
Abstract
Introduction
According to the German Federal Office of Civil Protection and Disaster Relief (Bundesamt für Bevölkerungsschutz und Katastrophenhilfe—BBK) situation reports (also known as situation awareness, incident information, emergency public information, common operating picture, Blanchard 2007) are defined as “visual or textual information about a specific [disaster] event” (Bundesamt für Bevölkerungsschutz und Katastrophenhilfe (BBK) 2011, 36). They mainly include the “who, where, why, and how information about the crisis. An example would be where the crisis has occurred, its scope, and the timeline of events” (Taylor 2010, 414). Based on Coppola (2015), situation reports on disaster information are “(…) drawn from data. Datasets relevant to the disaster response and recovery contexts include both pre-existing and newly acquired collections” (Coppola 2015, 333). Against this background, it is not surprising that situation reports represent an essential tool for responders and public authorities (e.g., government, stakeholders, and media) in managing disasters like the COVID-19 pandemic, by enabling them to gain an overview about a specific situation and potential evidence-based solutions. Besides the fact that situation reports are relevant for the response to and recovery from a disaster or crisis, they are also relevant in adequately informing the public about the ongoing situation (Beneito-Montagut et al. 2013).
In the context of the COVID-19 pandemic in Germany, these situation reports were mainly characterized by epidemiological data (e.g., number of infected and later of the vaccinated individuals) and provided daily by the public health institute Robert Koch Institute (RKI) to the federal government as well as (in excerpts) to the public (Robert Koch Institute 2021). Despite the distribution of essential epidemiological information about the COVID-19 pandemic and its development to both the managing authorities and the general public in Germany, experts raised concerns about focusing mainly on the epidemiological situation (Lüttschwager et al. 2022) and complained regarding the lack of considering psychosocial information concerning, for instance, pandemic restrictions (Hering et al. 2021). To date, a huge number of international literature has documented the negative psychosocial consequences caused by the COVID-19 pandemic and its related restrictions (Knox et al. 2022). Therefore, the question arises to what extent the negative consequences could have been reduced (at least) if decision-makers had considered the psychosocial situation of the population when the pandemic started.
In order to highlight the importance of integrating psychosocial information into future crisis situation reports in addition to epidemiological or physical and damage information only, the current paper investigates the question of how people assessed the situation from their own perspective, and argues why psychosocial information should be considered as an integral part of situation reports. Based on the transactional model of stress and coping (Lazarus and Folkman 1984) as well as the psychometric paradigm of risk perception (Slovic, Fischhoff, and Lichtenstein 1982; Slovic 1987; Peters and Slovic 2000), we define the psychosocial situation report as a collection of central information of the population or population groups to describe both the experience and perception (e.g., risk perception) of as well as the behavior (e.g., coping) towards the direct or indirect consequences of a crisis or disaster that occurred. These factors are relevant as they lead to psychosocial consequences (e.g., stress) and are shaped by individual resources (e.g., self-efficacy) and risk factors (e.g., age; definition extended from Gerhold et al. 2021; Gerhold, Kröling, and Sterl 2022; Lüttschwager et al. 2022). In the following, we pose detailed research questions that are useful to guide psychosocial monitoring in the context of crises and present results of cross-sectional representative online surveys. Furthermore, we will discuss our findings alongside the existing literature and its added value for general crisis situation reports.
Literature review
Psychosocial aspects in situation reports during the COVID-19 pandemic
During the COVID-19 pandemic, the RKI published daily situation reports (Robert Koch Institute 2021) focusing on the epidemiological situation in Germany (e.g., the number of COVID-19 infections and deaths). At the end of February 2020, crisis management started to become operational (Federal Ministry of Health April 2020) until the end of the pandemic as a global health emergency in May 2023 (Wise 2023). Based on these epidemiological data, the German government imposed several countermeasures that focused particularly on social distancing, leading to contact restrictions (“AHA” campaign: “stay a minimum of 1.5 meters away from others,” “follow the hygiene standards,” “wear a mask”; German Federal Government 2020).
Even though the epidemiological data were central to the estimation of the pandemic situation, 65 German experts from the field of psychosocial crisis management (Hering et al. 2021) published a position paper that outlined the importance of considering the psychosocial situation as an integral part of the COVID-19 pandemic situation reports. They conclude that “psychosocial situation reports must record the experience and behavior of the population or individual population groups and analyze risks, resources, needs, and requirements so that concrete recommendations for action for interventions and, if necessary, supporting measures can be derived from them” (Hering et al. 2021, 2). Furthermore, during the COVID-19 pandemic, it became apparent that possible effects of the restrictions, such as the fear of an economic collapse, placed a significant burden on society (Boin, McConnell, and Hart 2021) and psychosocial well-being (Alsharawy et al. 2021)—even though controlling the spread of the virus epidemiologically was still the primary goal. Hence, crisis managers also had to deal directly (e.g., by providing social and emotional support) or indirectly (e.g., by providing information) with the psychosocial well-being of the population, pointing to an increased vulnerability due to the pandemic (see also Dückers et al. 2017). Accordingly, Veil and her colleagues argue that it is important to understand people's concerns and worries when developing a relationship between crisis management and the public (Veil, Buehner, and Palenchar 2011). Therefore, it seems crucial to collect empirical data which documents the needs, fears, and moods of the population. In this context, Gerhold, Wahl, and Dombrowsky (2019), Helmerichs, Karutz, and Geier (2017), Dückers et al. (2017), and Hering et al. (2021) refer to the concept of the “psychosocial situation” to describe the experiences of the general population or specific groups of people (e.g., experts in crisis management) as they deal with the direct or indirect consequences of a crisis or disaster that has occurred. According to interviews with coronavirus crisis managers in Germany, Lüttschwager et al. (2022) showed that the psychosocial situation was perceived as relevant for the management of the situation but was not performed systematically based on solid data. The interviewees mentioned a non-strategic way to obtain information about the psychosocial situation, such as reading social media posts or talking to friends and family, which may facilitate perceptual biases (Lüttschwager et al. 2022; also Kuhlmann et al. 2021). Thus, it seems essential to collect psychosocial information of the population in a systematic way to generate an adequate psychosocial situation report.
Risk perception and the COVID-19 pandemic
In line with a dual process perspective, humans process risks in two fundamental ways, namely in an experiential-affective and cognitive-analytical manner (Slovic et al. 2004; Slovic and Peters 2006). These processes relate to the examination of the cognitive perception of probability, susceptibility, and severity of potential harm or loss and the experience of fear and worry. The COVID-19 pandemic exposed a (physical) health risk to everyone in Germany, even though specific “risk groups” (e.g., persons older than 60 years) required more intensive forms of protection than others (Schilling et al. 2020). Since, in general, new and unfamiliar risks may be rated more harmful than known ones (Slovic 1987), it can be assumed that the risk perception of the COVID-19 pandemic may change over time due to habituation effects (Costa et al. 2022).
In this regard, COVID-19 monitoring projects were initiated during the pandemic in Germany, like the “COVID-19 Snapshot Monitoring” (COSMO; Betsch et al. 2020b) or the “Electronic Survey for the Coronavirus Situation in Germany” (EUCLID; Renner et al. 2020). These insights into public perceptions of risk, protective, and preparedness behaviors over time informed authorities, media, and the general population. For instance, the EUCLID project uncovered that personal experience with the coronavirus predicted the perceived risk and in turn adaption of individual measures and support for collective measures (Koller et al. 2022). Considering these findings, it seems sensible that both the EUCLID and the COSMO project demonstrate substantial variations of affective and cognitive risk perception and consequential protective behaviors against the spread of the virus over time (Rattay et al. 2021). Risk perception is related to engagement with individual protection and acceptance of crisis policies and varies over time and with experience (Dryhurst et al. 2020; Cipolletta, Andreghetti, and Mioni 2022). Thus, we consider it important to survey developments in how people perceive the risk of the ongoing crisis. This leads to the following research question:
With the sudden changes to the accessibility and safety of places due to the COVID-19 pandemic and restrictions introduced, researchers suggest that people's attachment to these places will shift, too, which may in turn affect the appraisal and response to the COVID-19 risks (Reese et al. 2020). A mobile experience sampling study with a low sample size documented different risk perceptions in safe versus public places (Restel et al. 2022). This leads to the assumption that risk perception might vary between places that people commonly occupy or visit like their home, public places and transit, or nature.
Against the background of the epidemiological pandemic development, it is important for crisis managers to know whether risk perception is dynamic along the respective risk situation (e.g., at home vs. in public transit) or whether risk perception—at least in a certain epidemiological pandemic phase—is to be assessed as static. Conversely, this could have considerable consequences for epidemiological pandemic development due to lower protection measures in specific places and thus higher risk of infections.
