
Abstract
Background
Research suggests that the method used to determine voluntary consent (i.e., opt-in versus opt-out policies) greatly affects the number of registered organ donors in various countries. Although the concept of organ transplantation is broadly supported, the relatively low percentage of registered donors in opt-in countries is puzzling. We suggest that deviating from the status quo (such as signing an organ donor card in opt-in countries or removing oneself from the list of registered donors in opt-out countries) heightens one’s sense of vulnerability.
Design
We examined our prediction in 2 online experiments involving participants from the United States (studies 1 and 2), which has an opt-in organ-donation policy, and from the United Kingdom (study 2), a country that has recently changed its policy to opt out.
Results
In study 1, registered organ donors perceived their vulnerability as greater after being reminded of their decision, but vulnerability perceptions were not affected by such a reminder among nondonors who upheld the status quo. In study 2, imagining oneself making an organ donation decision that deviates from the status quo (signing a commitment under an opt-in policy or removing oneself from the registered donors list under an opt-out policy) increased participants’ perceived personal vulnerability.
Conclusions
The decision to become an organ donor may affect individuals’ sense of physical vulnerability, depending on their country’s donation policy. Potentially, deviating from the status quo may curtail willingness for organ donation. Understanding the psychological barriers to organ donation may help overcome them by presenting the issue in a manner that takes such perceptions into account. We recommend future research to explore whether this heightened sense of vulnerability potentially deters organ donation in opt-in countries.
Highlights
The decision to become an organ donor may affect individuals’ sense of physical vulnerability, depending on their country’s donation policy (opt in versus opt out).
Registered organ donors perceived their vulnerability as greater after being reminded of their decision, but vulnerability perceptions were not affected by such a reminder among nondonors who upheld the status quo.
Imagining oneself making an organ donation decision that deviates from the status quo (signing a commitment under an opt-in policy or removing oneself from the registered donors list under an opt-out policy) increased participants’ perceived personal vulnerability.
Future research is needed to examine whether this heightened sense of vulnerability affects actual organ donation decisions.
Despite the increase in the number of lifesaving organ transplants in recent decades, most countries continue to suffer from a severe shortage of organs for transplant from deceased donors. Research suggests that the percentage of people who choose to become potential organ donors (ODs) varies widely from one country to the next—in line with the method used to determine voluntary consent. Specifically, in countries with an “opt-out” policy (i.e., where anyone who has not expressly refused to donate is considered a donor), consent rates were about 70%, whereas in countries with an “opt-in” policy (where only those who have given explicit consent are donors), only 10% to 40% of the population voluntarily signed up as donors. 1
In recent years, many countries have implemented strategic public awareness campaigns and policy changes to increase donor registration rates, contributing to an overall rise in these figures. For instance, in recent years, the United States has seen an increase in registration among the adult population, now estimated at approximately 58%. 2 However, the gap between opt-in and opt-out countries remains significant. Countries such as Austria maintain a consent rate of nearly 99% due to their opt-out system,3,4 while countries such as Germany, with an opt-in system, have much lower rates—around 30% registered. 5 The gap between organ donation registration rates in Germany and Austria is noteworthy, considering their geographical proximity, cultural similarities, similar health care systems, and demographic characteristics, thus highlighting the importance of the policy used to determine voluntary consent.1,6
Since most people are broadly supportive of the concept of organ transplantation, the relatively low percentage of registered donors in opt-in countries is puzzling. For example, the majority of Americans (95%) are in favor of organ donation, but only 58% are actually registered. 2 This discrepancy occurs, at least in part, because the action of registering as a potential OD is perceived as being significantly more substantial in an opt-in regime than in an opt-out one. 6 This research approach is in line with previous work that highlights the roles of affect in health communication and in the formation of health preferences.7,8
In the present study, we suggest that deviating from the status quo (such as signing an OD card in opt-in countries or removing oneself from the list of registered donors in opt-out countries) heightens one’s sense of vulnerability and recommend future research to examine whether this heightened sense of vulnerability affects organ donation decisions. Research has shown that actions that diverge from the default are perceived as more active choices, whose outcomes are judged to be worse than the outcomes of omissions 9 and tend to lead to greater regret than inactions do. 10
Research on monetary donations suggests that turning down an appeal for a donation may increase people’s perceived vulnerability—for fear that doing so might make it more likely for them to fall victim to the same plight (albeit not to other, unrelated, misfortunes). 11 This tendency is especially pronounced among people with a strong belief in a just world (BJW), who tend to believe in a direct association between one’s actions and one’s fate, 12 which speaks to the intuitive nature of the effect.
