
Abstract
Objective
Dealing with uncertainty is a core competence for physicians. To evaluate the impact of an educational intervention on family medicine residents’ (FMRs’) intention to request diagnostic tests and their attitudes toward uncertainty.
Methods
Nonrandomized controlled trial. Intervention group (IG) FMRs participated in interactive “dealing with uncertainty” seminars comprising statistical lessons and diagnostic reasoning. Control group (CG) FMRs participated in seminars without in-depth diagnostic lessons. FMRs completed the Dealing with Uncertainty Questionnaire (DUQ), comprising the Diagnostic Action and Diagnostic Reasoning scales. The Physicians’ Reaction to Uncertainty (PRU) questionnaire, comprising 4 scales (Anxiety Due to Uncertainty, Concern about Bad Outcomes, Reluctance to Disclose Uncertainty to Patients, and Reluctance to Disclose Mistakes to Physicians) was also completed. Follow-up was performed 3 months later. Differences were calculated with repeated-measures analysis of variance.
Results
In total, 107 FMRs of the IG and 102 FMRs of the CG participated at baseline and follow-up. The mean (SD) Diagnostic Action scale score decreased from 24.0 (4.8) to 22.9 (5.1) in the IG and increased in the CG from 23.7 (5.4) to 24.1 (5.4), showing significant group difference (P = 0.006). The Diagnostic Reasoning scale increased significantly (P = 0.025) without a significant group difference (P = 0.616), from 19.2 (2.6) to 19.7 (2.4) in the IG and from 18.1 (3.3) to 18.8 (3.2) in the CG. The PRU scale Anxiety Due to Uncertainty decreased significantly (P = 0.029) without a significant group difference (P = 0.116), from 20.5 (4.8) to 18.5 (5.5) in the IG and from 19.9 (5.5) to 19.0 (6.0) in the CG.
Conclusion
The structured seminar reduced self-rated diagnostic test requisition. The change in Anxiety Due to Uncertainty and Diagnostic Reasoning might be due to an unspecific accompanying effect of the extra-occupational seminars for residents.
Background
Dealing with uncertainty is a core issue for physicians when it comes to medical decision making during patient care. Although widely recognized in research,1–4 it is rarely embedded in the modern medical curriculum. Medical students and residents are rigorously trained to turn clinical signs and symptoms and test results into solutions by rapidly identifying diagnoses, which creates a medical culture with a deep-rooted unwillingness to acknowledge uncertainty in medicine. 1 However, uncertainty is inherent in medicine. This may be partly explained by the fact that medicine is a rapidly evolving field in which the boundaries of knowledge are continually being pushed 3 but also due to the often vague presentation of symptoms, indifferent clinical patterns in individual patients, and the variable course of diseases. Gerrity et al. developed a questionnaire for the conceptualization and measurement of personal sources of uncertainty, 4 which was revised in 1995. 5 It could be shown that medical students with a higher tolerance of uncertainty are more likely to choose careers in fields such as primary care, whereas lower tolerance is more associated with urology or surgery.5,6 In addition, it was demonstrated that physicians with low tolerance of uncertainty tend to frequent test requisition.7,8 With respect to patients, positive expectations and unexplained complaints lead to more test requisition, 9 and psychosomatic comorbidity is associated with frequent referrals. 10
This is particularly problematic for diagnostic reasoning and decision making in primary care, where the pretest probabilities of diseases are lower compared with the hospital setting, 11 which in turn leads to more false-positive test results. 12 The Bayesian theorem helps us to understand that the probability of suffering from an indicated disease is lower in a test-positive patient when the pretest probability of the disease is low. 13 In addition, patients often see the doctor at the beginning of an illness, when the symptoms are less distinct than in the advanced stages. 14 Consequently, these unselected patient groups create multiple decisional opportunities accompanied by high diagnostic uncertainty as a severe deterioration in health status must also be taken into account. Strategies to deal with uncertainty comprise stepwise diagnostic procedures, “test-of-time” heuristics, and shared decision making, taking into account the familial and occupational circumstances of the patient.2,12,15,16 These strategies are essential for optimal patient management when considering test requests and referrals to balance overdiagnosis with underdiagnosis. It was shown that younger family medicine physicians, as well as family medicine residents (FMR) in particular, experience difficulties in managing uncertainty.17,18 Morgan et al. 19 developed an educational intervention to meet the needs of FMRs during the critical period in the development of appropriate patterns of test-ordering behavior. Their workshop led to the intended changes in attitudes and more rational test ordering. However, the impact of confounding variables, like adaption to the practice environment, remained unclear as this intervention was performed as a single-armed study.
The aim of our controlled trial was to evaluate the impact of an educational intervention on the FMRs’ attitude to uncertainty and test ordering. The expectation was that the seminar would lead to a more appropriate attitude toward diagnostic uncertainty in the primary care setting. Accordingly, the primary hypothesis was that the seminar would lead to a reduction in self-rated diagnostic test requisition; the secondary hypotheses were that it would increase diagnostic reasoning and decrease anxiety due to uncertainty and reluctance to disclose uncertainty.
Methods
Study Design and Participants
The study was performed as a controlled trial without randomization. Participants were FMRs who were taking part in structured courses run by the Competence Centre for Residency Training in Family Medicine Bavaria (CCRTB), a Bavarian residency training scheme in family medicine. In Germany, the residency for becoming a family physician takes at least 5 years. The traineeship combines clinical experience in hospital and primary care practice. Additional courses were established in 2014 within the CCRTB with the aim to stimulate professional development and motivate newly qualified family physicians to establish their own private practice. FMRs participate in these courses on a voluntary basis. The training scheme comprises classical clinical topics, communication skills, and management issues following the CanMeds Framework. 20
Intervention group FMRs participated in the “Dealing with Uncertainty in Primary Care” seminar, which lasts 90 minutes and is embedded within the day-course “The Difficult Patient”; the lecturers were AS and MR. Control group FMRs participated in day-courses covering different clinical topics. FMRs registered for the courses without previous in-depth knowledge of the seminar contents. Five intervention and 4 control courses were held between July 2018 and October 2019.
