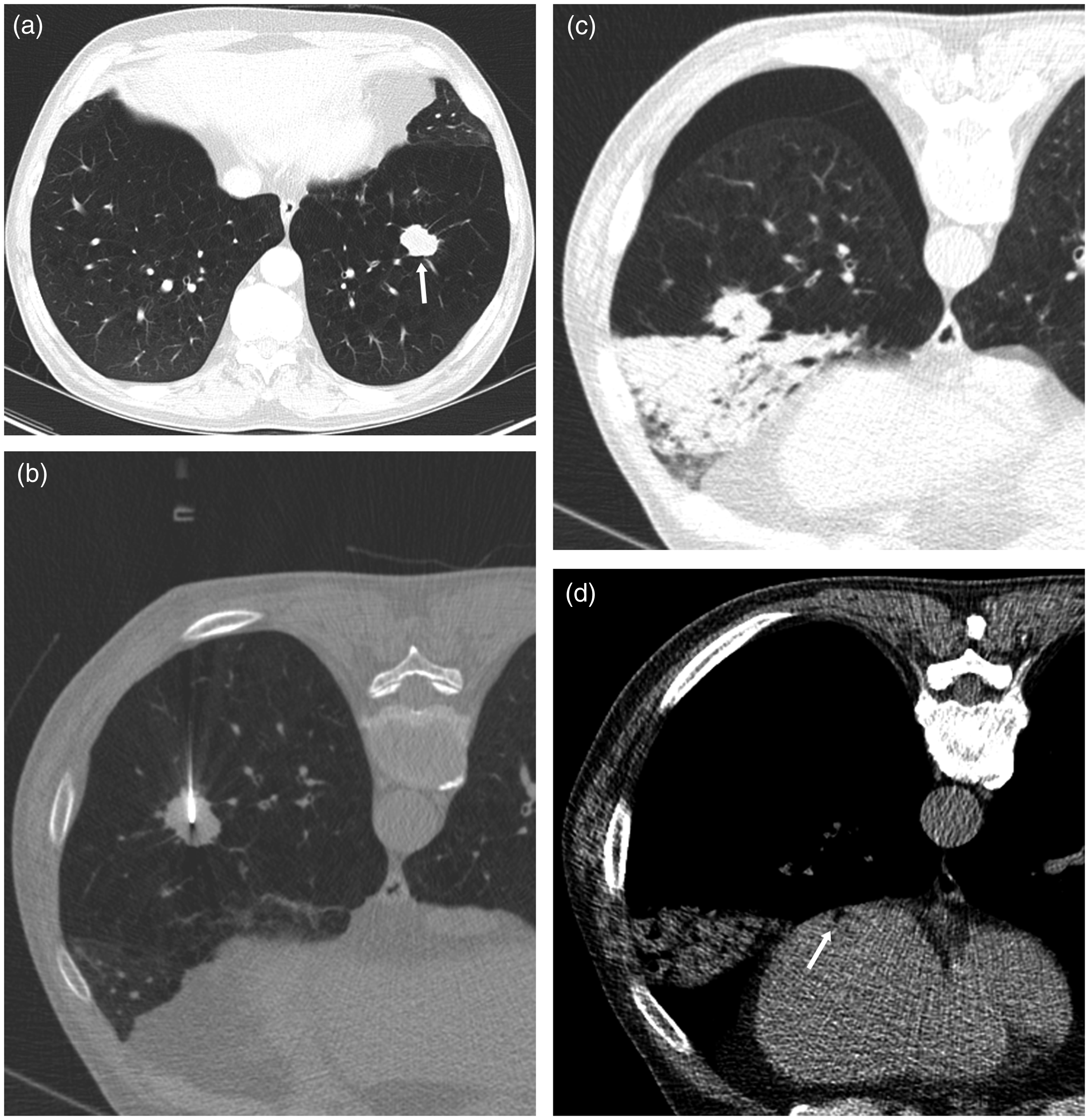
Radiation dose
The mean values of DLP and estimated effective radiation dose were 89.4 ± 110.1 mGy·cm and 1.5 ± 1.9 mSv, respectively, in Group I, and 39.5 ± 20.1 mGy·cm and 0.7 ± 0.3 mSv, respectively, in Group II. The mean DLP and estimated effective radiation dose were significantly lower in Group II than in Group I (P < 0.001 and P < 0.001, respectively) (Table 2). The radiation dose of Group II decreased by 53.3% compared with that of Group I.
