
Abstract
Background
Professional roles within a hospital system may influence attitudes behind clinical decisions.
Objective
To determine participants’ preferences about clinical decisions that either value equal health care access or efficiency.
Design
Deidentified survey asking participants to choose between offering a low-cost screening test to a whole population (“equal access”) or a more sensitive, expensive test that could be given to only half of the population but resulting in 10% more avoided deaths (“efficient”). Data collection took place from August 18, 2021, to January 24, 2022. Study 1644 was determined to be exempt by Tufts Health Sciences Institutional Review Board (IRB).
Setting
Tufts Medicine Healthcare System.
Participants
Approximately 15,000 hospital employees received an e-mail from the Tufts Medicine Senior Vice President of Academic Integration.
Measurements
Analysis of survey responses with chi-square and 1-sample t tests to determine the proportion who chose each option. Logistic regression models fit to examine relationships between professional role and test choice.
Results
A total of 1,346 participants completed the survey (∼9.0% response rate). Overall, approximately equal percentages of respondents chose the “equal access” (48%) and “efficient” option (52%). However, gender, professional role (categorical), and clinical role (dichotomous) were significantly associated with test choice. For example, among those in nonclinical roles, women were more likely than men to choose equal health care access. In multivariable analyses, having clinical roles was significantly associated with 1.73 times the likelihood of choosing equal access (95% confidence interval = 1.33–2.25).
Limitations
Generalizability concerns and survey question wording limit the study results.
Conclusion
Clinicians were more likely than nonclinicians to choose the equal health care access option, and health care administrators were more likely to choose efficiency. These differing attitudes can affect patient care and health care quality.
Highlights
Divergent preferences of valuing equal health care access and efficiency may be in conflict during clinical decision making.
In this cross-sectional study that included 1,346 participants, approximately equal percentages of respondents chose the “equal access” (48%) and “efficient” option (52%), a nonsignificant difference. However, gender, professional role (categorical), and clinical role (dichotomous) were significantly associated with test choice
Since clinicians were more likely than nonclinicians to choose the equal health care access option and health care administrators were more likely to choose efficiency, these differing attitudes can affect patient care and health care quality.
This is a visual representation of the abstract.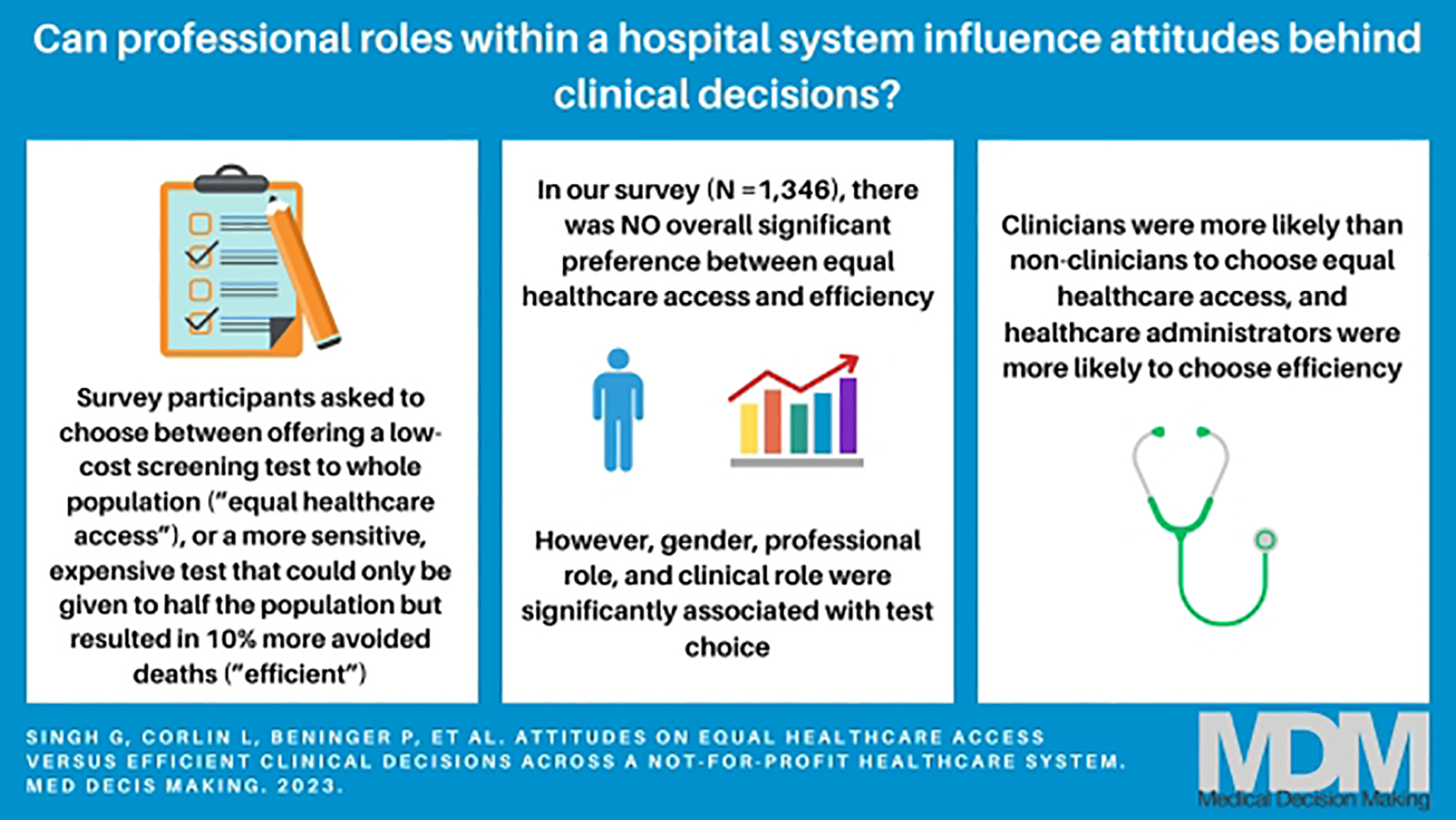
Keywords
Introduction
