
Abstract
Background
In orthopedics, the use of patient decision aids (ptDAs) is limited. With a mixed-method process evaluation, we investigated patient factors associated with accepting versus declining the use of the ptDA, patients’ reasons for declining the ptDA, and clinicians’ perceived barriers and facilitators for its use.
Methods
Patients with an indication for joint replacement surgery (N = 153) completed questionnaires measuring demographics, physical functioning, quality of life (EQ-5D-3L), and a visual analog scale (VAS) pain score at 1 time point. Subsequently, their clinician offered them the relevant ptDA. Using a retrospective design, we compared patients who used the ptDA (59%) with patients who declined (41%) on all these measures as well as the chosen treatment. If the use of the ptDA was declined, patients’ reasons were recorded by their clinician and analysed (n = 46). To evaluate the experiences of clinicians (n = 5), semistructured interviews were conducted and thematically analyzed. Clinicians who did not use the ptDA substantially (<10 times) were also interviewed (n = 3).
Results
Compared with patients who used the ptDA, patients who declined use had higher VAS pain scores (7.2 v. 6.2, P < .001), reported significantly worse quality of life (on 4 of 6 EQ-5D-3L subscales), and were less likely to receive nonsurgical treatment (4% v. 28%, P < .001). Of the patients who declined to use the ptDA, 46% said they had enough information and felt ready to make a decision without the ptDA. The interviews revealed that clinicians considered the ptDAs most useful for newly diagnosed patients who had not received previous treatment.
Conclusion
These results suggest that the uptake of a ptDA may be improved if it is introduced in the early disease stages of hip and knee osteoarthritis.
Highlights
Patients who declined the use of a patient decision aid (ptDA) for hip and knee osteoarthritis reported more pain and worse quality of life.
Most patients who declined to use a ptDA felt sufficiently well informed to make a treatment decision.
Patients who declined the ptDA were more likely to have received prior treatment in primary care.
Clinicians found the ptDA to be a helpful addition to the consultation, particularly for newly diagnosed patients.
Background
Shared decision making (SDM) is a collaborative process in which a clinician works together with a patient to reach a decision about care. 1 A patient decision aid (ptDA) is complementary to the consultation and supports SDM. In short, these tools aim to inform patients about treatment options and encourage them to consider which treatment option is most appropriate for them. Extensive evidence supports the benefits of these tools.2,3 A recent review study of randomized controlled trials that evaluated ptDAs for patients considering elective surgery, including hip and knee arthroplasty surgery, showed that these tools reduced decisional conflict, increased knowledge of disease and treatment, improved decision-making preparedness, and enhanced decision quality. 4 Although governments explicitly recommend the use of SDM in health care, successful implementation of SDM, including ptDAs, remains challenging.5–7 In orthopedics, implementation studies are sparse, and although orthopedic surgeons have positive attitudes toward SDM, 8 actual implementation of ptDAs in clinical care is limited. 9 A cross-sectional survey study of patients undergoing total hip or knee arthroplasty found that less than half of the participating patients reported that nonsurgical options or the risks of surgery were discussed during the decision-making process. 10 Another study that used observational measures to assess informed decision making reported similar findings, with discussion of options, potential benefits and harms of surgery, and elicitation of patient preferences occurring in fewer than half of the orthopedic consultations. 11 Little is known about the use of ptDAs in orthopedic clinical practice. Stacey and colleagues 12 conducted a survey study to determine the use of ptDAs in everyday practice following the completion of randomized controlled trials in a variety of clinical settings. They found that only 44% of ptDA trial authors reported some level of use in clinical practice after trial completion. 12
A review of patient barriers to SDM identified a lack of patient knowledge and a power imbalance in the doctor–patient relationship as key issues. 13 In this context, the term power pertains to patients’ perceived level of influence in the decision-making process, including patients’ self-efficacy in decision making and confidence in their knowledge and ability to make a decision. Patient information, for example, from ptDAs and pamphlets, are helpful in providing facts about diseases and treatment options, thereby increasing patient knowledge. However, if the power imbalance is not addressed, it has the potential to become a barrier to SDM. 13 Training clinicians in SDM skills is likely to empower patients and to encourage them to participate in the decision-making process and the care process as a whole. 14
A recognized physician barrier to SDM is lack of time. 15 A Cochrane review found that consultations took 2.6 min longer when a ptDA was used. 2 Other barriers to implementation include lack of applicability due to patient characteristics or the clinical situation. 16 Consequently, clinicians often neglect SDM in actual clinical practice because they feel that the situation is not appropriate.
Recommendations to improve uptake were made in a recent rapid review study on the effectiveness of strategies for ptDA implementation in routine clinical settings. 17 These recommendations included co-production between the ptDA developer and end users (e.g., clinician, patient, and carers), taking account of local needs, training the whole team, preparing patients to engage in SDM, and creating ownership of ptDA implementation by senior staff.