The situational dynamics of the crisis perception are therefore an important object of study to account for intrapersonal variations in the psychosocial situation report. For this reason, we derived the following research question:
While RQ1 and 2 delve into the extent and dynamics of perceived risk, they cannot explain why people appraise the risk that way. Based on Slovic's psychometric paradigm, which describes why people perceive critical developments as risky or not (Slovic, Fischhoff, and Lichtenstein 1982; Slovic 1987; Peters and Slovic 2000), risk perception is a multidimensional construct that primarily relies on subjective, qualitative risk attributes and not on the estimated (quantitative) probability of potential harm or loss (Gerhold, Wahl, and Dombrowsky 2019; Wiedemann and Schütz). The two main attributes describing the risk of the COVID-19 pandemic and many other hazardous events are whether the risk is unknown and dreadful (Bostrom et al. 2020). The attribute unknown connects to comparative studies showing, for example, that at the beginning of the pandemic, individuals estimated their own susceptibility to the new coronavirus as higher than to other well-known infectious diseases (Commodari, La Rosa, and Coniglio 2020). The perceived risk is also shaped by the dread it elicits. For instance, people that were more involved with the COVID-19 pandemic and more fearful and anxious also had a higher risk perception (Qian and Li 2020). The weighing of risk attributes of the pandemic versus the protective action in turn influences motivation and behavior. One year after the pandemic started, U.S. Americans generally perceived the pandemic as more dreadful but the vaccination as more unknown (Wong and Yang 2022). In this study, if an individual appraised the pandemic as more dreadful and unknown than the vaccination, this positively related to protective behavior and vaccination intention.
Thus, these qualitative attributes are highly relevant regarding the crisis management process and the psychosocial situation report because they shed light on whether the public understanding of the pandemic situation and countermeasures are adequate or not. Hence, we derive the following research question:
Transactional model of stress and coping and the COVID-19 pandemic
Well-established psychological models of stress and coping have shown that resources and coping strategies seem to contribute to stable health and the successful handling of stressful events (Antonovsky 1979; Lazarus and Folkman 1984; Becker 1992; Adler and Castro 2013). The transactional model of stress and coping (Lazarus and Folkman 1984; Lazarus 1991) defines stress as an interaction between the person and the environment, in which individuals appraise an event regarding both its personal relevance and their capacity to cope with it. Thus, the same event will not be perceived as equally stressful or coped with in the same way by all individuals; nor will it have the same impact on mental and physical health. The stress response depends on individual appraisals. When faced with a stressor, individuals make a primary appraisal and question whether a stressor is (potentially) harmful, benign, or irrelevant to them. Harm can be already experienced or anticipated as a threat or challenge. In this way, the primary appraisal of threat corresponds with risk perception. In a secondary appraisal, the individual considers whether they have the ability and resources to cope with the stressor. If the perceived abilities or resources are not sufficient to alleviate, adapt to, or buffer the harm or threat, stress may arise as a psychosocial consequence.
Along with appraisal, coping is seen as a key process in the model. In general, coping refers to the cognitive and behavioral strategies available to face challenges, harms, and threats, and is classified as either problem-focused or emotion-focused (Lazarus and Folkman 1984). Problem-focused coping strategies target the stressor itself. Individuals reflect on what is being (or has been) experienced in a stressful situation to reach a better understanding of it or to develop plans of action to change the situation (Folkman and Lazarus 1985; Gerhold, Kröling, and Sterl 2022). Emotion-focused coping regulates the emotions related to the stressor and aims at reducing emotional distress without directly addressing the cause of this distress (Folkman and Lazarus 1980). Numerous studies provide empirical support for the transactional model of stress and coping (e.g., van Bavel et al. 2020; Obbarius et al. 2021). Moreover, research shows that perceived control over the stressor influences the selection and effectiveness of coping strategies. When the situation is appraised as controllable, problem-focused coping is increasingly and more effectively used (Cheng 2001). In situations with low control perceptions, individuals increasingly use more emotion-focused coping strategies and rate them as more effective (Cheng 2001).
As risk situations like the COVID-19 pandemic represent a stressor that poses immediate threats to individuals and society (Lazarus and Folkman 1984; López-Vázquez and Marván 2003; Banerjee and Rai 2020) there is a growing body of research applying the transactional model of stress and coping to the COVID-19 pandemic. For instance, Welter, Welter, and Großschedl (2021) measured the primary and secondary appraisal regarding COVID-19 risks to determine a stress index. In doing so, the authors found that the perception of the COVID-19 pandemic as frightening or challenging declined over time which was reflected by decreases in protection behaviors. Concerning the secondary appraisal, it has been shown that, when individuals were not equipped with sufficient coping resources during the COVID-19 pandemic, they were more likely to experience negative psychosocial outcomes (Budimir, Probst, and Pieh 2021; Minahan et al. 2021; Cohrdes et al. 2023).
To better understand COVID-19 pandemic-related coping, the distinction between problem-focused and emotion-focused coping is useful. Problem-focused behavior in this context aims, for instance, at avoiding an infection. Emotion-focused coping may lead individuals to assess the risk in different ways, ignoring the existence of the virus or distancing themselves from its impact, like by avoiding or downplaying news reports. In this regard, Shigeto et al. (2021) found six qualitatively different typologies of coping (such as “Non-Resilient Flexible Problem-Focused Copers”) among young adults during the pandemic. In the context of the COVID-19 pandemic, most research focuses on problem-focused coping, namely protective actions such as washing and disinfecting hands, wearing face masks, avoiding people who belong to the so-called risk groups, avoiding public places, etc. (e.g., Luszczynska, Knoll, and Scholz 2020; Rieger 2020; Betsch et al. 2020b, 2020a; Perrotta et al. 2021). However, there has been little research into which different problem-focused as well as emotion-focused coping strategies individuals use to manage the demands of the COVID-19 pandemic. For instance, avoiding negative emotions and stressors, for example, through consumption of alcohol and other drugs, predicted increased depressive and anxiety symptoms, loneliness, and insomnia (Budimir, Probst, and Pieh 2021; Minahan et al. 2021). On the other hand, trying to find new meaning during the pandemic through positive reappraisal, was connected to psychological adaptation, for instance, to a higher quality of life and lower depressive and anxiety symptoms and stress (Budimir, Probst, and Pieh 2021; Cohrdes et al. 2023). The current study aims to understand the ways in which people cope with COVID-19 to reduce their perceived stress associated with the pandemic.
Methods
Procedure
To answer our research questions, we conducted four cross-sectional, online representative surveys (in terms of age, sex, and German federal state) using an ISO-certified panel provider Respondi (now called Bilendi, Germany). The surveys were conducted across a stratified quota sample, interviewing four online panels of respondents in Germany from March 19–23 (Survey 1), April 15–21 (Survey 2) and May 7–19, 2021 (Survey 3), and December 20, 2021 to January 2, 2022 (Survey 4). At first, a random sample from the population of the online access panel was drawn based on sociodemographic information. Then, a quota or, a stratification module was used.
The interviews lasted for 16.4 min (Survey 1), 8.8 min (Survey 2), 24.4 min (Survey 3), or 29.4 min (Survey 4) on average. The whole study was conducted according to the Code of Ethics of the World Medical Association (World Medical Association (WMA) 2013) and the General Data Protection Regulation (GDPR). Moreover, all subjects involved in the study gave their written informed consent. All information was collected anonymously.
Participants
In general, all respondents were between 18 and 74 years old (due to limitations of the panel provider). Those with a response time of less than the first 5% percentile of interview length were removed in each wave. Thus, Survey 1 comprises 1,242 valid interviews with 50.7% female and 49.3% male respondents and an average age of 46.0 years (SD = 15.1 years). Survey 2 includes 945 respondents with a proportion of both 50.0% female and male, participants being 45.5 years old on average (SD = 15.2 years), while Survey 3 comprises 1,341 respondents with 50.7% female and 49.3% male participants averaging 46.0 years in age (SD = 15.3 years). Finally, Survey 4 includes 1,397 participants with 51.2% female and 48.8% male respondents (M = 46.4 years; SD = 15.1 years).
Measures
To answer RQ1, we measured the cognitive and affective (quantitative) risk perceptions as well as age (grouped in five categories) and sex (male vs. female) for Surveys 1 to 4 to compare any differences between subsequent time points. For RQ2, we measured the quantitative risk perceptions and location-specific subjective feeling of safety for Survey 1 to compare both at the beginning of the COVID-19 pandemic. Then, we measured the risk characteristics of COVID-19 as well as problem-focused and emotion-focused coping strategies to study RQ3 and RQ4 for Survey 1, when COVID-19 started spreading in Germany in March 2020.
Quantitative risk perceptions
Affective risk perception
To assess affective risk perception in all four surveys, we used two different items about personal worry (e.g., “COVID-19 (Coronavirus SARS-CoV-2) worries me.,” RPA1) and fear (RPA2) using a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree) adapted from Trumbo et al. (2016) (see Table 1).