Health care organizations strive to provide the best possible care for patients. The Centers for Disease Control and Prevention describes health equity as the state in which everyone has a fair and just opportunity to attain their highest level of health. 1 Comparatively, health equality can be described as equal treatment and availability of health care services for all people. 2 Economic and political systems affect people’s access to health care and overall health status. 3 Clinicians are also mindful of being judicious stewards of limited resources, and thus, clinical decisions are likely influenced by a treatment’s effectiveness to diagnose diseases, also known as a test’s sensitivity. With other conditions remaining the same, tests with high sensitivity have a remarkable ability for disease screening and lower risk for false-positive results. 4 When test results are not accurate, they might be more harmful than helpful. In addition, clinicians sometimes must balance a test’s performance against its cost-effectiveness (which reflects tradeoffs involved in spending resources on one strategy to improve health versus another). 5 Many physicians accept cost-effectiveness as an appropriate consideration for clinical decision making, but this criterion is inconsistently applied. 6
The concepts of equity, equal health care access, effectiveness, and cost-effectiveness may be in conflict during clinical decision making. For example, Lane et al. 7 distinguished between maximizing equity for most people versus all people as a key factor in resource allocation. Ubel et al. 8 examined the views of medical decision-making experts, medical ethicists, and prospective jurors (i.e., members of the general public) on cost-effectiveness versus health care equity. Each group was asked to choose between 2 screening tests: 1 that prioritized health care equity and 1 that prioritized cost-effectiveness. Results showed that 41% of medical decision-making experts, 53% of medical ethicists, and 56% of prospective jurors chose the more equitable screening test over the cost-effective option. Similarly, the study by Perneger et al. 9 study in 2002 found that approximately 75% of Swiss physicians favored universal access to the screening test over a different more effective test that had to be selectively rationed to patients.
In 2017, Li et al. 10 expanded on these studies by modifying the participant population and probing for participants’ reasoning for their choice. The researchers found that attending physicians (53%) were more likely to choose the equitable screening option than were physician residents (44%), who were more likely to choose the equitable screening option than medical students (36%). Many participants who chose health equity rejected the cost-effective option, reasoning that it was unfair as it could not be could not be widely distributed and unethical with questions about how half the population could be chosen in an unbiased manner. Similarly, Leep Hunderfund et al. 11 observed that medical students were more cost conscious than physicians were, even among new attending physicians.
In this study, we evaluated clinical decision making regarding a colon cancer screening test with the goal of analyzing equal health care access versus efficiency preferences across an entire hospital system of health care professionals, including clinical and nonclinical personnel, business, and support staff. To our knowledge, such a comprehensive evaluation has not been previously conducted. Learning more about a health care organization’s constituents’ opinions about equal health care access and efficiency is important to inform and optimize organizational decision making and patient care.