In a previously published article, we described the implementation of a program to improve SDM in orthopedic care and reported that only 17% of the eligible patients with hip and knee osteoarthritis used the ptDA that was routinely offered as part of the program. 18 This program included a comprehensive training in SDM and ptDA use, and most of the recommended measures for successful implementation of PtDAs 17 were adopted. These findings raise the question of why ptDA uptake had been so low in this study. In the current study, we explore patient factors associated with ptDA use and decline, patient-reported reasons for not using the ptDA, and clinicians’ perceived barriers and facilitators to ptDA use. To our knowledge, the relationship between patient characteristics and ptDAs has rarely been investigated. Understanding the characteristics of patients who do not use ptDAs and the reasons for this may help to identify what support they need to make decisions about hip and knee osteoarthritis and what clinicians need to better support their patients.
Method
Design
This study is a process evaluation following the multifaceted SDM intervention described previously. 18 Consecutive hip and knee osteoarthritis patients who met the inclusion criterion were offered the use of a ptDA and were asked to participate in the study. The treating clinicians determined whether patients met the inclusion criteria. A mixed-methods study was used to evaluate implementation of the ptDAs. Using a retrospective design, we compared the demographics and clinical outcomes of patients who used the ptDA with a group of patients who declined. If use of the ptDA was declined, patients’ reasons were recorded by their clinician. To evaluate the experiences of clinicians, semi-structured interviews were conducted.
Population
Patients
Inclusion criteria for the study were in line with the criteria for ptDA use. Eligible patients were adults who had been newly referred with hip or knee osteoarthritis, for whom a surgical intervention (joint replacement surgery) was an appropriate option as judged by their orthopedic clinician. Between August 2019 and March 2020, orthopedic clinicians offered the ptDA to all adult patients who met these criteria. We provided paper forms for the surgeons to indicate which patients were given the ptDA and which were not and for what reason. Medical ethical approval was obtained from the regional Medical Ethical Board (METC Z, nr 16-N-195).
Clinicians
As part of the SDM intervention, 18 19 clinicians from a large Dutch training hospital received training in SDM and ptDA use. This group consisted of 8 orthopedic surgeons, 8 residents in training, and 3 physician assistants. Of this group, 12 clinicians were involved in hip and/or knee osteoarthritis care. Clinicians who used the ptDA substantially (more than 10 times) were interviewed to evaluate the ptDAs used (see Figure 1). Additional brief interviews were undertaken with 3 clinicians who did not use the ptDAs substantially (<10 times), in order to understand why they did not use the tool. The invitations to be interviewed were sent by email.
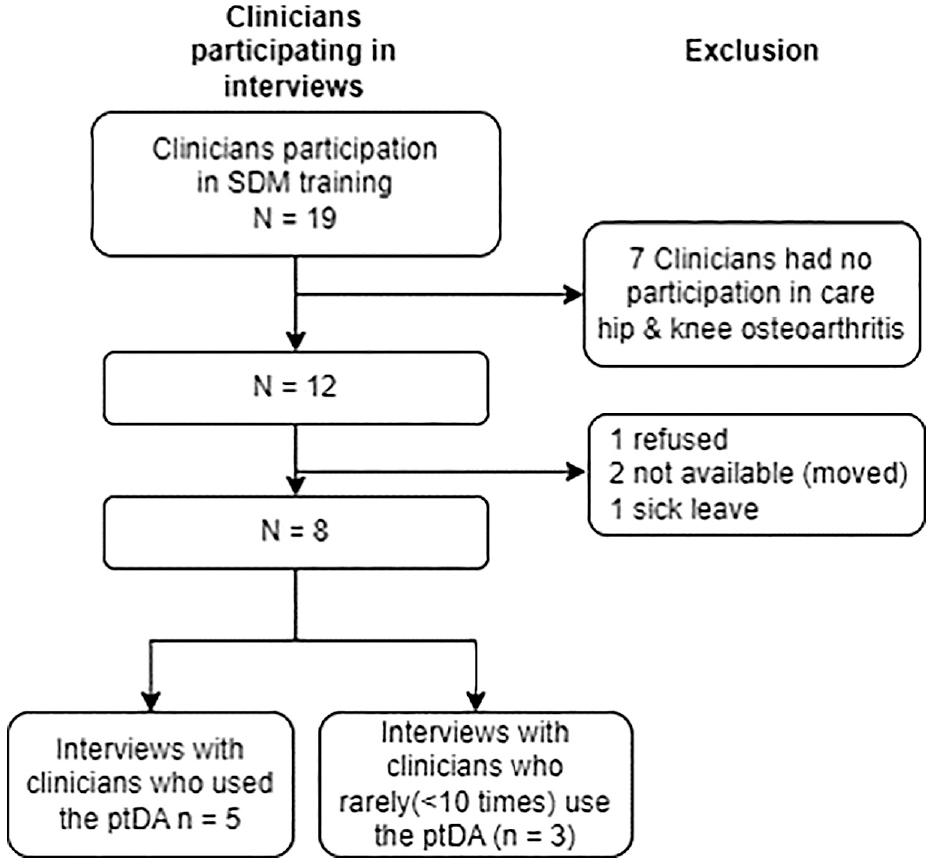
Flowchart of clinician participation for the interviews.