Items for the measurement of risk perception of being infected by COVID-19.
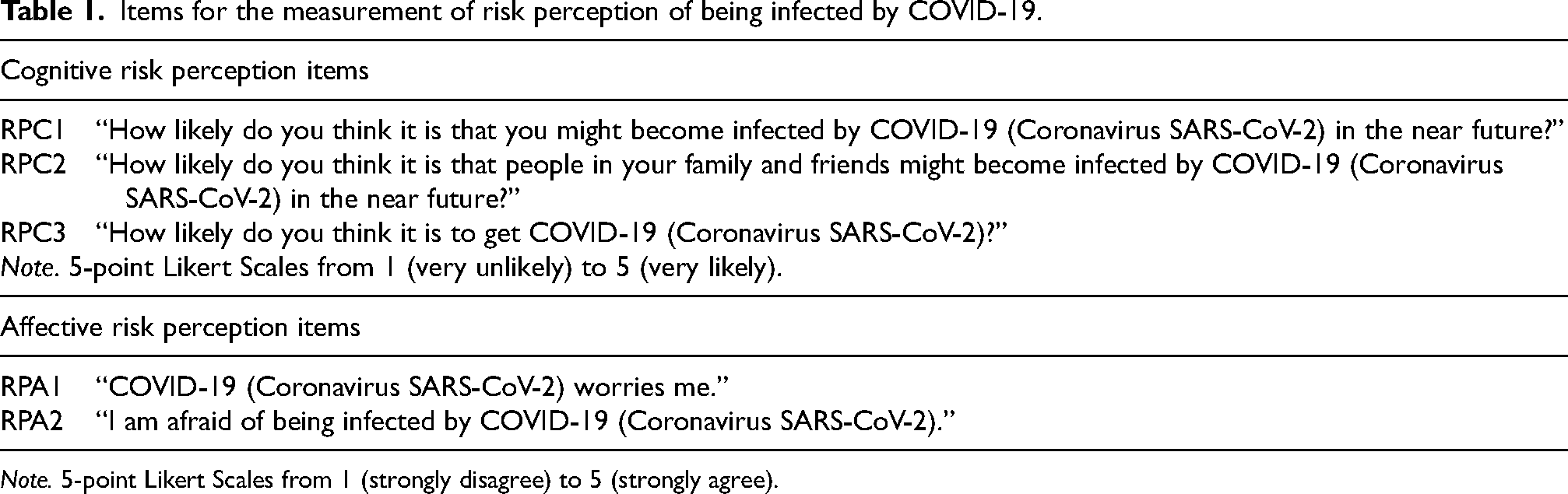
Note. 5-point Likert Scales from 1 (strongly disagree) to 5 (strongly agree).
Cognitive risk perception
In total, we measured cognitive risk perception with three different items to rate the likelihood of getting infected by COVID-19 soon (RPC1) and in general (RPC3, e.g., “How likely do you think it is to get COVID-19 (Coronavirus SARS-CoV-2)?”). Also, one item asked about the likelihood of the respondent's family and friends to get infected by COVID-19 (RPC2). We used a 5-point Likert scale ranging from 1 (very unlikely) to 5 (very likely) adapted from the 4-point Likert scale by Quah and Hin-Peng (2004) and since Survey 2 was shorter, we only measured RPC3. See Table 1 for the complete item wording.
Perceived characteristics of COVID-19
To measure the perceived characteristics of COVID-19, we adapted 19 items that addressed the “dread risk” and “unknown risk” dimensions (Slovic 1987; Jenkin 2006) that can help to describe COVID-19 from a subjective point of view. We used 13 items such as “COVID-19 (Coronavirus SARS-CoV-2) is a global disaster” to measure the subdimension “global catastrophe” as “dread risk,” whereas we presented six items like “COVID-19 (Coronavirus SARS-CoV-2) is something completely new for all of us” to examine, for instance, a new risk as “unknown risk.” The items were scrutinized in Survey 1 using a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree) (see Tables 2 and 3).
Characteristics of risk perception: “Dread Risk” characteristics.
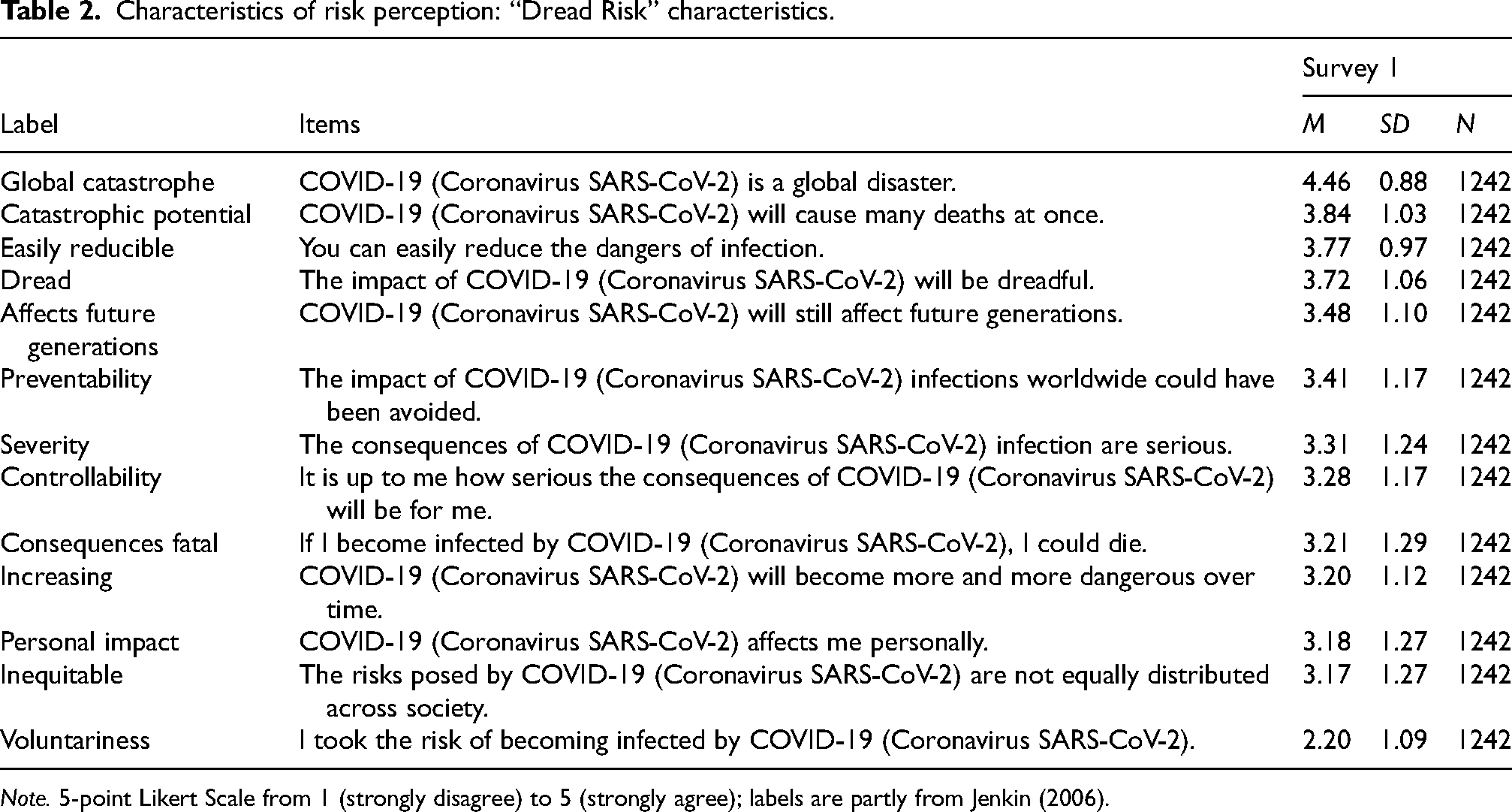
Note. 5-point Likert Scale from 1 (strongly disagree) to 5 (strongly agree); labels are partly from Jenkin (2006).
Characteristics of risk perception: “Unknown Risk” characteristics.