FMRs filled in the Physicians’ Reaction to Uncertainty (PRU) questionnaire and Dealing with Uncertainty Questionnaire (DUQ) (described below) before the beginning of the course (t1). Participants were requested to fill in the questionnaire by email through LimeSurvey 3 months later (t2). Nonresponding participants received a second email and, after that, a one-time postal inquiry to fill in the questionnaire for follow-up. The study was approved by the Ethics Committee of the Medical Faculty of the Technical University Munich, and all FMRs gave their written informed consent.
Content and Format of the Seminar
Intervention group
“The Difficult Patient” course included 3 main parts. The first reflected on professional attitudes and handling patients with, for instance, low socioeconomic status or communication problems. A second part covered management of refugees in family medicine. The third seminar, titled “Dealing with Uncertainty in Primary Care,” was introduced with a clinical example of a female patient presenting with a persistent cough. The FMRs had to work out differential diagnoses related to this symptom. This leads to a large spectrum of diagnoses, ranging from common diseases, such as common cold, asthma, gastroesophageal reflux disease, or medication side effect, to very rare and more serious diseases such as a lung carcinoma or pulmonary embolism. A group discussion was initiated to debate the diagnostic management, which highlighted the complexity of diagnostic decision making. Following the discussion, strategies and heuristics for diagnostic workup in family practice were introduced to the FMRs in lectures that comprised 5 steps: 1) The FMRs were invited to discuss and reflect on the diagnostic value of a hypothetical diagnostic test with high sensitivity and specificity. However, the positive predictive value of the hypothetical test was low due to low disease prevalence. 2) Subsequently, the FMRs had to calculate 2 different scenarios, thereby working out the high impact of the pretest probability on the predictive values of a test. Then we explained the relationship between sensitivities and specificities with positive and negative predictive values and prevalence of disease, as described by Bayes’s theorem. 13 3) The selection process of patients along different sectors of a health care system was illustrated by presenting the “The Ecology of Care Revisited” survey by Green et al., 11 with the aim of demonstrating primary care practice as a “low prevalence area” in the context of diagnostics. 4) Through group discussions, we illustrated that a reasonable diagnostic strategy in primary care comprises “precise history taking,”“physical examination,”“stepwise diagnostic procedures with use of technical diagnostic instruments,” and “test-of-time” strategies to successively improve pretest probabilities in terms of stepwise diagnostic procedures. 12 “Test-of-time” strategies are related to heuristics that take the disease course into account. That could be the reevaluation of a patient a couple of days later or questions regarding the duration of symptoms (e.g., a 10-year history of migraine would rule out a malignant brain tumor because a brain tumor, if left untreated, would prove fatal within a few years at most). 5) The “fishbowl” method was used to reflect on a case of an overlooked pulmonary embolism. In the “fishbowl” method, an inner group discusses an issue or topic while the outer group listens, looking for themes, patterns, or soundness of argument, or uses a group behavior checklist to give feedback to the group on its functioning.21,22 Three FMRs had to advocate for diagnostic management from the position of hospital specialists, normally treating highly selected patients. This should lead to the argument that persistent cough is a “typical sign” for pulmonary embolism, which is ecologically adapted to a care setting with high prevalence of serious disease, such as the emergency department of a tertiary care hospital. Three other FMRs had to defend their diagnostic management of the patient with persistent cough from the perspective of a family physician, dealing with low selection of patients in primary care. This should lead to the argument that it might be irrational to manage every coughing patient as a pulmonary embolism case. From this point of view, investigating a patient with cough for pulmonary embolism is justified only under very rare circumstances. The aim of this conflictive discussion was to deliberate the inherent statistical uncertainty of diagnostic testing and its impact on patient management in primary care.
Control group
The 1-day courses attended by the control group included “Management of Patients with Type 2 Diabetes,”“Management of Patients with Thyroid Disease,” and “Management of Patients with Skin Conditions.” Lectures on etiology, prevalence, and management by national guidelines were followed by reflective case scenarios to enhance the clinical reasoning of the FMRs. This part also touched upon aspects that included diagnostic strategies related to the case scenarios. However, typical heuristics were not explicitly discussed or prepared in-depth. Additional topics covered included legal orders and aspects of practice organization. The participants in the control arm did not participate in the intervention group seminars before the follow-up evaluation.
Questionnaires
PRU
Gerrity et al. developed a questionnaire to measure physicians’ affective reaction to uncertainty, 4 the PRU, which was revised in 1995. 5 The German version of the PRU was validated and culturally adapted in 2007 with satisfying psychometric properties. 23 The PRU comprises the following 4 scales: Anxiety Due to Uncertainty (range, 5–30), Concern about Bad Outcomes (range, 3–18), Reluctance to Disclose Uncertainty to Patients (range, 5–30), and Reluctance to Disclose Mistakes to Physicians (range, 2–12). The items are rated on a 6-point Likert scale: 1 = strongly disagree, 2 = moderately disagree, 3 = slightly disagree, 4 = slightly agree, 5 = moderately agree, and 6 = strongly agree. The scales are scored by summing physicians’ responses to each item in the scale. The greater the score, the greater the physicians’ affective reaction to uncertainty at that scale. The PRU is provided in the supplement.
DUQ
The DUQ was developed to measure the level of diagnostic activity to avoid uncertainty and to describe the active reasoning behind dealing with uncertainty in primary care. 24 The DUQ comprises 2 scales: Diagnostic Action (range, 6–36) and Diagnostic Reasoning (range, 4–24). The Diagnostic Action scale was intended to reflect the level of diagnostic activity, which is undertaken to solve a medical problem (e.g., ordering laboratory tests and imaging procedures). The internal consistency was sufficient with a Cronbach’s α of 0.75. The Diagnostic Reasoning scale aimed to capture strategies like the use of heuristics by family doctors by using the test-of-time strategy or including the psychosocial context to make a medical diagnosis. The Cronbach’s α of the Diagnostic Reasoning scale was less satisfying (0.62). The items are rated on a 6-point Likert scale, identical to the PRU questionnaire. The scales are scored by summing physicians’ responses to each item in the scale. The greater the score, the greater the diagnostic activity or, respectively, the use of primary care heuristics like “test of time” and “psychosocial anamnesis.” It was shown that the Diagnostic Action scale correlated positively with Anxiety Due to Uncertainty, Concern about Bad Outcomes, and Reluctance to Disclose Mistakes to Physicians. 24 The DUQ is provided in the supplement.
