
Abstract
Background
Informed choice is of the highest importance in health care. However, confusion and challenges remain toward how it is conceptualized and measured.
Purpose
This umbrella review aimed to establish how informed choice is operationalized in health care and the characteristics and performance of the most commonly used measurement instruments.
Data Sources
Four electronic databases (Ovid MEDLINE, Ovid EMBASE, APA PsycINFO, and Cochrane Library) were searched up to January 29, 2024. Reference lists of included studies were hand searched for further relevant publications.
Study Selection
After the titles and abstracts of 10,434 articles were screened by one reviewer and 10% were screened by a second reviewer for consistency, 2 reviewers independently screened 60 full-text articles for inclusion. Key eligibility criteria included systematic reviews in adult health care settings where the aim included an evaluation of measures of informed choice. Sixteen articles were included.
Data Extraction
Data were independently extracted by 2 reviewers using a standardized template. Data Synthesis. Data were synthesized using the summarization technique with systematic reviews as the main unit of analysis and additional subanalysis of primary measurement instruments identified.
Limitations
Heterogeneous definitions complicate search strategies, and eligibility criteria may limit external validity. The ROBIS appraisal identified many reviews as high risk of bias, limiting the conclusions drawn. Due to heterogeneity, meta-analysis was not possible, and conclusions were limited to narrative reviews.
Conclusions
There remains no consensus on how informed choice should be conceptualized and measured within health care. This review attempts to bridge these gaps by presenting available concepts and instruments for clinicians, researchers, and policy makers. Future recommendations include achieving consistent definitions of informed choice and related concepts, followed by the use of standardized, validated, multidimensional instruments informed by theory in diverse populations.
Highlights
Informed choice is of key importance and increasingly emphasized across health care.
Despite this importance, confusion and challenges remain regarding how informed choice is conceptualized and measured in health care.
Consistent definitions and the use of standardized, validated, multidimensional instruments, informed by theory and patients themselves, in diverse populations should be the first steps to improve this.
These recommendations apply to all in health care, including health professionals, researchers, and policy makers.
Keywords
Informed choice is of the highest importance in health care and increasingly emphasized, especially in clinical trials, treatment decisions and screening.1–5 In addition to the ethical and legal responsibilities,6–8 informed choice carries potential economic and patient outcome benefits.9,10 Measuring informed choice, however, remains difficult,11–13 including a lack of consensus on what qualifies as “informed”14–17 and individual variability.6,14,18,19 Evidence shows that patients’ needs for information differ.11,15,16,20,21–23 One surgical-based trial found that 88% of patients wanted to know the short-term effect on activities postoperatively, yet only 62% wanted the technical details. 24 Similarly, in breast screening, a qualitative study found disagreement among participants as to whether they would want to be informed of overdiagnosis as a risk. 25 What constitutes necessary information by those responsible for imparting it—health professionals, researchers, or policy makers—can also differ from the public’s wants.11,14,15,20,21 A separate UK study on breast screening leaflets found that while experts advocated for scientific precision and detailed statistics, participants favored simple explanations. 26
Another challenge is the overlapping concepts in literature and guidelines.11,15,20,27 Table 1 presents example definitions for informed choice and related concepts. As observed, O’Connor et al.’s definition of an effective decision being “informed, consistent with values and congruent with behaviour” 28 has also formed the basis for concepts including informed choice, informed decision, and decision quality.15,20,27–31
Example Definitions of Informed Choice and Similar Concepts
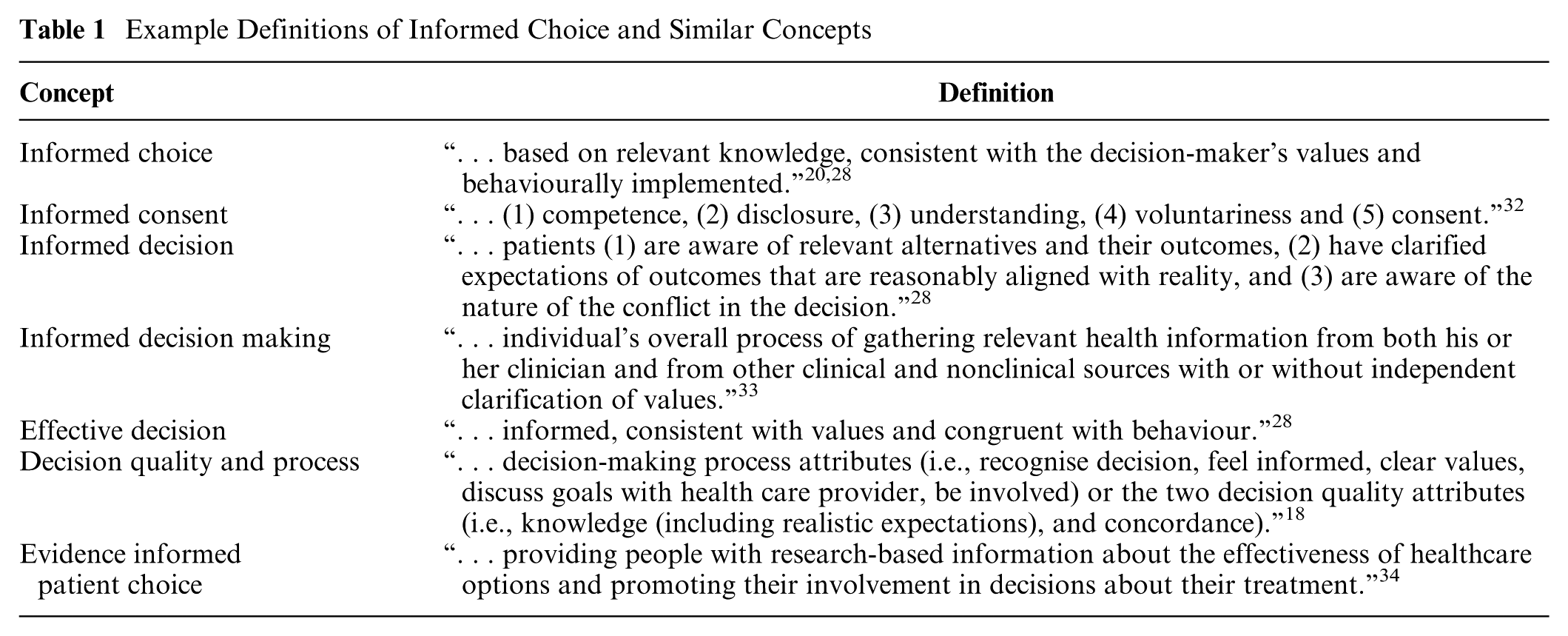
Subject experts have attempted to distinguish between terms.15,30,35 Jepson et al. 15 argued that informed choice, unlike informed consent, is more suitable in screening where individuals are invited and choose to participate, without necessarily interacting with health care professionals. Østerlie et al. 14 agreed, seeing informed choice as fitting for nonobligatory health services. Rimer et al. 35 went further to differentiate informed consent from informed or shared decision making. They emphasized decision making’s focus on value congruence (an individual’s values reflected in their decision) and patients having flexible participation. Briss et al. 30 also distinguished shared from informed decision making, noting that shared decision making involves both patients and professionals, often in a clinical setting, participating in decisions in a personalized manner. They further suggested that informed decision making can occur without professional involvement, such as in screening contexts. 30 While these explanations clarify subtle differences, confusion remains over when each concept is more appropriate. 14
This confusion extends to which components should be measured.27,36–38 Knowledge, representing “informed,” appears logical to measure,11,15,30,31 yet other domains, such as anxiety during decision making, are more contentious.23,19,31,39 Bekker et al.31,39 cautioned against the use of anxiety when measuring the effectiveness of patient decision aids (PtDAs)—tools designed to support an individual’s decision process to reach an informed choice40,41—finding it inadequate and lacking evidence in its association with adverse consequences of decision making. 39 Despite this, the 2017 Cochrane review of PtDAs found that 30% of studies continue to assess anxiety. 42
Despite existing guidelines to support the choice and development of measuring instruments, 43 such as the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN),44–46 or the International Patient Decision Aid Standards (IPDAS) collaboration, 47 and more specific Core Outcome Sets, including Gillies et al. 48 for informed consent in randomized control trials (RCTs), or Convie et al.’s 49 evaluation of surgical informed interventions, measuring informed choice remains difficult.11,13,19 Systematic reviews provide some insight,11,13,19 although they are mostly limited to the comparison of one concept across individual studies. 50 Furthermore, accessing and using high-quality evidence among multiple reviews is difficult. 51 An umbrella review, which collates systematic reviews, is an efficient way to gather the best available evidence and is often used in health care policy.50,52–54 The approach is especially useful for bridging gaps between closely related concepts often analyzed separately, enhancing the understanding of different perspectives.50,51,55
This umbrella review aims to establish how informed choice is operationalized and measured across health care and to determine the characteristics and performance of the most commonly used or appraised measurement instruments identified for informed choice. This will enable health professionals, researchers, and policy makers alike to select the concept or instrument that best suits their work and support future high-quality research in the field.
Methods
Methods were guided by the Joanna Briggs Institute Umbrella Review Approach and Cochrane’s Overview of Reviews.50,52 Reporting adheres to the Preferred Reporting Items for Overviews of Reviews (PRIOR). 53 The protocol for this review was registered with the International Prospective Register of Systematic Reviews (PROSPERO CRD42024513810). 56
Search Strategy
Search strategies were devised in consultation with medical librarians. The following databases were searched for relevant studies on January 29, 2024.