Methods
Study Participants
The study population included all personnel within the Tufts Medicine health care system, encompassing Tufts Medical Center (a 415-bed tertiary care center), Melrose Wakefield Hospital (a 234-bed community hospital), Lowell General Hospital (a 390-bed community hospital), and Lawrence Memorial Hospital (a 189-bed community hospital). Approximately 15,000 people (approximately 2,000 physicians) with Tufts Medicine e-mail addresses were sent an e-mail from the senior vice president of academic integration in August 2021 with information describing the optional survey. Data collection took place from August 18, 2021, to January 24, 2022. The de-identified survey was hosted on the platform SurveyMonkey. At the end of the survey, participants could optionally e-mail the survey coordinator with identifiable information to enter a lottery for gift cards from an online e-commerce platform. This study (No. 1644) was determined to be exempt by Tufts Health Sciences Institutional Review Board on May 12, 2021.
Survey
The primary outcome of interest was assessed with a survey question reproduced from Ubel et al.
8
:
A group of doctors was formed to help the government decide which of two tests to offer low-risk people. Test 1 is inexpensive but does not always detect cancers in their early stages. Test 2 is more expensive but is better at detecting early cancers. The decision is complicated by budget limitations: the government has only a certain amount of money available to pay for the screening tests. After evaluating the costs and benefits of each test, the doctors have reached the following conclusions. The budget is just large enough to offer Test 1 to all the low-risk people. With this approach, everyone can receive the test, and 1000 deaths from colon cancer will be prevented. The budget is just large enough to offer Test 2 to half of the low-risk people. With this approach, half of the people can receive the test and half cannot, and 1100 deaths from colon cancer will be prevented. Which test would you administer?
Ubel et al. and Li et al. categorized participants who chose test 1 as prioritizing health equity and participants who chose test 2 as prioritizing cost-effectiveness. In our work, we chose to characterize test 1 as prioritizing equal health care access (i.e., all patients get the same test) and test 2 as prioritizing efficiency (i.e., the test that is cost-effective and produces the best results for patients). 4
Participants were asked to self-report demographic characteristics and their professional role in the hospital system (see Appendix).
Statistical Analysis
We first described the number and proportion of participants who identified with each level of each demographic characteristic (i.e., age, educational attainment, gender, sexual orientation, race/ethnicity, immigration status, political affiliation, professional role, and clinical role). Then, we calculated the proportion of participants who chose each test option (“equal health care access” versus “efficiency”) overall and by each demographic characteristic. We used Pearson chi-square tests to identify the bivariate associations between test preferences and each demographic characteristic. We also calculated 1-sample tests of proportions to determine if the proportion of participants who chose each test preference in each level of each demographic characteristic differed from 50%. In addition, we calculated the proportion and 95% confidence interval (CI) of respondents who chose each test preference and identified in intersecting identities (i.e., clinical role and age group, clinical role and gender, age group and gender).
To examine the associations between clinical role and test preference, we fit logistic regression models with the dependent variable of test option (referent: equal health care access) and primary independent variable of clinical role (referent: nonclinical). The first set of models additionally included 1 other demographic variable: age (18–25/26–35/36–49/50–65/65+ y; note that 65-y-olds could identify in 2 categories, but we assume all 65-y-olds identified in the oldest age group), educational attainment (high school or GED/college/graduate school), gender (male/female), sexual orientation (heterosexual/other/prefer not to answer), race/ethnicity (Asian/Black or African American/Hispanic or Latinx/White/multiple or other/prefer not to answer), immigration status (foreign born/at least 1 parent foreign born/both parents US born/unaware or other or prefer not to answer), or political affiliation (Democrat, Republican, Independent, none of the above, prefer not to answer). Then, we fit a single model with all demographic variables included as covariates. All analyses were performed with Stata v17.
Role of the Funding Source
There was no significant financial support for this work.
Results
A total of 1,346 participants out of approximately 15,000 employees completed the survey in its entirety, leading to a response rate of approximately 9.0%. Sample characteristics are described in Table 1. Most of the participants were between 26 and 65 y of age (83%), had at minimum a college-level education (89%), identified as female (78%), identified as heterosexual (84%), identified as White (75%), were children of 2 parents born in the United States (57%), and had a clinical role in the hospital system (67%). More than one-third of the sample identified as Democrat (37%) and approximately one-third identified as Independent (34%).