Statistical Analysis
Differences between the scales relating to gender and duration of work experience were calculated with analysis of variance (ANOVA), t test, or χ2 test where appropriate. By inspection and Q-Q plot, there was no relevant deviation from the normal distribution detected in the considered variables. Due to the low Cronbach’s α of the DUQ in the previous analysis, 24 we explored the factorial validity with a maximum likelihood factor analysis based on polychoric correlations with oblimin rotation for the DUQ items at baseline. The criterion for the factor extraction was a parallel analysis 25 based on polychoric correlations and the empirical Kaiser criterion (EKC). All analyses were conducted with R 26 and the package psych 27 and the MBESS package. 28 For the EKC, an R syntax was written and used. To replicate the previous findings, 24 we assessed the internal consistency with Cronbach’s α.29,30 We used all items of the previous DUQ without leaving the previously nonfitting items. The items were summarized according to their associated scales.
To test for systematic changes in quantitative outcomes between the first and second evaluations, ANOVA for repeated measures was carried out. “Intervention v. control group” served as a between-subject factor, and gender and duration of work experience were used as covariates. In the repeated-measures ANOVA model, similar changes in the scales in both groups were designated as a “time effect.” Differences between the intervention and control group with respect to the changes in scales were described by an “interaction effect between time and group,” which was specifically due to the effect of an intervention. Correspondingly, the primary end point was the difference in group-specific changes in the Diagnostic Action scale, which was determined by the interaction effect between time and group. The differences between the change in other scales served as secondary end points. A level of significance of P < 0.05 was used. We could not perform a power calculation a priori, because we had no information about the minimal important differences between the questionnaire scales. Previous studies have shown that medical educational interventions in family medicine were effective when they were evaluated with 150 to 200 participants.17,19,31 Based on these studies, our aim was to include at least 100 FMRs in each group. The expected dropout rate during follow-up was 25%. Thus, we aimed to include at least 140 FMRs in each group at baseline.
Results
All 283 FMRs of the 9 seminars participated at baseline, 139 in the intervention group (30 [22%] male) and 144 in the control group (27 [19%] male). A total of 107 (77%) intervention group FMRs (22 [21%]) and 102 (71%) control group FMRs (20 [20%] male) participated in the follow-up evaluation (Figure 1). There were no significant differences with respect to gender, workplace, age, and years of experience between responders and nonresponders at follow-up (not in table). The mean (SD) age of the completers of follow-up was 36.1 (7.7) years in the intervention group and 35.1 (6.3) years in the control group (Table 1). Duration of work experience was on average 3.4 years in both groups. Both groups were also comparable with respect to gender and workplace, with no significant differences in each group.
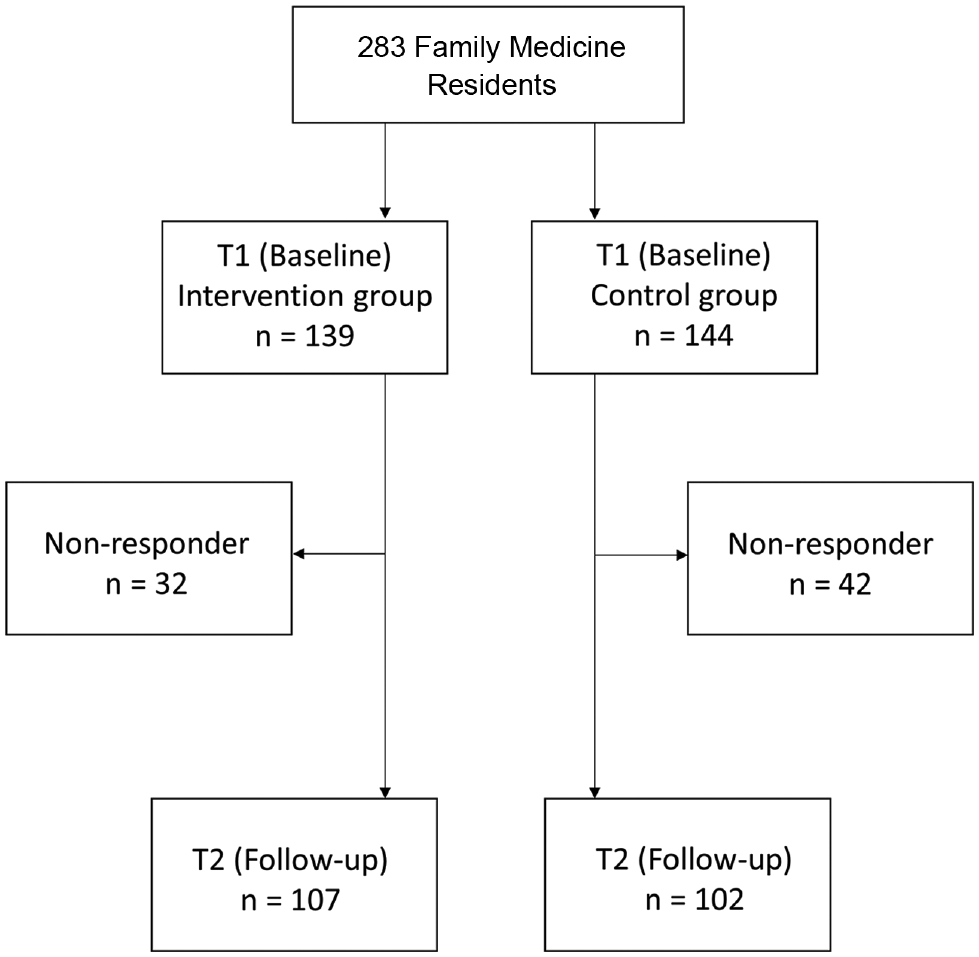
Flowchart of participants.
