
Abstract
Drawing on the work of Layton and Duffy, and Williams, Davey and Johnstone, this paper examines the infant formula marketing system. Using a Systems of Provisioning approach, marketing system failure as a result of regulatory intervention at the intersection of two systems is conceptualized - the infant health system and the infant formula marketing system. Positive population-based outcomes for breast feeding rates and negative stigmatizing outcomes at an individual consumer level occur as the two provisioning systems respond to regulatory interventions. The mechanisms are identified whereby intervention restricts participant choice and coevolution of the marketing system contributing to the failure. Taking a Systems of Provisioning approach, we advance the understanding of marketing system failure, and we recommend co-design processes involving multiple stakeholders as a way forward to remedy such occurrences.
Introduction
Society is faced with a multitude of wicked problems which arise through adaptive change in marketing systems (Kadirov 2011; Layton 2015; Layton and Duffy 2018). The United Nations Sustainable Development Goals (UNSDG) refine the global wicked problems of our time to 17 key areas for improvement, explicitly acknowledging the complex interconnectedness of wicked problems and the need for systems changes. Furthermore, the UN Global Compact calls on businesses universally to mobilize efforts toward sustainable development goals with two key goals being to reduce inequality in access to services and to ensure health and well-being (unglobalcompact.org). Importantly, a marketing systems perspective is a promising way to meet these human needs and safeguard sustainable development. Macromarketing holds that marketing systems, defined as “complex social networks of individuals and groups linked through shared participation in the creation and delivery of economic value through exchange” (Layton 2015, p. 303), exist to ensure well-being for all (Fisk 1981; Layton 2007; Shultz 2007). While consumer value and benefit are the intended consequences of action in a marketing system, situations that result in any negative consequences for public good are marketing system failures (Duffy, Layton, and Dwyer 2017) since the system has not managed or remediated such outcomes. Williams, Davey, and Johnstone (2021) specifically define marketing system failure as “a response that occurs when patterns of interactions and system structures result in any of the system elements becoming worse off - either individually or collectively/societally” (p. 411).
Our focus is on UNSDG #3, to “Ensure healthy lives and promote well-being for all at all ages” (https://www.unglobalcompact.org/ and https://sdgs.un.org/goals), that places nutrition at the forefront of world development and a sustainable planet (Binns et al. 2017, https://sustainabledevelopment.un.org/post2015/transformingourworld/publication) and more specifically, infant nutrition. Within this context there are two provisioning systems operating with a goal to ensure infant nutrition – the infant health system and the infant formula marketing system. These two interrelated systems share the common goal of provisioning. However, they diverge on other objectives and characteristics. The infant health system strives to improve health and health equity (World Health Organization 2000) while the infant formula marketing system strives for consumer satisfaction and profit maximization (Layton and Domegan 2021). Marketing systems provide open choice and wide assortments. However, the health system is seen as a prescriptive supply chain with narrow product/service assortments and thus restricted choice (Kennedy 2017; Layton and Domegan 2021) since it is “top-down, hierarchical, controlling, and prescriptive in what is made available…” (Layton and Domegan 2021, p. 7).
In the current paper we use Layton's Marketing Systems lens (Layton 2007, 2015; Layton and Duffy 2018) and that of systems of provisioning (SoP) (Fine, Bayliss and Robertson 2018; Layton and Domegan 2021) to examine the intersection of the infant health system and the infant formula marketing system where “…the combination of the material processes of provision and the material cultures associated with the commodity…uniquely engage with one another in specific instances” (Fine, Bayliss and Robertson 2018, p. 30). At the intersection of such systems unintended consequences occur (Williams, Davey, and Johnstone 2021). Although Williams, Davey, and Johnstone (2021) examine system failure and the points at which stakeholder or policy intervention can avoid or mitigate the impacts of system failure, intervention by stakeholders and policy/regulation as contributors to system failure have received little attention. In the infant feeding case, the health and marketing systems intersect and at this intersection regulation shifts power to the health system which assumes responsibility for infant nutrition in general. Previous literature has not yet considered the interactive effects of two provisioning systems with different goals nor the impact of the places of intervention as proposed by Williams, Davey, and Johnstone (2021). This research explores the interactive nature of two complex provisioning systems – the infant health system (encompassed within the larger health system) and the infant formula marketing system. We address this purpose via two research questions:
RQ1: How does the interaction and interdependence of these two systems impact consumers and society? RQ2: How can the points of failure at the intersection of these two provisioning systems, one of which is a marketing system, be mitigated?
The contributions of this article are threefold: 1) We contribute to the work of Roger Layton, Christine Domegan, and Sarah Duffy in the area of marketing systems theory by exploring intersecting provisioning systems (health and marketing) for the first time; 2) we provide an extension to the marketing system failure theory by identifying points of failure and methods for mitigation; and 3) we provide insight for macromarketers and public health regulators to avoid stigmatizing and disadvantaging stakeholders (e.g., new parents). These contributions are delivered through a conceptual review of literature, interspersed with reflections on both the role of the marketing system, health system and regulatory bodies in system failure.
The Infant Feeding Context
The infant feeding context is characterized by the considerable and intense debate regarding breastfeeding and infant formula feeding.
Human breast milk is considered the optimal source of infant nutrition conferring metabolic, emotional, and immunologic advantages (Lessen and Kavanagh 2015; Rollins et al. 2016; Victora et al. 2016). Based on evidence and beliefs about benefits endowed to mother 1 and baby (Kramer and Kakuma, 2012), widespread interventions and practices promote and support breastfeeding practices to ensure breastfeeding rates are improved (or maintained). Breastfeeding is also promoted as convenient, financially less costly than the purchase of formula (Hastings et al. 2020) with lower environmental impact (Smith 2019). Breastfeeding is supported by public health campaigns, lactation-friendly work environments, and education of health professionals that directs practice toward breastfeeding (Porta et al., 2016). Increasingly, social marketing explores how women can be persuaded and supported to adopt and maintain breastfeeding (e.g., Gallegos et al. 2014; Wolf 2007).