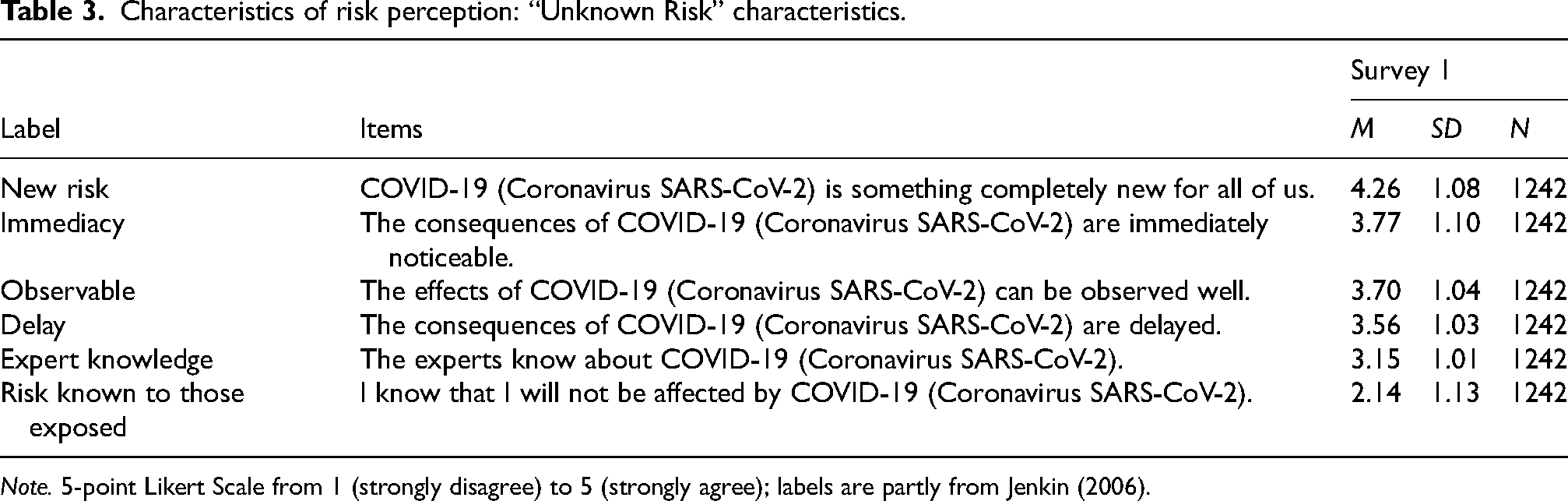
Note. 5-point Likert Scale from 1 (strongly disagree) to 5 (strongly agree); labels are partly from Jenkin (2006).
Location-specific subjective feeling of safety
To measure the subjective feeling of safety by location for Survey 1, we used a five items battery on a 5-point Likert scale from 1 (very unsafe) to 5 (very safe) adapted from Gerhold (2020). We introduced the item battery with the question “How safe do you feel…?” The respondent could then rate, for example, the subjective safety for private places like “… in your own home” or public places, such as “… outside your home in shops or restaurants” (see Table 4).
Cognitive and affective risk perception and places (Survey 1).
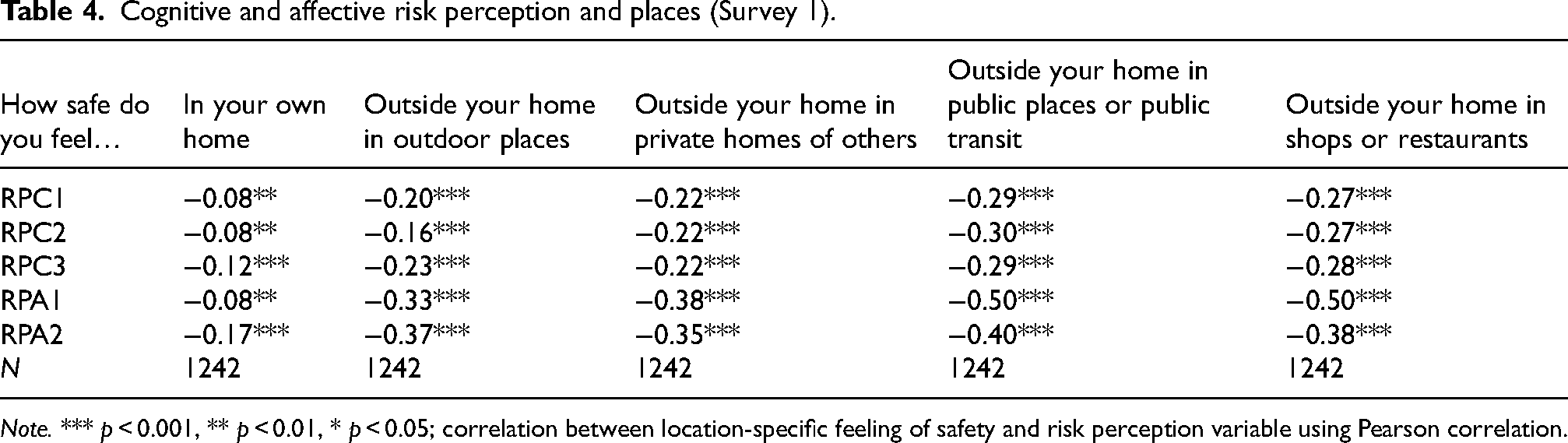
Note. *** p < 0.001, ** p < 0.01, * p < 0.05; correlation between location-specific feeling of safety and risk perception variable using Pearson correlation.
Coping strategies
Finally, we measured problem-focused and emotion-focused coping strategies in the context of COVID-19 with 27 questions adapted from a scale by Ferring and Filipp (1989) for Survey 1 in March 2020. First, we introduced the item battery with the following text: “Below we ask you some questions about how to deal with COVID-19 (Coronavirus SARS-CoV-2). When you think of COVID-19 (Coronavirus SARS-CoV-2), to what extent do the statements regarding the way you deal with it apply?” Then, respondents could rate 14 problem-focused items such as “I listen to the experts and follow their advice” and 13 emotion-focused items like “It will emerge over time; there is nothing more to do but wait” on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree) (see Tables 5 and 6). To compare the overall means of problem-focused and emotion-focused coping, we checked Cronbach's alpha values (alpha = 0.80 and alpha = 0.79, respectively), which are rather good before computing a scale for the two using the overall mean of all single items for both coping strategies.
Problem-focused ways of coping.
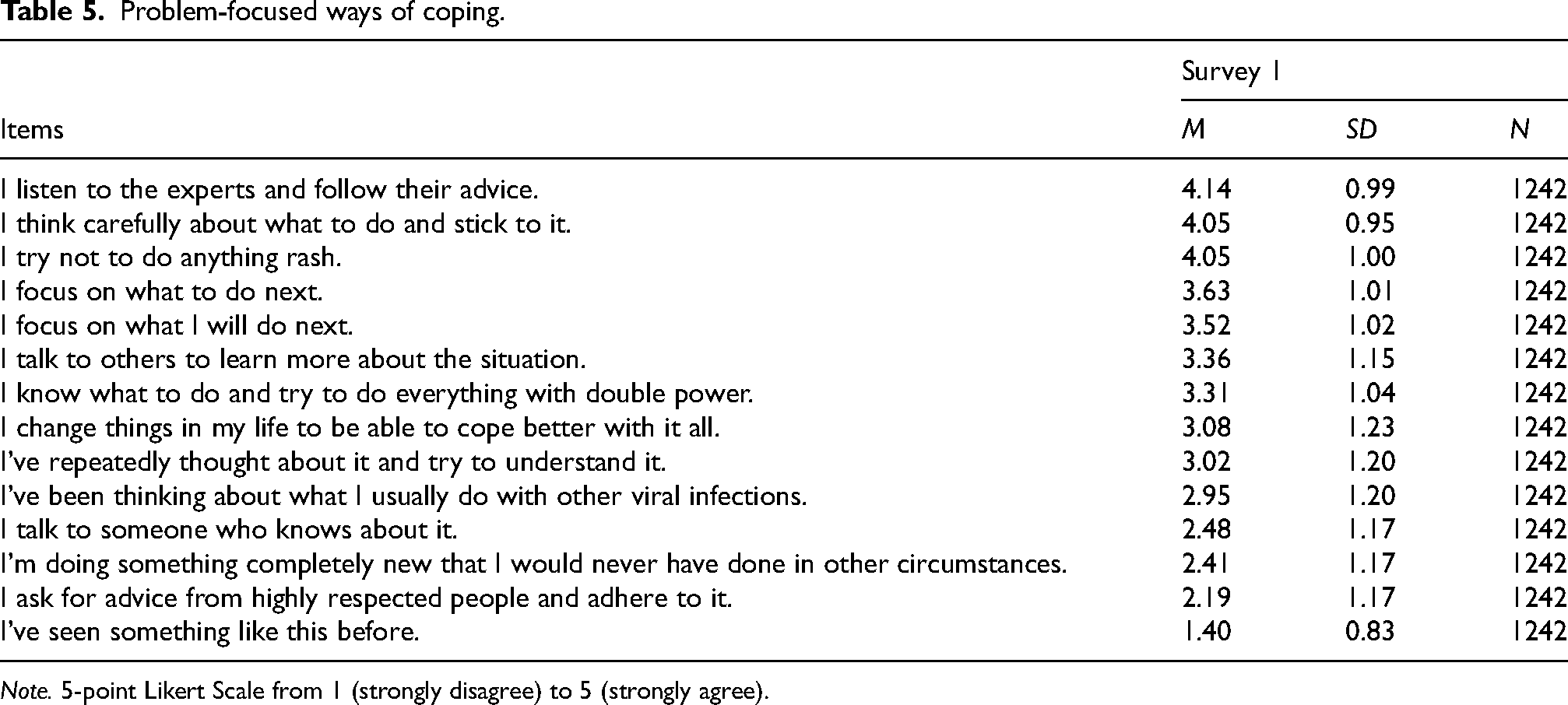
Note. 5-point Likert Scale from 1 (strongly disagree) to 5 (strongly agree).