Vulnerability is generally defined as the potential for harm or loss of life. It can refer to an individual’s susceptibility to harm and potential losses, 13 or it can describe the risk of having insufficient capacity to manage harm and its consequences. 14 The term perceived vulnerability refers to one’s belief about the likelihood of experiencing a negative event or condition, such as illness or harm. It plays a significant role in health psychology and risk perception, affecting people’s protective motivation 15 and their willingness to take preventive actions. 16 Perceived vulnerability, although potentially informed by factual data, is often skewed by nonrational processes such as heuristics and emotional reactions, which can lead to discrepancies between perceived and actual risk levels. 17 Specifically, intuitive “magical thinking” may create a link between certain behaviors and perceived vulnerability. For example, people tend to feel more vulnerable to misfortune when they are uninsured compared with when they have purchased insurance, even though the insurance does not actually affect the likelihood of the misfortune occurring. 18 Likewise, people have the intuition that actions that tempt fate increase the likelihood of negative outcomes. For example, wearing a shirt from a prestigious university may decrease the perceived probability of being accepted to study there. Such biased vulnerability perceptions also play a role in the context of prosocial decisions.11,19
In light of that line of research, we surmised that the decision to become an OD (or not) may affect a person’s perceived physical vulnerability in general and in particular their perceived vulnerability to needing an organ donation in the future, depending on the organ-donation policy in their own country. Specifically, any deviation from the status quo of the organ donation policy in one’s own country would increase one’s sense of vulnerability to physical harm and, in particular, to one’s own future need for organ transplantation. Accordingly, we hypothesized that in an opt-in regime, signing an organ donation card would increase one’s perceived vulnerability, compared with abiding by the status quo. Conversely, under an opt-out policy, removing oneself from the list of registered donors would increase one’s perceived vulnerability compared with maintaining the status quo.
We examined our prediction in 2 studies i involving participants from the United States (studies 1 and 2), which has an opt-in organ-donation policy, and from the United Kingdom (study 2), a country that has recently changed its policy to opt out. In study 1, we measured participants’ sense of personal vulnerability prior to and after being reminded of their organ donation status. In study 2, we examined participants’ personal vulnerability perceptions in a scenario in which they live in a country with either an opt-in or opt-out policy for organ donations and they have decided to become (or remain) ODs (or not). We then measured their perceived vulnerability.
Based on prior research,11,19 in both studies, vulnerability was measured using 1 item that is directly related to the decision context, namely, one’s perceived chance of needing an organ donation, and 2 other misfortunes that are not directly related to this context: the chance of being severely ill and the chance of being injured in a car accident. Since becoming severely ill and being injured in a car accident may also raise thoughts about organ donation, we conducted a pilot study to ensure that these misfortunes do not spontaneously raise such thoughts among people.
Pilot Study
Method
Seventy-eight Prolific participants, 28 from the United States and 58 from the United Kingdom, 38 women, 39 men, and 1 participant who identified as nonbinary, Mage = 34.77 y (SDage = 12.72 y), completed the survey. Participants were asked to rate the likelihood of becoming seriously ill, being injured in a severe car accident, and needing an organ donation, all within the next 5 y, using a scale from 1 (no chance at all) to 10 (definitely). After evaluating each vulnerability item, participants shared their thoughts following the described misfortune by providing 3 free associations. Subsequently, they rated the extent to which each event prompted considerations of them becoming ODs in the next 5 y on a 10-point agreement scale.
Results from a within-subject analysis of variance (ANOVA) indicated a significant difference in the perceived likelihood of the various misfortunes, F(2, 154) = 46.64, P < 0.001. Perceived vulnerability was significantly lower for needing organ donation (M = 2.23, SD = 1.38) compared with both the chances of becoming seriously ill (M = 3.82, SD = 1.84) and being injured in a car accident (M = 3.63, SD = 1.77). The ratings for the latter 2 perceptions did not significantly differ.
In examining participants’ associations regarding the various misfortunes, we found that thoughts about becoming ill or being injured in a car accident did not generate spontaneous associations with organ donation; none of the participants mentioned the words organ or donation in their responses. However, when considering the possibility of needing an organ transplant, 10 participants included the word organ and 6 mentioned donation in their associations. Ratings of the extent to which each misfortune triggered thoughts about becoming an OD were relatively low for each scenario (for becoming ill, M = 3.64, SD = 2.50; for being injured in a car accident, M = 3.56, SD = 2.40; and for needing an organ donation, M = 3.88, SD = 2.80, all measured on a scale from 1 to 10). These ratings did not significantly differ across the various misfortunes, F(2, 154) = 0.89, P = 0.41. However, it appears that the 3 misfortune events evoke a sense of general vulnerability, as participants used the words death, fear, and anxiety in approximately 30% of their associations following each event: 28 times in the context of illness, 30 times in the context of an accident, and 29 times in the context of organ donation. We believe that these indicators, along with their use in prior research, make the 3 vulnerability items suitable for our study.
Study 1
Previous research suggests that reminding people of their status (such as having insurance or not 18 or acceding to, or refusing, a donation appeal to help contend with a frightening cause 11 ) affects their perception of their own vulnerability. Accordingly, in study 1, we built on that research by examining participants’ perceived vulnerability to needing an organ donation (or incurring other physical harm) twice, namely, before and after being reminded of their OD status (as donors or decliners). We hypothesized that donors and participants who expressed their willingness to become donors while completing the questionnaire (who, unlike nondonors, deviated from the status quo or intended to do so) would feel more vulnerable after being reminded of their proactive decision (time 2) than when they were not reminded of such (time 1). We illustrated the study design and our prediction in Figure 1.