Distribution of Sample Characteristics Overall and by Test Choice, and Proportion Who Agree with Each Test Choice within These Demographic Characteristics
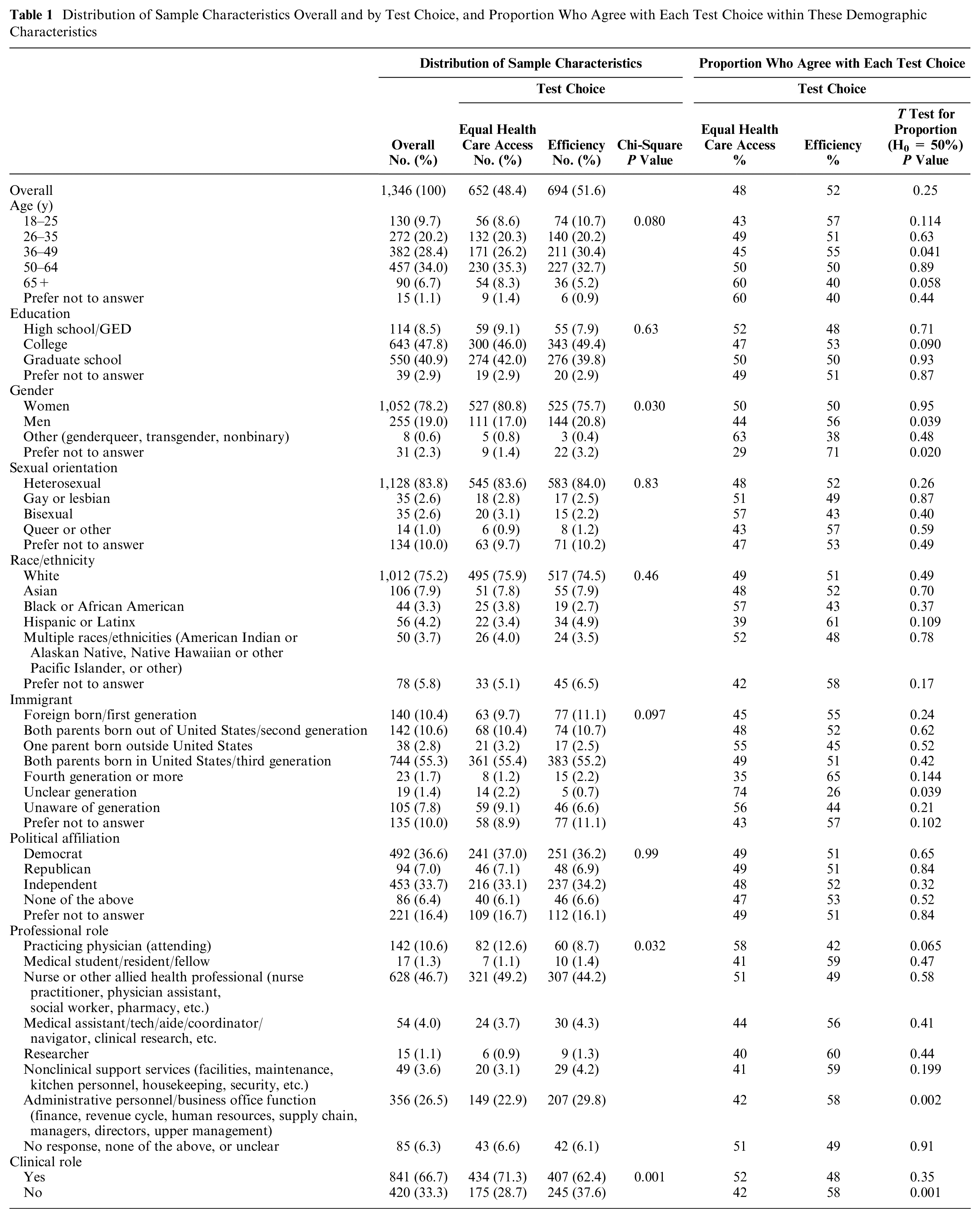
Overall, there was no significant population preference between the equal health care access option and efficiency option (48% v. 52%, P = 0.25; Table 1). However, among males as well as people who preferred not to disclose gender, 36- to 49-y-olds, administrative personnel and those with business office functions, and people with nonclinical professional roles, significantly more people chose the efficiency option (P < 0.05 for each; Table 1). The only group among whom a significantly higher proportion of participants chose the equal health care access option was people whose immigrant generation was unclear (Table 1).