Emotion-focused ways of coping.
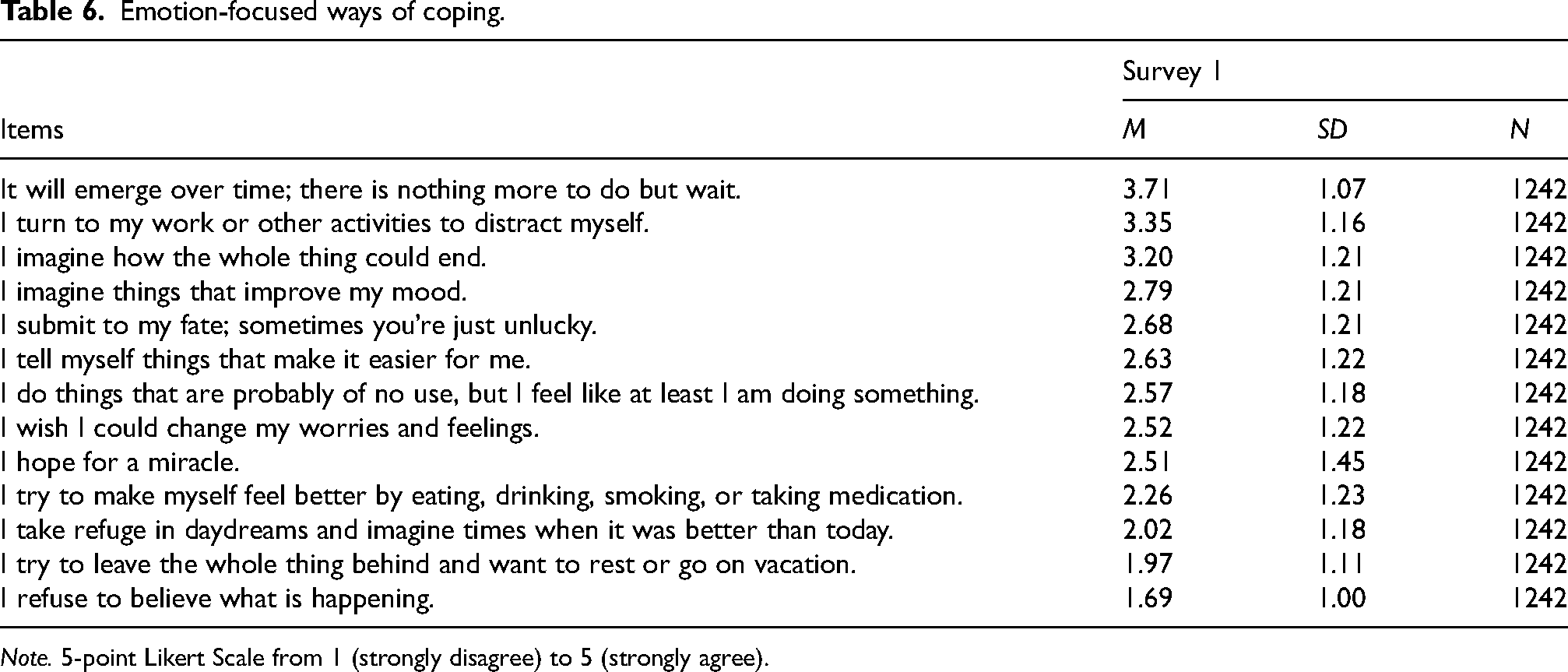
Note. 5-point Likert Scale from 1 (strongly disagree) to 5 (strongly agree).
Statistical analyses
To prepare and analyze the survey data, we used the statistical software Stata 17 (StataCorp 2021). After data cleaning, we conducted univariate as well as bivariate analyses to examine RQ1. To analyze the change of risk perception over time, we computed independent t-tests of means between directly sequential surveys (e.g., between Surveys 1 and 2 or Surveys 2 and 3, see Table 7). To study differences in sex per survey wave, we conducted independent t-tests and, for age, Pearson correlations between each dimension of risk perception and the metrically surveyed age (see Tables 8 and 9). For RQ2, after describing the relative percentages of people (strongly) agree to the items, we conducted Pearson correlations between the perceived feeling of safety and each dimension of the quantitative risk perceptions (see Table 4). For RQ3 as well as for RQ4, means of both dimensions of perceived characteristics of COVID-19 and coping strategies, respectively, are depicted in descending order to show the highest rated items in each (see Tables 2, 3, 5 and 6).
Development of cognitive and affective risk perceptions over time.
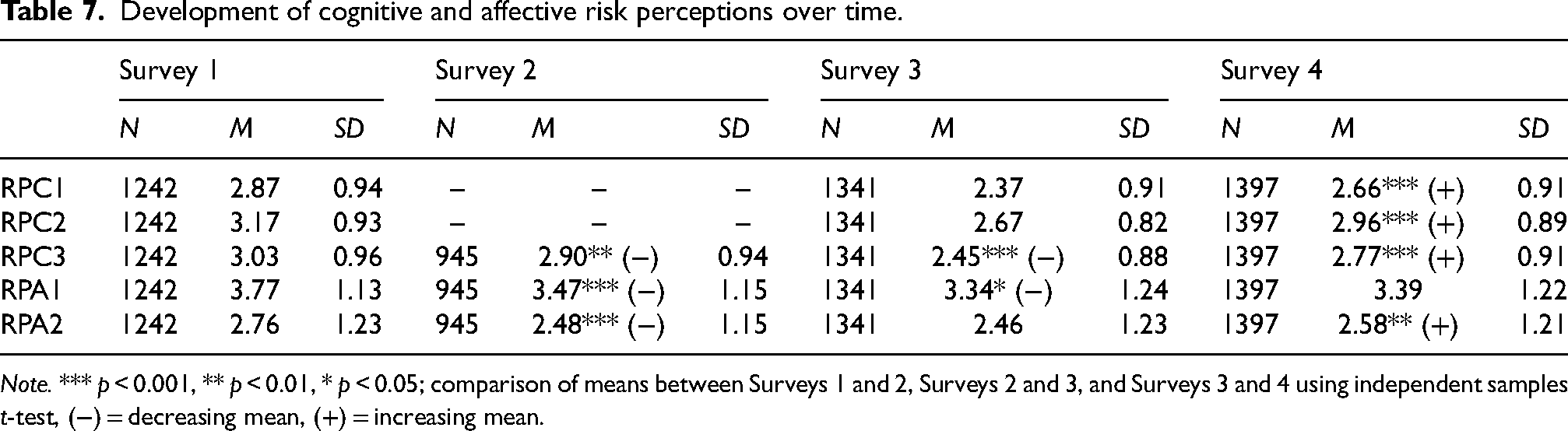
Note. *** p < 0.001, ** p < 0.01, * p < 0.05; comparison of means between Surveys 1 and 2, Surveys 2 and 3, and Surveys 3 and 4 using independent samples t-test, (−) = decreasing mean, (+) = increasing mean.
Development of cognitive and affective risk perception over time, by sex.
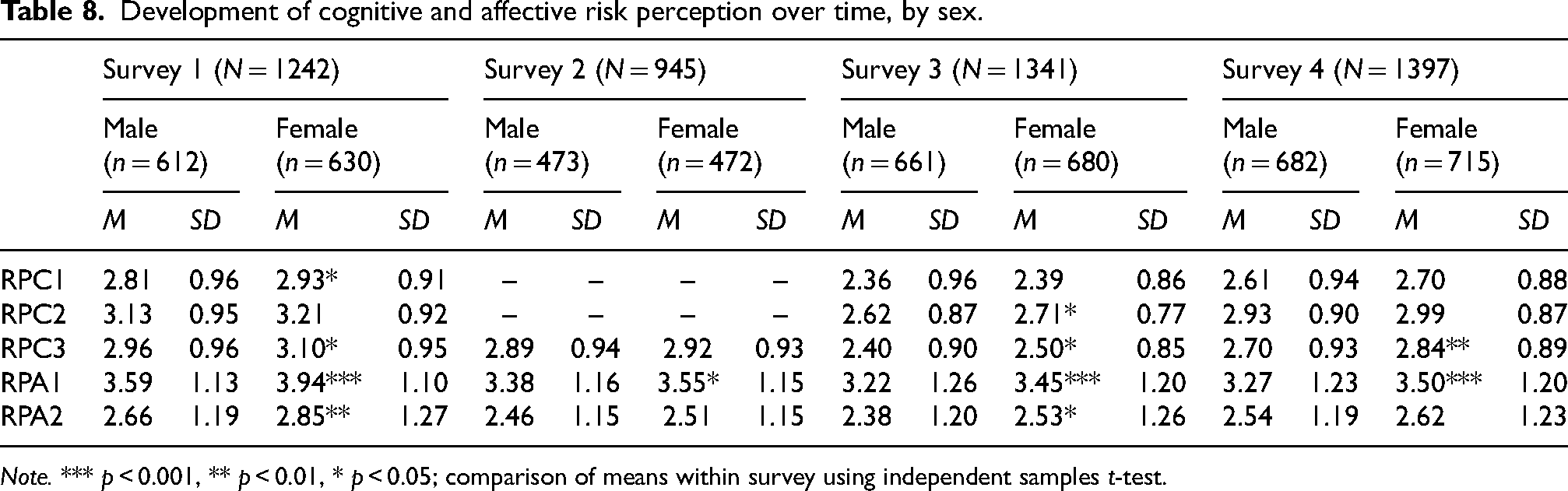
Note. *** p < 0.001, ** p < 0.01, * p < 0.05; comparison of means within survey using independent samples t-test.