Ovid MEDLINE (1946 to January 26, 2024)
Ovid EMBASE (1974 to January 26, 2024)
APA PsycINFO (ProQuest)
Cochrane Library (Advanced Search)
Searches were limited to English language, human studies, meta-analysis or systematic review, and 1990–current, reflecting the limited number of systematic reviews before 1990. 50 The search strategy exemplar for Ovid EMBASE is presented in Appendix 1. The reference lists of the included studies were hand searched to identify further relevant publications.
Eligibility Criteria
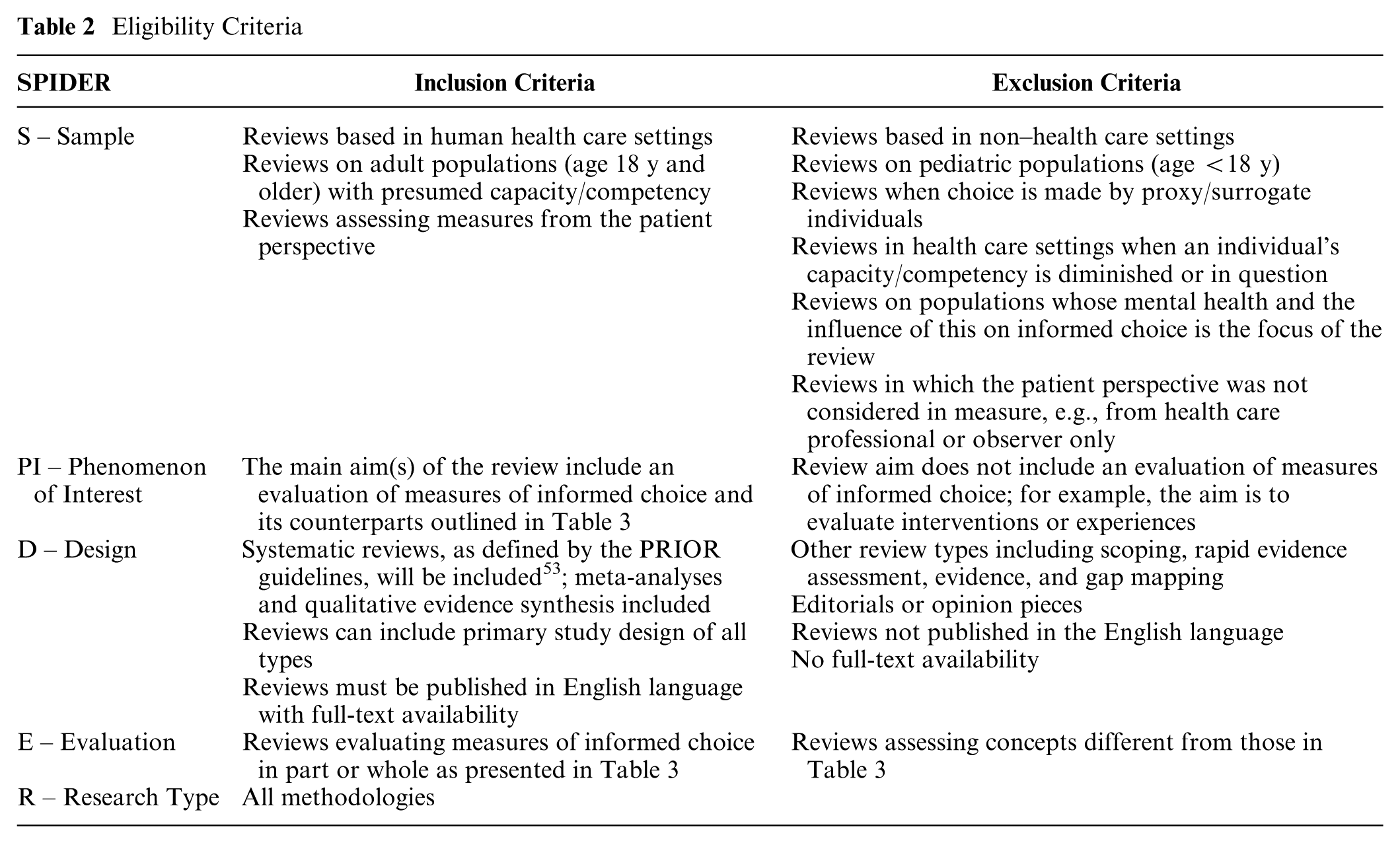
The inclusion and exclusion criteria applied are shown in Table 2. For consistency and conciseness in this review, when referring to measures of informed choice, it will encompass measures of all the concepts stated in Table 3 unless explicitly stated otherwise.
Eligibility Criteria
Concepts Relating to Informed Choice
One reviewer screened all titles and abstracts, with 10% of articles randomly screened by a second reviewer for consistency. Where disagreements on an article’s inclusion for full-text screening arose, these articles were included. Eligibility criteria were then piloted using 10 full-text articles, with final eligibility criteria formalized subsequently with third and fourth reviewers. Two reviewers then applied the criteria to assess all full-text articles independently. Disagreements on final eligibility were resolved with all reviewers, with consensus on included articles reached. In the case of overlapping systematic reviews, all relevant reviews were included. 52
Data Extraction
Data extraction was performed independently by 2 reviewers using a standardized template (Appendix 2). Extracted data included review demographics; the concept assessed; definitions; how measurement instruments were evaluated; key study findings, including any psychometric results, specific measurement instruments, and their properties; and any limitations or recommendations made by reviews. Any discrepancies were resolved with third and fourth reviewers, with a consensus reached.
Critical Appraisal
Independent critical appraisal by 2 reviewers using the Risk Of Bias In Systematic Reviews (ROBIS) tool was conducted. 57 The third and fourth reviewers were consulted for any disagreements to reach a consensus. All systematic reviews were included to assess the breadth of available evidence, irrespective of appraisal outcomes.
Data Synthesis
Data synthesis was performed with the systematic reviews as the unit of analysis and then again in a subanalysis with the primary instruments measuring informed choice identified within the systematic reviews as the unit of analysis to meet the 2 aims of the review.
Extracted data from systematic reviews were analyzed and reformatted in alignment with summarization techniques for umbrella reviews.50,52 The subanalysis focused on the most commonly used or highly rated measures of informed choice, selected based on their frequency cited in reviews or when singled out for appraisal or discussion by reviews, with additional data from primary studies and wider literature supplementing findings.
Meta-analysis was not performed due to the heterogeneity between reviews and the inclusion of qualitative and quantitative data.
Results
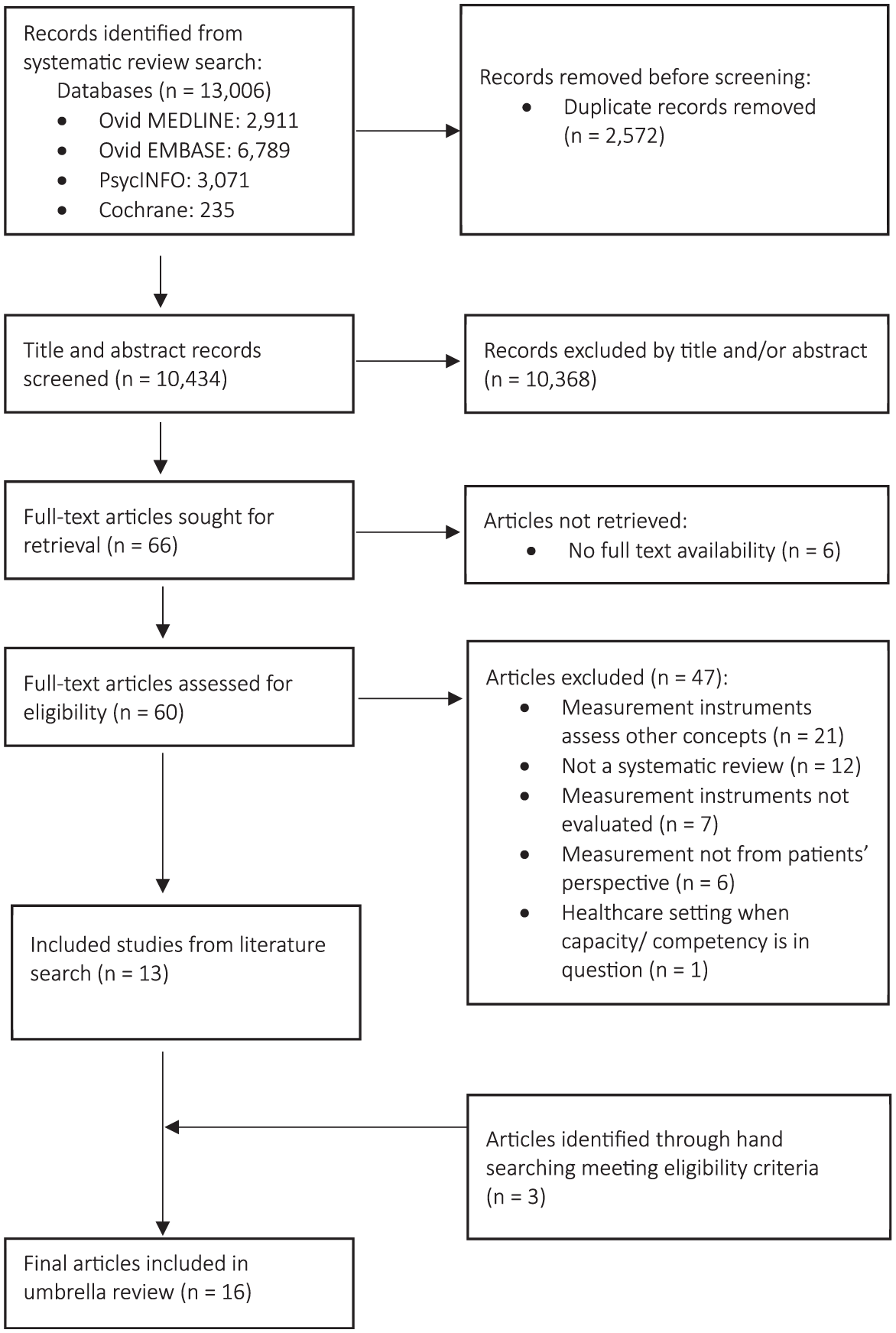
The search results are presented in Figure 1. In total, 13,006 citations were identified from electronic databases. A total of 2,572 duplicates were removed, leaving 10,434 unique results. Title and abstract screening resulted in 10,368 exclusions. The consistency of the interrater reliability for screening was 99.45%. Of the 66 remaining articles, 6 had no full-text availability, with the other 60 full texts screened using eligibility criteria. Forty-seven articles were excluded for not meeting the criteria. Appendix 3 provides the list of excluded articles with reasons. Thirteen articles from the electronic search met eligibility criteria, with a further 3 eligible articles identified through hand searching the reference lists. The final 16 systematic reviews are presented in Table 4.