In bivariate analyses, gender, professional role, and clinical role were significantly associated with test choice (Table 1). In addition, there were a few combinations of variables that affected test choice. For example, among people with nonclinical roles and among men, increasing age was generally associated with a higher proportion of agreement with the equal health care access test choice (Figures 1 and 2). Similarly, among those in nonclinical roles, women were more likely than men to choose the equal health care access test (Figure 3).
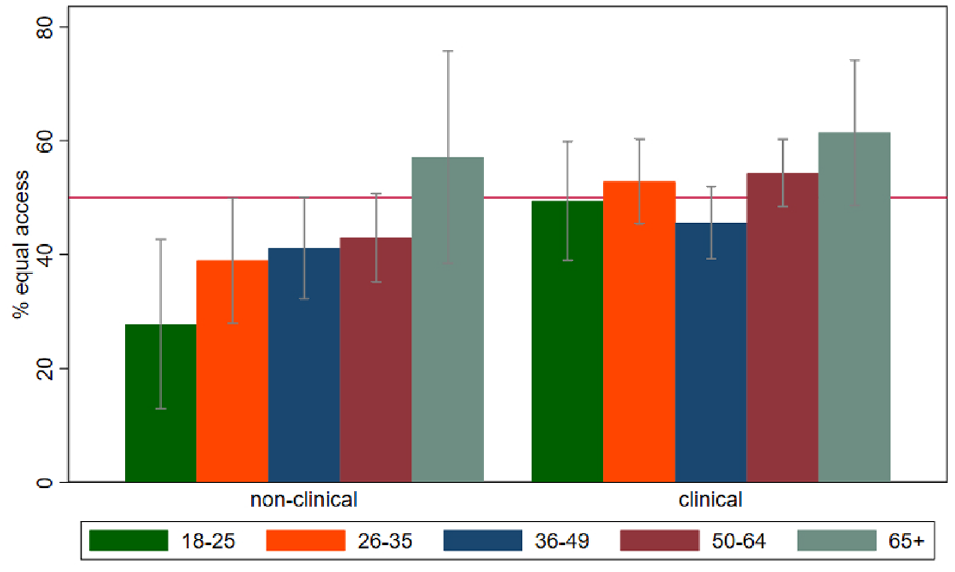
Proportion of people who agree with the equal health care access option stratified by professional role and age group (in years). Red horizontal line = 50%. Gray bars = 95% confidence intervals.
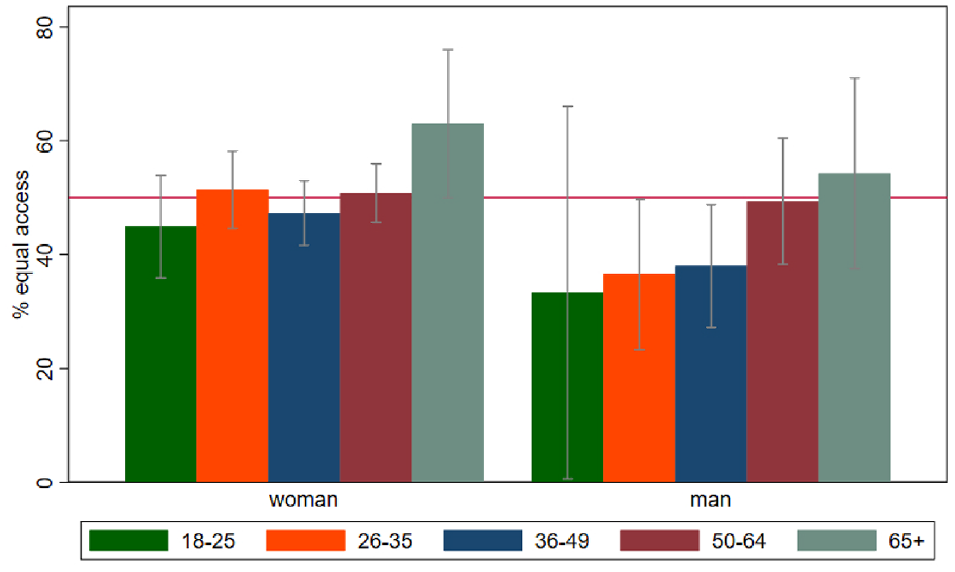
Proportion of people who agree with the equal health care access option stratified by gender and age group (in years). Red horizontal line = 50%. Gray bars = 95% confidence intervals.