Baseline Characteristics a
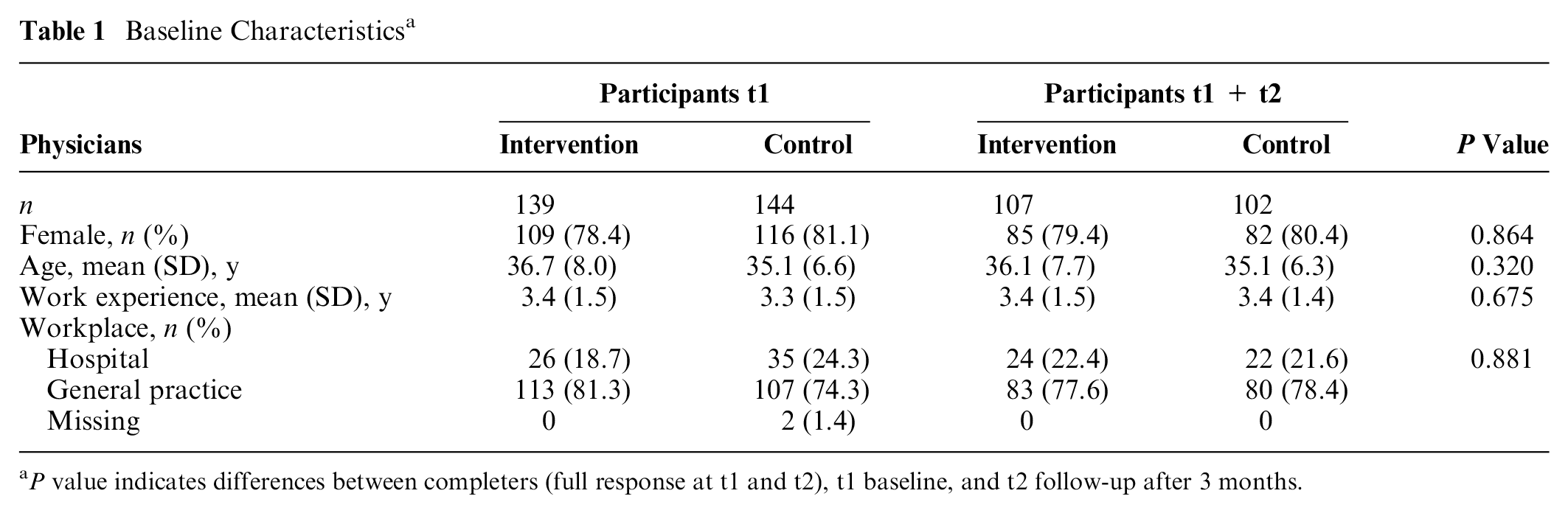
P value indicates differences between completers (full response at t1 and t2), t1 baseline, and t2 follow-up after 3 months.
Factor analysis was only performed with questionnaires without missing values (n = 270). Table 2 shows the results of the maximum likelihood (ML) factor analysis with oblimin-rotation with 3 factors that were extracted, based on the parallel analysis. The EKC suggested 4 factors. We have chosen 3 factors because they are easier to interpret and a more parsimonious model. The item “My diagnostic uncertainty is reduced when guidelines include applicable instructions for making diagnoses” did not fit into any scale. The problem with the item was that it loaded negatively with the third factor and very low on the other factors, which was not expected. The factor analysis showed a U-shaped relationship between the “guideline” item and the other items of the Diagnostic Action scale. Therefore, we analyzed the relationship between the answer options for the “guideline” item (independent variable) with the other scales (as dependent variables) (Table 3). We found that residents with very high and very low agreement with the item “My diagnostic uncertainty is reduced when guidelines include applicable instructions for making diagnoses” showed higher anxiety and concern about bad outcomes, and they had higher scores in the Diagnostic Action scale. Greater agreement with this item was related to higher levels in the Diagnostic Reasoning scale, whereas low agreement was related to lower levels in that scale.
Factor Analysis with All Items of the Dealing with Uncertainty Questionnaire (DUQ)
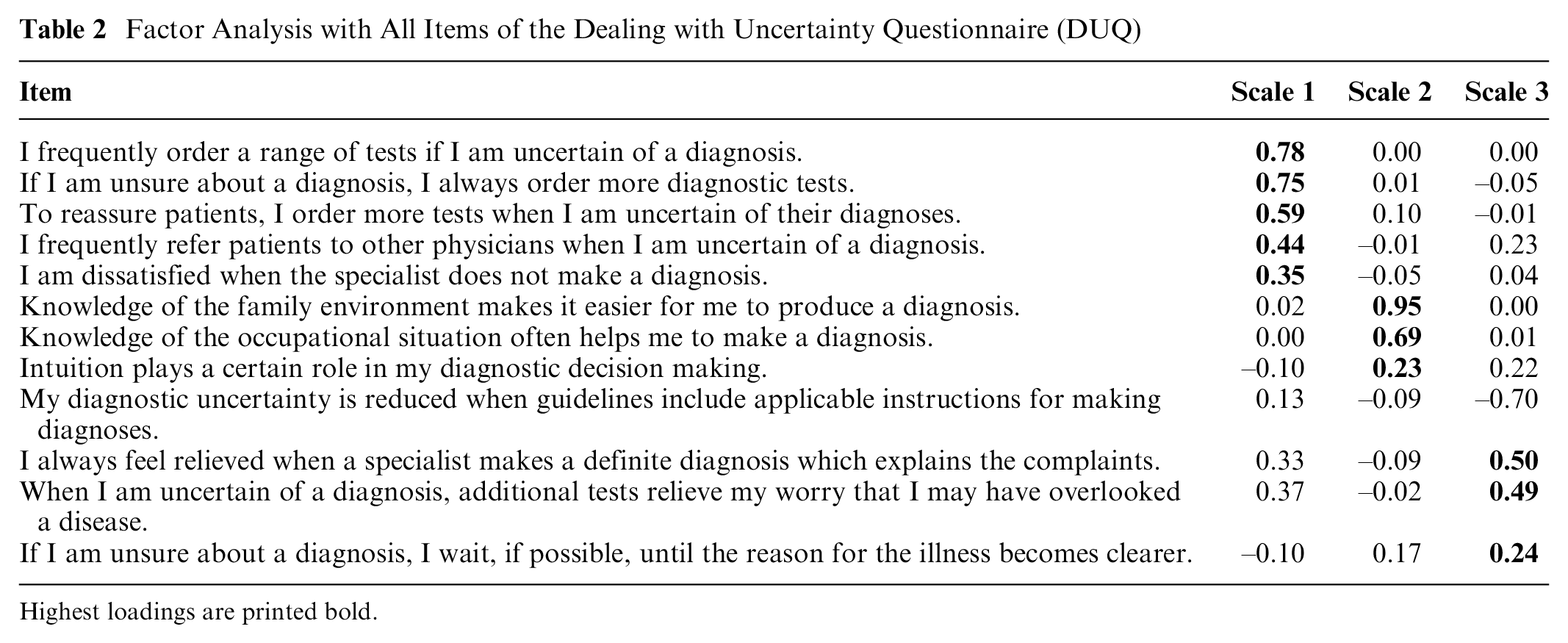
Highest loadings are printed bold.