Demographic and Conceptualization Features of the Included Studies
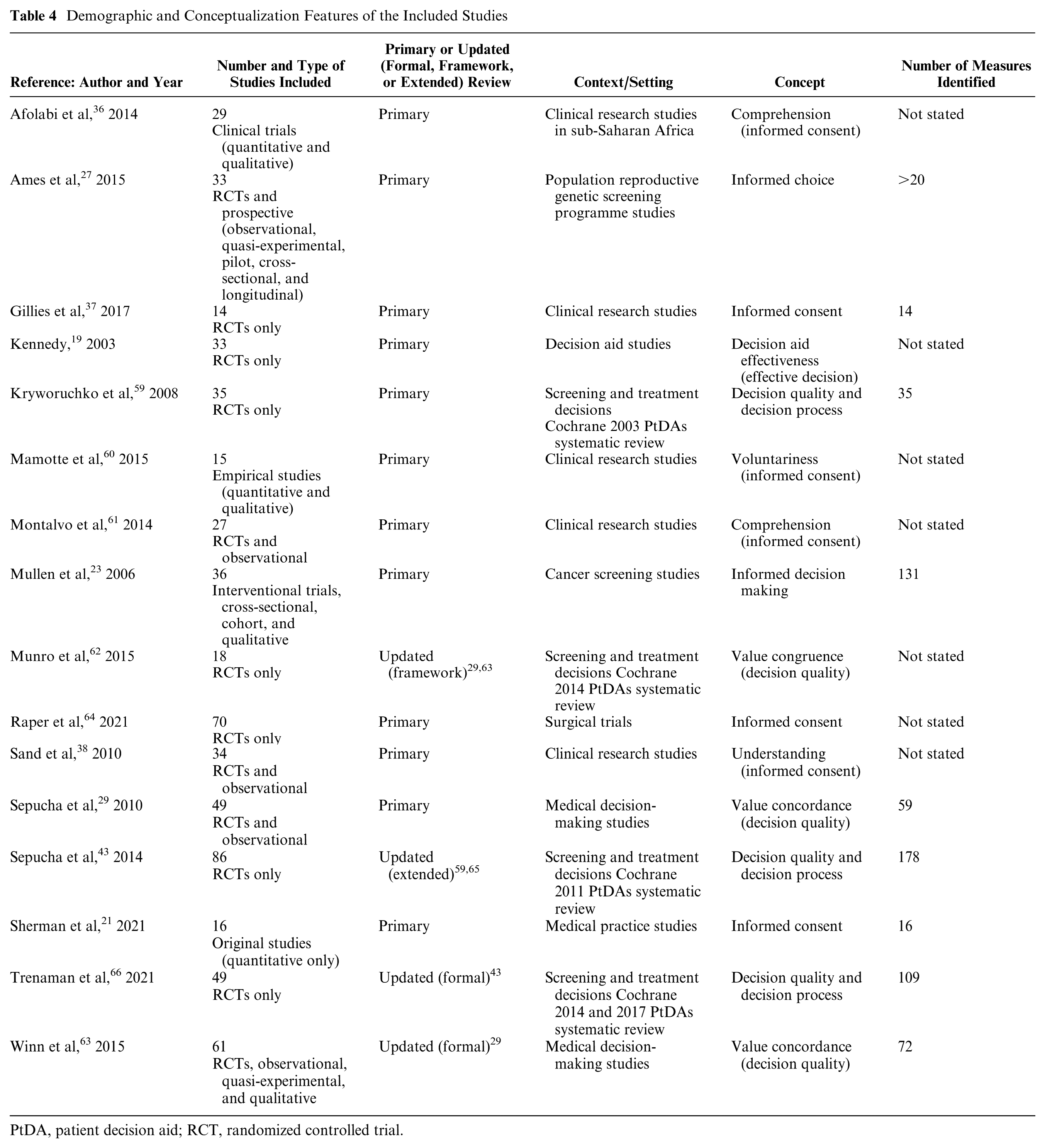
PtDA, patient decision aid; RCT, randomized controlled trial.
Critical Appraisal
The ROBIS results for each review are presented in Appendix 4. Appendix 5 demonstrates the percentage of reviews attaining a low, high, or unclear bias risk for each phase 2 domain and phase 3’s overall risk. Fifteen reviews were rated as being low risk for study eligibility criteria, identification, and selection of studies. One review prompted high-risk assessments for both domains due to a lack of transparent criteria, adequate search strategies, and justification for decisions. 19 Most studies were rated as high risk for data collection, study appraisal, synthesis, and findings, with 5 rated as low risk. This was largely due to no risk-of-bias assessment performed by the reviews themselves. Of the 5 rated low risk, 1 performed their assessment, 61 and the remaining used the Cochrane assessment on which they were based.43,62–66 This contributed to 10 reviews being scored as high risk of bias overall and 6 reviews being scored as low risk. One review that did not perform a risk-of-bias assessment justified its reasons—the review focused on methods rather than outcomes—and discussed this limitation. 63 As the concern was addressed, a low risk of bias was given.
Review Demographics
Review publication dates ranged from 2003 19 to 2021.21,66,64 The number of studies per review ranged from 14 to 86.37,43 Seven reviews included only RCTs,19,37,43,62–66,64 with the remainder including additional study types. i Three reviews focused on specific contexts—surgical trials, 64 reproductive genetic screening, 27 and cancer screening 23 —with the remainder consisting of generalized decision-making and clinical research studies. ii Concepts assessed included informed consent,21,37,64 informed choice, 27 informed decision making, 23 decision aid effectiveness (effective decision), 19 and decision quality or process.43,59,66 Seven reviews focused on a component of these concepts, including comprehension,36,61 understanding, 38 or voluntariness, 60 for informed consent and value congruence or concordance as part of decision quality.29,62,63 In addition to a narrative synthesis, 2 reviews also performed a meta-analysis using a random effect model due to study heterogeneity.36,62 Of the reviews that did not include a meta-analysis, 5 justified this as not possible due to heterogeneity.27,29,19,61,64
From the 16 systematic reviews, 15 had available lists of the included primary studies they reviewed. iii In the review by Mullen et al., 23 the authors reported their data in a table that was inaccessible online. From the 15 reviews, there were a total of 569 primary studies. This included 456 distinct studies and 113 that were present across more than 1 review, resulting in a primary study overlap of 20%.
Summary of Review Evidence
Table 5 summarizes common themes identified across systematic reviews regarding how informed choice is operationalized. These themes cover the underlying conceptualization, the methods of measurement (referred to as measurement instrument or tool), and how they are reported on by researchers in the literature.