The ptDAs
The hip and knee ptDAs were designed in accordance with International Decision Aids Standards (IPDAS criteria). 19 The Web-based ptDAs contained 5 different elements: information, comparison of treatment options, summary of important points, patient preferences, and questions to verify patient knowledge. The information in the ptDA was provided in colloquial language. The Easy Reading Foundation (in Dutch: Stichting Makkelijk Lezen) assessed the text used in the ptDAs and provided a certificate confirming that the text was easy for lay people to understand. 20 The implemented ptDAs are described in detail in previous literature. 21
Implementation Strategy
The implementation of the ptDA was tailored to the specific needs and context of the orthopedic clinic as described in the parent study. 18 Prior to implementation, all clinicians and outpatient clinic staff were trained. The training consisted of a 1-h e-learning session and a face-to-face training. The training was divided into 2 sessions of 2 h each and was led by 2 trainers with experience in SDM: 1 general physician who is an SDM expert and 1 resident in orthopedic surgery. To enhance practical skills, clinicians were trained in SDM communication and ptDA use through role-play exercises. A senior orthopedic surgeon (and head of the residency program) championed the implementation of the ptDAs.
Patients who met the inclusion criteria and who gave informed consent to participate in the study were invited to use the ptDA. This was done at the first visit before the decision was made. Patients who were willing to use the ptDA were provided a personal access code and an information leaflet so that they could go through the Web-based ptDA at home. After 2 weeks, a telephone consultation with a clinician took place to review the ptDA and to make a treatment decision.
Data Collection and Analyses
Comparison of clinical outcome measures of decision aid users and nonusers
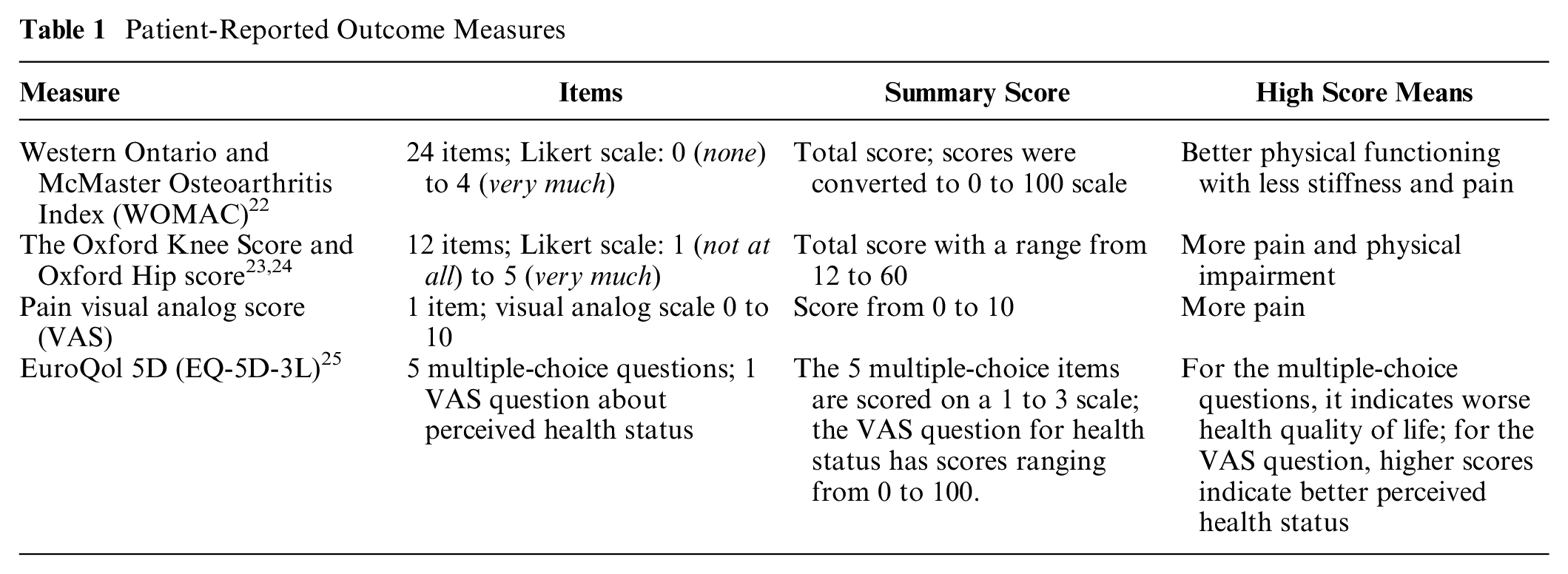
Prior to the first consult, patients completed the following questionnaires: the Western Ontario and McMaster Osteoarthritis Index (WOMAC), the Oxford Knee Score and Oxford Hip score, Pain Visual Analogue Score, and the EQ-5D-3L (see Table 1). In the participating hospitals, the EQ-5D-3L was routinely used as a patient-reported outcome measure (PROM). Therefore, we chose to use this questionnaire, instead of the EQ-5D-5L, to increase feasibility and reduce the administrative burden on the participating patients. The questionnaires were completed at 1 time point.