Mean of the PRU and DUQ Scales (Dependent Variable) as a Function of the Answer Options of the Item “My Diagnostic Uncertainty Is Reduced When Guidelines Include Applicable Instructions for Making Diagnoses” (Independent Variable) a
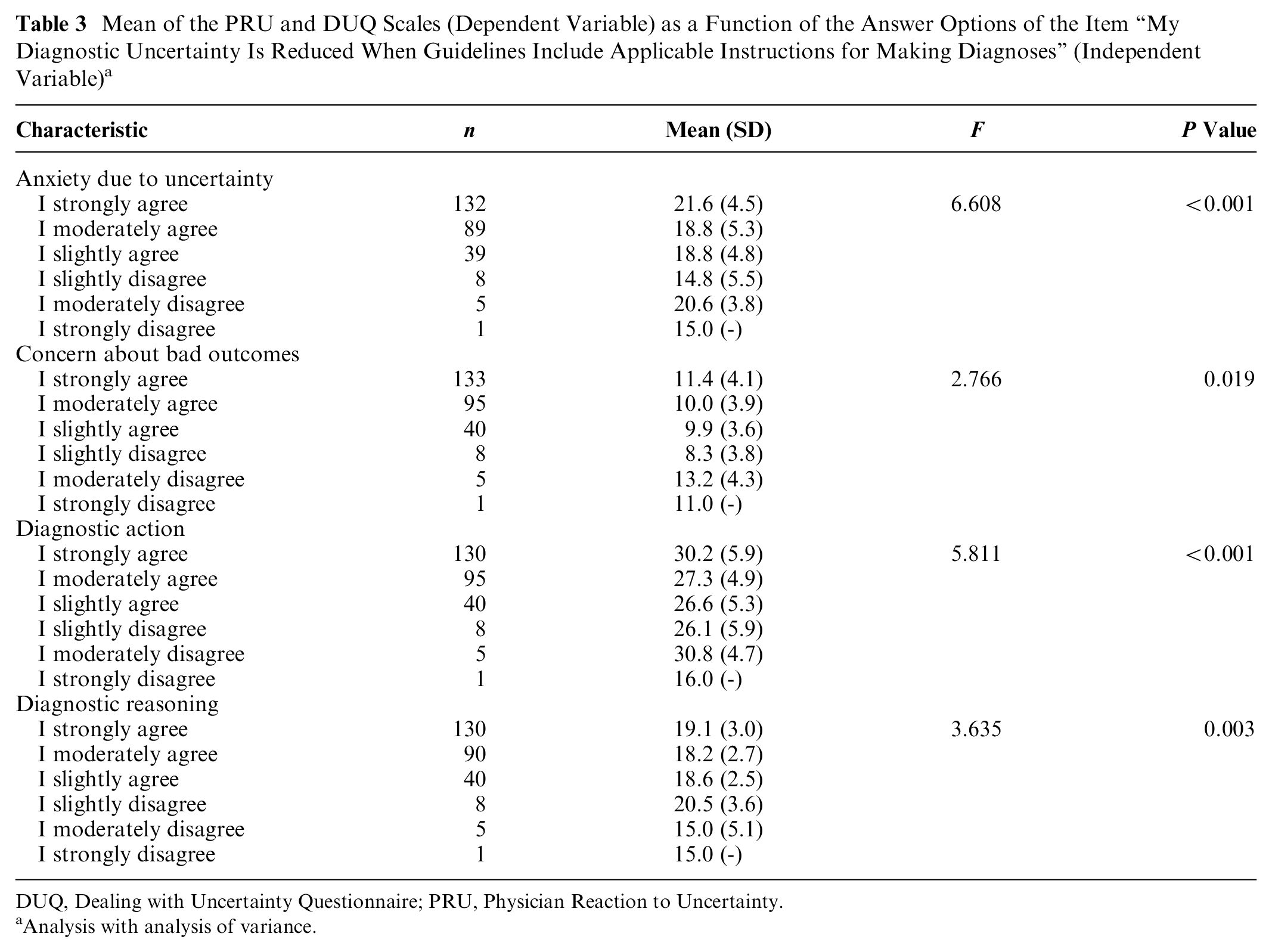
DUQ, Dealing with Uncertainty Questionnaire; PRU, Physician Reaction to Uncertainty.
Analysis with analysis of variance.
With the aim of replicating the Diagnostic Action scale and the Diagnostic Reasoning scale, we repeated the analysis without the “guideline” item. Both the parallel analysis and the EKC suggested 3 factors. The ML factor analysis with oblimin rotation based on polychoric correlations is shown in Table 4. This second analysis showed a satisfying grouping of the Diagnostic Action scale (items 1–7) with a Cronbach’s α of 0.76 (95% confidence interval [CI], 0.71–0.80). This scale comprises different questions regarding intention to request tests and referrals. The Diagnostic Reasoning scale includes items that extended the anamnesis to include familial and occupational circumstances, which reflects the biopsychosocial model of medicine. The 2 items that described “the role of intuition” and a “test-of-time” strategy were also grouped in this scale. However, the Diagnostic Reasoning scale showed less satisfying results with a Cronbach’s α of 0.59 (95% CI, 0.49–0.67), which corresponds with previous results. 24 The item “I always feel relieved when a specialist makes a definite diagnosis which explains the complaints” was grouped as a distinct factor, which contradicts previous findings. 24 One explanation for the distinct grouping might be that this item is more emotionally pronounced than the other items of the scale. This item was not included for further analysis.