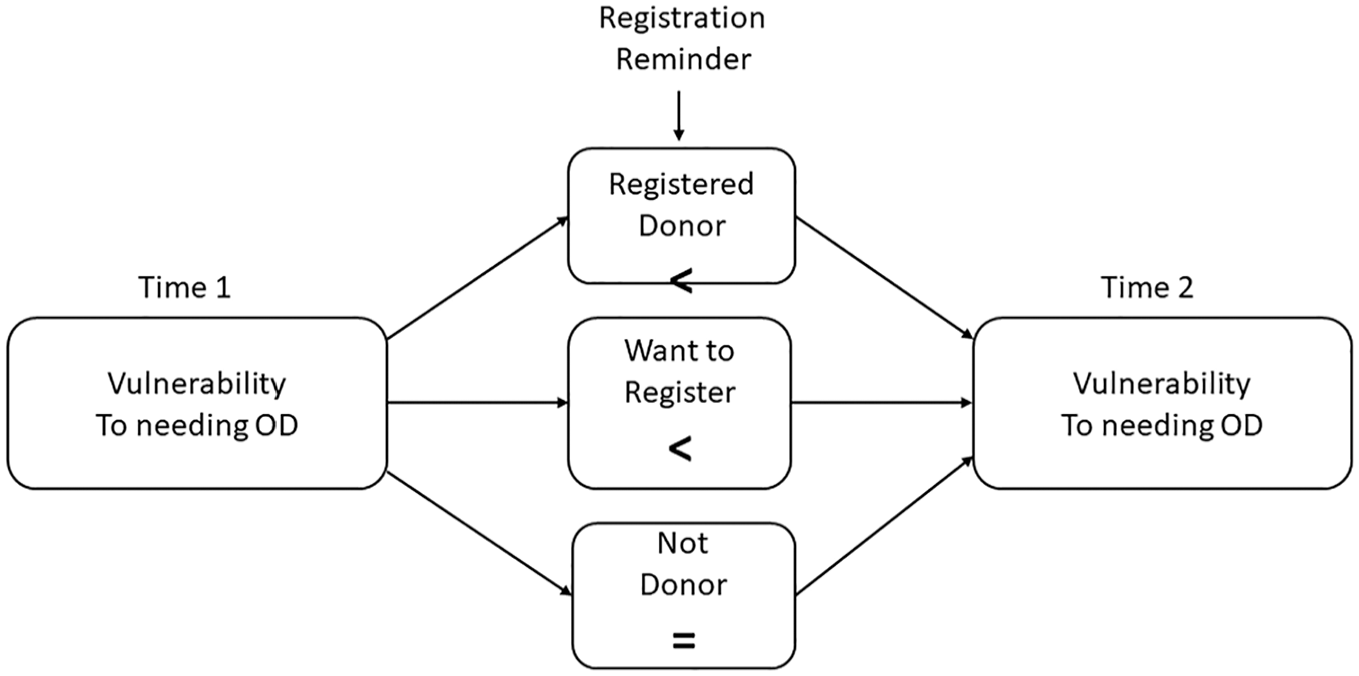
Model of expected changes in perceptions of vulnerability to needing organ donation, based on reminder of registration status: comparing participants who refused to sign (no change in vulnerability) with those who signed or are willing to sign (increased vulnerability).
Method
We used a 2-part longitudinal, within-/between-subjects design. Expecting a 20% to 30% dropout between time 1 and time 2, we targeted a sample of approximately 200 participants. At time 1, 250 Prolific participants from the United States completed an online questionnaire and were paid £0.75 for participation. The questionnaire consisted of demographic questions, followed by 3 items that assessed the participants’ perceived vulnerability—specifically, their chances of needing an organ donation in the next 5 y (main dependent variable (DV)), their chances of falling seriously ill during that time, and their chances of being injured in a road accident during that period—all rated on a scale ranging from 1 (no chance at all) to 10 (definitely). These items are based on previous research on perceptions of vulnerability11,19 and were tested in the pilot study.
At the end of the questionnaire, participants were given an instructional manipulation check (IMC) question, 20 which gauges whether or not they had read the instructions. This question asked the participants to ignore it, thereby providing confirmation that they had indeed read the instructions. 20 Those who correctly answered the IMC question—89.9% of participants—were invited to complete the second part of the survey a week later (time 2; see questionnaire in supplementary material). Finally, participants completed the 8-item BJW for the Self questionnaire 21 to examine whether the previously found link between BJW and prosocial behavior holds in the context of OD registration.