Notwithstanding the evidence of breastfeeding benefits and the resurgence of breastfeeding in the 1970s, the World Health Organisation (WHO) established the International Code of Marketing of Breast-milk Substitutes in 1981 in order to protect consumers and avoid the harms claimed to be associated with unethical and aggressive milk formula marketing. The global Code aims to contribute to the provision of safe and adequate nutrition for infants by the protection and promotion of breastfeeding and by ensuring the proper use of breast milk substitutes. In particular, the Code addresses advertising to the public, retail promotions, marketing in health care systems, and labelling of breast-milk substitutes. By restricting the advertising and promotion of breast-milk substitutes it sought to correct the marketing system failure (Williams, Davey and Johnstone, 2021). This International code is designed to be effective irrespective of country level differences, such as cultural values or religious values, that might affect breast feeding rates (Gallegos et al. 2020). While each country has their own legislation related to breast-milk substitutes, regulation of the infant formula marketing systems across most of the world is based on this international code. Despite four decades of the International Code, there are ongoing claims that the commercial milk formula business manipulates parents, misuses science (Clark and Ghebreyesus 2022; Doherty et al. 2023; Mahase 2022; WHO, 2022), and engages in exploitative marketing practices underpinned by “sales and shareholder interests before infant and population health” (WHO, 2022, p. x). Even with such regulations internationally, scholars and health professionals point to inadequate progress at a macro level in improving breastfeeding practices with only 48% of the world's infants and young children exclusively breastfed up to six months of age as recommended (Baker et al. 2023; Pérez-Escamilla et al. 2023; Rollins et al. 2023).
In New Zealand (the current context) breastfeeding is promoted as optimal feeding for babies. New Zealand (NZ) adheres to standards and practice recommendations that foster the establishment for exclusive breastfeeding till at least six months of age and then breastfeeding with complementary feeding to a year. The Baby Friendly Hospital Initiative (BFHI) was launched in NZ in 1999 and in 2023 98% of hospitals are BFHI accredited (New Zealand Breast Feeding Alliance 2022). To foster the establishment of breastfeeding in NZ, skin to skin contact with mother and baby is the norm, immediately, or at least within one hour of birth. Support for the establishment and continuance of breastfeeding is a key aim during contact with a mother. The infant formula marketing system in NZ is regulated based on the international code adopted in 1983. The International Code is implemented in NZ under four NZ codes: Code of Practice for Health Workers (Health Workers’ Code), New Zealand Infant Formula Marketers’ Association Code of Practice for the Marketing of Infant Formula (the NZIFMA Code of Practice) (NZIFMA 2007), Advertising Standards Authority Code for Advertising of Food (ASA 2006), Australia New Zealand Food Standards Code (Food Standards Code) (FSANZ 2002). (https://www.health.govt.nz/system/files/documents/publications/breast-milk-substitutes-marketing-code.pdf)
Dominant Discourse, Barriers and Stigma
Despite WHO/UNICEF (2022) acknowledging that infant formula has a place for those women and parents who are not able, or do not want, to breastfeed, the “breast is best” message is upheld through pre-natal education of parents, tight regulation of marketing of infant formula, and hospital and birthing centre pro-breastfeeding policies. This discourse in the marketing system drives the co-evolution of differential endowments such as the belief a ‘good mother breast feeds’, changing norms and distorting perceptions (Layton 2015; Redmond 2018; Runciman 2009) leading to stigmatization around infant formula feeding. The regulation of infant formula marketing that has occurred since the early 1980's effectively shifted responsibility for dissemination of infant formula information to the health professionals and inadvertently created stigma around formula feeding of infants due to changed norms and beliefs. 2 According to Crocker and Major (1989), stigma is where a person is identified as part of a group toward whom others hold negative attitudes. This includes negative stereotypes and beliefs about the behavior, values, and thinking of group members (in this case, non-breastfeeding parents). The outcome of stigma is institutional inequities, prejudice, discrimination, and overall devaluation by society; group members being ostracized; and access to social, health, and marketing systems restricted (Link and Phelan 2001; Major and O’Brien 2005). Stigma devalues and discredits a part of a person's identity (Crocker, Major, and Steele 1998; Goffman 1963) and perceived competence (Fiske 1998), which may explain why non-breastfeeding mothers are perceived as “bad mothers”, and experience feelings of shame and also blame for not breastfeeding (Corrigan 1998; Van Brakel 2006). In this paper we argue these consequences negatively impact mental health (stress, anxiety, depression) outcomes for some mothers (Van Brakel 2006) and hence constitute marketing system failure (Duffy, Layton, and Dwyer 2017).
The additional regulatory requirements, stigma of formula feeding, and lack of product information for consumers, reduce consumers’ ability to make good consumption decisions (Fallon et al. 2017; Malek et al. 2019; Moss-Racusin et al. 2020) further indicating marketing system failure for parents who may wish to use infant formula. There is a good deal of discussion that formula feeding mothers experience barriers to accessing information and support in establishing formula feeding because of the discourse and actions of health professionals (e.g., Lagan et al. 2014; Lakshman, Ogilvie, and Ong 2009; Wirihana and Barnard 2012). Such behaviors show Social Mechanisms at play, which again reinforce breastfeeding behavior through co-operation between health system members and signalling to mothers (Layton 2015). Although breastfeeding is presumed to be an innate ability, some women make a choice to formula feed for many reasons (for example, returning to work, disruptions that impede early establishment of breastfeeding, or mental wellbeing) and, although relatively scant, some academic literature challenges the widespread notions of breast feeding as the only choice to maximize maternal and infant welfare (Moss-Racusin et al. 2020; Wolf 2007).