Summary of Common Themes on Informed Choice Operationalization across Systematic Reviews
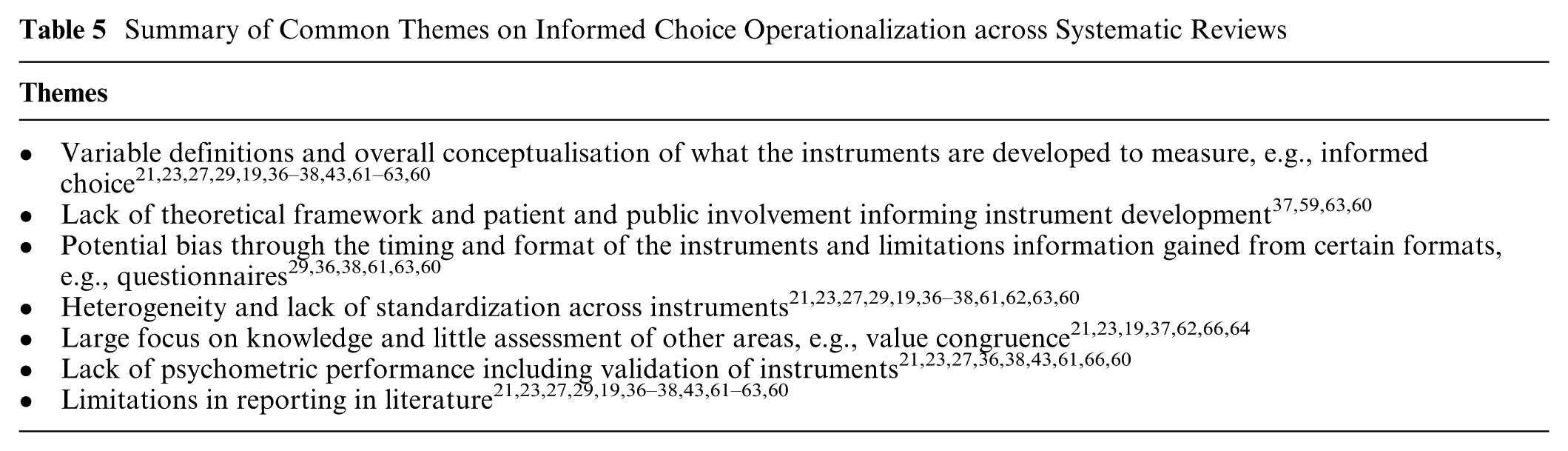
Variable Definitions for the Conceptualization of Informed Choice
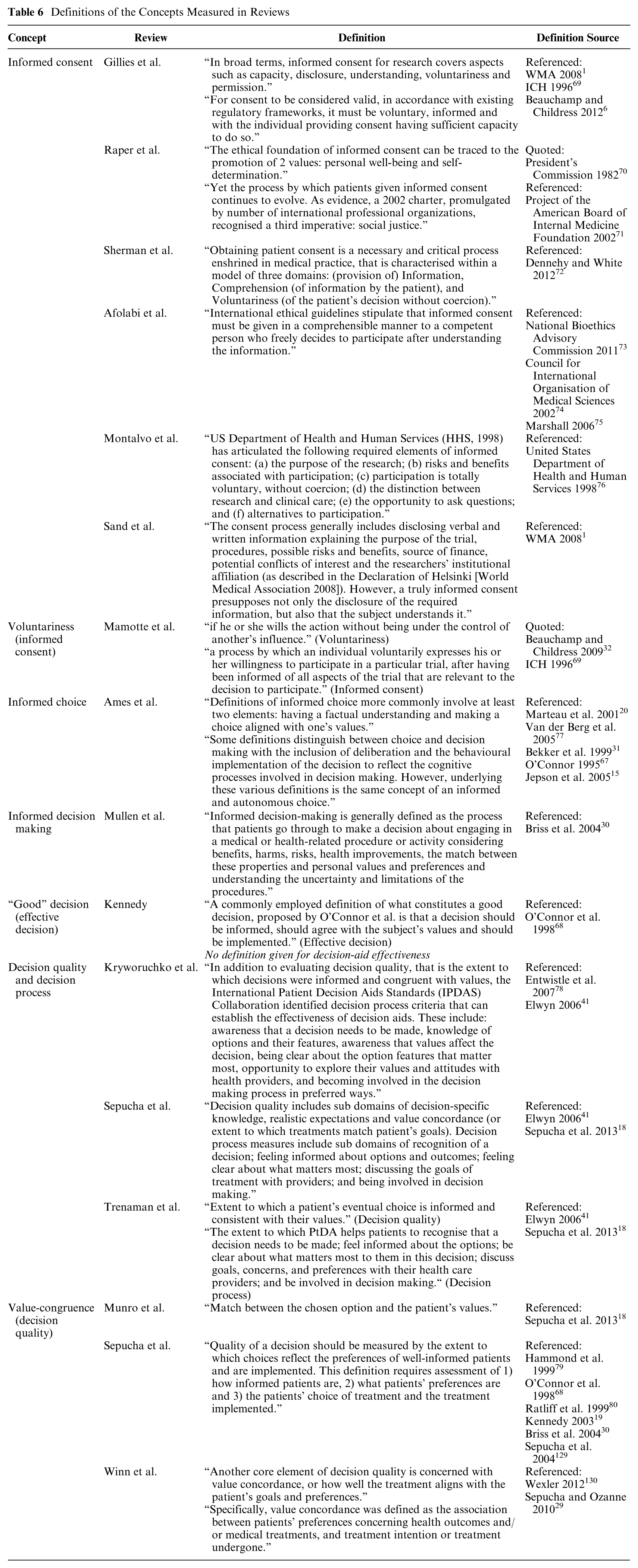
Table 6 details the definitions each review provided for informed choice. No 2 definitions for the same concept are identical, with a variety of sources referenced. Some reviews described similar definitions for terminologically different concepts. For example, Ames et al.’s informed choice definition includes “having a factual understanding and making a choice aligned with one’s values.” 27 Comparatively, Kennedy’s definition of a “good” (effective) decision includes “informed, should agree with the subject’s values and preferences.” 19 Both share O’Connor et al. as a source67,68 and are similar to definitions describing decision quality and informed decision making.23,29,43,62–63 Others’ definitions are based on organizational or governing recommendations, for example, the World Medical Association’s (WMA’s) Declaration of Helsinki. 1 Variability in definitions and conceptualization was a common theme identified in 9 of 16 reviews.23,27,29,36–38,61,62,60
Definitions of the Concepts Measured in Reviews
Underlying Theories and Patient and Public Involvement for Measure Development
Three reviews examined the role of theory in an instrument’s development. They highlighted how theory clarifies definitions, connects to broader knowledge, and supports construct validity.37,63 Gillies et al. 37 found that only 5 of 14 studies cited a theory, while Sepucha and Ozanne 29 reported more than half (28/49) referenced a framework, although Winn et al.’s 63 updated review found fewer (23/61). Two further reviews identified a lack of patient and public involvement (PPI) in an instrument’s development, reported in 5 of 14 and 1 of 8 studies, respectively.37,59
Timing and Format of Instruments
Eleven reviews assessed timing and/or instrument format. Timing varied from immediately after consent to more than a year later.36–38,60 Questionnaires with closed-ended questions were most common, while in-depth interviews and focus groups were less frequently used. For example, Mamotte and Wassernaar 60 found that 12 of 15 studies used questionnaires versus 3 of 15 using interviews. Some reviews used eligibility-mandated questionnaires or excluded purely qualitative studies.21,27,37 Six reviews acknowledged the potential bias that may arise through different instrument timings and formats and/or the limitations in information gained from certain formats, for example, questionnaires.29,36,38,61,63,60
Instrument Heterogeneity, Focus on Knowledge, and Concept Evaluation by Reviews
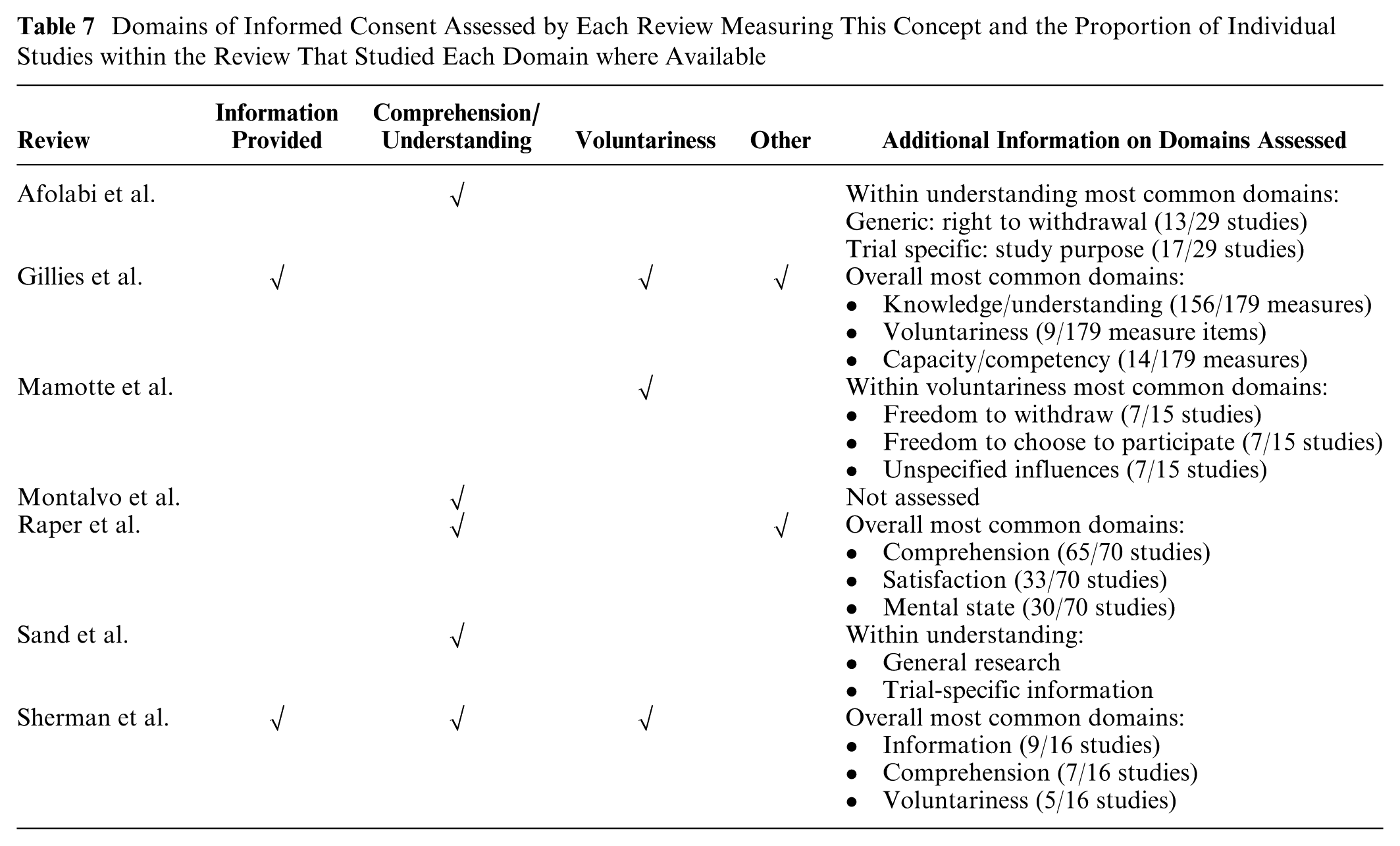
Heterogeneity and the lack of measurement instrument standardization were the most commonly identified themes across reviews (12/16). iv This will be exemplified in later results, although it is reflected in the reviews evaluating them also. Although most reviews examined which concept domains an instrument measures, their methods varied. For example, Sepucha et al. and Trenaman et al. used IPDAS criteria to code decision quality and process,41,43,66 while Raper et al. evaluated informed consent through autonomy, beneficence, and social justice.64,71,81 Due to the varied concepts and evaluation methods, pooling of the data was not feasible. Instead, Tables 7 to 9 describe the domains assessed by reviews and individual studies within them. The tables are divided based on the definition and concept they assess for comparison. Table 7 covers informed consent reviews; Table 8 shows informed choice, decision making, and effective decision, decision quality, and process; and Table 9 lists specific subdomains related to value congruence.