Development of cognitive and affective risk perception over time, by age.
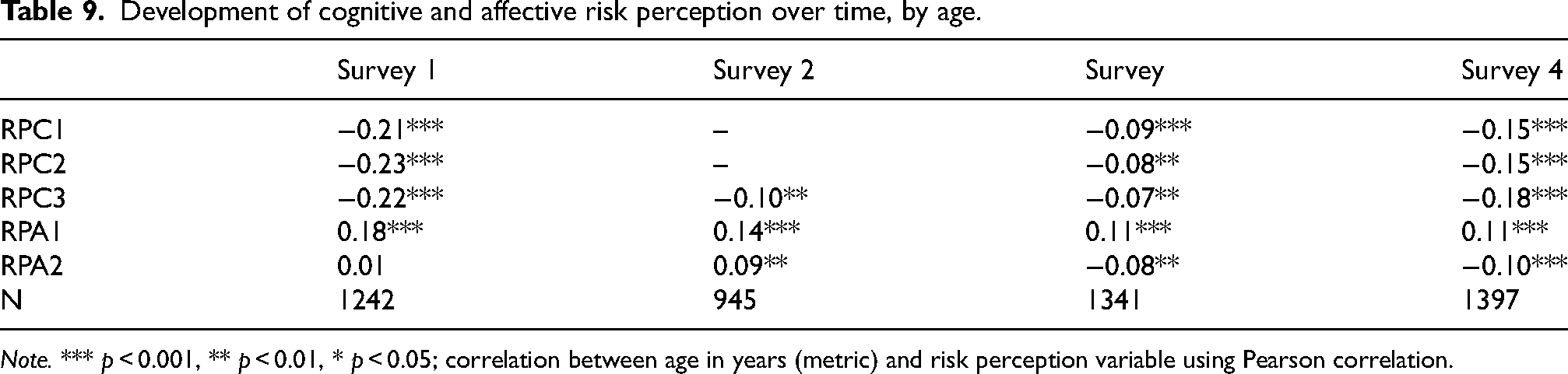
Note. *** p < 0.001, ** p < 0.01, * p < 0.05; correlation between age in years (metric) and risk perception variable using Pearson correlation.
Results
RQ1: Risk perception during the COVID-19 pandemic in Germany
Our first research question addressed the risk perception during the COVID-19 pandemic in Germany. In March 2020 (Survey 1), both cognitive and affective risk perceptions were rated higher compared to the subsequent surveys (see Table 7). Data shows that the likelihood of family and friends to be infected (RPC2) is highest among the cognitive dimensions (M = 3.17, SD = 0.93), whereas respondents are highly worried about COVID-19 in general (M = 3.77, SD = 1.13; RPA1), but are less afraid of becoming infected (M = 2.76, SD = 1.23; RPA2).
Compared to Survey 1, the likelihood of getting infected with COVID-19 in general (t(2185) = 3.02, p < 0.01; RPC3) as well as being worried (t(2185) = 6.13, p < 0.001; RPA1) and being afraid of COVID-19 (t(2185) = 5.30, p < 0.001; RPA2) are significantly decreasing in Survey 2 (April 2020). When comparing Surveys 2 and 3 (May 2021), it can be seen that both the likelihood of getting infected with COVID-19 in general (t(2284) = 11.79, p < 0.001; RPC3) and being worried about COVID-19 (t(2284) = 2.52, p < 0.05; RPA1) decrease significantly from Surveys 2 and 3, whereas there is no change in fear about COVID-19 (t(2284) = 0.51, p > 0.05; RPA2). Interestingly, all risk perceptions except being worried about COVID-19 (t(2736) = −1.10, p > 0.05, RPA1) increase between Surveys 3 and 4 (December 2021/January 2022) again. All cognitive dimension items—namely, the likelihood of getting infected in the near future (t(2736) = −8.20, p < 0.001; RPC1), getting infected in general (t(2736) = −9.35, p < 0.001; RPC3) and the likelihood of family and friends becoming infected (t(2736) = −8.86, p < 0.001; RPC2)—are significantly higher than in Survey 3. Regarding the affective dimensions, only being afraid of getting COVID-19 (t(2736) = –2.66, p <0.01; RPA2) is significantly higher than in Survey 3.
Differentiated by sex, the near-term likelihood of being infected with COVID-19 (RPC1) is rated slightly yet significantly higher by women than men only in Survey 1 (t(1240) = −2.17, p < 0.05) whereas the likelihood of family and friends getting infected by COVID-19 (RPC2) is rated higher for women in Survey 3 (t(1339) = −2.14, p < 0.05) only (see Table 8). Also, the likelihood of getting infected in general (RPC3) is rated significantly higher by women in Survey 1 (t(1240) = −2.53, p < 0.05), Survey 3 (t(1339) = −2.14, p < 0.05) and Survey 4 (t(1395) = −2.91, p < 0.01) apart from Survey 2 (t(943) = −0.59, p > 0.05). Concerning the affective risk perceptions, worrying about COVID-19 (RPA1) is significantly higher for women in all surveys (t(1240) = −5.50, p < 0.001 for Survey 1; t(943) = −2.25, p < 0.05 for Survey 2; t(1339) = −3.52, p < 0.001 for Survey 3; t(1395) = −3.60, p < 0.001 for Survey 4). However, women are more afraid concerning COVID-19 (RPA2) in Survey 1 (t(1240) = −2.83, p < 0.01) and Survey 3 (t(1339) = −2.22, p < 0.05) only.
Age is negatively correlated with the cognitive dimensions of risk perception throughout all surveys (see Table 9). The likelihood of getting infected in the near future (RPC1) and of family and friends catching COVID-19 (RPC2) is significantly lower with increasing age for Survey 1 (r = −0.21, p < 0.001; r = −0.23, p < 0.001), Survey 3 (r = −0.09, p < 0.001; r = −0.08, p < 0.01), and Survey 4 (r = −0.15, p < 0.001; r = −0.15, p < 0.001). Also, getting infected with COVID-19 (RPC3) in general is negatively associated with older people (r = −0.22, p < 0.001 for Survey 1; r = −0.10, p < 0.01 for Survey 2; r = −0.07, p < 0.01 for Survey 3; r = −0.18, p < 0.001 for Survey 4). Regarding the affective dimensions of risk perception, only worrying about COVID-19 (RPA1) is significantly higher with increasing age in all surveys (r = 0.18, p < 0.001 for Survey 1; r = 0.14, p < 0.001 for Survey 2; r = 0.11, p < 0.001 for Survey 3; r = 0.11, p < 0.001 for Survey 4). However, being afraid about COVID-19 (RPA2) is positively correlated with age in Survey 2 (r = 0.09, p < 0.01), but decreasing with growing age in Survey 3 (r = −0.08, p < 0.01) and Survey 4 (r = −0.10, p < 0.001).
RQ2: Cognitive and affective risk perceptions of COVID-19 and its correlation with specific places
Our next research question examines how cognitive and affective risk perceptions of COVID-19 are correlated with specific places. In general, the data collected in March 2020 (Survey 1) demonstrate that 94.5% of respondents (strongly) agree they feel safe in their homes, while 54.3% (strongly) agree they feel safe outside their homes in outdoor places and 38.4% feel safe outside their homes in the private homes of others. However, only 8.2% and 7.3% (strongly) agree they feel safe outside their homes in shops, restaurants, public places, or public transit, respectively.