The prevailing focus on breastfeeding as the norm and superior mode of infant feeding, sanctions, stigmatizes and potentially isolates women who do not conform (Dattilo et al. 2020; Fallon et al. 2017; Wolf 2007; Moss-Racusin et al. 2020). Outcomes experienced from non-compliance with breastfeeding norms can threaten feelings of self-worth and attainment of the idealized motherhood role (Bresnahan et al. 2020), potentially leading to experienced vulnerability at an important transition point in a woman's life (Commuri and Ekici 2008). Mothers who need to use infant formula cannot access information, may be treated with disrespect, and made to feel they are failing their babies within the infant feeding social system (Appleton et al. 2018; Dattilo et al. 2020; Williams, Donaghue, and Kurz 2013). In their systematic literature review Dattilo et al. (2020, p. 4) conclude that “the majority of studies with mothers that could not, or elected not to BF [breast feed], particularly for the duration they intended, reported ‘feelings of shame, guilt, or stigma’” and Fallon et al. (2017) found two thirds of formula feeding mothers surveyed in their study felt guilty about their choice of feeding method, impacting mothers’ self- perception as good mothers and importantly, emphasizing the strength and prevalence of the rhetoric around the ideal infant feeding regime.
Although developed to protect consumers and avoid the harms associated with unethical infant formula marketing, regulation (the International Code and country specific implementation of the Code) creates barriers for those consumers who want or need to formula feed in the infant formula marketing system. The breast is best discourse takes on a moral imperative “inseparable from the concept of good mothering” (Marshall, Godfrey, and Renfrew 2007, p. 2147). Thus, in combination, there is a shortfall in meeting human needs, namely marketing system failure.
Method
This conceptual study follows the theory-in-formation method (Laczniak and Shultz 2021) to provide a revised perspective on the concept of marketing systems (MacInnis 2011). Thus, we use theory adaptation (Jaakkola 2020) to expand the application of Layton's Marketing Systems foundational work by using Systems of Provisioning (SoP) theory (Fine, Bayliss and Robertson 2018) to the extant conceptualization of marketing system failure, namely when failure is caused at the intersection of two provisioning systems. The alternative frame of reference guiding this theory adaptation is the marketing system failure from regulatory intervention within two complex, intersecting provisioning systems. We propose that SoP theory (Fine, Bayliss and Robertson 2018) and marketing system failure (Williams, Davey, and Johnstone 2021) extend the understanding of marketing systems, but at the same time confirming the value of marketing systems for addressing the wicked problems leading to system failure.
Conceptual Foundations
Fine, Bayliss and Robertson (Fine, Bayliss and Robertson 2018 ) propose that the level and meaning of consumption can be understood through the lens of Systems of Provision. They propose a reflexive role for consumers in terms of their consumption and draw on four categories for theorizing such systems which will be discussed using Layton and Duffy (Layton and Duffy 2018) framework. These overlapping categories, that is Structures in access or provisioning; Processes through which provisioning occurs and these may be influenced by structures involved. Agents, that is the participants in the provisioning system, including tensions and conformity; and Relations between these three factors, dependent on roles, power, conflicts and resolution (Fine, Bayliss and Robertson 2018, p.34–35).
Intersections of Marketing Systems
Systems have a core place within Macromarketing (Layton and Grossbart 2006), with most of the more recent development coming from Roger Layton and his colleagues. Systems are groups of interdependent and interrelated entities existing in relatively stable hierarchies (Anderson and Johnson 1997; Kramer and Smit 1977). Both the entities that make up a system and the system itself have their own goals. They often work together to achieve any shared goals, so feedback loops can be used for self or imposed regulation and sanctions. Problems may arise with conflicting goals, decision making issues, and with unclear feedback or interaction processes (Anderson and Johnson 1997; Kauffman 1980). The interdependence of the entities and embeddedness of the systems within one another leads to ripple effects from even small changes or conflicts (Kennedy 2017). A marketing system is formed through “the creation and delivery to customers of assortments of goods, services, experiences and ideas, enhancing the perceived quality of life of the communities in which the marketing systems operate as well as providing economic benefits for each of the systems” (Layton 2015, p. 305).
Recent systems literature is concerned with the evolution and growth of marketing systems. Moving beyond linear understandings of change and process, to non-linear, causal dynamics, and path dependencies (e.g., Brychkov and Domegan 2017; Domegan et al. 2016, 2017; Layton 2015, 2019; Layton and Domegan 2021; Layton and Duffy 2018) these scholars delve into the complexity of change, humans, interactions, organizational decision making, and that which influences them. Layton (2015) introduces MAS theory in explaining systems change, while Layton and Duffy (Layton and Duffy 2018) extend this to focus on the social mechanisms of 1) market delivery systems; 2) stakeholder action fields; 3) technology evolution systems; and 4) value exchange fields. Layton and Domegan (2021) explore marketing and other systems as provisioning systems and move beyond marketing as the only provisioning system for society. Here, marketing systems are seen to provide open choice, wide assortments of provisions with high levels of diversity in their delivery. In contrast, another provisioning system, the health system (Kennedy 2017; Layton and Domegan 2021), is seen as a prescriptive supply chain with narrow product/service assortments and thus restricted choice and diversity. This stems from the health system being “top-down, hierarchical, controlling, and prescriptive in what is made available…” (Layton and Domegan 2021, p. 7)
So, while marketing systems are part of the broader economic system, they are interrelated with various other social systems (Dixon 1967), such as the health system. For a society to function, it must solve a series of functional problems through internal system interactions, as well as between system interactions (Dixon 1984, p. 4). Marketing's primary goals tend to be for customer satisfaction for profit maximization (through delivery of an assortment of goods and services – Layton 2019), while health system goals are “…improving health and health equity, in ways that are responsive, financially fair, and make the best, or most efficient, use of available resources…[through] greater access to and coverage for effective health interventions…” (World Health Organization 2000, 2007). The shared outcome goals of the two systems are 1) provisioning; along with 2) fairness, justice, and sustainability; and 3) quality of life and wellbeing (Layton 2009; Layton and Domegan 2021). These outcome goals also create and perpetuate values, norms, practices and institutions. Any change in a marketing system, whether internally or externally imposed will have an impact on wellbeing and quality of life (Layton 2019).