Domains of Informed Consent Assessed by Each Review Measuring This Concept and the Proportion of Individual Studies within the Review That Studied Each Domain where Available
Domains of Informed Choice or Decision Making, Decision Quality/Process, or Effective Decision and the Proportion of Individual Studies within the Reviews Measuring Each Domain where Available
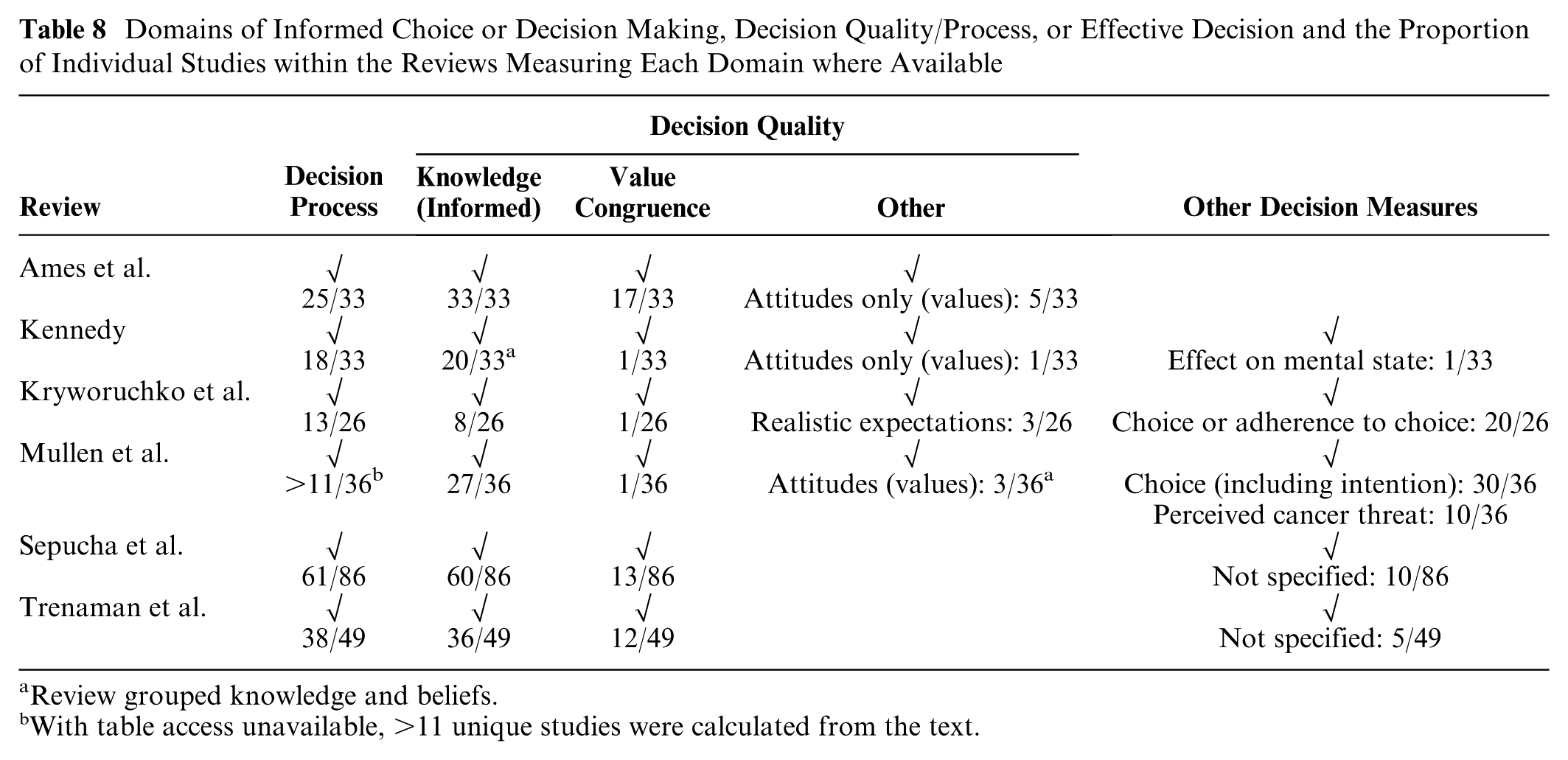
Review grouped knowledge and beliefs.
With table access unavailable, >11 unique studies were calculated from the text.
Subdomains within Value Congruence from 3 Reviews Solely Assessing This Domain a
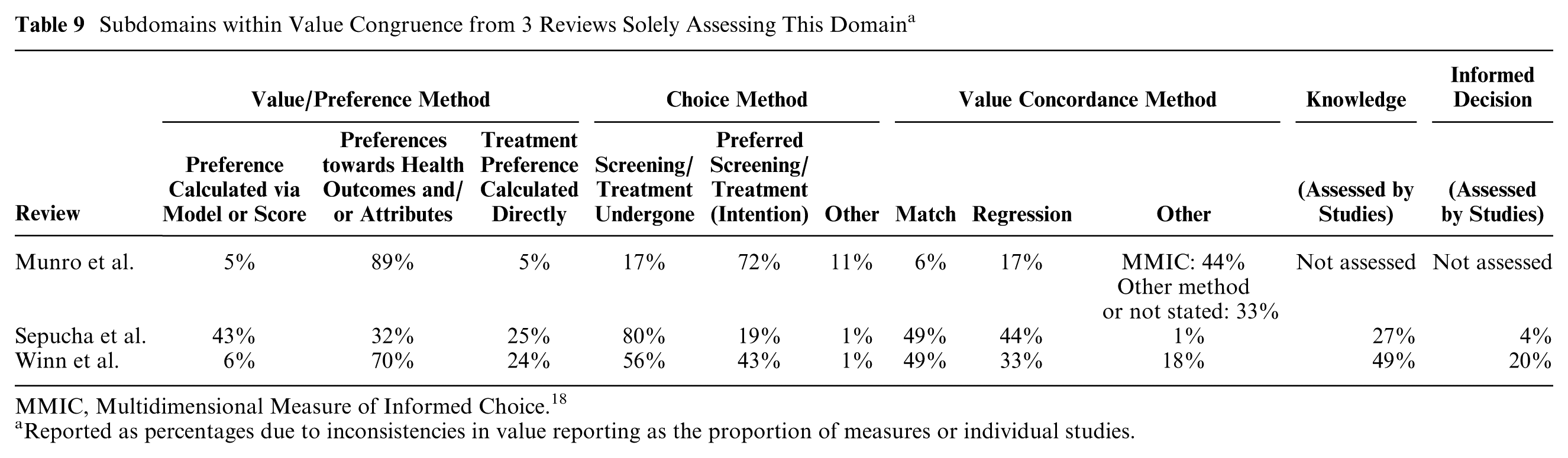
MMIC, Multidimensional Measure of Informed Choice. 18
Reported as percentages due to inconsistencies in value reporting as the proportion of measures or individual studies.
Key informed consent domains identified in Table 7 reviews included information provision, comprehension/understanding, voluntariness, and other.21,36–38,61,64,60 Within this, knowledge (information provision and/or comprehension) was the most measured in 6 of 7 reviews.21,36–38,61,64 One review by Gillies et al. 37 found knowledge included in 156 of 179 instrument items. Other domains, such as satisfaction, were studied less frequently.21,37,64 In specific comprehension/understanding or voluntariness reviews, study purpose and the right to withdraw were measured more than blinding, randomization, or therapeutic misconception.36,38,60
Knowledge remained one of the most measured domains in Table 8,23,27,19,43,66 although some reviews identified decision process measures such as decisional conflict or role preference 18 as more popular.43,59,66 Despite it being a requirement in the definitions for these concepts, value congruence was less commonly assessed.23,27,19,43,59,66
Table 9 reviews all used Sepucha et al.’s framework to define and calculate value congruence and its relationship to knowledge.29,62,63 Through this, they identified the variability in individual study methods, drawing conflicting conclusions in some areas.29,62,63 Relating to knowledge above, less than half of the individual studies assessed this alongside value congruence,29,63 with even fewer reporting if an overall informed decision was made.29,63 The Multidimensional Measure of Informed Choice (MMIC), 20 used in 44% of articles in Munro et al.’s review, 62 will be discussed further under characteristics of common measurement instruments.