A total of 186 participants (50.0% women, Mage = 34.33 y, SDage = 11.73 y) answered the survey at time 2 and were paid £1.00 each for participation. A sensitivity power analysis conducted in G*Power 22 indicated that given this sample size, with α = 0.05 and power of 0.8, statistical significance would be detected with a small effect size (f = 0.10). At time 2, participants were asked first if they were registered ODs (the reminding manipulation). Specifically, they were asked to indicate which 1 of 3 options applied to them: “I am a registered OD,” “I am not a registered OD but would like to register now,” or “I am not a registered OD and do not want to register.” ii They then answered the same 3 items as at time 1 to assess their perceived vulnerability.
Results
Of the participants, 49.5% reported being registered ODs (n = 92), 17.7% were willing to register (n = 33), and 32.8% refused to do so (n = 61).
Since we had the same hypothesis regarding donors and prospective donors (those who express willingness to sign a commitment), and given the small number of participants who expressed their willingness to sign a commitment, the 2 types of participants were combined for the analysis.
A mixed-model ANOVA—with perceived vulnerability to needing an organ donation at time 1 and at time 2 as a within-subject factor (reflecting the change in these evaluations following the reminding manipulation) and the participant’s OD status as a between-subject factor—revealed a significant main effect of time, F(1, 184) = 5.11, P = 0.025, ηp 2 = 0.03, and an interaction between time and OD status, F(1, 184) = 4.40, P = 0.037, ηp 2 = 0.02. Specifically, overall, participants perceived themselves as being more vulnerable to needing an organ donation when reminded of their OD status (M = 2.21, SE = 0.11, 95% confidence interval [CI] = [2.00, 2.44]) at time 1 and M = 2.44, SE = 0.12, 95% CI = [2.20, 2.68] at time 2). Moreover, as illustrated in Figure 2, in line with our prediction, participants who were not registered ODs, did not deviate from the status quo, and were not interested in registering did not perceive themselves as more vulnerable after being reminded of their OD status (M = 2.23, SE = 0.19, 95% CI = [1.86, 2.60] at time 1 and M = 2.25, SE = 0.20, 95% CI = [1.85, 2.64] at time 2). Conversely, those who were registered ODs, or wanted to register—thus deviating from the status quo—perceived themselves as being more vulnerable after being reminded of their OD status (M = 2.19, SE = 0.13, 95% CI = [1.93, 2.45] at time 1 and M = 2.63, SE = 0.14, 95% CI = [2.36, 2.91] at time 2). iii
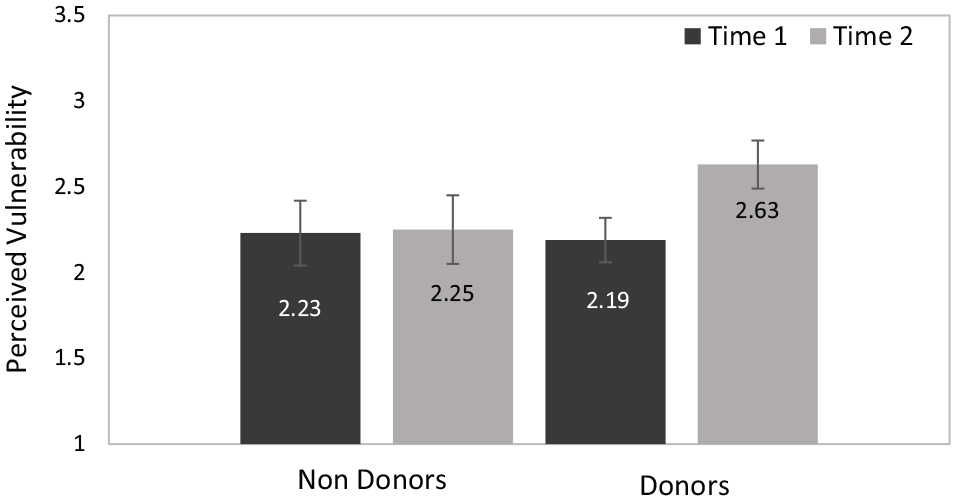
Perceived vulnerability to needing an organ donation (means) before and after the reminder as a function of the participant’s organ donation decision (error bars represent 95% confidence interval).
A mixed-model ANOVA—with perceived vulnerability to falling seriously ill and perceived vulnerability to being injured in a road accident at time 1 and at time 2 as within-subject factors (reflecting the change in those evaluations) and the participant’s OD status as a between-subject factor—did not yield significant results (see Supplementary Material).
Finally, unlike the findings of previous research suggesting a positive link between BJW for the Self and prosocial behavior, BJW did not significantly predict OD registration (Wald = 2.03, P = 0.15, in a binary regression analysis). We will further discuss this finding in the “Discussion” section.
The results of study 1 indicated that individuals perceived themselves as more vulnerable for needing an organ donation after being reminded that they are registered ODs or are willing to become donors. The increase in perceptions of vulnerability is directly related to the unique misfortune of needing an organ donation, pointing to the intuitive nature of this process. This finding is in line with the results of Kogut and Ritov, 11 who found that people who refused a donation request to help women with cancer felt vulnerable to having cancer but not to other misfortunes (see also the general discussion).