Williams, Davey, and Johnstone (2021) extend Layton and Duffy (2018) work on path dependency to explore system changes which bring about negative effects (such as on wellbeing or quality of life) on the system leading to marketing system failure. They explore such failure and the points at which stakeholder or policy intervention is used to avoid or mitigate its impacts. These points are a) before failure, where problems can be predicted and mitigated, and b) after failure, in response to negative outcomes. They do not explore points of external intervention, by stakeholders or policy which, in turn, cause system failure. These real impacts on system performance can be uncovered by comparing “adjacent, embedded and complementary systems” (Layton and Domegan 2021, p. 12) particularly when intervention is designed to bring two systems together. While both the health system and marketing system seek to provision products and services, their structures and value delivery goals differ substantially beyond that creating conflict, tension, and dynamic relationships. Previous literature has not yet considered the interactive effects of two provisioning systems with such different goals, nor the impact of the points of intervention proposed by Williams and colleagues (2021). As Layton and Domegan (2021) posit, such provisioning systems are on the edge of chaos as they try to interact with one another, the state and within themselves. Externalities, internalities, intended and unintended consequences across multiple systems are possible.
Marketing System Failure at the Intersection of Two Complex Provisioning Systems
The following sections discuss marketing system failure in the infant formula marketing system that has occurred in response to regulatory intervention. The two adjacent systems – the infant health system and the infant formula marketing system - collectively function on the constant process of feedback, interaction and emergence to enable evolution and system adaptation. In this case regulation is designed to correct marketing system failure (Williams, Davey and Johnstone, 2021). However, failure for the individual (e.g., Fallon et al. 2017) may be overlooked despite there being societal benefits (e.g., Layton and Duffy 2018; Williams, Davey and Johnstone, 2021) unless the complex system and embedded nature of the marketing systems are considered. We discuss this failure using the core concepts in any complex system: marketing system failure, system history and regulation, co-evolution of choice, and network level social mechanisms, and relate them to the system of provision of infant nutrition in which a marketing and health system respond to regulation (Fine, Bayliss and Robertson 2018; Layton and Duffy 2018).
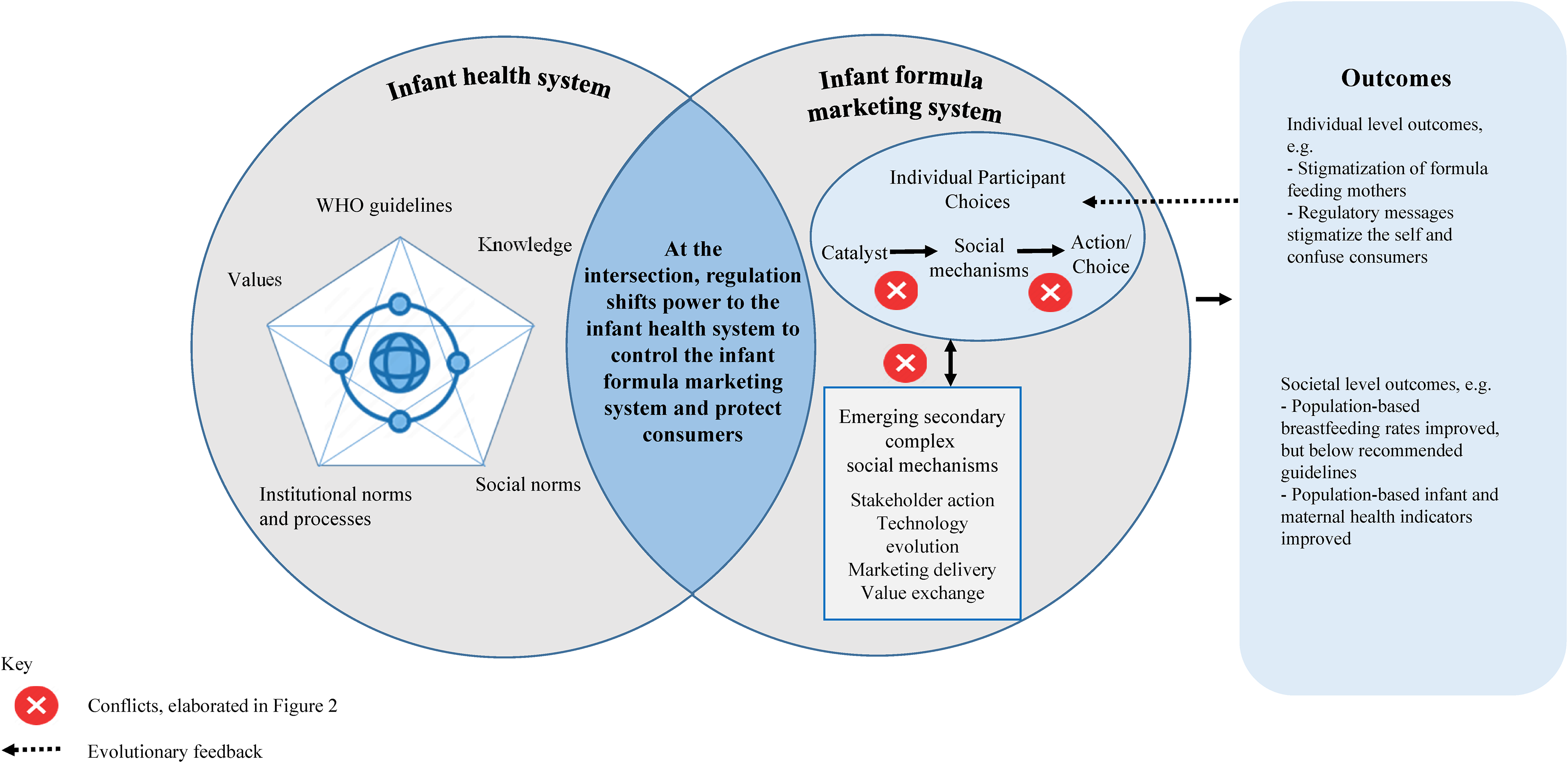
First, we provide the context for the application of two complex provisioning systems and then propose how regulation at their intersection leads to Marketing System Failure. Figure 1 is an illustrative overview of the intersection of the two complex provisioning systems, identifying conflicts contributing to marketing system failure. Figure 2 details the conflicts (and where they occur), explaining the marketing system failures with two propositions.