Patient-Reported Outcome Measures
For the analysis of these quantitative data, we used independent-samples t test and chi-square tests to analyze this normally distributed data set. Since the cell count was low for the categorical variable nonoperative treatment in the ptDA decliner group, we also used Fisher’s exact test to assess the association with the categorical variable intervention (ptDA use or ptDA decline). Stata software was used for the statistical analyses (StataCorp, v14).
Reasons why patients declined to use the ptDA
Clinicians were asked to record which patient accepted and which declined ptDA use, on a paper-based form. When patients declined to use the ptDA, clinicians briefly noted the patient-reported reasons but did not conduct in-depth interviews to explore underlying thoughts or beliefs.
For the analysis, these handwritten reports were digitized and evaluated using content analysis. Three members of the research team read the reports and through discussion identified 4 categories of reasons for declining (as described in the “Results” section). Two authors then assigned each of the reported reasons to 1 of the 4 categories. Because the detail in the stated reasons was limited and there were only 4 categories, this was a straightforward process, and the 2 coders were in full agreement.
Interviews with clinicians
The junior researcher (J.A.W.) who conducted the interviews with the clinicians was a medical student. Although she had some experience in SDM research, she was unfamiliar with qualitative interviewing for research purposes and was therefore trained and supervised by an experienced senior researcher (J.J.). To ensure her independence, J.A.W. confirmed that she had never met any of the clinicians prior to the interview. Further, she declared that she held no preconceived notions about, or prejudices toward, the way in which the clinicians handled the SDM process with patients. The interviews were semi-structured, and we used a brief topic guide that was developed by the whole research team. The online or telephone interviews explored clinicians’ experiences with ptDA implementation and perceived barriers and facilitators for its use. The interviews ranged between 15 and 25 min, during which only the interviewed clinicians and the researcher were present. Notes were taken during the interviews, and audio recordings were made and transcribed afterward. No interviews were repeated, and the transcripts were not returned to the interviewed clinician for comment or correction. Moreover, the participating clinicians did not provide feedback on the findings.
At a later phase, separate interviews were done with 3 other clinicians who did not use the ptDA substantially, in order to find out why they did not use the tool. These brief interviews were done by telephone and have been analyzed separately. A summary of each interview is provided in the “Results” section.
To analyze the interviews, transcripts and notes were studied using framework analysis. 26 The analysis was undertaken primarily by 3 of the 4 authors of the study: J.A.W., J.K.J.B., and J.J., who hold the credentials of BSc, MD, and PhD, respectively. Author J.A.W. started by reviewing the interviews and developing a list of themes and topics using an inductive perspective. Those themes, along with the interview schedule (deductive approach), formed the basis of the coding framework. Two additional authors (J.J. and J.K.J.B.) reviewed the coding framework, and changes were discussed and made accordingly. Once the coding framework was agreed upon, author J.A.W. coded all interviews. Author J.J. double coded a subset of interviews. Coding similarities and differences between authors were discussed and changes were made to the themes when deemed necessary. Data saturation was assessed by the whole team, and after 5 interviews, we had a clear picture of the clinicians’ experiences of ptDA use. The COREQ checklist, a criteria list for reporting qualitative research, 27 was used for reporting the analysis of the interviews (see Supplement 2).
Results
Comparison of Clinical Outcome Measures of Decision Aid Users and Nonusers
In total, a group of 153 patients met the inclusion criteria and were invited to use a ptDA. Of this group, 91 patients used the ptDA, and 62 patients declined. The mean age was 70 y, and 60% (n = 92) were female; 54% (n = 82) were diagnosed with hip osteoarthritis and 46% (n = 69) with knee osteoarthritis. These characteristics did not differ significantly between the ptDA users and nonusers. Patients who used a ptDA chose a conservative treatment in 28% (n = 25) of the cases, compared with 4% (n = 2) of the nonusers (P < .001). PtDA users had a visual analog scale (VAS) pain score of 6.2 compared with a score of 7.2 for the nonusers (P < .001). Quality of life was significantly worse in the group who declined the ptDA on 4 of the 6 EQ-5D subscales, with worse scores for self-care (1.48 v. 1.26; P = .008), usual activities (2.02 v. 1.77; P = .004), pain and discomfort (2.39 v. 2.18; P = .042), and health status (49.31 v. 60.79; P < .001). The disability related to hip osteoarthritis (WOMAC and Oxford questionnaires) did not differ between the 2 groups (see Table 2).