With respect to the association between cognitive and affective risk perceptions and location-specific subjective feelings of safety, the data show medium to strong negative correlations (see Table 4). While the negative correlations are rather low in the respondent's own home (from r = −0.08, p < 0.01 to r = −0.17, p < 0.001), they become higher—depending on the location context the respective items refer to—and are highest outside the respondent's home in public places or public transit (from r = −0.29, p < 0.001 to r = −0.50, p < 0.001). Throughout all locations, the correlations of affective risk perceptions (RPA1 and RPA2, from r = −0.08, p < 0.01 to r = −0.50, p < 0.001) are higher than those for the cognitive risk perceptions (RPC1, RPC2, and RPC3, from r = −0.08, p < 0.01 to r = −0.30, p < 0.001).
RQ3: COVID-19 risk perception characteristics
Besides looking at the affective and cognitive risk perceptions during the COVID-19 pandemic, our third research question examined the COVID-19 risk perception characteristics. Concerning the perceived characterization of COVID-19 as a “dread risk,” it can be seen that the item “COVID-19 (Coronavirus SARS-CoV-2) is a global disaster.” expressing a global catastrophe is rated highest by far (M = 4.46, SD = 0.88) followed by COVID-19 to be of catastrophic potential (M = 3.84, SD = 1.03) and the item including the dangers of infection as easily reducible (M = 3.77, SD = 0.97) (see Table 2; Survey 1, March 2020). Respondents rated items lowest concerning the personal impact of COVID-19 (M = 3.18, SD = 1.27), “the risks posed by COVID-19 [...] not [to be] equally distributed across society” (M = 3.17, SD = 1.27), and the item saying the respondent took the risk of an infection voluntarily (M = 2.20, SD = 1.09).
Analyzing COVID-19 as “unknown risk” it can be stated, that the item “COVID-19 (Coronavirus SARS-CoV-2) is something completely new for all of us” expressing COVID-19 to be a new risk is agreed most by far (M = 4.26, SD = 1.08) followed by the subdimensions of immediacy (“The consequences of COVID-19 (Coronavirus SARS-CoV-2) are immediately noticeable”; M = 3.77, SD = 1.10) and observability (“The effects of COVID-19 (Coronavirus SARS-CoV-2) can be observed well”; M = 3.70, SD = 1.04) (see Table 3). The items stating delayed consequences of COVID-19 (M = 3.56, SD = 1.03), expert knowledge about COVID-19 (M = 3.15, SD = 1.01), and the risk known to those exposed (M = 2.14, SD = 1.13) are agreed to the least.
RQ4: COVID-19-related coping mechanism
Our last research question focuses on the COVID-19-related coping mechanism. In Survey 1 (March 2020), respondents coped more with problem-than emotion-focused strategies considering the respective overall scales (M = 3.11, SD = 0.57 vs. M = 2.61, SD = 0.63).
Having a more detailed look at problem-focused ways of coping, respondents stated to “listen to the experts and follow their advice” most (M = 4.14, SD = 0.99) followed by “think[ing] carefully about what to do and stick to it” (M = 4.05, SD = 0.95) and “[not] try[ing] [...] to do anything rash” (M = 4.05, SD = 1.00) (see Table 5). However, respondents rated statements concerning “doing something completely new” (M = 2.41, SD = 1.17), “ask[ing] for advice from highly respected people” (M = 2.19, SD = 1.17), and “see[ing] something like this before” (M = 1.40, SD = 0.83) lowest.
Compared to problem-focused strategies, the level of emotion-focused coping is lower as shown above. For instance, the item “It will emerge over time; there is nothing more to do but wait.” is the highest rated (M = 3.71, SD = 1.07), followed by “turn[ing] to my work or other activities to distract myself” (M = 3.35, SD = 1.16) and “imag[ing] how the whole thing could end” (M = 3.20, SD = 1.21) (see Table 6). The respondents, however, agreed less to items including “tak[ing] refuge in daydreams” (M = 2.02, SD = 1.18) and cope less by “try[ing] to leave the whole thing behind and want to rest or go on vacation” (M = 1.97, SD = 1.11) or “refus[ing] to believe what is happening” (M = 1.69, SD = 1.00).
Discussion
The current article evaluates the relevance of a “psychosocial situation report” for more effective crisis management in Germany by examining how people in Germany perceived the risk of being infected by COVID-19 on an affective and cognitive level during the pandemic (RQ1), how cognitive and affective risk perceptions of COVID-19 correlated with specific places (RQ2), what characterized the perception of COVID-19 (RQ3) and how people coped with COVID-19 (RQ4). In many regards, our results (partly) replicate previous findings on how people perceive COVID-19 risks (e.g., Renner et al. 2020; Betsch et al. 2020b; Collective Service 2022) and cope with crisis situations (e.g., Budimir, Probst, and Pieh 2021; Cohrdes et al. 2023). However, our study also led to new insights regarding risk perception and coping. In the following, we discuss the results belonging to the research questions and how they contribute to the application of the psychometric paradigm to risk perception and the transactional model of stress and coping on the crisis context. Subsequently, we suggest a theoretical integration of these two models that may guide the monitoring of important psychosocial determinants in crisis management. By that, we show that both, the psychometric paradigm to risk perception and the transactional model of stress and coping are useful for structuring the monitoring of psychosocial factors in crisis management. When monitoring the psychosocial situation in crises, the following factors need to be faced and mapped in data: Cognitive and affective risk perception (RQ1 and RQ2), risk perception characteristics (RQ3), and coping strategies (RQ4). While our study focuses on the COVID-19 pandemic we assume that this framework could also serve for other crisis situations.
RQ1: Cognitive and affective risk perception during the COVID-19 pandemic in Germany
With respect to the first research question, our results revealed that the cognitive and affective risk perceptions were highest at the beginning of the pandemic. Over the course of the pandemic, the most striking result is the almost continuous flattening of respondents’ risk perceptions. A possible explanation for this might be a habituation effect, as unfamiliar risks are rated often as more threatening (Costa et al. 2022). Given the background of a declining risk perception along the course of the pandemic and the fact that protective behavior is (often) linked to it (Cipolletta, Andreghetti, and Mioni 2022), this habituation effect can turn into a problem for crisis management, since protective measures might not be followed in the long run, despite stakeholders such as crisis managers depending on the population's adherence to the established measures. Hence, the sensitization of risk perception and thus a clear risk communication to the population during long-lasting crises should be a central aspect to motivate the population to maintain their protective behavior. At the same time, this process must also consider different (vulnerable) groups so as not to cause an additional psychological burden (see also RQ4).
However, our findings regarding the declining tendency of risk perception are only partially confirmed by the results of the EUCLID as well as COSMO monitoring projects (Renner et al. 2020; Betsch et al. 2020b). Thus, further research is needed to understand potential habituation effects that may mitigate risk perception. Apart from the possibility of a habituation effect, it cannot be ruled out that the respondents felt increasingly informed about the course of the pandemic and therefore also felt safer, which in turn could explain the reduction in risk perception (e.g., widespread media coverage and successful processes of crisis communication by public authorities; see also Bundesinstitut für Risikobewertung 2020; Betsch et al. 2020b). Although lower compared to Survey 1, there is a slight increase in risk perceptions between Surveys 3 and 4. This can be explained by the Omicron wave starting in November 2021 and rising numbers during the sample period. This is in line with other research (Collective Service 2022) and shows changing perceptions due to the context, yet on a lower level compared to the beginning of a new, unknown COVID-19 crisis.
The present study was also designed to determine the effect of sociodemographic characteristics on cognitive and affective risk perception. Consistent with other monitoring projects (e.g., Betsch et al. 2020b), this research found that older participants tend to perceive lower risk of becoming infected by COVID-19 and the likelihood of becoming infected to be higher for other people than for themselves, indicating an optimistic bias. This is consistent to existing research like Glöckner et al. (2020), who found that the participants on average believe they can protect themselves better than others are able to. An explanation for these results might be that people tend to be inappropriately optimistic and think that the illness is less likely to affect them when compared to others (van Bavel et al. 2020). However, older people belong to a risk group with a higher likelihood of severe infection (Karagiannidis et al. 2020) and should thus protect themselves more often. Furthermore, we find an increased risk perception among women—in line with Cipolletta, Andreghetti, and Mioni (2022). Both results suggest that risk perception can vary due to several (risk) factors, such as sociodemographic characteristics. Hence, from a crisis management perspective, it seems essential to address the risk groups (e.g., the elderly) effectively (Leung 2020; Zhang et al. 2021), in particular, those facing a discrepancy between factual and perceived risk using appropriate risk and crisis communication strategies tailored for specific groups at risk. At the same time, trust in certain institutions (e.g., medical experts and authorities) should be increased which relates to protective measures like vaccinations in a later pandemic stage (Sterl et al. 2023).