Conflicts contributing to marketing system failure at the intersection of two complex provisioning systems.
Explaining the conflicts contributing to marketing system failure at the intersection of two complex provisioning systems.
Marketing System Failure – the Application
Appreciating that marketing strategies shape societal outcomes, the infant health system instigated regulation on the infant formula marketing system to curb the excesses of earlier marketing practices, initiating a particular type of marketing system failure. Associated with its prevailing dominant breastfeeding philosophy, the infant health system fashioned powerful norms and values causing tensions and constraints within the infant formula marketing system's co-evolution of choices. According to Mittelstaedt, Duke, and Mittelstaedt (2009) constrained consumption logic, “participants cannot interact with equitable agency” (Williams, Davey and Johnstone, 2021, p. 412) due to the powerful forces of the infant health system intersecting with the evolutionary paths and processes of the infant formula marketing system. Regulation occurs at the interface between the infant health system and the infant formula marketing system (Figure 1). Infant formula regulation is designed to facilitate desirable outcomes at a macro level (for example, improved breastfeeding rates, decreased infant mortality) but creates negative consequences at a micro level, reducing wellbeing for formula-feeding mothers since regulatory barriers on infant formula information and advice result in unmet needs and wants of customers.
Regulation and the Infant Health System
Due to claims of misbehavior by powerful stakeholders in the infant formula marketing system and the associated internalities of infant illness and death as well as externalities for the health of populations globally, the WHO and governments intervened. The intervention via regulation of the marketing of breastmilk substitutes seeks to reduce the power of the profit-driven stakeholders in the marketing system to protect and enhance breastfeeding rates. As proposed by Williams, Davey and Johnstone (2021), the marketing system failure resulted from the activities of powerful market actors and their profit driven motives. However, regulation at the system setting level shifts the power from the marketing system to the adjacent health system with the goal of greater ethical consideration in guiding value-based choice of potential infant formula marketing system participants at the individual consumer level and creating a larger complex system. Shifting of control to health providers in combination with negative historical associations restricts self-organization of the marketing system. New networks of individuals assume control restricting information exchange. This leads to positive outcomes for populations in line with the work of Williams and colleagues (2021). In the current case, these include outcomes of higher breastfeeding rates and improved infant and maternal health result (see Figure 1). However, the infant formula marketing system is prevented from responding to consumer needs as feedback loops are severed, restricting emergence and adaptation of the marketing system within the embedded system to respond. The promotion of breastfeeding and concomitant restriction of information regarding infant formula leads to externalities of the infant health system, which are negative outcomes for those individuals unable or unwilling to breastfeed (Figure 1). At the individual level, mothers are stigmatized and confused as their choices are restricted (Dattilo et al. 2020; Fallon et al. 2017; Moss-Racusin et al. 2020).
Corporate power and manipulative methods are often at the forefront of arguments for stronger regulation and enforcement (Hastings et al. 2020). Yet these arguments often conflate marketing practices with the marketing system. Harsh regulation to reduce unethical practices limits choice for consumers and undervalues the highly specialized product development to meet needs of consumers. Moreover, forced into covert messaging, infant formula companies can perpetuate such practices in a vicious circle due to marketing system failures.
System History
Over time system history reinforces these patterns. The marketing system failure which embedded [infant health] system philosophy and practice structures into marketing system structures as a system of provision cannot easily be dismantled or reassembled. Powerful habitual professional behavior and institutional logic embed regulatory controls.
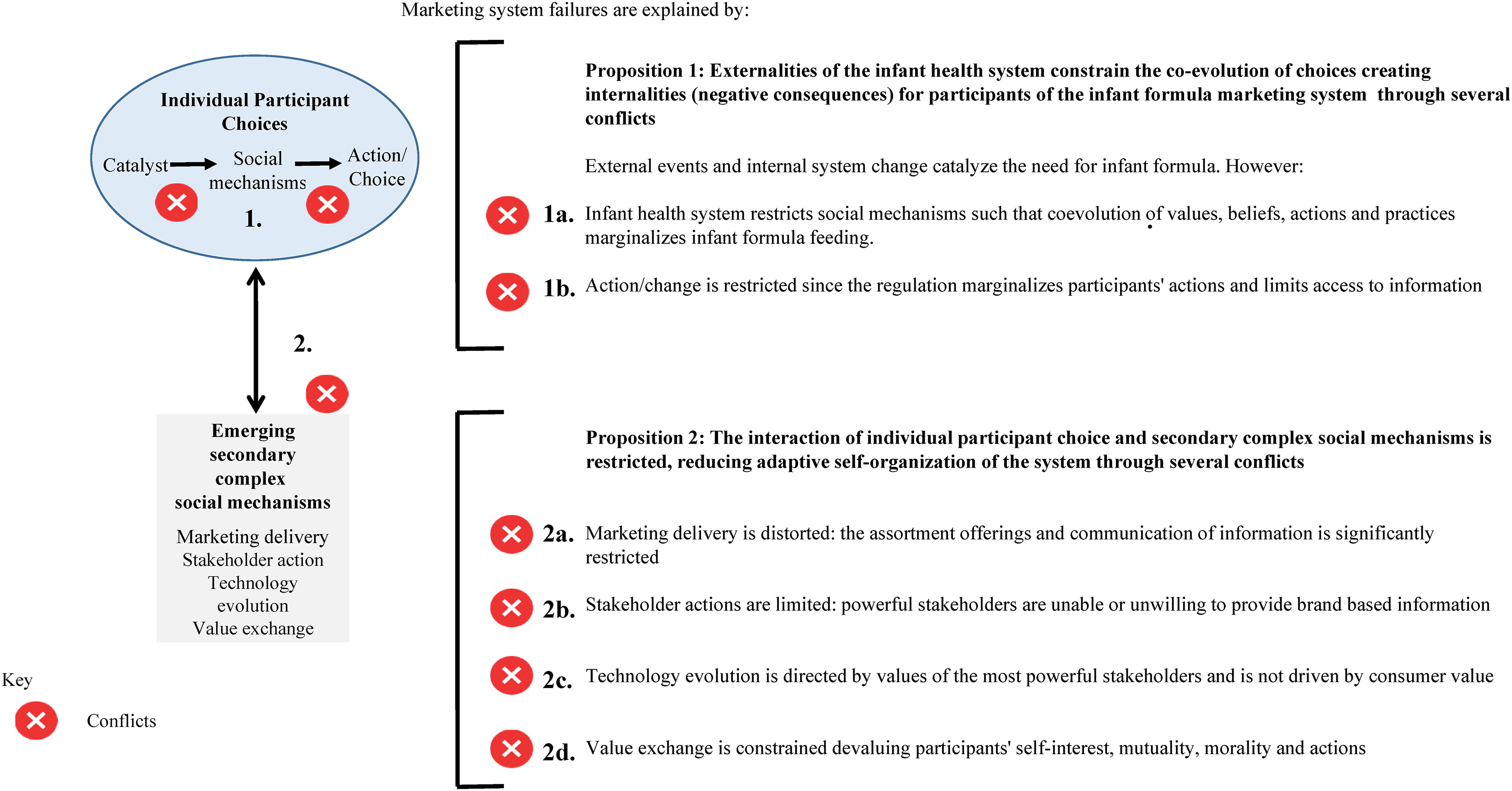
We discuss below the points of marketing system failure from regulatory intervention, illustrated in Figure 2. The conflicts are labelled according to the two propositions (1a, 1b, and 2a, 2b, 2c, and 2d) in the narrative and the figure illustration.