While in study 1, we sought to examine people’s sense of vulnerability regarding their actual status quo and organ-donation decision, In study 2, we used hypothetical scenarios to shift the participants’ perception of the status quo by asking them to imagine themselves making organ-donation decisions. This method allowed us to randomly assign people to different policies and registration decisions, controlling for individual differences that may affect actual decisions, such as individual differences in fear of death 23 or in reciprocity tendencies. 24
Study 2
Method
We targeted a conservative small-to-medium effect size (f = 0.20) with a power of 0.80. The power analysis—conducted in G*Power 22 for F tests, of an ANOVA with 2 main effects and an interaction—indicated a required sample size of N = 200 in each country (United States and United Kingdom each, 400 participants in total) to detect a significant effect (α = 0.05). Four hundred one participants on the Prolific platform—201 from the United States and 200 from the United Kingdom (59.1% women, Mage = 37.1 y, SDage = 13.85 y)—were randomly allocated to 1 of 4 experimental conditions of a 2 × 2 (Imagined policy in participant’s country [opt-in/opt-out]×Decision [yes/no]) between-subjects design. Participants were each paid £1.00 for taking part. To avoid any possible external influences, participants in both countries completed the questionnaire on the same day and during the same hours of the day.
Since priming manipulations are sensitive and are not anticipated to have an impact unless directly connected to the subsequent task or assignment, 25 participants were instructed to answer all the questions in sequence and to avoid engaging in other, unrelated activities while participating in the study to make the manipulation effective. A pretest indicated an average completion time of approximately 5 min.
Specifically, participants in the opt-in [opt-out] condition and in the donor [nondonor] condition read: Imagine that you live in a country with an opt-in [opt-out] policy, where citizens are not registered organ donors after death unless they have expressly registered as such [where all citizens are considered potential organ donors unless they expressly decide to opt out]—and you have decided to become [not to be] an organ donor.
Next, participants were asked to rate their perceived vulnerability—specifically, their chances of needing an organ donation in the next 5 y (the main DV), their chances of falling seriously ill during that time, and their chances of being injured in a road accident during that period—on a scale ranging from 1 (no chance at all) to 10 (definitely). Some individuals might fear that being registered as ODs could lead to doctors not making every possible effort to save their lives in an emergency, making them less likely to register as ODs as a result. 26 This fear may serve as an alternative mechanism linking OD agreement and vulnerability. Since in many countries, health care professionals often seek consent from the family before proceeding with organ donation, 27 we asked the participants to assess the likelihood that in the next 5 y, a medical team might ask their close family to donate their organs, on a scale from 1 (no chance at all) to 10 (definitely). Participants then answered questions about their demographics and whether or not they are registered as ODs. Finally, because countries in the United Kingdom only recently changed their OD policy, we asked participants to indicate the policy in their country (opt-in or opt-out; see the questionnaire in supplementary material). Figure 3 illustrates our model predicting vulnerability perceptions according to the manipulated variables in the scenario: policy and decision.
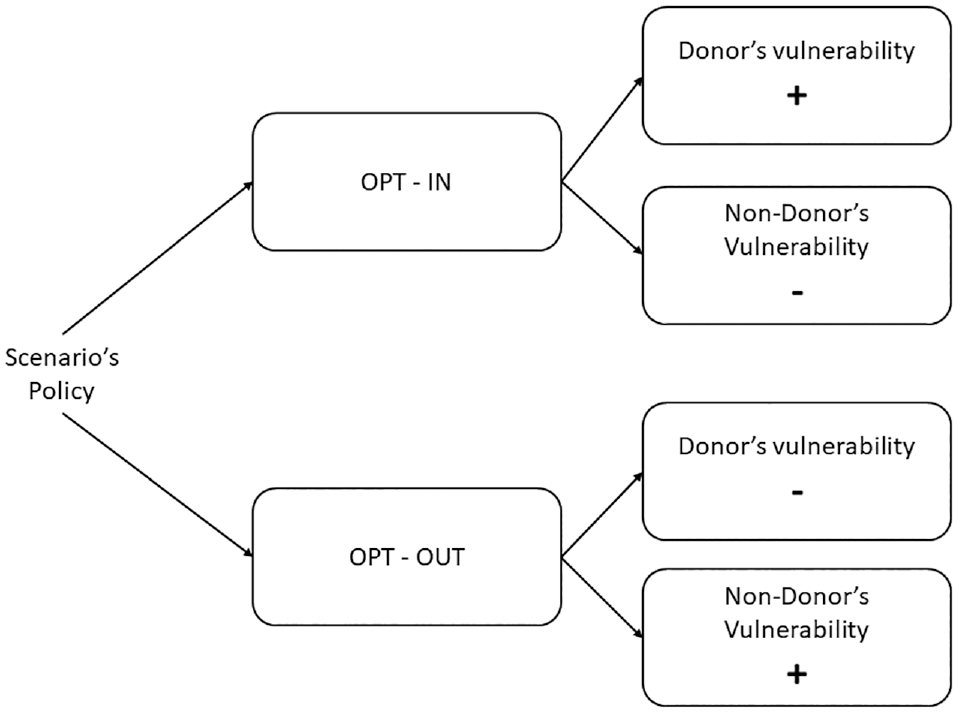
Model of expected perceptions of vulnerability to needing organ donation based on the scenario’s policy (opt-in v. opt-out) and decision (donor v. nondonor).