Factor Analysis of the Dealing with Uncertainty Questionnaire without the Item “My Diagnostic Uncertainty Is Reduced When Guidelines Include Applicable Instructions for Making Diagnoses”
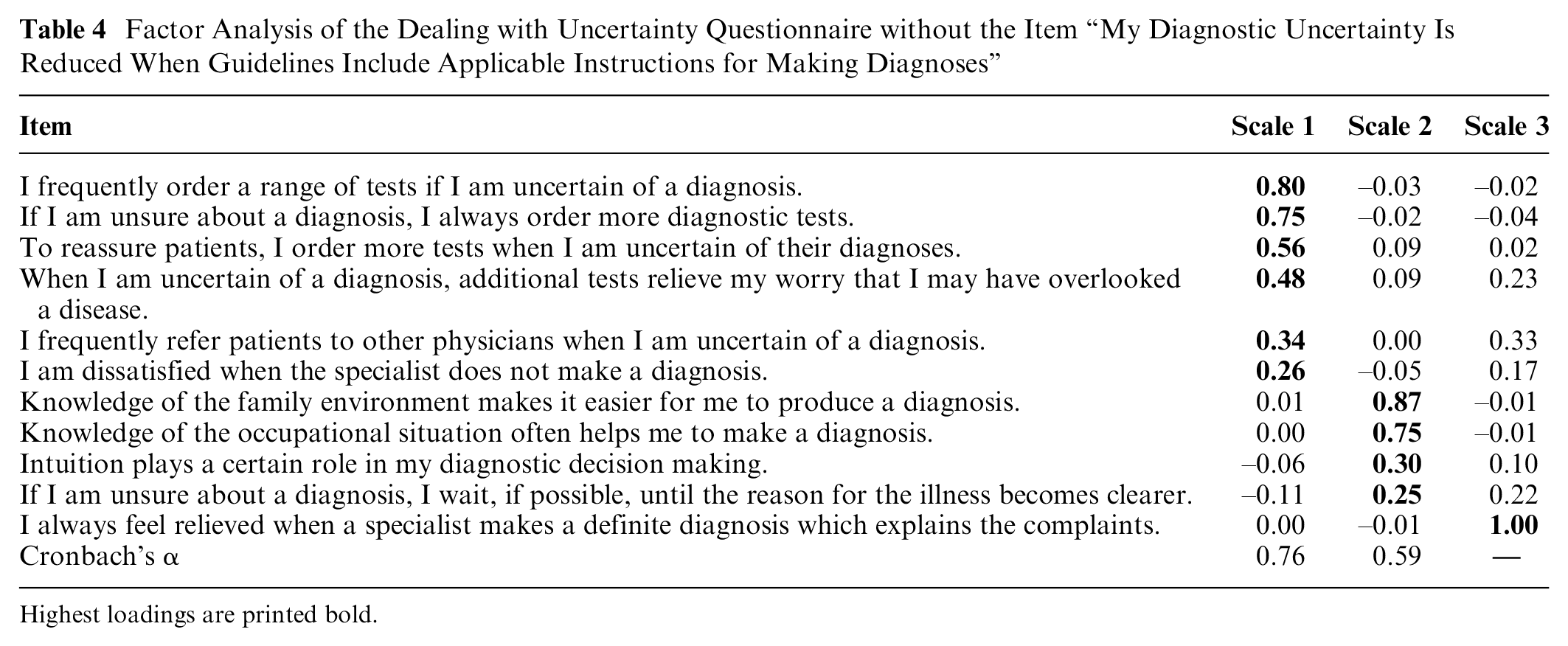
Highest loadings are printed bold.
There was no significant relationship between duration of work experience and the scales of the PRU and the final scales of the DUQ (Table 5). Females showed a trend toward higher Anxiety Due to Uncertainty (P = 0.057) and Concern about Bad Outcomes (P = 0.024). Reluctance to Disclose Uncertainty to Patients (P = 0.012) was also increased in females, as well as the mean of the Diagnostic Action scale (P = 0.029).
Relationship between PRU and DUQ Scales and Gender and Years of Work Experience a
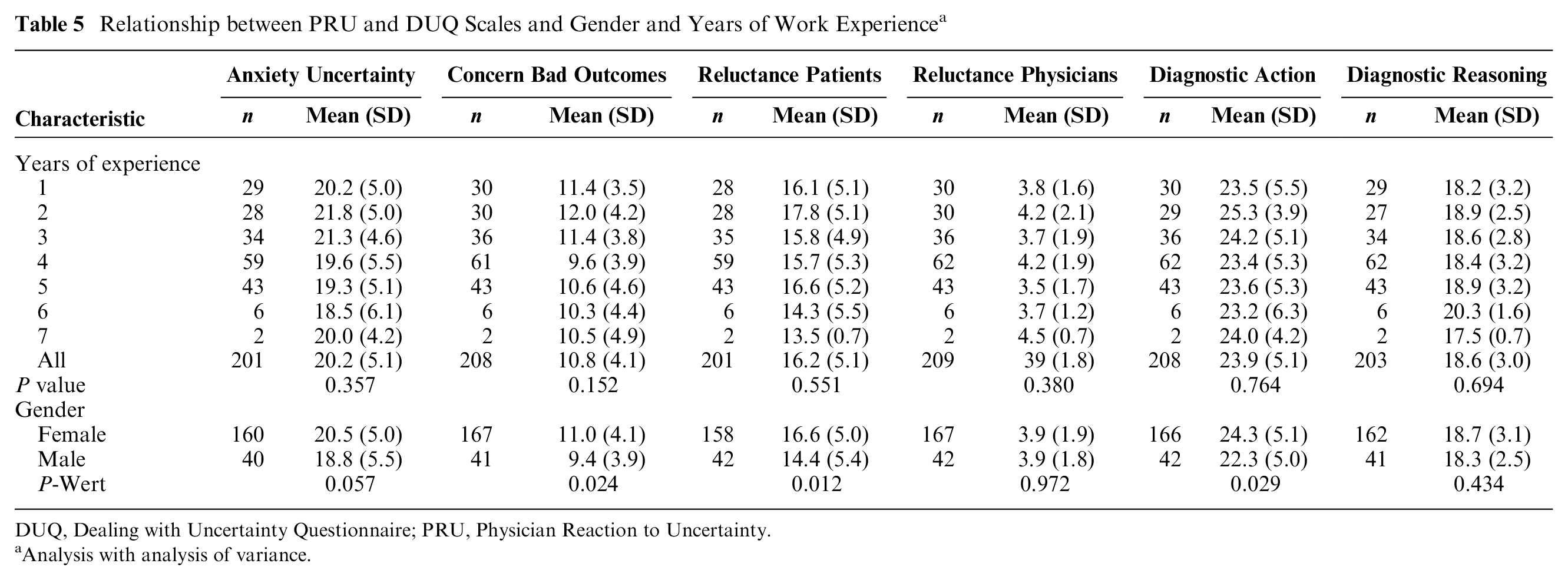
DUQ, Dealing with Uncertainty Questionnaire; PRU, Physician Reaction to Uncertainty.