Marketing System Failure #1: Constrained Co-evolution of Choice
The institutional structure is shaped by the regulation which shifts control of information away from the infant formula marketing system and influences participant choices. Agency is enabled for health professionals and constrained for marketers of infant formula. While this increases agency for consumers who can, and choose to, breastfeed, it simultaneously decreases agency for consumers in the infant formula marketing system. While external events catalyze a want or need to formula feed, consumers no longer interact with the infant formula marketing system to determine co-operative choice and instead rely on individual health professionals who are often embedded in organizational structures with associated institutionalized logic promoting breastfeeding (such as the Baby-Friendly Hospital Initiative, WHO/UNICEF 2018). Social mechanisms of co-evolving values, beliefs, actions, and practice in support of infant formula feeding are restricted or even discredited (Figure 2 conflict 1a). Health professionals may be apprehensive about providing information regarding infant formula perceiving it as a risk to their obligations as a health professional. To do so may be construed as a threat to their mandate to provide optimal health outcomes for mothers and infants and their expertise. Again, the provision of information may be constrained or nonexistent. Consumers in the infant formula marketing system become less well-off and as such are externalities of the infant health system, either unable to access information or derogated and/or labelled as failing by either (or both) systems. As a result, they experience reduced power and may even be powerless to make change (Figure 2 conflict 1b). They may assign choice to another system actor or if they do act, not disclose or lie to reduce negative responses from powerful actors in the infant health system.
Amid the debate regarding infant nutrition is the issue of power dynamics. Light (1991) conceptualized countervailing powers to help explain the complicated power distribution, relationships, and tensions in the market-based health system. The notion of countervailing powers, where power is contextual and subject to counter moves by other actors, is useful to understand the infant nutrition debate and the intended (and unintended consequences) of regulatory interventions. Yet, stigma created due to the breast is best narrative are socio-cultural, historical constructions (Crocker, Major, and Steele 1998), and thus are created and change. They can only occur when the dominant voice proposing the stigma is also the most powerful (Link and Phelan 2001).
Thus, stigma in this case is enacted through discriminatory practices “in the community, at home, in the workplace, in the media and in legislation, and in health and social services…public health programs…media images…and in educational materials” (Van Brakel 2006, p 328). The process of stigmatization occurs through 1) Negative treatment and discrimination by way of limited access to health care, due to institutional practices (Crandall and Eshleman 2003); 2) Expectancy confirmation bias that leads stigmatized people to inadvertently live up to the negative attributes attached to their stigma (for instance being perceived as a bad parent); 3) Automatic stereotype behavior where the stigmatized person adopts the related negative attributes (they act as a ‘bad parent’); and lastly through 4) Identity threat which one might assume is stronger for first time parents who are only just integrating their social identity as a parent, and can lead to increased stress and anxiety around the social identity which is challenged (Major and O’Brien 2005).
Therefore, while infant formula adoption may be seen as challenging health professionals’ authority and expertise, a constrained co-evolution of choice (as shown through a systems lens) limits consumers’ choices, their voice, and can affect their mental health and self-identity as a parent, leading to Proposition 1: Externalities of the infant health system constrain the co-evolution of choices creating internalities (negative consequences) for participants of the infant formula marketing system through several conflicts, Conflict 1a: Infant health system restricts social mechanisms such that coevolution of values, beliefs, actions, and practices marginalizes infant formula feeding. Conflict 1b: Action/change is restricted since the regulation marginalizes participants’ actions and limits access to information.
Marketing System Failure #2: Restricted Co-evolution of Secondary Social Mechanisms
Intervention in the form of regulation leads to consequent structural and procedural changes in the infant health system which restrict catalyzed evolution of choice for consumers through power imbalance and conflict that arises. The second proposition relates to the way this in turn influences network level social mechanisms within the infant formula marketing system in a reciprocal manner.