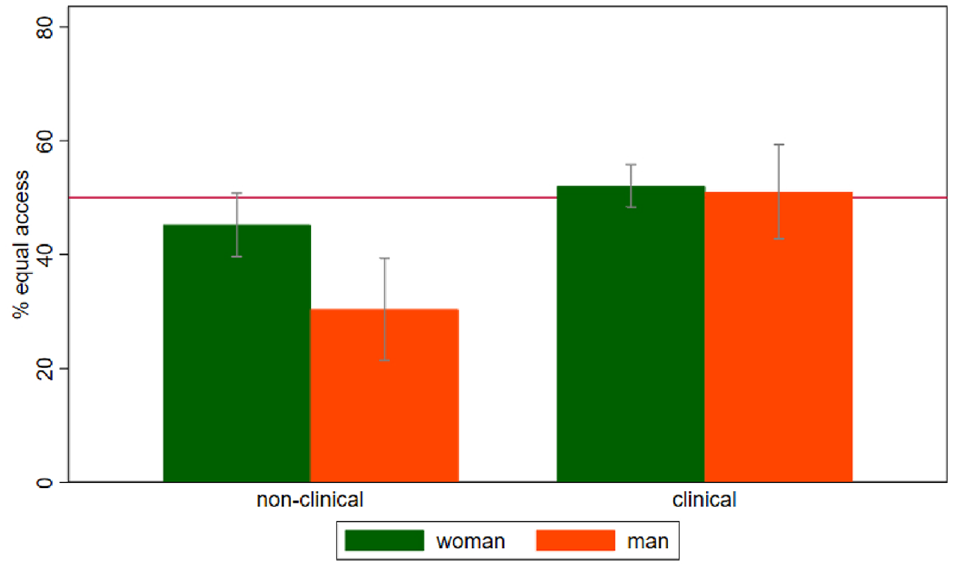
Proportion of people who agree with the equal health care access option stratified by professional role and gender. Red horizontal line = 50%. Gray bars = 95% confidence intervals.
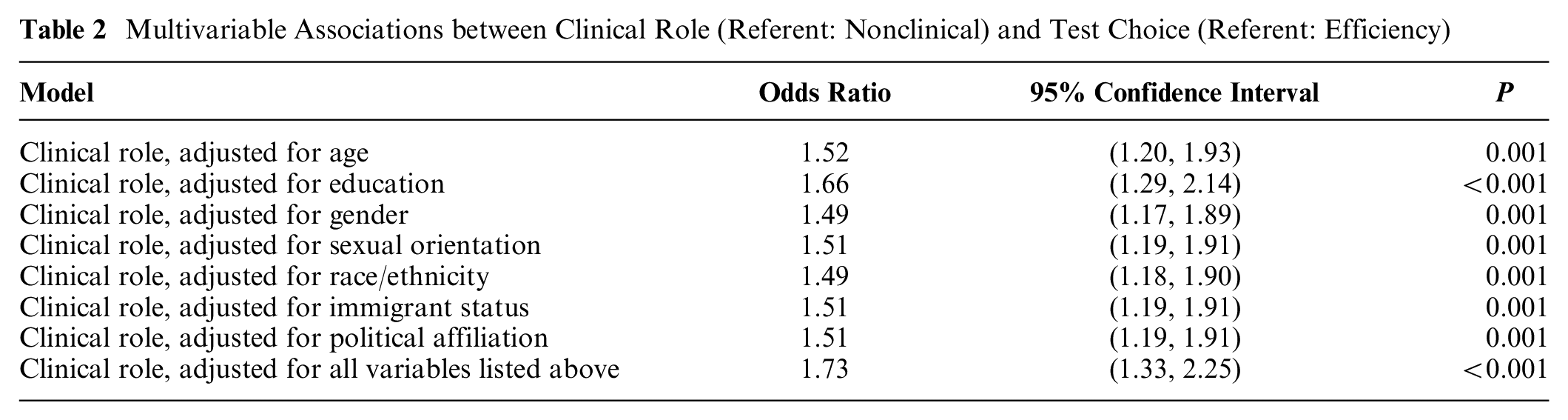
In multivariable analyses, occupying a clinical role was significantly associated with an increased likelihood of choosing the equal health care access test when adjusted for each demographic covariate (both alone and in a model adjusted for all demographic covariates; Table 2). Specifically, in the model adjusted for all covariates, having a clinical role was significantly associated with 1.73 times the odds of choosing the equal health care access test over the efficiency test (95% CI = 1.33, 2.25).