Analysis with analysis of variance.
The change in the final DUQ and PRU scales is illustrated in Figure 2. The mean (SD) Diagnostic Action scale score decreased from 24.0 (4.8) to 22.9 (5.1) in the intervention group and increased slightly in the control group from 23.7 (5.4) to 24.1 (5.4). These changes were significantly different between the groups (P = 0.006). The Diagnostic Reasoning scale increased from 19.2 (2.6) to 19.7 (2.4) in the intervention group and from 18.1 (3.3) to 18.8 (3.2) in the control group, showing a time effect (P = 0.025) without significant group difference (P = 0.616). The PRU scale Anxiety Due to Uncertainty decreased in the intervention group from 20.5 (4.8) to 18.5 (5.5) and in the control group from 19.9 (5.5) to 19.0 (6.0), also showing a time effect (P = 0.029) without a significant group difference (P = 0.116). There were no significant changes in the other scales. Details are depicted in Supplemental Table S1.
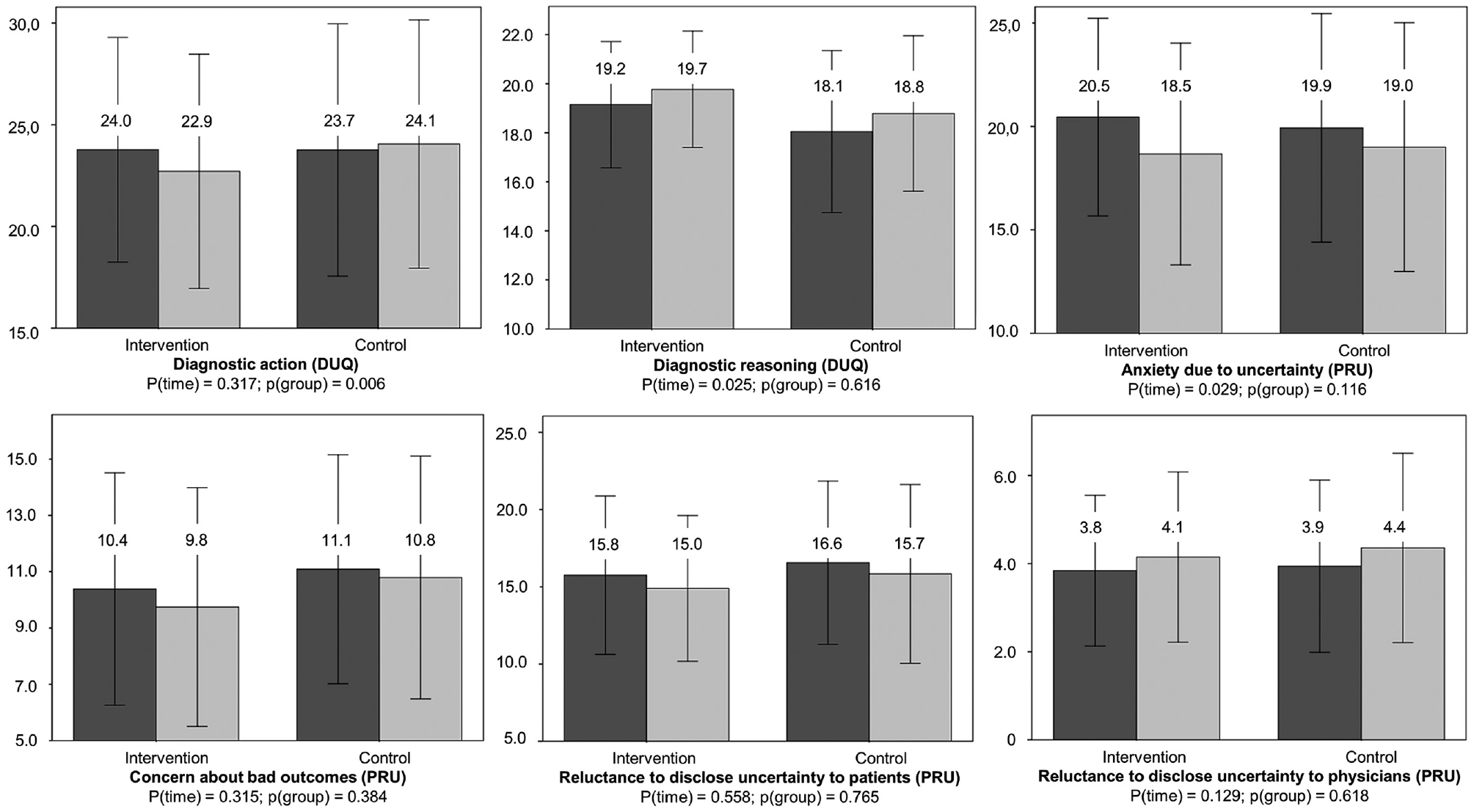
Differences between intervention and control groups with respect to the change in scales of the Dealing with Uncertainty Questionnaire (DUQ) and Physicians’ Reaction to Uncertainty (PRU) questionnaire. Values are mean; bars are standard deviation; blue column = baseline evaluation; green column = follow-up after 3 months.
Discussion
To our knowledge, this is the first controlled trial to evaluate the impact of an interventional education on attitudes to uncertainty and diagnostic test requisition. We found that self-reported diagnostic action-taking decreased in the intervention group but not in the control group. Diagnostic reasoning increased and anxiety due to uncertainty decreased significantly in both groups.
The in-depth explanation of the statistical relationship between pretest probability and positive and negative predictive values as described by the Bayes’s theorem, in combination with stimulated group discussion within the “fish bowl” concept, might have led to a reflection process and increased awareness regarding test requisition. These results are in line with the findings of the single-armed study by Morgan et al., 19 who detected a change in attitude through statements like “I believe that over-testing is a problem in Australian practice,” or “I believe that tests can lead to harm to patients.” Our evaluation with a specific questionnaire shows that these changes in mind-set are likely tied to the seminar, as we did not identify this development in the control group. The self-rated diagnostic action increased in the control group, even though diagnostic aspects were also touched on in their seminars. This might serve as a hint that specific seminars are needed to reduce overtesting. Interestingly, the “anxiety due to uncertainty” decreased in both groups. This might be an unspecific accompanying effect of extra-occupational seminars, but it might also be attributed to a learning process in the primary care environment. Obviously, female physicians seemed to feel more uncomfortable with diagnostic uncertainty. These characteristics should be considered in further studies, particularly with respect to the design of educational interventions to optimize individual learning.