RQ2: The correlates of risk perceptions of COVID-19 with specific places
As mentioned in the literature review, a previous mobile experience sampling study documented varying levels of risk perception of COVID-19 in different places (Restel et al. 2022). Our results showed that the surveyed respondents feel uncomfortable outside their homes, in shops or restaurants as well as in public places or public transit. Further, correlations between places and risk perceptions show that objectively riskier places (such as public transit or shops and restaurants) are also perceived as riskier, which is a hint that people understand that social distancing is relevant to reducing the spreading of COVID-19 in the early stage of the pandemic. One possible explanation for this is that these places were often thought to be at higher risk of infection at the beginning of the pandemic, even though studies published later also indicate that COVID-19-infected individuals contracted in their own houses as well (Kühne, Kreil, and Kohler 2021). Moreover, the reported correlations are more marked for the affective risk items, which is in line with findings from other studies suggesting that places and social identification are interconnected and that emotional bonds exist between people and the places they find meaningful (Scanell and Gifford 2010; Reese et al. 2020). Nevertheless, the numerous restrictions regarding public places and shopping centers, for instance, and due to social distancing impede an adequate interpretation of the correlations. Consequently, further research is needed to examine the relationship between perceived risk and places as it is important to know for which locations risk communication must be enforced in case risk perceptions are underestimated subjectively.
RQ3: COVID-19 risk perception characteristics
Following the psychometric paradigm (Slovic, Fischhoff, and Lichtenstein 1982; Slovic 1987), respondents should assess selected characteristics that they attribute to COVID-19 as a risk. Concerning the “dread risk” dimension, people rated COVID-19 as a “global catastrophe” with catastrophic potential that “will cause many deaths at once.” However, they stated the dangers of infection as easily reducible on a personal level. The personal level addressed in some items might be the reason why, in contrast to the “dread risk” dimension in the psychometric paradigm (Slovic 1987), attributes like dread, globally catastrophic, and increasing risk are correlated with reducibility, which deviates from Slovic's findings. This leads to the assumption that for COVID-19, the assessment of the disease as a global disaster with dreadful and high impacts—even on future generations—does not exclude the ability to perceive a capacity for coping with it on a personal level by reducing the dangers of an infection. As thinking of a crisis as a global catastrophe with highly deadly potential is assumed to be related to higher levels of negative psychosocial consequences, it is important to focus on individual resources such as self-efficacy and the possibility of easily reducing dangers on an individual level to prevent negative psychosocial outcomes and increase the ability to control the own situation using protective measures which mitigate negative physical and psychosocial effects.
Taking a closer look at the “unknown risk” dimension, rating COVID-19 as a new risk most highly is an expected result, as the population is not used to the experience of worldwide pandemics with a new pathogen like experts are. This also agrees with the previous finding about people's perception of the novelty of COVID-19 (Bostrom et al. 2020), especially when viewed from the theoretical standpoint of the psychometric paradigm, whereby people perceive COVID-19 as a new risk and unknown to those exposed but which at the same time is immediate and observable. This might be because the pandemic has both dominated news and media discourses for weeks and because it has been well documented for and effectively disseminated to the general public, such as by means of dashboards from John Hopkins University (2023).
In conclusion, the data about risk characteristics of COVID-19 paint a complex picture: Germans characterize COVID-19 as a “dreadful catastrophe,” but at the same time as easy to reduce on a personal level. Additionally, respondents say that the disease is new, but observable at the same time. Regarding these perceived characteristics it seems to be adequate for crisis management to address people's roles and responsibilities and strengthen the perception of COVID-19 as controllable by personal behavior as mentioned further above. Moreover, as the characteristics of COVID-19 as a risk presented here can be assumed to relate to the quantitative dimensions of risk perceptions in RQ1, further research is needed to ascertain their associations as quantitative risk perceptions which, in turn, leads to adequate protective measures.
RQ4: COVID-19-related coping strategies
Several studies on COVID-19 risks address problem-focused coping (e.g., Luszczynska, Knoll, and Scholz 2020; Rieger 2020; Perrotta et al. 2021) and emotion-focused coping (e.g., Budimir, Probst, and Pieh 2021; Minahan et al. 2021), separately. The underlying results extend these insights by comparing problem- with emotion-focused coping strategies in Germany. On average, more problem-focused coping strategies were used than emotion-focused strategies. Specifically, most respondents tried to cope with the threat of the pandemic by following the advice of experts, while only a few tried to reduce fear by denying or wishing to escape the situation (also see Betsch et al. 2020a, 2020b). The strong reliance on external expertise seems adequate for a risk that is subjectively characterized as unknown and connects to the finding that most respondents perceived the risk as easily reducible on a personal level (see RQ3).
The dominance of problem-focused coping relying on expert knowledge could also be a sign that crisis communication and management had been successful in reaching most Germans. However, no direct connection can be presumed between the findings on coping behavior and the influence of crisis management. Thus, it cannot be determined from our data whether, for instance, policies to reduce the spread of COVID-19 are directly connected with problem-oriented coping strategies in the population. Thus, future research is needed to examine the role of specific coping strategies related to, for example, the adherence to measurements and the development of coping during future manifestations of the pandemic.
The monitoring of the psychosocial situation during crises
Regarding the question of how these findings contribute to a situation report for crisis management and public authorities, we conclude that they allow for a better and more detailed understanding of who is affected by COVID-19 and in which way. The current study shows that the psychometric paradigm (Slovic, Fischhoff, and Lichtenstein 1982; Slovic 1987; Peters and Slovic 2000) and the transactional model of stress and coping (Lazarus and Folkman 1984) are useful to structure a comprehensive situation report of psychosocial factors in crisis management. Thereby, a psychosocial situation report can enable crisis management authorities to make sense of perceptions as well as available and needed resources to cope with a crisis like the COVID-19 pandemic and base further decisions on that information (Dückers et al. 2017).
As described in the introduction, the primary appraisal of a threat corresponds with the concept of risk perception. In the first step, the adequate risk perception scrutinized in RQ1, RQ2, and RQ3 is crucial for the adoption and acceptance of protective measures on the individual and collective level. Perceived characteristics of a crisis as, for example, unknown, dreadful, or reducible, may determine the coping response. Moreover, the availability and appraisal of coping resources determines whether problem- or emotion-focused coping strategies are adopted (see RQ4). If a risk is perceived as high but resources to control the problem are low, emotion-focused coping is often the only option and mental distress can arise.
Therefore, the data on risk perception as well as coping behavior in different groups is an invaluable decision basis for targeting resources or balancing out the communication of potential harms and threats and coping possibilities to vulnerable groups. For instance, this study found a discrepancy between the risk perception reported by older people and their actual risk (see RQ1), implying the need to emphasize the risks more. For other groups, the risk perception may lead to a higher level of distress or health anxiety (e.g., Han et al. 2021; Lindner et al. 2022) indicating interventions that focus on strengthening coping resources instead. Generally, the data shows that measuring the primary appraisal and coping strategies appears to be appropriate for the COVID-19 pandemic. An analysis of the role of resources like self-efficacy, social support, trust in authorities, and other psychological factors are not included in the current study but should be considered in future crisis monitorings (as measured in ongoing projects like “Managing psychosocial situations in crises and disasters” (PsychoKat 2024)).
Beyond generating the data on psychosocial situations, it is important to provide the data to crisis managers in a convincing and easy-to-use way. COVID-19 crisis managers in Germany mostly rely on anecdotal information on the psychosocial situation from their close social environment or social media instead of statistical and systematic information (Lüttschwager et al. 2022). Consequently, future research should be incorporated into technical solutions tailored for political decision-makers and authorities to help visualize a psychosocial situation report to get a quick overview of the situation happening. For instance, Sterl et al. (2024) are developing a “Multi-Functional Crisis Information Platform for Psychosocial Situations (CIP-PS)” for Germany which helps visualize, research, and document psychosocial information in a systematic way using a dashboard, research, and documentation component.
Limitations
We do not wish to conceal that the present study has its limitations on a contextual as well as methodological level. While we collected data for this study, changes and new information (i.e., disseminated by media) were emerging daily. However, our study mainly addresses individuals’ affective and cognitive risk perception of the pandemic and their coping strategies. Hence, this study does not take into account different factors (e.g., media consumption, belonging to a risk group, and socioeconomic status) that might have an influence on individuals’ perception. For this reason, upcoming studies should consider other factors that may influence risk perception and coping strategies.
Furthermore, the generalizability of our study is subject to certain limitations. Even though our research comprises four representative surveys in the German population, our data used only online participants of different sex, age groups (from 18 to 74 years), and German states. Thus, our data did not gather specific groups or those without online access (e.g., persons older than 74 years). To minimize this limitation, future studies should also conduct telephone (CATI) or personal interviews (CAPI). A further issue that was neglected in this study was the panel causality between the cross-sectional survey. Consequently, interpretations of the data are linked to the time and location of data collection. Installing panel surveys could therefore be a fruitful addition to the existing work.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bundesministerium für Bildung und Forschung (grant number 13N16269).