Results and Discussion
The average completion time was M = 280.59 s, SD = 523.02 s (similar to our pretest). Participants who took more than 600 s to complete the questionnaire (∼5% at the upper-end distribution, suggesting long pauses while answering the questionnaire) were removed from further analysis, since it is likely that they did not remember the manipulation (of whether they live in an opt-in or an opt-out country or whether they were donors when answering the vulnerability questions; for a similar procedure, see Pittarello and Kogut 28 ). This left us with N = 384 participants and an average completion time of M = 228.64 s, SD = 92.90 s. Of these participants, 63.8% reported that they were registered ODs. iv
An ANOVA of the perceived probability of needing an organ donation by the imagined policy in the participant’s country (opt-in/opt-out), their decision in the scenario (donor/nondonor), the participant’s country of residence (United States or United Kingdom), and the participant’s own respective donation status (donor/nondonor) v revealed a significant effect of donation status, such that overall registered donors felt more vulnerable than unregistered ones did (M = 2.75, SE = 0.10, 95% CI = [2.55, 2.94] versus M = 3.12, SE = 0.13, 95% CI = [2.86, 3.38]), F(1, 3.68) = 5.17, P = 0.024, ηp 2 = 0.01. The predicted interaction between the scenario’s decision and policy, F(1, 368) = 4.04, P = 0.045, ηp 2 = 0.01, was also significant. As shown in Figure 4, under an opt-in policy, participants tended to perceive their vulnerability as greater when deviating from the status quo (i.e., choosing to become ODs) than when they upheld the status quo: M = 3.22, SE = 0.16, 95% CI = (2.90, 3.53) versus M = 2.92, SE = 0.14, 95% CI = [2.65, 3.20], F(1, 368) = 2.57, P = 0.11. Similarly, under an opt-out policy (where the status quo is to remain an OD), participants tended to perceive their vulnerability as greater when they decided to remove themselves from the organ donation registry (M = 2.93, SE = 0.21, 95% CI = [2.52, 3.31] v. complying with the default status: M = 2.58, SE = 0.17, 95% CI = [2.52, 2.91]), F(1, 368) = 1.49, P = 0.22. Interestingly, the perceived vulnerability of participants who were assigned to the “not registered” condition was similar under both scenario policies, whereas scenario-registered participants felt much more vulnerable when the scenario decision deviated from the status quo than when it was due to inaction.
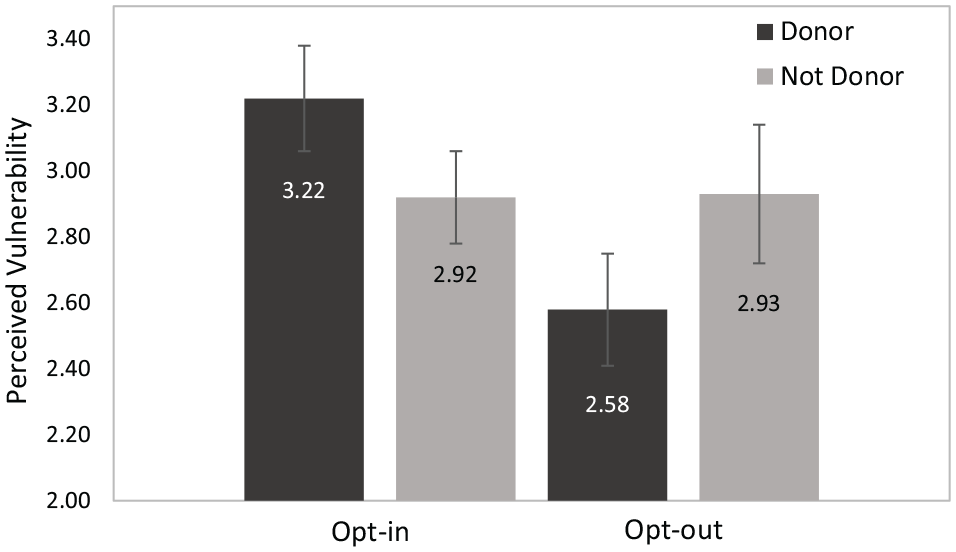
Perceived vulnerability (means) by scenario policy and scenario organ donor decision (error bars represent 95% confidence interval).