Characteristics for ptDA Users and ptDA Decliners
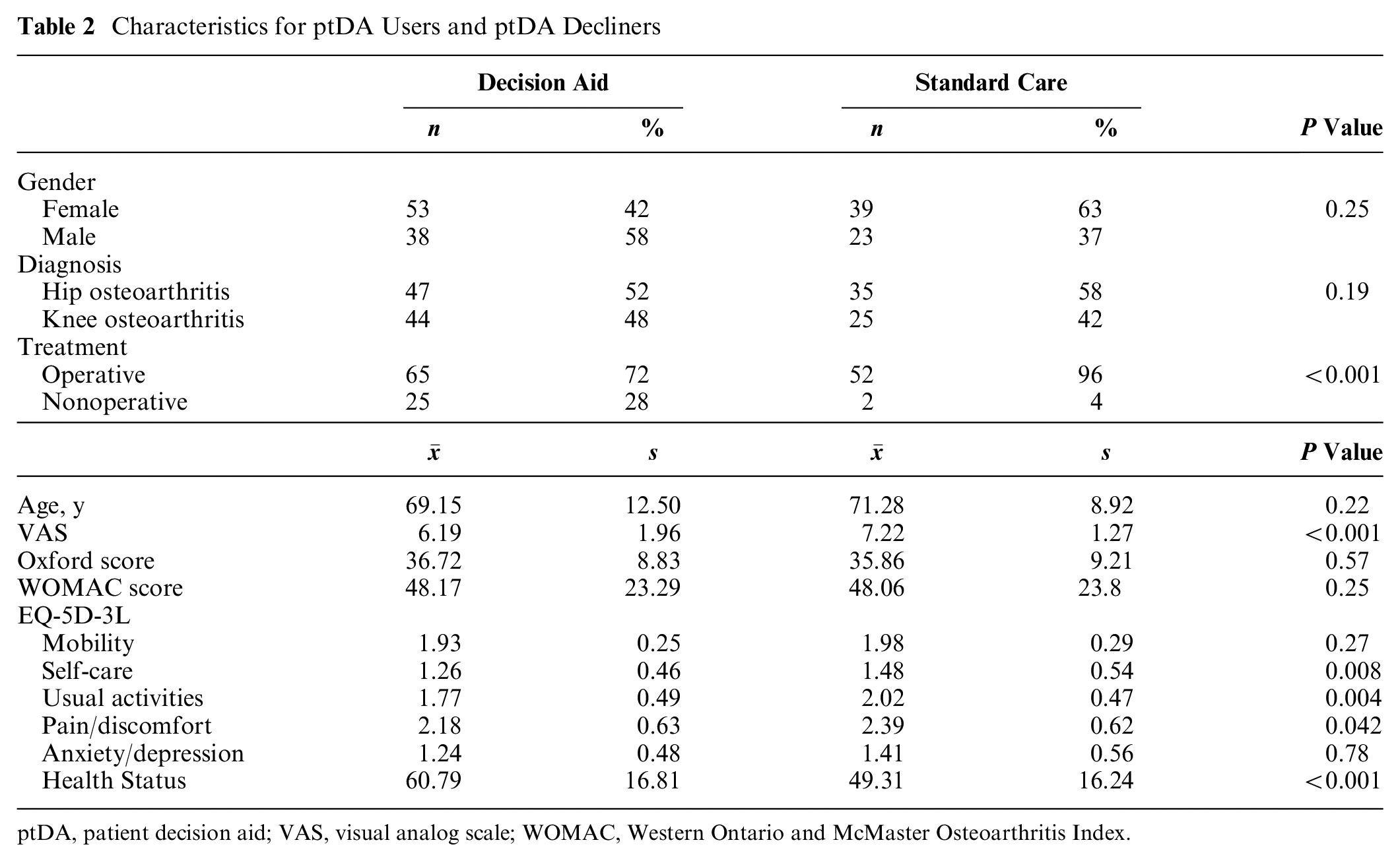
ptDA, patient decision aid; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Osteoarthritis Index.
Reasons Why Patients Declined to Use the ptDA
Of the 62 ptDA nonusers, 46 patients (39%) reported why they declined to use the tool. The main reason for declining the ptDA was that they felt they did not need it because they were sufficiently informed about their disease and the treatment options (46%, 21/46). For example, these patients had already received extensive information from their general practitioner (GP) or had undergone hip or knee replacement surgery previously. In addition, patients (33%, 15/46) indicated that they had no desire for information regardless of their existing level of knowledge about the disease and treatment options. Another reason given was that the use of a ptDA required an extra consult, and the patients did not want to delay the treatment process (11%, 5/46). Finally, some patients (11%, 5/46) were not able to use the digital ptDA due to insufficient digital skills (digital illiteracy) or because they did not have a smartphone or computer (see Figure 2).
