
Abstract

We read with interest the study by Trouiller and Laramée investigating health technology assessment (HTA) decisions made between England and France, 1 demonstrating a discordance in reimbursement outcomes between countries for the same cancer medicines.
The results perhaps reflect key differences in assessment criteria, namely, cost-effectiveness in England and clinical effectiveness in France. In addition to evaluating cost-effectiveness, the English HTA agency, the National Institute for Health and Care Excellence (NICE), also considers 3 distinctive elements that can influence decision making: 1) end of life/severity (end of life was a criterion for assigning more value to treatments for indications with a life expectancy of less than 24 mo; this was replaced in 2022 by a severity modifier, which assigns more value to treatments for severe diseases), 2) innovation (if a technology provides benefits that may not have been captured in cost-effectiveness calculations, it may be given more value) and 3) equality (considerations around inequalities). 2
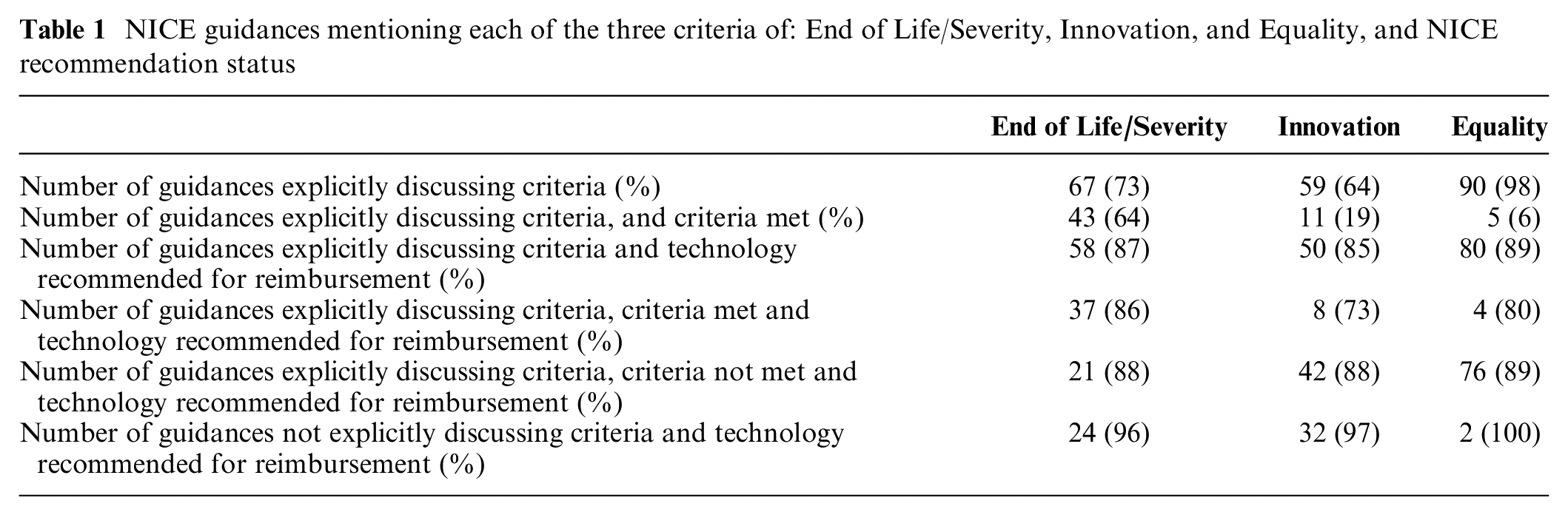
We reviewed assessments made by NICE for oncology products between January 2021 and June 2023 (N = 92 assessments). Technology appraisal guidances were investigated for discussions around the 3 distinctive elements mentioned above as well as the potential impact of these elements on reimbursement decisions. Of the assessments, 27% and 36% were missing any specific discussion around end of life/severity and innovation, respectively. There was no clear relationship between explicitly discussing one of these criteria and/or a treatment meeting one of these criteria and receiving a positive recommendation from NICE (Table 1).
NICE guidances mentioning each of the three criteria of: End of Life/Severity, Innovation, and Equality, and NICE recommendation status
For assessments mentioning that the technology was innovative, we checked whether the French National Authority for Health (Haute Autorité de Santé; HAS), the Canadian Agency for Drugs and Technologies in Health, (CADTH), and the Australian Pharmaceutical Benefits Advisory Committee (PBAC) also mentioned these factors in their assessments, despite these agencies not explicitly calling out innovation as assessment criteria.3–5 There were 5 products assessed in common between NICE and HAS, 6 between NICE and CADTH, and 6 between NICE and PBAC. For the HAS comparison, 1 assessment had the reasons for innovation given by NICE mentioned in transparency committee reports (this medicine was positively recommended compared with 2 of the 4 products having transparency committee reports not mentioning the NICE reasons for innovation). For the CADTH comparison, 4 assessments had the reasons for innovation given by NICE mentioned in reimbursement recommendations (3 of these 4 positively recommended, compared with 2 of the 2 products having reimbursement recommendations not mentioning the NICE reasons for innovation). For the PBAC comparison, 2 assessments had the reasons for innovation given by NICE mentioned in the public summary documents (1 of these 2 positively recommended compared with 2 of the 4 products having public summary documents not mentioning the NICE reasons for innovation).
As noted by others, 6 it is currently not clear how assessment criteria are weighted by HTA bodies and/or whether factors that are not explicitly stated play a role in decision making. Transparency in decision making is important for many stakeholders as learnings can be made from past submissions. Current circumstances are far from optimal given the ultimate consequences for patient access to medicines. Updates to HTA agency processes and proposed collaborations between HTA agencies should make a concerted effort to address this issue.7–9