Finally, we found a significant 3-way interaction between scenario decision, scenario policy, and the participant’s own donation status, F(1, 368) = 4.12, P = 0.043, ηp 2 = 0.01, suggesting that individuals who are not registered donors were more affected by the experimental manipulations. Among nonregistered ODs, participants who imagined living in a country with an opt-in policy perceived their vulnerability to be greater when deviating from the status quo—that is, when they chose to become ODs—than when they upheld it (M = 3.67, SE = 0.29, 95% CI = [3.10, 4.24] v. M = 3.10, SE = 0.25, 95% CI = [2.61, 3.59]). Similarly, among those who imagined living under an opt-out policy (in which the status quo is to remain an OD), participants perceived their vulnerability to be greater when they decided to opt out of organ donation (M = 3.00, SE = 0.30, 95% CI = [2.41, 3.59] v. M = 2.46, SE = 0.26, 95% CI = [1.95, 2.97]), F(1, 132) = 4.12, P = 0.044, ηp 2 = 0.03. For participants who reported that they were registered ODs, there were no significant differences in perceptions of vulnerability across conditions. As shown in Figure 4, the overall effect (the 2-way interaction) is primarily driven by the sense of vulnerability experienced by subjects who read about being donors, with a high sense of vulnerability reported under the opt-in policy and very low under the opt-out policy. It appears that individuals who are not registered donors were more influenced by the idea of becoming donors—a topic they had likely avoided in the past. It seems that the cause of being a donor (whether through an active or passive decision) significantly affected their sense of vulnerability, more so than for those who are already donors. This finding is consistent with the results of study 1, which indicate that participants who expressed a willingness to become donors during the study reported a particularly heightened sense of vulnerability.
A similar ANOVA of the perceived probability of falling seriously ill revealed a significant 3-way interaction, replicating the pattern described above, F(1, 368) = 3.96, P = 0.047, ηp 2 = 0.01. However, the 2-way interaction was not significant (see Supplementary Material). Ruling out an alternative explanation (that becoming an OD makes it more likely that doctors may be less inclined to fight for one’s life knowing that one is a donor), an ANOVA of the perceived probability of one’s family being asked to donate one’s organs revealed no significant results (see Supplementary Material). No further significant results were found: namely, the interactions between the participant’s country of residence and the other variables were not significant, suggesting that the scenario similarly affected participants in the different countries.
The results of study 2 show that deviating from the status quo heightens people’s sense of vulnerability. When asked to imagine their own organ-donation decision under an opt-in versus an opt-out policy, participants felt more vulnerable to needing an organ donation when they imagined deviating from the status quo than when remaining with it. Moreover, we found that donors feel less vulnerable when their decision is passive (i.e., the status quo) than when it is proactive (deviating from the status quo). This finding is important, as it may help explain previous research that found a disparity between the percentages of registered people under the 2 policies. Importantly, participants who were asked to imagine that they were donors were more affected by the policy manipulation than participants who were assigned to the not-donor condition. This finding is in line with the results of study 1, in which only registered donors were affected by the reminder of their status. We further discuss this pattern in the discussion below.
Discussion
Building on research on “tempting fate” and the omission bias,17,29,30 we predicted and found that deviating from the status quo—by becoming an OD in an opt-in country or withdrawing from the list of registered donors in an opt-out country—heightens individuals’ perceived vulnerability. In study 1, participants reported their perceived vulnerability before and after being reminded of their OD status (whether they were registered as ODs or not). Participants who were registered ODs or were willing to become donors, thereby deviating from the status quo in the United States, perceived their vulnerability to needing an organ donation as higher after being asked about their OD status. However, their perception of other vulnerabilities (e.g., becoming ill) was not affected by the reminder. Conversely, nondonors (who conformed with the status quo) were not affected by the reminder about their OD status, nor did they perceive their vulnerability to needing an organ donation as being greater after stating their OD status.
In study 2, we measured participants’ perceptions of their vulnerability while imagining living in a country that has either an opt-in or an opt-out policy. We found that under an opt-in policy, participants saw themselves as more vulnerable to needing an organ donation when they deviated from the status quo—that is, imagining themselves becoming ODs—than when they upheld it. Similarly, under an opt-out policy in which the status quo is to be an OD, participants perceived themselves as more vulnerable when the decision was to remove themselves from the organ donation registry. We found that participants who were asked to imagine themselves as donors felt significantly more vulnerable to needing an organ donation under the opt-in policy manipulation (compared with an opt-out policy), whereas those who were assigned the nondonor role did not experience such an effect. This pattern, observed in both studies, may be attributed to the concept of mortality salience. When individuals acknowledge their status as registered ODs, it naturally evokes thoughts of mortality, which are less prevalent when considering not being a registered donor. The process of becoming an OD, or even considering this option, highlights mortality and health risks, something less pronounced among nondonors who have not actively engaged with the organ donation decision-making process. 31
When examining vulnerability perceptions, we included questions about the vulnerability to needing an organ donation—a fear directly related to the OD registration decision—as well as other, less related vulnerabilities (i.e., falling severely ill or being injured in a road accident). Our results are consistent with regard to the perceived vulnerability to needing an organ donation, while the general vulnerability revealed weaker, less consistent results. Previous research on monetary donations and perceptions of vulnerability has also yielded mixed results. One study found that refusing a donation appeal increases one’s sense of vulnerability specifically to the plight that the donation was requested for (i.e., cancer)—but not to one’s general sense of vulnerability overall. 11 Conversely, Motsenok et al. 19 found a general positive association between one’s sense of vulnerability and prosocial behavior, such that people with a greater sense of vulnerability exhibited a greater willingness to help in general, and not only in the specific issue at hand. Thus, future research is needed to further explore this issue.
