
Abstract
Background
Informal caregivers often serve as decision makers for dependent or vulnerable individuals facing health care decisions. Decision regret is one of the most prevalent outcomes reported by informal caregivers who have made such decisions.
Objective
To examine levels of decision regret and its predictors among informal caregivers who have made health-related decisions for a loved one.
Data sources
We performed a systematic search of Embase, MEDLINE, Web of Science, and Google Scholar up to November 2018. Participants were informal caregivers, and the outcome was decision regret as measured using the Decision Regret Scale (DRS).
Review methods
Two reviewers independently selected eligible studies, extracted data, and assessed the methodological quality of studies using the Mixed Methods Appraisal Tool. We performed a narrative synthesis and presented predictors of decision regret using a conceptual framework, dividing the predictors into decision antecedents, decision-making process, and decision outcomes.
Results
We included 16 of 3003 studies identified. Most studies (n = 13) reported a mean DRS score ranging from 7.0 to 32.3 out of 100 (median = 14.3). The methodological quality of studies was acceptable. We organized predictors and their estimated effects (β) or odds ratio (OR) with 95% confidence interval (CI) as follows: decision antecedents (e.g., caregivers’ desire to avoid the decision, OR 2.07, 95% CI [1.04–4.12], P = 0.04), decision-making process (e.g., caregivers’ perception of effective decision making, β = 0.49 [0.05, 0.93], P < 0.01), and decision outcomes (e.g., incontinence, OR = 4.4 [1.1, 18.1], P < 0.001).
Conclusions
This review shows that informal caregivers’ level of decision regret is generally low but is high for some decisions. We also identified predictors of regret during different stages of the decision-making process. These findings may guide future research on improving caregivers’ experiences.
When making health-related decisions, feelings of being uninformed, unsupported, or unclear about personal values may lead to regret or blame. 1 Decision regret is a prevalent patient-reported outcome measure defined as “remorse or distress over a decision.” 2 Even though there is no consensus on a specific cutoff point for clinically significant decision regret, higher Decision Regret Scale (DRS) scores have been associated with worse health outcomes, self-blaming, and reduced quality of life.2–8 Decision regret is considered an essential measure of the quality of a decision and is of increasing interest to clinicians. 2
Decision making in health care settings can be challenging for vulnerable care recipients such as cognitively impaired persons or children. 9 When they are not able to make informed decisions about their own health conditions, they often rely on a family caregiver to help them. Family caregivers (or informal caregivers) include family, close relatives, friends, and/or neighbors who provide unpaid care to someone close to them, in contrast to a formal caregiver, who provides paid care services.10–15 Family caregivers 11 play an invaluable role in the health care system and benefit society and government budgets by providing unpaid care and psychological support to a person in need with whom they maintain a personal relationship. 10 They may also help care recipients make preference-sensitive decisions in a variety of clinical contexts.10,16,17 Research has characterized the experience of informal caregivers as stressful and burdensome,18–20 including when serving as health care decision makers for care recipients. 21 In addition, evidence has shown that whenever decision outcomes fail to satisfy patients, those involved in the decision-making process may experience decision regret.2,22 Informal caregivers are thus at increased risk of experiencing decision regret.23,24
Although there have been studies on decision regret following health-related decisions, few studies have shown how decision regret affects informal caregivers who make health decisions for their loved ones. 4 Evaluating regret among informal caregivers could help determine where additional support is needed.1,2,25–27 We therefore aimed to review levels of decision regret among informal caregivers making proxy health-related decisions and to identify predictors of this regret.
Methods
We report this review according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement. The protocol was not registered. 28
Eligibility Criteria
Eligibility criteria were defined according to the PICOS approach: Population (P): informal caregivers (i.e., a person who provides direct and unpaid care for children, elderly people, or other care recipients with any health condition) who have made a health-related decision for a loved one11,29–31; Intervention/Exposure (I): any risk factor of decision regret; Comparator (C): no restrictions; Outcome (O): decision regret measured with the validated DRS reported as the primary or secondary outcome2,4,25; and Study Design (S): no restrictions. The DRS is a 5-point Likert-type scale that is reliable, validated, and widely used. It was developed and tested specifically for health care settings.4,25 There were no restrictions on year of publication, setting, or language.