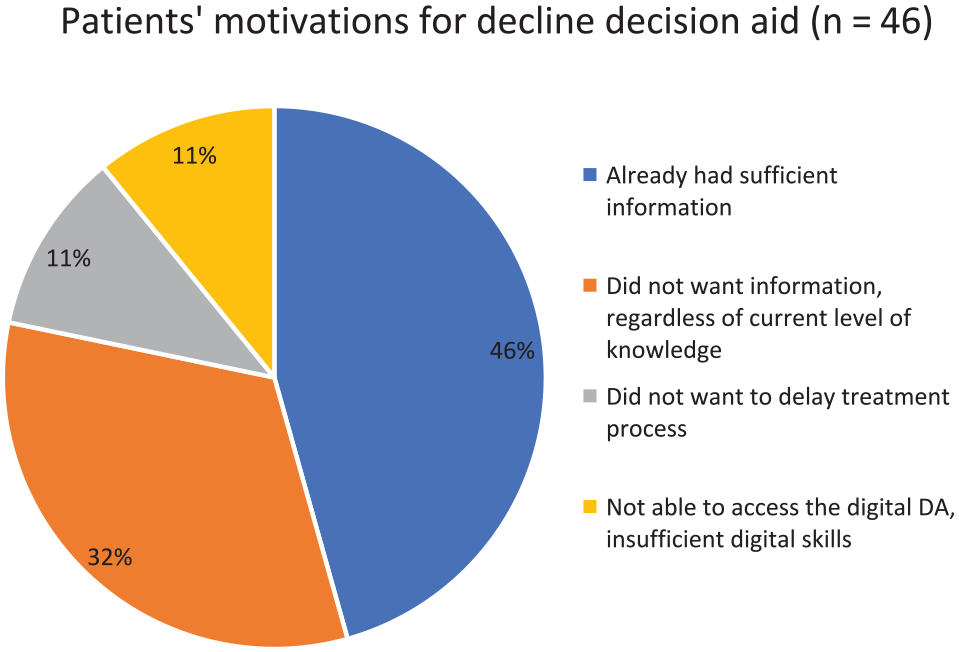
Pie chart on patients’ motivation for declining the decision aid.
Interviews with Clinicians
Nine clinicians reported substantial use of the ptDA (at least 10 times). Three clinicians rarely used the ptDA, and a summary of their reasons for nonuse is given at the end of this paragraph. Of the 9 clinicians who used the ptDAs, 2 clinicians were not available for the interviews because they worked in other hospitals at the time of the interviews. One clinician was unavailable because of sick leave. One refused to be interviewed due to time constraints. We interviewed 5 clinicians to evaluate the ptDAs that were implemented: 3 orthopedic surgeons, 1 orthopedic resident, and a physician assistant. The clinicians who were interviewed had a mean age of 46 y (range 38–63 y) and mean clinical experience of 21 y (range 12–39 y). All interviewed clinicians were male. Data saturation was reached after 5 interviews with no new themes emerging. The central themes derived from the interviews were “benefits of ptDA use,” “barriers to ptDA use,” and “timing of the ptDA in the care process” (see Supplement 1 for quotes supporting the major themes and minor themes).
Benefits of ptDA use
Information provision
Four of the 5 clinicians indicated that the ptDA was a helpful addition to the conversation. The clinicians noticed that patients were better informed and had more specific questions after going over the ptDA.
The ptDA was found most useful for a subgroup of patients
Most clinicians (4 of 5) observed that the usefulness of the ptDA depended on what stage of care the individual patient was in. It was found to be particularly useful for recently diagnosed patients, who were overwhelmed by the diagnosis, as it often provided new information about the pros and cons of different treatment options. Another group of patients who were perceived to especially benefit from the ptDA were those who were unsure about which treatment was best for them. According to the clinicians, these patients valued the ptDA because it allowed them to take the time they needed to absorb all the information and consider different treatment options.
One of the clinicians mentioned that he found the ptDA useful for patients who had not deliberated on different treatment options well enough. The clinician felt that these patients needed information and time to consider different treatment options, as they were not yet ready to make an informed decision. The ptDA encouraged these patients to consider the different treatment options and to avoid making a hasty or uninformed decision.
Helpful in time constrained clinic
One clinician stated that the tool was helpful in a time-deficient clinic. The provision of information is one of a clinician’s tasks. As the ptDA provides information, this clinician perceived the tool as supporting the consultation process and thus reducing his workload.