Claims of aggressive marketing of infant formula eventually led to the WHO Code and subsequent World Health Assembly resolutions banning the promotion of infant formula and other breastmilk including through advertising and other forms of promotion (WHO 1981). In particular, mothers were “often inundated with incorrect and biased information from direct advertising, health claims on products, information packs from sales representatives, the distribution of samples of infant formula” (p. 32), and marketing messages “idealized the use of breastmilk substitutes” (Pomeranz and Harris 2019, p. 34). Maternity paediatric organizational processes (e.g., Ten Steps to Successful Breastfeeding guidelines, WHO/UNICEF 2018), health professional/stakeholder espoused values govern infant feeding practice. Campaigns and slogans supporting the breastfeeding message, such as the breast is best slogan, are well known and disseminated widely through antenatal education classes and educational media. Strong moral and social norms directly link to notions of idealized motherhood where failure to breastfeed leads to discourses of transgression and stigma (Dattilo et al. 2020; Moss-Racusin et al. 2020; Símonardóttir and Gíslason 2018; Williams, Donaghue, and Kurz 2013). Furthermore, actor health professionals and policy makers contain considerable power to distribute sanctions or penalties. Thus, the development of powerful institutional logic and norms along with regulation underpin the infant nutrition social system.
Layton (2007, 2015) and Layton and Duffy (2018) propose four network level mechanisms in marketing system evolution that can contribute to this context of observed marketing system failure described above.
- Marketing delivery: Marketing delivery decisions may become focused on marketplace sales access and volume. Indeed, while some markets emphasize formula sales via pharmacies others rely on supermarket distribution. In this environment, heuristics such as price and packaging may drive demand rather than other technological changes that cannot be communicated to consumers and/or are heavily regulated. These shift evolutionary processes related to consumers away from opportunities such as ingredient quality and product improvement that are not ‘visible’ in commercial contexts (Figure 2 conflict 2a). Infant formula companies may invest in costly one to one marketing via health professionals, channeling of resources away from innovation and restricted communication of such innovation to mothers Companies may attempt to communicate with their target consumers via covert means, marketing, and providing information about transitional feeding milks for older infants in an effort to build brand equity (Baker et al. 2021; Berry, Jones, and Iverson 2012). - Stakeholder actions: Power now resides with health professionals (Figure 2 conflict 2b). Following the code of practice and due to prior unethical marketing practices by infant formula companies (Hastings et al. 2023), these stakeholders may be fearful of providing individual advice. They may instead be motivated by group level health outcomes and not wish to advance what they could consider as the interests of infant formula companies, by advising parents about products. In attempting to remain impartial these stakeholders may not recognize functional benefits of competing alternatives. Group level decisions such as contracts with maternity and pediatric hospital departments may influence marketing stakeholder power. Infant formula companies are incentivized to gain economies of scale through increased production and reduced ingredient costs if their target market cannot access information. - Technology evolution: Health professionals assume the position of catalysts of change in the infant formula feeding system and system evolution becomes focused on the values and norms of this group. This may lead innovation toward ethical conduct at the expense of scientific product composition innovation and other consumer driven factors such as convenience (Figure 2 conflict 2c). Consumer value may fail to drive change. Self-correcting evolutionary dynamics that are driven by consumer demand may not occur as consumers cannot access infant formula companies for advice. Companies are then not motivated to innovate. - Value exchange: Value exchange and mechanisms of value provision are constrained due to the highly restricted access to information in the infant formula marketing system and often, also in the adjacent infant health system. At network level the emphasis is on value exchange for the gatekeepers rather than the consumers, constraining consumer's choice criteria and known attributes. Studies continue to demonstrate the limited information and support for parents regarding formula products and the lack of resources to aid in product decision-making, with negative consequences (Fallon et al. 2017; Malek et al. 2019) devaluing participants’ actions and the basis of the choice in terms of self-interest, mutuality, and morality (Figure 2 conflict 2d). In addition, infant formula companies are required to always advocate breastfeeding and in so doing, may inadvertently contribute negatively to the value exchange and stigma attributions toward infant formula. If consulted, health professionals may encourage loyalty to one formula brand and once the baby is settled, parents are unlikely to change formulas unless there are adverse changes, locking in choice. Parents can experience such stigma through the attitudes of health professionals towards their use of formula, the lack of health services to help them to use formula, discrimination from social groups where breastfeeding is the key activity, as well as perceived and internalized stigma (Van Brakel 2006). Stigma may restrict consumer transparency. Catalyzing events for stigmatized participants shift influence away from the agents empowered by the regulatory intervention (health professionals) inadvertently forcing consumers to rely on stakeholder actions such as distribution in convenient locations and pricing. Proposition 2: The interaction of individual participant choice and complex social mechanisms is restricted, reducing adaptive self-organization of the system through several conflicts, Conflict 2a: Marketing delivery is distorted: the assortment offerings and communication of information is significantly restricted. Conflict 2b: Stakeholder actions are limited: powerful stakeholders are unable or unwilling to provide brand based information. Conflict 2c: Technology evolution is directed by values of the most powerful stakeholders and is not driven by consumer value. Conflict 2d: Value exchange is constrained devaluing participants’ self-interest, mutuality, morality and actions.
This leads to
Policy and Regulatory Intervention to Remedy Provisioning and Marketing Systems Failure
We argue that regulation has contributed to marketing system failures at the intersection of two complex provisioning systems. Paradoxically, we also propose that regulatory mechanisms can mitigate these marketing system failures. Padela, Wooliscroft, and Ganglmair-Wooliscroft (2023, p. 392) remind us that “marketing systems operate through the flows of ownership, possession, finance, risk and information.” Examining the infant health system and the infant formula marketing system interaction demonstrates the need for these elements and interactions to be better integrated to avoid marketing system failures noted above. Integration of these processes can be achieved through a co-design and co-creation approach to regulation, and information flows, or at the least, participatory processes that include more open and transparent information and resource exchange. Whereby infant formula marketing system stakeholders are brought into the infant health system alongside stakeholders of government, health professionals (including frontline staff in the infant nutrition arena), caregivers and parents. Regulation co-design will be challenging to implement demanding negotiation and interaction among multiple stakeholders who have powerful habitual professional behaviors and embedded institutional logics. However, protocols for such interactions have already been proposed and tested (McHugh, Domegan, and Duane 2018).