The desired result regarding test requisition was to stimulate a positive attitude toward “dealing with uncertainty in primary care,” thereby encouraging stepwise diagnostic testing to reduce overtesting, and to increase tolerance to diagnostic uncertainty. Uncritical test requisition is not only costly but might also be harmful to patients due to the increased rate of false-positive results in the case of overtesting. 32 In this context, the questionnaire results are helpful to understand the attitudes of the young physicians. The statement “My diagnostic uncertainty is reduced when guidelines comprise applicable instructions for making diagnosis” did not fit into any scale, contrary to our initial expectations. 24 Therefore, we decided to leave this item out because of nonconformity. In-depth analysis might explain the nonfitting structure of this item, because it showed a U-shaped relationship between this item and anxiety due to uncertainty, concern about bad outcomes, and diagnostic action, and high agreement was related to higher levels on the Diagnostic Reasoning scale. It appears that increased aversion toward uncertainty is associated with both increased and reluctant guideline orientation. The test properties of the Diagnostic Reasoning scale remained similar, including the relationship between “test of time” and “intuition.” 24 Thus, a coincidental finding seems unlikely, and the initial estimation that the “test-of-time” strategy could contribute to a simple heuristic that fits well with the Bayes’s theorem by enhancing pretest probabilities with a watchful waiting approach might hold true. The mean of this scale increased without group differences. Similar to Anxiety Due to Uncertainty, changes in diagnostic reasoning might be influenced by the learning process in the practical setting or in an unspecific manner by the seminars.
The more than 30-year-old dictum of “our stubborn quest for diagnostic certainty” 32 is of growing importance in modern medicine with its increasing but often poorly evaluated diagnostic methods. Actually, it is advocated that competency in dealing with uncertainty should receive more attention and that diagnostic reasoning, the possibility that there may be more than one right answer, and consideration of our patients’ values need greater emphasis. 1 Our results might serve as a hint that attitudes toward uncertainty and test requesting could be modified with structured seminars. Further research including clinical outcomes (e.g., with real test frequencies) is needed to evaluate to which extent these kinds of seminars for FMRs lead to an improved adaption to the “real world of primary care.” Beyond that, the integration of further diagnostic reasoning aspects like the concepts of the hypothetico-deductive method and pattern recognition, 33 as well as “inductive foraging” and “triggered routines,” 34 into the curriculum might be valuable to optimize diagnostic management in primary care.
There are some limitations to discuss. First, the results are based on self-estimation through the questionnaire, and a social desirability bias on the part of the responders cannot be excluded. The intervention might have resulted in reported attitudinal change without a change in real behavior. Second, it is difficult to estimate the real impact on resource use, because the differences between the scales were not very large, although they were statistically significant. However, formal educational interventions as reported here are only part of the professional socialization of young physicians. In the long run, they might contribute to a change of attitude, values, and behaviors of the profession as a whole. Third, the DUQ’s Diagnostic Reasoning scale showed low Cronbach’s α. This points to the fact that the construct is not satisfactorily saturated. Fourth, the reanalysis showed that the item “I always feel relieved when a specialist makes a definite diagnosis which explains the complaints” was grouped as a distinct factor. Further research would be necessary to identify more items to saturate this factor. However, this did not hamper our results regarding the group difference in diagnostic action taking. We suggest reevaluating the internal consistency when the DUQ is used in further studies. Fifth, it was not possible to perform randomization. It is unlikely that this distorted the results, as FMRs registered for the courses without in-depth knowledge of the content. Sixth, control group FMRs were less responsive to follow-up. Assuming that the more motivated FMRs responded, it seems likely that the results underestimated the effect of the seminar.
To conclude, a structured seminar on the issue of dealing with uncertainty in primary care reduced self-rated diagnostic test requisition. The reduction in anxiety due to uncertainty and increase in the Diagnostic Reasoning scale might be an unspecific accompanying effect of extra-occupational seminars for FMRs. Alternatively, this effect may be due to a learning process in the primary care environment, which deserves further study to enhance and optimize learning processes in primary care.
Supplemental Material
sj-docx-1-mdm-10.1177_0272989X21989692 – Supplemental material for Educational Intervention Reduced Family Medicine Residents’ Intention to Request Diagnostic Tests: Results of a Controlled Trial
Supplemental material, sj-docx-1-mdm-10.1177_0272989X21989692 for Educational Intervention Reduced Family Medicine Residents’ Intention to Request Diagnostic Tests: Results of a Controlled Trial by Antonius Schneider, Markus Bühner, Therese Herzog, Siona Laverty, Stefanie Ziehfreund, Alexander Hapfelmeier, Dagmar Schneider, Pascal O. Berberat and Marco Roos in Medical Decision Making
Footnotes
Acknowledgements
We thank all participating trainees of the Bavarian vocational training scheme. The “Competence Centre for Residency Training in Family Medicine Bavaria” (CCRTB)—Kompetenzzentrum Weiterbildung Allgemeinmedizin Bayern (KWAB)—is a corporation of the Bayerische Landesärztekammer (Bavarian doctors chamber), Kassenärztliche Vereinigung Bayerns (Bavarian Association of Statutory Health Insurance Physicians), Koordinierungsstelle Allgemeinmedizin Bayern (Bavarian Coordination Unit Family Medicine), Bayerischer Hausärzteverband (Association of Bavarian General Practitioners/Family Physicians), Junge Allgemeinmedizin Deutschland (Association of Trainees and Newly Qualified General Practitioners/Family Physicians Germany), and the 4 Departments of General Practice/Family Medicine of the Bavarian Universities. Members of the Bavarian Competence Center for Residency Training (BCCRT) Network include Ildikó Gagyor, Jochen Gensichen, Thomas Kühlein, Marco Roos, Antonius Schneider, Dagmar Schneider, and Anne Simmenroth.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided in part by the government agency Kompetenzzentrum Weiterbildung Allgemeinmedizin Bayern (KWAB). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.