Barriers to the use of ptDAs
Most clinicians (4 of 5) pointed out that the tool was often considered to be superfluous by a particular group of patients. Clinicians described this group of patients as those who were already fully aware of the diagnosis and had been treated by their GP or by a physiotherapist. They often came to the hospital with a clear request for surgery and felt sufficiently informed about different treatment options. There were a significant number of patients with this background in the orthopedic clinic. Clinicians observed that when the ptDA was offered to these patients, they did not think it was necessary, and the patients often declined to use it.
Delays to care process
Patients often expressed concern that the ptDA would delay the care process. This is because the decision to use a ptDA requires a second meeting to be scheduled for final decision making, after the patients had been given the opportunity to complete the ptDA at home. Patients often felt ready to make a treatment decision at their initial meeting and therefore declined to use the tool in order to avoid treatment delay.
Concerns about the concept of ptDA
One surgeon pointed out that making the ptDA mandatory could result in less interaction between the orthopedic surgeon and the patient. He was concerned that the ptDA might reduce the need for doctor–patient communication and thus replace the consultation.
Digital literacy
Although clinicians reported that most patients were able to use the Web-based online ptDA, 3 of 5 clinicians remarked that some patients had no smartphone, computer, or the skills needed to access the Web-based tool.
Timing of ptDA use in care process
Requisites for ptDA use
Most of the clinicians pointed to the importance of having a confirmed diagnosis before using a ptDA. Therefore, implementation of this tool in primary care was not found to be appropriate, as orthopedic expertise and diagnostics were perceived to be lacking in that setting. Another consideration expressed was that the ptDA was found to be suitable only for patients eligible for a surgical treatment, because it contained information about surgical treatment options. The clinicians were concerned that patients who had no indication for surgery might mistakenly be led by the ptDA to believe that surgery was an option for them. They proposed that patients should be eligible for surgery as a condition of receiving the ptDA.
Early care process
The clinicians commented that uptake of the ptDA might be improved if it were used at an early stage of the disease, when all treatments are optional. Following on with that idea, one clinician mentioned that implementation in primary care might improve uptake of the ptDA, in contrast to the views of other clinicians who considered implementation in primary care inappropriate (see above).
Summary of interviews with clinicians who used the ptDAs
All in all, most clinicians were positive about the use of the ptDA and found it to be a helpful addition to the conversation with patients. The ptDA was perceived to be especially useful for newly diagnosed patients and for patients who were uncertain about the right treatment. For these patients, the ptDA was considered an excellent tool, as it gave them time to consider treatment options at home. However, the clinicians pointed out that the ptDA was not suitable for all patients. As an example, they cited patients with more advanced osteoarthritis, who commonly have a clear preference for surgery. These patients found the ptDA to be unnecessary and the cause of needless delay. Digital illiteracy was considered a barrier for a small group of patients. Regarding the timing of the ptDA dissemination, the clinicians were in agreement that it is preferable to distribute it at an early stage of the disease but only after a diagnosis had been established.
Interviews with clinicians who did not use the ptDAs substantially
We had brief additional interviews with clinicians (n = 3) who did not use the ptDA substantially in order to understand their reasonings. Two of them were male, and 1 clinician was a female, with ages ranging between 45 and 63 y. The first clinician expressed a desire to be in control of the whole decision-making process. That clinician was concerned that patients who used a ptDA outside of the clinician’s office would be less likely to choose a treatment that coincided with the clinician’s studied opinion. The second clinician reported that use of the ptDA was not feasible because of time constraints. The third clinician thought that the decision-making process was too complex for a ptDA to be of assistance. That clinician pointed out that the conversation with the patient is the single most important modality in the decision-making process. Time constraints along with a dislike of administration and new tasks also played a role in not using the ptDA.
Discussion
This research study is a follow-up study to a published paper in which we tested and implemented a program to improve the use of SDM in the orthopedic care setting. 18 In that article, we reported that only 17% of the patients with hip and knee osteoarthritis used a ptDA. 18 In the current study, we used qualitative and quantitative analyses to assess perceived barriers to and facilitators of the implementation of ptDAs in hip and knee osteoarthritis.