Importantly, such regulatory mechanisms will serve to de-conflate infant formula marketing practices from the marketing system. The top-down regulatory /government driven infant nutrition system and the consumer-advocate driven bottom-up forces need to co-exist with the marketing system to provide consumer choice, overt evolution of specialized product development, shared power and agency, to meet the needs and wants for goods and services. Such an approach is possible when considering such frameworks as the Dynamic Stakeholders’ Framework which combines Layton's MAS mechanisms and Coleman's Boat to account for the dynamic nature of these interactions (Domegan et al. 2019). Regulatory intervention to remedy marketing systems failure must be seen within the provisioning system which Fanning, O’Neill, and Buchs (2020) define as “a set of related elements that work together in the transformation of resources to satisfy a foreseen human need” (p. 3). Top-down regulating in one system in isolation of the related elements and market access to satisfy multi-stakeholder needs (consumers, caregivers, health professionals) in another is likely to be ineffective.
Hastings et al. (2020) suggest some radical revisions to infant formula marketing practices to reduce “dangerous over-consumption in the interests of corporate profits” (p.10) calling for a Framework Convention with global reach equivalent to tobacco and climate. We do not disagree with the need for radical revision but argue (possibly controversially) that any regulatory intervention must be undertaken through a participatory framework, adopting a systems approach whereby the regulation is co-produced by government and consumer stakeholders (Fusco, Marsilio, and Gugliemetti 2020) and that the human perspective is not overlooked. Approaches to co-production and co-design of regulation, as well as social marketing intervention, must be balanced and non-judgmental to facilitate deinstitutionalisation of norms around infant nutrition (Kemper and Kennedy 2021), compared to the often divisive ‘breast is best’ messaging (Brown 2016; Holcomb 2017). The shaping of messaging in all infant nutrition across a large and diverse global community should seek to emphasize the valuable outcomes to be achieved for all stakeholders.
Implications
Layton (2007) highlights the integral role of the macroenvironment in marketing systems and Fine and colleagues (Fine, Bayliss and Robertson 2018) concur building in the systems of provision perspective whereby the level of consumption and its meaning evolve from such systems of provision. In this article we combine these perspectives to consider how marketing system failure can occur under conditions of regulation. We build on the solution to path dependent lock-in suggested by Williams, Davey, and Johnstone (2021) in their work on marketing system failure by integrating the role of stakeholder considerations in these processes. As such we provide three contributions:
We extend the model of the marketing system (Layton 2007, 2015; Layton and Duffy 2018) for when regulation extends a provisioning system beyond the focal marketing system. A ‘system of provision’ perspective (Fine, Bayliss and Robertson 2018; Layton and Domegan 2021) integrates systems beyond the marketing system in a more nuanced way. It allows us to consider how institutional structures are shaped by regulation, how the processes through which service providers relate to consumers can create tensions between systems and interactions with agents or agencies become negative, and even stigmatizing, due to power imbalance and conflict in relations. Williams, Davey, and Johnstone (2021) proposed that using a systems perspective (macro, meso and micro) could direct intervention to resolve negative outcomes for society (for sustainability and wellbeing) that is resolving ‘Marketing System Failure’. They propose this could be done by shifting stakeholder power. The current work focusses on the situation where failure has occurred as a result of regulatory intervention. This idea is not new (Carman and Harris 1986) but as the current case illustrates it is not the implementation of the policy nor interference that is at fault, but rather power imbalance that privileges macro level societal considerations as the determinant of the failure. Concurrent stigmatizing effects at micro level remain invisible. We propose government and consumer participation in co-production and co-design of regulation so that macro and micro level concerns are integrated via co-production taking into account the complexity of the social construction of value by regulated provisioning systems at the intersection of health and marketings.
Future Research
This conceptualization of the provisioning systems raises a number of research questions that can be addressed in further studies. Firstly, qualitative investigation should address marketing systems failure under conditions of provisioning systems by exploring:
- How key stakeholders in the infant health system interpret the WHO regulations and perceive their roles in relation to the infant formula marketing system. - How key stakeholders in the infant formula marketing system interpret the WHO regulations and perceive their roles in relation to the infant health system. - What negative effects consumers in the marketing system experience in their interactions with the infant health system. In particular how consumers traverse the two systems when they engage in both infant feeding practices.
Future research should also quantify marketing system failure in order to assist with improving societal outcomes at both a population level as well as at the level of agent practices when two complex systems intersect.
Concluding Comments
Using the example of the infant formula marketing system and responding to the UNSDGs’ call and Macromarketing's underpinning to advance societal goals, we extend marketing system failure conceptualization under conditions of system regulation, blocking co-evolution of choices in the marketing system. Applying Layton's marketing systems framework, we provide an extension of the knowledge around marketing system failure, and the interaction of two systems on that failure.
Whereas elsewhere intervention and regulation are recommended to remediate marketing system failure (e.g., Williams, Davey and Johnstone, 2021), in this case, regulation (brought in largely due to poor practices of infant formula marketing initially) restricts the marketing system's ability to co-evolve causing system failure. Externalities of the social system constrain the co-evolution of choices creating internalities (negative consequences) for participants of the infant formula marketing system, due to (inter alia): decreasing power to marketers to share information to consumers (the usual disseminators of marketing product related information), asymmetric information negating the capabilities and agency of mothers, de-legitimization of the infant formula market and stigmatization of participants further decreasing consumer engagement with the market. Together, restraining the marketing system and denying certain groups market access which can lead to “detrimental choices in the very market that can potentially benefit those individuals” (Leary and Ridinger 2020, p. 100). While value is the intended consequence of action in the marketing system, marketing system failure occurs when desirable “social benefit” for participants do not occur (Redmond 2018, p. 422). In this conceptual study we propose that regulation that links a marketing system to an adjacent health system leads to marketing system failure when the complex provisioning systems and embedded nature of the marketing system are overlooked.
The unique context explored in the current work involves a binary choice between two alternatives where one is clearly superior in terms of scientific composition, cost, and many other benefits. The infant formula marketing system can be likened to other commercially available alternatives when nature fails as a suitable option. Examples include products like fertility services, synthetic blood, and optionally available pharmaceutical products for conditions such as weight loss or depression. This work will be useful in other similar contexts where regulation links the health and marketing systems for provision of information to consumers.
Footnotes
Associate Editor
Ben Wooliscroft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article