Discussion
Our study was the first to investigate the feasibility of 100 kVp for CT-guided PTNB in a large population. In our study, the 100-kVp protocol was comparable with the 120-kVp protocol in both accuracy and safety. Our results were comparable to the diagnostic accuracy of 82.6% to 96.8% that were reported by previous studies that used standard dose protocol (120 kVp) (1,5,14,15).
For GGNs, Lu et al. (16) reported that the accuracy of PTNB using a 20-gauge cutting needle for GGNs that were smaller than 3 cm in diameter (mean size = 17.2 ± 7.3 mm) was 93.0% (40/43), and Kim et al. (17) reported a 91.3% (42/46) accuracy using 18-gauge or 20-gauge cutting needles for GGNs (mean size = 19.0 ± 9 mm). Our data showed a relatively higher diagnostic accuracy for GGNs compared with previous studies. Based on our results, we believe that a 100-kVp protocol can be used practically for all pulmonary lesions, including GGNs.
The rates of pneumothorax in this study were within the range (17.0–34.0%) that have been described in other studies (1–3). When comparing the two groups, there was no significant differences in our study. This may be due to the fact that they showed similar characteristics about risk factors for pneumothorax such as length of needle path-way, the number of pleural punctures, and lesion location (5,18).
The rate of hemoptysis in our study population (2.3% and 3.2%) was relatively low compared with rates reported in other studies (3.0–6.9%) (1,2,19). This difference may be attributed to the use of a 20-gauge cutting needle as well as the nodule characteristics in our population. The rate of hemoptysis was also not significantly different between two groups, and it may be related with no significant difference of risk factors for hemoptysis such as GGN lesions between two groups. Given our results, the reduction of radiation dose with the use of the lower 100 kVp was not considered to affect the risk for both pneumothorax and hemoptysis.
Air embolism occurred in one case of this study (0.07%). The incidence of air embolism has been reported to be in the range of 0.16–0.27% (20–23). In a multicenter study of 2216 lung biopsy procedures, Ishii et al. (23) reported that the risk factors associated with air embolism were parenchymal hemorrhage, lower lobe lesion, and the use of larger biopsy needles.
In this study, the 100-kVp CT protocol for PTNB reduced radiation dose by 53.3% compared with the 120-kVp protocol. As radiation dose is approximately proportional to the square of the change in tube voltage, a smaller change in tube voltage can result in a larger decrease in radiation dose (24,25).
There have been few studies examining the use of a low-kVp protocol for CT-guided biopsy. Chang et al. (12) reported the results of CT-guided biopsy in 65 patients using the LDCT protocol (pre-procedure/procedure = 100 kVp, 50 mA; post-procedure =100 kVp, 30 mA). However, the mean effective radiation dose in that study was 2.5 mSv, which was higher than that in our study (0.7 mSv). This difference may be related to the automatic exposure control with 25 mA reference that was used, and operators with well-educated technicians also have made a lot of efforts to optimize the scan range in our institute.
Two other studies used ULD CT protocol (100 kVp and 7.5 mA) for CT-guided lung biopsy (10,11). Although significant radiation dose reduction was achieved in both studies (0.3 mSv and 2.3 mSv), the study population was relatively small (n = 50 and n = 72) and diagnostic accuracy for GGNs was not assessed. Therefore, concerns regarding the general application of a ULD protocol to perform CT-guided biopsy remain.
Our study had several limitations. First, due to the retrospective study design, different numbers of patients were compared across the two groups. Nevertheless, we included a large number of patients, with similar demographics between the two groups. Second, the length of the scans varied according to the size of targeted lesions, patient size, and operator preferences; body mass index was not considered. These factors may affect the comparability of the radiation doses in both groups. Finally, we used DLP and mean effective radiation dose parameters on the CT dose report for evaluating radiation exposure.
In conclusion, the 100-kVp protocol for CT-guided PTNB was a highly accurate and safe diagnostic method for pulmonary lesions, including GGNs, with the advantage of radiation dose reduction compared with that using conventional tube voltage (120 kVp).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.