We found that patients who used the tool were more likely to choose conservative treatment over surgery. This ptDA group reported less pain and a better quality of life. Patients who declined the use of a ptDA reported having sufficient information to make a decision and had frequently received prior, conservative treatment. Patients with more severe complaints were more likely to want surgery for their hip or knee complaint and less often felt the need for a ptDA. These patients commonly perceived surgery as the only suitable treatment option and therefore considered a ptDA to be superfluous. Other studies pointed out that surgery is often seen as the default treatment for severe osteoarthritis, 28 and this is a barrier to the use of ptDAs. Similarly, surgeons have confidence in their surgical treatment and generally consider joint replacement as the only solution for advanced hip or knee osteoartritis. 29 Although hip joint replacement surgery is especially successful in terms of patient satisfaction, 30 the dissatisfaction rate after total knee arthroplasty still ranges between 15% and 25%. 31 A ptDA stimulates patients to consider all treatment options instead of just focusing on the surgical solution. Consequently, the tool has the potential to produce more realistic expectations. 2
The interviews revealed that clinicians generally found the ptDA to be useful. It provides additional information to patients, and in their experience, patients asked more specific questions after completing it. The tool was found to be most helpful for recently diagnosed patients who had little knowledge of the diagnosis and treatment options. The ptDA was least helpful for patients who felt well informed enough to make a decision at the first consultation. The interviews revealed that patients who declined the tool had often been treated conservatively and had previously discussed treatment options with their GP or physiotherapist. Although these patients often believed themselves to be sufficiently informed to make a treatment decision, we know from previous research that patients are often unaware of their misconceptions, and their treatment preferences may be based on limited knowledge. 32 In a study about Parkinson’s disease, most patients thought they were well-informed, but only 41% were aware of the different treatment options. 33 We know that patients who are better informed make different treatment choices. 14 Therefore, clinicians should not assume that their patients have adequate knowledge of disease and treatment options. They should strive to verify this to ensure that patients do indeed make informed decisions.
When considering ways to improve the uptake of the ptDA, it seems logical to implement the ptDA in the early stages of hip or knee osteoarthritis. The primary care setting would appear to be opportune for introduction of the ptDA, as newly diagnosed patients who have not exhausted all treatment options tend to be more inclined to use the tool. However, when asked about alternative implementation approaches, the interviewed clinicians did not believe it was appropriate for GPs to discuss the ptDA with their patients. The clinicians felt that a diagnosis needed to be made first, before considering treatment options, and in their view, a confirmed diagnosis can be made only by an orthopedic clinician. In addition, they did not think it was right for the GP to discuss the options for surgical treatment in detail when going through the PtDA. These beliefs need to be addressed to improve ptDA use in orthopedic care. Recently, initiatives have been taken to implement specialized orthopedic care in the primary care setting to reduce referral rates from primary care to the orthopedic clinic in the hospital. 34 This arrangement allows orthopedic clinicians to make a diagnosis in the primary care setting. This may address the concerns of the clinicians, and with that, the disease-specific ptDA can be distributed to patients at an early phase of hip or knee osteoarthritis care. This scenario could have a positive effect on the uptake of ptDAs.
Limitations
Patients who were eligible to use the ptDA were invited to participate in the study. A decline to use the ptDA was also recorded. Although the clinicians confirmed that they had invited all eligible patients for ptDA use, we did not collect data on this, and it is possible that some eligible patients were overlooked due to the nature of clinical practice. For example, patients with very severe complaints of advanced osteoarthritis may have been scheduled directly for surgery at short notice, without considering a ptDA. However, the number of such incidents is estimate to be small, as consecutive patients were invited to use the ptDA and the burden on patients was low as the questionnaires obtained were part of the hospital’s PROM’s set. Patients’ reasons for declining the ptDA were collected and written down on special forms by the clinicians. This could have introduced bias and elicited socially desired responses from patients. On the other hand, this information was important for clinicians, as it enabled them to check if the patient had correctly understood the options and the aim of the PtDA. The clinicians limited themselves to simply noting the reason for declining the ptDA; they did not conduct in-depth interviews with the patients to explore underlying thoughts or beliefs. Another limitation of our study is the relatively small sample size for the interviews obtained. However, we interviewed the majority of the clinicians who were involved in the care of hip and knee osteoarthritis and participated in the SDM program (8 of 12 clinicians). We believe that saturation had been reached after the interviews and were able to derive a central and shared message from these interviews. In addition, our findings from the interviews were supported by reasons given by patients for declining the ptDA and by the data from the questionnaires.
Conclusion
Findings suggest that the ptDA is most suitable for patients with a recent diagnosis and less advanced disease and symptoms. Implementation of the tool earlier in the illness trajectory might be more appropriate, provided that the patients have a confirmed diagnosis. More research is needed to determine the optimal setting, timing, and target population for the ptDA for hip and knee osteoarthritis. Our study highlights the importance of considering context including patient characteristics when implementing ptDAs.
Supplemental Material
sj-docx-1-mdm-10.1177_0272989X231205858 – Supplemental material for Implementation of a Decision Aid for Hip and Knee Osteoarthritis in Orthopedics: A Mixed-Methods Process Evaluation
Supplemental material, sj-docx-1-mdm-10.1177_0272989X231205858 for Implementation of a Decision Aid for Hip and Knee Osteoarthritis in Orthopedics: A Mixed-Methods Process Evaluation by Jeroen Klaas Jacobus Bossen, Julia Aline Wesselink, Ide Christiaan Heyligers and Jesse Jansen in Medical Decision Making
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.