Multivariable Associations between Clinical Role (Referent: Nonclinical) and Test Choice (Referent: Efficiency)
Discussion
We observed no clear overall preference between equal health care access and efficiency in choices for different cancer screening tests across a large health care system. These results suggest that respondents struggled with what researchers have characterized as the Best Outcomes/Fair Chances ethical dilemma, questioning how much one should favor producing the best outcome with limited resources versus giving people a fair chance at obtaining the limited resources. 12 Oftentimes, resource allocation decisions in health care seek to address 2 criteria: they should be cost-effective, and the allocation should be equitable or just. 13 But sometimes, the criteria are in conflict. Our study results of no clear preferences between the 2 concepts of equal health care access and efficiency reinforces the challenges of balancing these criteria.
Compared with Li et al. 10 (N = 881) and Ubel et al. 8 (N = 715), our study (N = 1,346) had a 53% to 88% larger sample and examined a greater variety of professional roles. Our study found that a similar percentage of attending physicians chose the equal health care access test (58%) in comparison with Li et al. 10 (53%). Similarly to Perneger et al., 9 clinicians in our sample were significantly more likely than nonclinicians to choose the equal health care access versus the efficiency option. In contrast, administrative personnel and those with business office functions significantly chose efficiency over equal health care access, which may reflect the financial decision making and incentives inherent in their role. 14 The difference between clinician and nonclinician responses can perhaps be explained by the priority clinicians place on their ethical responsibility to serve all patients equitably, an ethical value highlighted in their medical training with its emphasis in the Hippocratic Oath and Nightingale Pledge.15,16 In addition, some physicians think that “doctors are ethically and morally responsible to promote care for all types of patients.” 17 Finally, one study found that clinicians made better quality decisions than nonclinical personnel did in uncertain probabilistic scenarios, possibly due to varying emotional affect or the “agent affect” (i.e., making decisions for others may involve different levels of loss aversion, with which clinicians may be more comfortable). 18
In our study, men were significantly more likely to prefer the efficiency option. The influence of gender further intersected with professional role. For nonclinical men versus clinical men, the preference for the efficiency option was more pronounced than for nonclinical women versus clinical women. In their 2017 study, Li et al. 10 noted a similar gender finding in the clinical groups they analyzed consisting of medical students, physician residents, and attending physicians, in which women within each cohort were more likely to choose the equitable option compared with men. In contrast, Perneger et al. 9 found no gender difference in preferences in the clinical physician population they assessed in their 2002 study. Evidence that women may generally be more empathetic than men may help explain the preference for the equal health care access option among nonclinicians in our sample. 19 Similar to Li et al.,10,20 we found that nonclinicians and men were more likely to choose the equal health care access option with increasing age, suggesting that one’s life experiences (e.g., with stigma and discrimination) may be a factor in developing decision-making preferences.
Limitations
We were unable to determine the total number of participants who received and opened the initial survey in August 2021. We have estimated the number of eligible participants as 15,000 based on numerous interactions with Tufts Medicine administrators. In addition, it is not clear how generalizable our findings are to other populations. Web-based surveys may lead to inadequate coverage, uneven sampling, and high nonresponse rates. 21 Our response rate of 9% is low as compared with the previous similar study of Li et al. 10 (44.3%). Furthermore, there were fewer than 100 respondents in most of the secondary demographic categories. However, we note that our definition of response rate is conservative as we do not know how many individuals who received the survey actually opened it, but all were included in the denominator. In addition, we had a high number of total responses, 88% more than a previous study (i.e., Ubel et al., 8 N = 715). A low response rate does not necessarily affect the validity of our results but suggests that selection bias may be likely. It will be important to test for nonresponse effects in future studies.
It is also unclear how respondents interpreted the equal health care access and efficiency scenarios (i.e., test 1 and test 2, respectively). The scenario was identical to the one used by Ubel et al. 8 and Li et al., 10 but neither study validated the prompt by medical and ethical experts as a measure of health equity versus cost-effectiveness. Furthermore, we reclassified the scenario to evaluate equal health care access versus efficiency to better reflect the underlying concepts tested.7,9 In addition, embedding the epidemiologic concept of sensitivity in the scenario with the word sensitive may not have been clear to all participants, and we did not ask about participants’ epidemiology expertise.