Psychometric and Other Performance
Seven reviews evaluated the appropriateness, psychometric performance, and clinical sensibility of measurement instruments or their reporting.21,23,27,43,59,66,60 Kryworuchko et al. and Sherman et al. appraised measurement instruments themselves using published criteria.21,41,59,82,83 Kryworuchko et al. 59 found all 8 instruments rated positively for feasibility, followed by validity (7/18) and precision the least (1/8). Sherman et al. 21 found all 16 instruments internally consistent, but divergent (construct) validity was the least met (1/16). Sepucha et al. 43 and Trenaman et al. 66 focused on reporting, with reliability and validity reported in 21% to 23% and 6% to 16% of studies, respectively. Although feasibility was appraised positively above, 59 only 1 study in these reviews reported it.43,66 The remaining reviews discussed the number of studies attempting to establish validation and re-reported rather than reassessed these numbers.23,27,60 All except 1 of these 7 reviews commented on the lack of validation (or its reporting) of the measurement instruments.21,23,28,43,66,60 A further 3 reviews did not evaluate instrument psychometrics to the same extent, although they also commented on the lack of validation of chosen instruments.36,38,61
Limitations in Reporting in the Literature
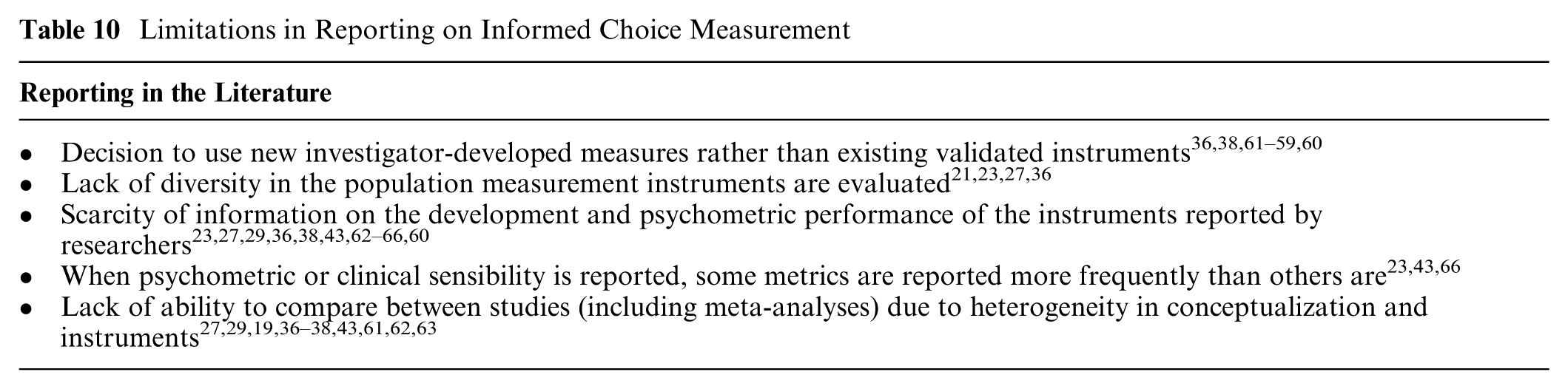
In addition to the challenges in measuring informed choice, there are those relating to its reporting in research. Table 10 summarizes the common limitations identified when reporting on informed choice measurement. The most common included the decision by investigators to use newly developed measures rather than existing validated instruments (10/16 reviews) and, related to this, the lack of ability to compare between studies due to heterogeneity (10/16).
Limitations in Reporting on Informed Choice Measurement
Characteristics of Common Measurement Instruments
Identifying common measures was challenging due to the heterogeneity in how reviews presented and assessed measurement instruments, with some reviews listing only 1 instrument per study21,37 and others not naming specific instruments.36,60 Tables 11 and 12 highlight the most common measures reviews identified and their features. Psychometric properties were supplemented by additional sources.
Key Features of Common Measurement Instruments Identified in Systematic Reviews
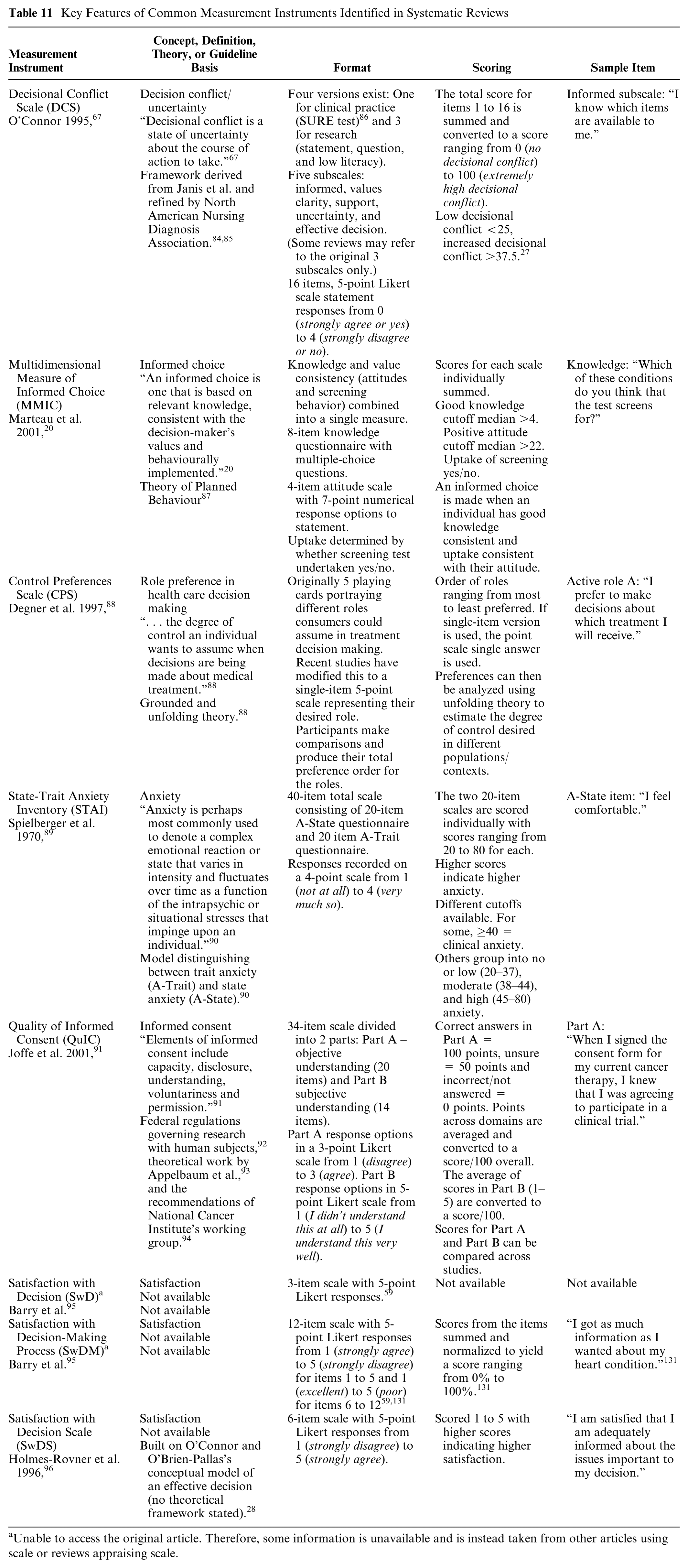
Unable to access the original article. Therefore, some information is unavailable and is instead taken from other articles using scale or reviews appraising scale.
Psychometric Properties and Clinical Sensibilities of Common Measurement Instruments Identified in Systematic Reviews
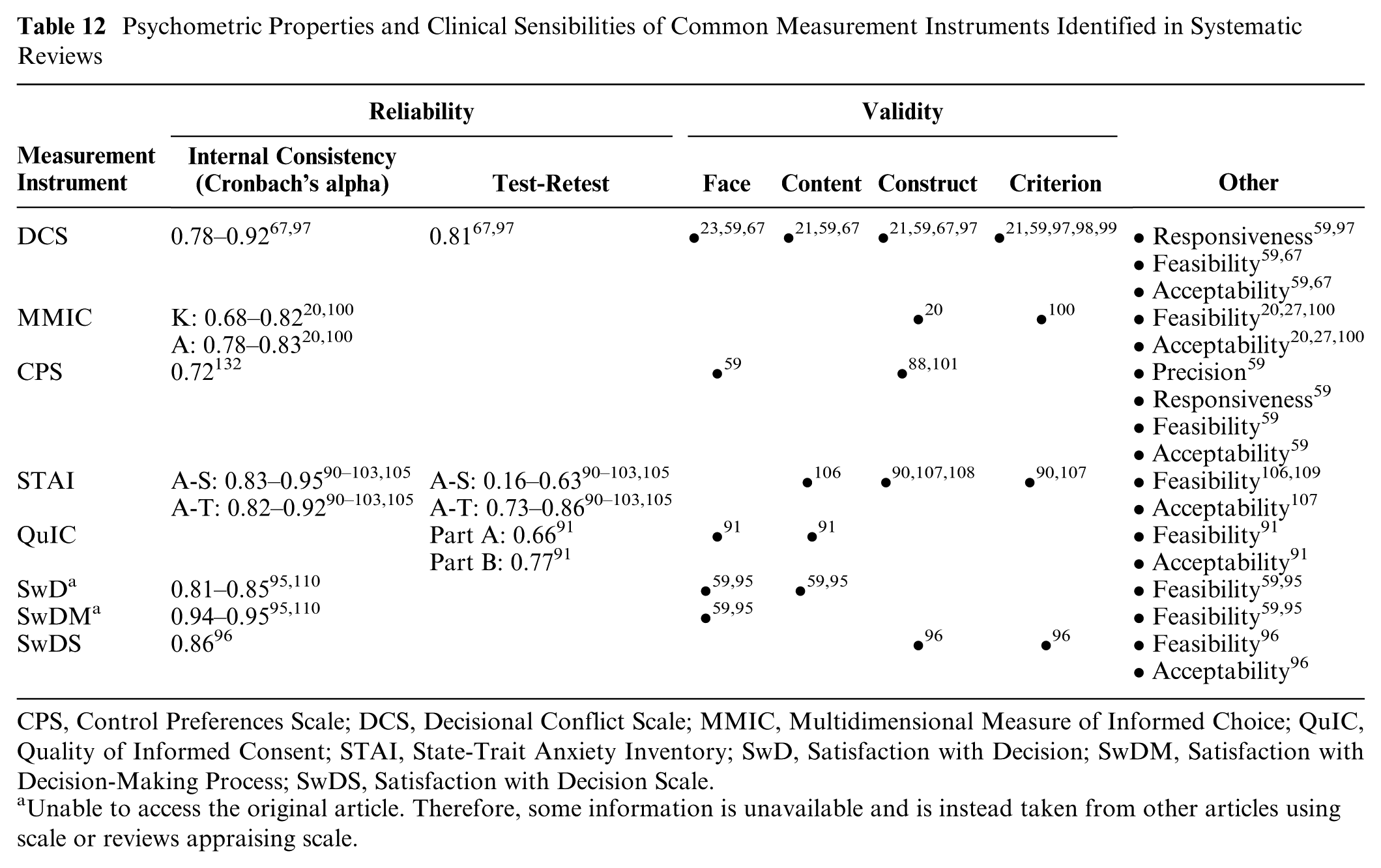
CPS, Control Preferences Scale; DCS, Decisional Conflict Scale; MMIC, Multidimensional Measure of Informed Choice; QuIC, Quality of Informed Consent; STAI, State-Trait Anxiety Inventory; SwD, Satisfaction with Decision; SwDM, Satisfaction with Decision-Making Process; SwDS, Satisfaction with Decision Scale.