Despite some similarities, our studies join a new line of research that suggests that the mechanisms behind OD decisions may be fundamentally different from those found in other prosocial decisions—such as monetary donations or volunteering.23,31,32 While refusing a monetary donation appeal heightens the respondent’s own perceived vulnerability, 11 with OD decisions (in opt-in countries) it is consent that does so. This is possibly because in monetary donations people perceive the decision to donate as the recommended, socially desired outcome, and therefore their perceived vulnerability is heightened by deviating from it. In addition, while previous research suggests a positive link between BJW for the Self and prosocial behavior, we found no significant association between BJW and OD registration. This may be attributed to the unique psychological mechanisms that influence OD decisions, particularly heightened thoughts about one’s own mortality, 24 which may take precedence over other factors such as BJW in shaping these decisions. Such death-related thoughts are less likely to affect other prosocial behaviors.
Our research has several limitations. First, while we examined how deviating from the status quo predicts a sense of vulnerability, suggesting that such thoughts may inhibit organ donation registration in opt-in countries, this assumption was not directly tested in the current study and warrants further investigation. Previous research indicates that in opt-in countries, many people are reluctant to register as ODs due to a sense of discomfort, often without a rational explanation. 33 Future studies should explore whether this reported discomfort includes an increased sense of vulnerability. In addition, future research should manipulate participants’ sense of vulnerability and examine its direct effect on willingness to commit to organ donation. We assessed participants’ perceived vulnerability following a reminder of their self-reported OD decision or imagining themselves making such a decision. Future studies should explore individuals’ sense of vulnerability while making OD decisions. Lastly, participants were self-selected to participate in the studies as part of their registration to the Prolific platform. Future work could benefit from examining representative samples.
Our research contributes to the decision-making literature on status quo, omission bias, and loss aversion as well as to the broader organ donation literature focusing on the drivers of donation decisions. First, we illustrate that individuals often experience a heightened sense of vulnerability when considering deviations from their current state, which can deter action. This underlying mechanism warrants examination in other decision-making contexts, where it might evoke specific senses of vulnerability relevant to each situation. For instance, in the context of children’s vaccination decisions, parents often feel vulnerable to causing side effects through active choice, even when the probability of side effects is much lower than that of the virus itself. 30
Loss aversion has been proposed as a mechanism underpinning omission bias.9,10 Our research raises the possibility that focusing on potential losses might amplify feelings of vulnerability. Specifically, regarding organ donations, loss aversion may inhibit individuals’ willingness to change their donation status by amplifying fears of losing bodily integrity 30 and concerns over autonomy. 34 Such fears can increase an intuitive sense of vulnerability. However, further research is needed to examine this proposition directly.
Our research offers valuable insights into improving the presentation of organ donation decisions to reduce the sense of vulnerability among registered donors in opt-in countries, which comes with deviating from the status quo. For example, campaigns might focus on highlighting the positive outcomes of organ donation for recipients. By featuring testimonials from recipients or their families, the narrative shifts to generosity and legacy rather than focusing on the potential risks donors might perceive. 31 Moreover, crafting messages that position organ donation as a widely accepted social norm—through peer testimonials or community endorsements—could further enhance this perception. This approach can help mitigate donors’ feelings of vulnerability by making organ donation feel like a common and normative behavior, even if it is not yet the status quo. Research on implicit endorsements suggests that default options convey an implicit recommendation or approval from policy makers or society, influencing individual decisions.35,36 In opt-in countries, people might view nonregistration as the endorsed status, increasing their sense of vulnerability when considering registering. Thus, it is vital for authorities to advocate for registration, emphasizing it as the recommended choice.
Supplemental Material
sj-docx-1-mdm-10.1177_0272989X251346213 – Supplemental material for Organ Donation Decisions: When Deviating from the Status Quo Heightens Perceived Vulnerability
Supplemental material, sj-docx-1-mdm-10.1177_0272989X251346213 for Organ Donation Decisions: When Deviating from the Status Quo Heightens Perceived Vulnerability by Marina Motsenok and Tehila Kogut in Medical Decision Making
Footnotes
Acknowledgements
This work has been presented at the following meetings: The annual meeting of the European Social Cognition Network, ESCON-2022. Milan, Italy, and the annual meeting of the International Association for Conflict Management - IACM 2023, Thessaloniki,. Greece.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Israel Science Foundation (ISF) grant 1426/20. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Authors’ Note
This work was conducted at the School of Education, Ben Gurion University of the Negev.
Ethical Considerations
The studies were approved by the authors’ university Ethics Committee (approval No. 1913-1). All measures, manipulations, and exclusions are reported. The studies were not preregistered but were preplanned and described in detail in a funded research proposal.
Consent to Participate
All participants provided informed consent to participate in the studies.
Consent for Publication
Not applicable.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.