Our survey methodology also had limitations. First, our choices to categorize certain professional roles (especially as clinical or nonclinical) were based on participants’ self-report and were somewhat arbitrary (e.g., we labeled researchers as having “nonclinical” roles unless they specified “clinical researcher,” even though some researchers have some clinical duties). Second, the cross-sectional survey was conducted during the COVID-19 pandemic, which might have influenced results in unpredictable ways and contributed to the lower response rate than Li et al. 10 Third, our results may not generalize to other nonprofit health systems, especially if the hospital systems differ systematically in their culture or personnel demographic characteristics. We are unable to make comparative statements about other (e.g., for-profit) health systems. Finally, there were potential limitations with the survey questions themselves. The question assessing gender identification used terms for sex rather than gender (i.e., male/female, not men/women) and omitted a category for nonbinary. In addition, the question about immigration status yielded strongly worded written feedback from several participants indicating the question may have been offensive, and it omitted response options for people who were fourth or later generation immigrants or who had only 1 parent born in the United States. The question assessing age included response options with an overlapping age of 65 y old between 2 options. Finally, the question assessing educational attainment assumed that all participants had earned at least a high school diploma or GED and included 1 response option for “college” and 1 for “graduate education,” thereby accounting only for degree completion.
Conclusion
To our knowledge, this is the first study to evaluate the preferences of a wide range of health care professionals for prioritizing equal health care access versus efficiency across an entire health care system. We found that clinicians were more likely than nonclinicians to prioritize equal health care access in clinical decision making and that health administrators/people with business office functions prioritized efficiency. This study was conducted at a large health care system whose strategic plan emphasizes prioritizing health equity, which is likely similar to many health care institutions in the United States. 22 Therefore, additional studies may be needed with updated scenarios to better understand participants’ decision-making preferences about equal health care access, equity, cost-effectiveness, and efficiency. Furthermore, awareness about the differences in attitudes toward equal health care access and efficiency should be increased within health care institutions, as these differing attitudes can ultimately affect patient care and health care quality.
Supplemental Material
sj-docx-1-mdm-10.1177_0272989X231206750 – Supplemental material for Attitudes on Equal Health Care Access versus Efficient Clinical Decisions across a Not-for-Profit Health Care System
Supplemental material, sj-docx-1-mdm-10.1177_0272989X231206750 for Attitudes on Equal Health Care Access versus Efficient Clinical Decisions across a Not-for-Profit Health Care System by Ganeev Singh, Laura Corlin, Paul R. Beninger, Peter J. Neumann, Marcia M. Boumil, Shreya Mehta and Deeb N. Salem in Medical Decision Making
Supplemental Material
sj-pdf-2-mdm-10.1177_0272989X231206750 – Supplemental material for Attitudes on Equal Health Care Access versus Efficient Clinical Decisions across a Not-for-Profit Health Care System
Supplemental material, sj-pdf-2-mdm-10.1177_0272989X231206750 for Attitudes on Equal Health Care Access versus Efficient Clinical Decisions across a Not-for-Profit Health Care System by Ganeev Singh, Laura Corlin, Paul R. Beninger, Peter J. Neumann, Marcia M. Boumil, Shreya Mehta and Deeb N. Salem in Medical Decision Making
Footnotes
Acknowledgements
We acknowledge Raina Connelly and Alexa Roberto at Tufts Medical Center for their technical support during the survey creation and distribution phases of the project.
Author Contributions
The authors made the following contributions: study conception, DNS; study design, GS, LC, PRB, PJN, MMB, SM, DNS; data collection, DNS; data analysis, LC, PJN; manuscript – first draft, GS. All authors reviewed the manuscript multiple times and approved the final version of the manuscript.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LC is supported by Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD) grant number K12HD092535 and by Tufts University. PRB is supported by the Clinical and Translational Science Awards, National Institutes of Health (award No. UL1TR002544). He has also received compensation as a topic editor for Clinical Therapeutics (Elsevier) 2016–2022 and as co-editor-in-chief beginning in 2022, as a subject matter expert for AAAS in 2019, and as a training consultant for small pharmaceutical companies in 2020–2022 for less than 5% of compensation. DNS receives support from the Tupper Research Institute.
Research Ethics
This study (No. 1644) was determined to be exempt by Tufts Health Sciences Institutional Review Board on May 12, 2021. No patient data were obtained as there are no patients in this study. No identifiable information is included about the survey respondents. Survey data and other study materials will be made available upon request to the corresponding author.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.