Unable to access the original article. Therefore, some information is unavailable and is instead taken from other articles using scale or reviews appraising scale.
Decisional Conflict Scale (DCS) 67
The DCS by O’Connor et al.67,97 was discussed most frequently across reviews21,23,28,19,43,59,66 and measures an individual’s uncertainty in decision making. 67 Of the 4 existing versions, the statement format is the most commonly used in health care studies. 97 The DCS was the most common validated measure in 4 reviews19,43,59,66 and the second most common in a fifth. 27 Notably, the DCS was used as a measure of the decision process in more than 50% of studies in 2 reviews.43,66 As Table 12 demonstrates, there is a general agreement and evidence toward multiple facets of validity and other psychometric properties for the DCS, although occasional discrepancies do exist. For example, although Sepucha et al. 43 found 15% of their studies reported on precision/accuracy, precision was the only area in which no data were available in the studies included in Kryworuchko et al.’s review. 59
Multidimensional Measure of Informed Choice (MMIC) 20
The MMIC by Marteau et al. 20 was the second most highlighted review measure.27,43,62,63 They adapted O’Connor et al.’s effective decision to define informed choice after suggesting that existing measures were not multidimensional, usually only assessing knowledge.20,28 Less widely validated than the DCS, as evidenced in Table 12, the MMIC was the most used measure in Ames et al.’s reproductive screening review in 17 of 33 studies. 27 This review also thoroughly discussed the measure’s performance, with criticism including the dichotomization of knowledge and attitude scales relying on a cutoff, of which there are varying standards (e.g., for “good” knowledge). 27 Additionally highlighted was the risk of oversimplification of choice through the use of binary variables and the lack of cognitive processes (e.g. deliberation included). 27
Control Preferences Scale (CPS) 88
The CPS by Degner et al. 88 aims to measure health care consumers’ desired level of control and was conceived during a period when evidence showed better outcomes for those involved in their treatment decisions. Reviews highlighted its popular use as a decision process measure and in evaluating role preference.23,66 One review specifically by Kryworuchko et al. 59 found that although used in only 2 of 35 studies, it psychometrically scored the second highest after the DCS, as reflected in Table 12, and was particularly praised for its feasibility in subsequent studies. 59
State-Trait Anxiety Inventory (STAI) 90
First conceptualized in the 1960s by Spielberger et al., the STAI is based on a model distinguishing between state anxiety, a transitory emotional response to perceived dangers (A-State), and trait anxiety, a stable disposition to respond anxiously to threats (A-Trait).90–103 The test–retest reliability values in Table 12 reflect A-State transience and are expectedly lower than A-Trait.102,103 Despite the debate on its utility,39,111 anxiety is commonly measured as a decision aid outcome reflecting the process or post–decision outcomes.23,31,42,104 Reference to its use by included studies was noted by multiple reviews, but it received minimal discussion,23,19,64 with Table 12 evidence an example supported by additional literature.90–103,105–109
Quality of Informed Consent (QuIC) 91
The QuIC questionnaire by Joffe et al. 91 was developed to standardize consent evaluation and measures actual (objective) and perceived (subjective) understanding. The QuIC was featured in 3 reviews,37,38,61 although it was the most common measure in only one. 61 It was particularly highlighted by Gillies et al. 37 for assessing 4 of 5 domains of understanding in informed consent (content validity) and praised by Montalvo et al. 61 and Sand et al. 38 for its described development and validation compared with other instruments.
Satisfaction Measures95–96
Satisfaction and decision regret scales measure decision outcomes through the hypothesis that informed decisions may increase satisfaction/decrease regret. 27 Six reviews discussed satisfaction with the decision or decision-making process.23,27,19,61,59,64 Although other validated scales were mentioned,112,113 3 were highlighted as used in subsequent papers following their initial development: Barry et al.’s Satisfaction with Decision (SwD), 95 Barry et al.’s Satisfaction with Decision-Making Process (SwDM), 95 and the Holmes-Rovner et al. Satisfaction with Decision Scale (SwDS). 96
The SwD and SwDM scales feature across 4 reviews.23,27,19,59 The SwD assesses whether the right choice was made and satisfaction with the decision and rates the decision itself.59,95 The SwDM covers questions assessing information adequacy, support, and role satisfaction.59,95 Kryworuchko et al.’s 59 review specifically appraised them, with both scoring positively for reliability, validity, and feasibility and the SwDM additionally scoring for responsiveness and interpretability. Holmes-Rovner et al.’s SwDS featured in trials in 4 reviews.23,19,61,64 Although its validity was acknowledged,23,64 the relevance of this measure in easily reversible decisions as opposed to more permanent decisions has been questioned. 23
Discussion
Key Findings
Informed choice has become increasingly prominent in health care.1–5,40 Despite the spotlight and interventions strategized to improve it,40,42 this review highlights the persisting challenges in the operationalization and measurement of informed choice.
Difficulties in Conceptualizing Informed Choice and Associated Concepts
Systematic reviews used varying terminology and definitions, reinforcing confusion and heterogeneity. While most reviews analyzing the same concept (e.g., informed consent) aligned broadly, no 2 definitions matched.
Informed consent definitions emphasized information provision, capacity, and voluntariness, reflected in the domains given in Table 7.36–38,61,64,60,82 Such an agreement likely reflects the strong ethical and legal foundations of informed consent shaped by Beauchamp and Childress and the WMA statements.1,6,32 Yet, alternative interpretations persist, such as Raper et al.’s distinct diagnostic approach, 64 contributing to ongoing variation.
Similarly, although informed choice, informed decision making, effective decision, and decision quality and process are often considered as separate concepts, Tables 6, 8, and 9 highlight their commonalities.23,27,29,19,43,62–63 For example, O’Connor et al.’s definition of effective decision—centered on information and value congruence 28 —appeared across other terms.15,20,27–31 These overlaps suggest potential for conceptual bridging, as reflected in shared domains in Table 8.
Lack of Theory and PPI Underlying Measurement Instrument Development
Reviews noted the lack of theory and PPI in developing measures, raising concerns about the instruments’ validity. 37 Many decision-making theories, such as normative, descriptive, and prescriptive theories, exist, 31 guiding instrument development and reducing confusion surrounding concepts. 63 The most commonly used and validated instruments highlighted in Tables 11 and 12 were explicit in their theory, for example, the MMIC (theory of planned behavior,20,87 or the CPS (grounded and unfolding theories). 88
Heterogeneity and Lack of Standardization in Instruments
Measurement heterogeneity is the biggest challenge, noted in 12 systematic reviews, v resulting in limited comparability across studies and a lack of meta-analyses. vi The use of standardized instruments and adherence to consistent guidelines, such as those mentioned in the introduction, is encouraged. vii Only 1 review, by Gillies et al., 37 followed COSMIN’s protocols,44,45,114 whereas 4 used IPDAS criteria.29,43,59,66 Despite available guidelines such as the ELICIT core outcome set developed by the authors of 1 included systematic review,37,48 this umbrella review highlights these ongoing measurement inconsistencies.
