
Abstract
Introduction
Surgeons are entrusted with providing patients with information necessary for deliberation about surgical intervention. Ideally, surgical consultations generate a shared understanding of the treatment experience and determine whether surgery aligns with a patient’s overall health goals. In-depth assessment of communication patterns might reveal opportunities to better achieve these objectives.
Methods
We performed a secondary analysis of audio-recorded consultations between surgeons and patients considering high-risk surgery. For 43 surgeons, we randomly selected 4 transcripts each of consultations with patients aged ≥60 y with at least 1 comorbidity. We developed a coding taxonomy, based on principles of informed consent and shared decision making, to categorize surgeon speech. We grouped transcripts by treatment plan and recorded the treatment goal. We used box plots, Sankey diagrams, and flow diagrams to characterize communication patterns.
Results
We included 169 transcripts, of which 136 discussed an oncologic problem and 33 considered a vascular (including cardiac and neurovascular) problem. At the median, surgeons devoted an estimated 8 min (interquartile range 5–13 min) to content specifically about intervention including surgery. In 85.5% of conversations, more than 40% of surgeon speech was consumed by technical descriptions of the disease or treatment. “Fix-it” language was used in 91.7% of conversations. In 79.9% of conversations, no overall goal of treatment was established or only a desire to cure or control cancer was expressed. Most conversations (68.6%) began with an explanation of the disease, followed by explanation of the treatment in 53.3%, and then options in 16.6%.
Conclusions
Explanation of disease and treatment dominate surgical consultations, with limited time spent on patient goals. Changing the focus of these conversations may better support patients’ deliberation about the value of surgery.
Highlights
In decision-making conversations about high-risk surgical intervention, surgeons emphasize description of the patient’s disease and potential treatment, and the use of “fix-it” language is common.
Surgeons dedicated limited time to eliciting patient preferences and goals, and 79.9% of conversations resulted in no explicit goal of treatment.
Current communication practices may be inadequate to support deliberation about the value of surgery for individual patients and their families.
This is a visual representation of the abstract.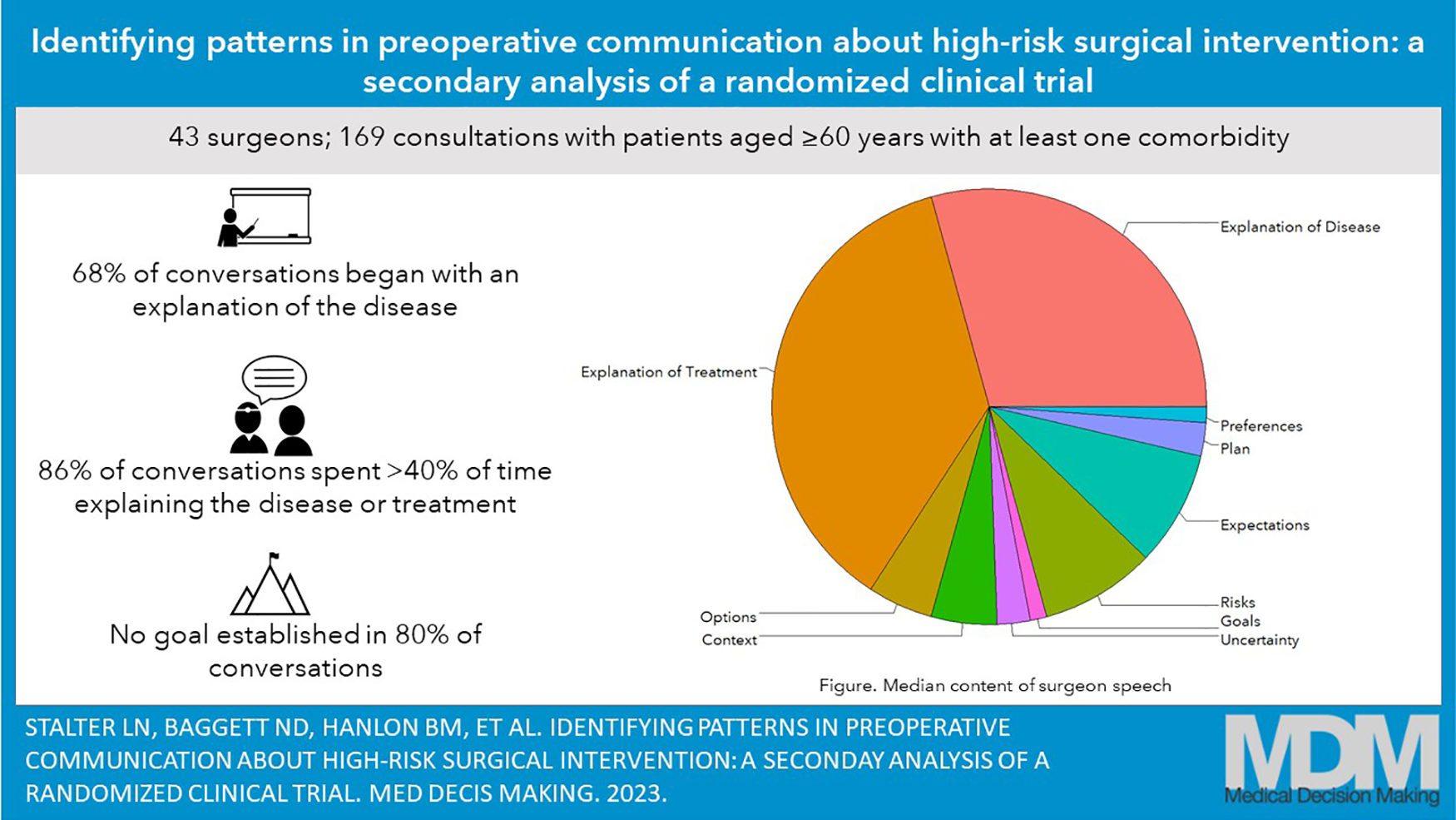
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.