Decision to Use Investigator-Developed Instruments and Inconsistent Instrument Validation
Researchers often chose unique, investigator-developed instruments,36,38,61–59,60 frequently lacking details on their development or validation, viii rather than using preexisting scales. ix Even the reporting of validated tools varies.23,43,66 Journal word limits may restrict details, although supplementary materials can alleviate this. 43
Characteristics of Measurement Instruments
The DCS, MMIC, CPS, STAI, QuIC, and satisfaction measures were among the most frequently used and well-appraised tools, with many having gained seminal status.67,88,90 These instruments are theory or framework based with varying psychometric properties, with some measuring entire concepts (e.g., MMIC or QuIC),20,91 while others focus on specific domains or subconcepts.18,41,67,88,95–96 To fully assess informed choice, multiple instruments are often needed. 21 Even multidimensional tools such as the MMIC do not cover aspects like anxiety, regret, or satisfaction, 20 although the utility of measuring some of these remains undetermined.39,40
Recommendation Summary for Researchers
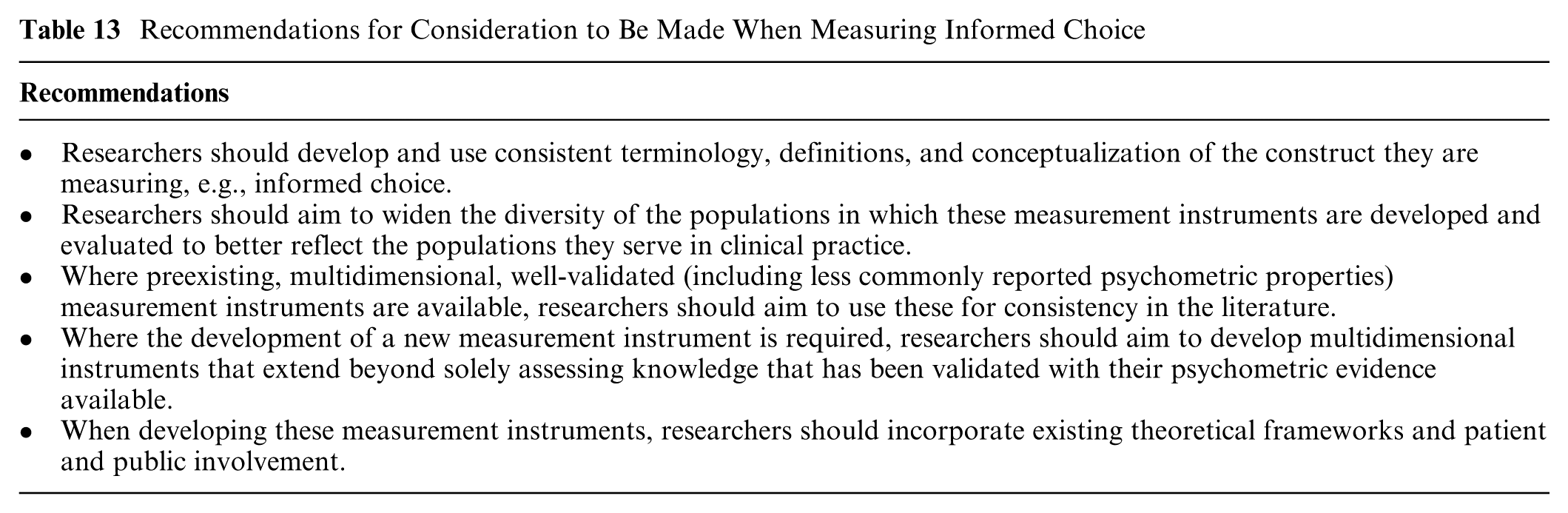
Table 13 summarizes the recommendations for researchers measuring informed choice in the future. While researchers will primarily be responsible for implementing these, the wider scientific community also has an important role. For example, in their critical appraisal, reviewers should consider whether measurement instruments have been validated with available results. Editors can consider population diversity across studies they are publishing, and organizations such as IPDAS should continue to provide up-to-date evidence-based guidance for researchers to access. 78
Recommendations for Consideration to Be Made When Measuring Informed Choice
Strengths
To our knowledge, this is the first umbrella review evaluating the operationalization and measurement of informed choice in health care, presenting a concise summary for health professionals, researchers, and policy makers. The methods and tools used follow Joanna Briggs Institute (JBI) and Cochrane recommendations, with a protocol available on Prospero to maintain transparency. A comprehensive search strategy in consultation with specialist librarians was performed, and study selection, appraisal, and data extraction were conducted in duplicate in alignment with guidelines. 115 The ROBIS critical appraisal allows for the interpretation of results accordingly, and despite the potential bias identified through this, the highest evidence available has informed findings.
Limitations
Despite following JBI, Cochrane, and PRIOR guidelines,50,52,53 limitations remain. Informed choice is defined in varied ways,27,19,36,38,61,62,60 complicating the search strategy. Terms were chosen after scoping and consultation but may not cover all indexing variations. The search was conducted only once, and to comply with PRIOR recommendations, 53 only systematic reviews were included, meaning other review types that may have contained relevant data were excluded. Reviews were limited to adult populations with presumed competency in decision making from a patient perspective to enable comparison between reviews. The measurement of informed choice in other populations or from a professional or observer perspective is an important research question that this review cannot answer.
Conceptual overlaps, such as informed consent or informed decision making, added complexity.11,15,20,27,38 Eligibility criteria were carefully defined and justified under the methods section, although the inability to include possibly relatable concepts is recognized as a limitation. The ROBIS appraisal identified many reviews as high risk for bias, limiting confidence in conclusions. Despite these limitations, including all reviews regardless of their appraisal score appears to be the most appropriate method, where the purpose was to summarize the available evidence. Aside from not performing a risk-of-bias assessment themselves, most reviews otherwise scored well in the phase 2 questions. Furthermore, as one review discussed, the purpose was to assess methods (measurement instruments) rather than outcomes. 63 If anything, this quality appraisal presents where improvements in the literature are required.
Limitations also arose from using tools designed for quantitative, interventional trials, necessitating flexibility with guidelines, including SPIDER and PRIOR.53,116 Given the heterogeneity of the included reviews, meta-analysis was not possible, with the conclusions drawn limited to those from narrative synthesis. This reflected the challenge faced by most of the included systematic reviews, with only 2 performing meta-analyses36,62 and others citing similar reasons for not doing so.21,27,19,61,63,64
Bridging the Gap for the Future
This umbrella review examined how informed choice is measured in health care, highlighting challenges that require further research. Core outcome sets and guidelines, such as COSMIN, aim to streamline this process.44,45,48,49,114 Meanwhile, this review also reveals gaps that can be bridged across concepts and stakeholders—researchers, health care professionals, and policy makers alike.
Conceptual similarities are clear: knowledge is measured almost universally, and recommendations such as PPI in measure development and psychometric testing apply across concepts. While they may have originated in different contexts and diverged in their integration and acceptance into health care, there are examples of how advances in one area can inform another. For example, informed consent is a cemented concept in health care contexts such as surgery or clinical trials.1–3 Its importance is exemplified in research falling under the United States Food & Drug Administration guidelines 117 and the UK General Medical Council Consent guidelines for practitioners. 118 Conversely, in screening, the focus has only recently shifted from promoting uptake to informed choice.15,119–122 This change is reflected in the updated UK National Screening Committee guidance, 5 in which many informed consent studies are cited, reflecting the influence of the informed consent literature on the program’s quality assurance evaluation. 123
This review bridges research and practice, highlighting the relevance of findings beyond academia to other stakeholders. For policy makers, informed choice requires clear measurement and evaluation strategies. With limited resources 9 and RCTs often unfeasible,124–126 efficient approaches using practice-based or policy-driven evidence are needed.124–126 Despite limitations in evidence quality, this umbrella review can be used by policy makers for practice. Health care professionals play a key role in facilitating informed choice at the clinical interface, and a familiarity with these concepts and measures supports reflection on clinical interactions. Presenting exemplar instruments offers a foundation for understanding perspectives and selecting the most appropriate tools.
Although improvements continue, what tools are currently accessible to users? The MMIC appears most suitable for measuring informed choice, assessing both knowledge and value congruence. Alternatively, combining the knowledge questionnaire, DCS, and the 4 MMIC value items enables the evaluation of decision quality and process. Promising tools include the Amsterdam Informed Decision-Making Scale, recently presented as a preliminary conference poster, which incorporates individual information needs and decision processes informed by theory and PPI. 127
In clinical trials, key informed consent domains in competent patients include information provision, comprehension, and voluntariness.1,2,6,21,48,64,69–76 The QuIC instrument is well-regarded with supporting validity evidence.37,38,61 Alternatively, the Brief Informed Consent Evaluation Protocol (BICEP) is a multidimensional, validated measure that includes open-ended questions and satisfaction assessment. 128 Other suitable domains or instruments likely exist beyond those identified in this review.
Conclusion
This review emphasizes that although informed choice is crucial in health care, its measurement and operationalization remain debated. A first step is achieving consistent definitions of informed choice and related concepts. Following this, using standardized, validated, multidimensional instruments informed by theory and PPI in diverse populations is recommended. Available examples include the DCS, MMIC, and QuIC. While these future steps undergo implementation, this review provides a unified piece of work for health professionals, researchers, and policy makers to access to understand the different components of these concepts and choose the best-suited measurement instrument.
Supplemental Material
sj-docx-1-mdm-10.1177_0272989X251413276 – Supplemental material for Operationalizing and Measuring Informed Choice in Health Care: An Umbrella Review
Supplemental material, sj-docx-1-mdm-10.1177_0272989X251413276 for Operationalizing and Measuring Informed Choice in Health Care: An Umbrella Review by Holly Sprosen, Chiara Re, Grant D. Stewart and Juliet A. Usher-Smith in Medical Decision Making
Footnotes
Acknowledgements
The authors acknowledge the advice and feedback of Dr. Kate Garrott at the University of Cambridge during this research process. Further acknowledged is the assistance and expertise of Dr. Veronica Phillips and Senior Fellow Isla Kuhn as medical librarians at the University of Cambridge during the literature search.
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GDS has received educational grants from AstraZeneca, consultancy fees from Evinova, and travel expenses from MSD; he is clinical lead (urology) for the National Kidney Cancer Audit and Topic Advisor for the NICE kidney cancer guideline. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided in part by a grant from the Yvonne A Smith Charitable Trust Scholarship. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. The research was conducted at the University of Cambridge, Cambridge, UK.
Ethical Considerations
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability
All relevant data are contained within the article, or within previously published articles, and appendices.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.