Information Sources and Searches
An information specialist (N.R.) developed the search strategy and discussed it with the authors. We considered any type of document or study specifications except editorials, letters, abstracts, protocols, and systematic reviews. Search terms included “decision making or choice or judgment or decision or choice or judgment” and “regret or remorse or negative emotion or self-blame or treatment* near/2 regret.” (Supplementary File 1). Articles published up to November 2, 2018, were identified using EMBASE and MEDLINE. A reverse search was performed in Web of Science (up to November 2, 2018) and Google Scholar (up to November 6) to identify articles related to the DRS. We also searched published bibliographies of related studies and bibliographic reference lists of relevant literature reviews.4,25,32,33
Study Selection
After eliminating duplicates, 2 reviewers (H.E. and T.T.A.) independently retrieved the unique citations obtained from the chosen data sources. In step 1, titles and abstracts of unique citations were selected according to inclusion criteria. In step 2, reviewers read full texts to make the final study selection. Disagreements were resolved through discussion between the reviewers.
Data Extraction
Using an extraction grid (Supplementary File 2) used successfully by our team, 4 we extracted the following information: 1) study characteristics (first author’s name, year of publication, country, total number of participants, study design, decision type, and clinical context), 2) participant characteristics (age, proportion of women, participant follow-up period, and response rate), 3) the DRS (psychometric characteristics of the sample of each included study, mean of DRS scores and range, proportion of participants with decision regret), 4) potential predictors for decision regret identified from variables used in statistical models (name of any variable significantly associated or not with decision regret, measurements, type of regression model used, potential predictor effect, 95% confidence interval, P value), and 5) the quality of studies (see details below). Two reviewers (H.E. and T.T.A.) independently extracted data after a conclusive pilot test. Discrepancies were discussed between reviewers and resolved by consensus with a third reviewer (R.A.).
Methodological Quality Assessment of Individual Studies
Two independent reviewers (H.E. and R.A.) assessed the quality of each identified study using the Mixed Methods Appraisal Tool, 34 a validated tool for evaluating the quality of qualitative, quantitative, and mixed methods studies. 34 H.E. and R.A. discussed discrepancies and resolved them by consensus.
Data Synthesis
Given the clinical, methodological, and statistical heterogeneity of studies included, we performed a narrative synthesis using the results of descriptive analyses from data extracted. We used tables and charts to summarize the results. We performed data synthesis in 6 steps. First, we described the selection process using a flow chart. Second, we compared the studies according to the type of decision made (e.g., treatment, screening), the clinical context in which studies were conducted (e.g., oncology, geriatrics), and the analytical approaches used (e.g., descriptive analysis, multivariate model). Third, we described the methodological quality of the studies, rating criteria according to study design. Fourth, we analyzed how the authors reported the DRS results (e.g., mean score, proportion). Fifth, we compared levels of decisional regret reported (no regret, mild regret, and moderate to strong regret). Lastly, we used a conceptual framework of the decision-making process designed by Sepucha and Mulley to classify the various potential predictors of decisional regret (decision antecedents, decision-making process, and decision outcomes).35,36 We also explored individual studies to contextualize results at each step.
Role of Funding Body
Other than providing financial support, the Canada Research Chair in Shared Decision Making and Knowledge Translation played no role in this review. The information in this article is the responsibility of the authors alone.
Results
Study Selection and Study Characteristics
Among the initial 3003 citations identified, we removed 1392 duplicates and screened 1611 titles/abstracts (Figure 1). A total of 1448 did not meet our inclusion criteria. Thus, we screened 163 full texts, and 16 articles were included in our review.23,24,35,37–48
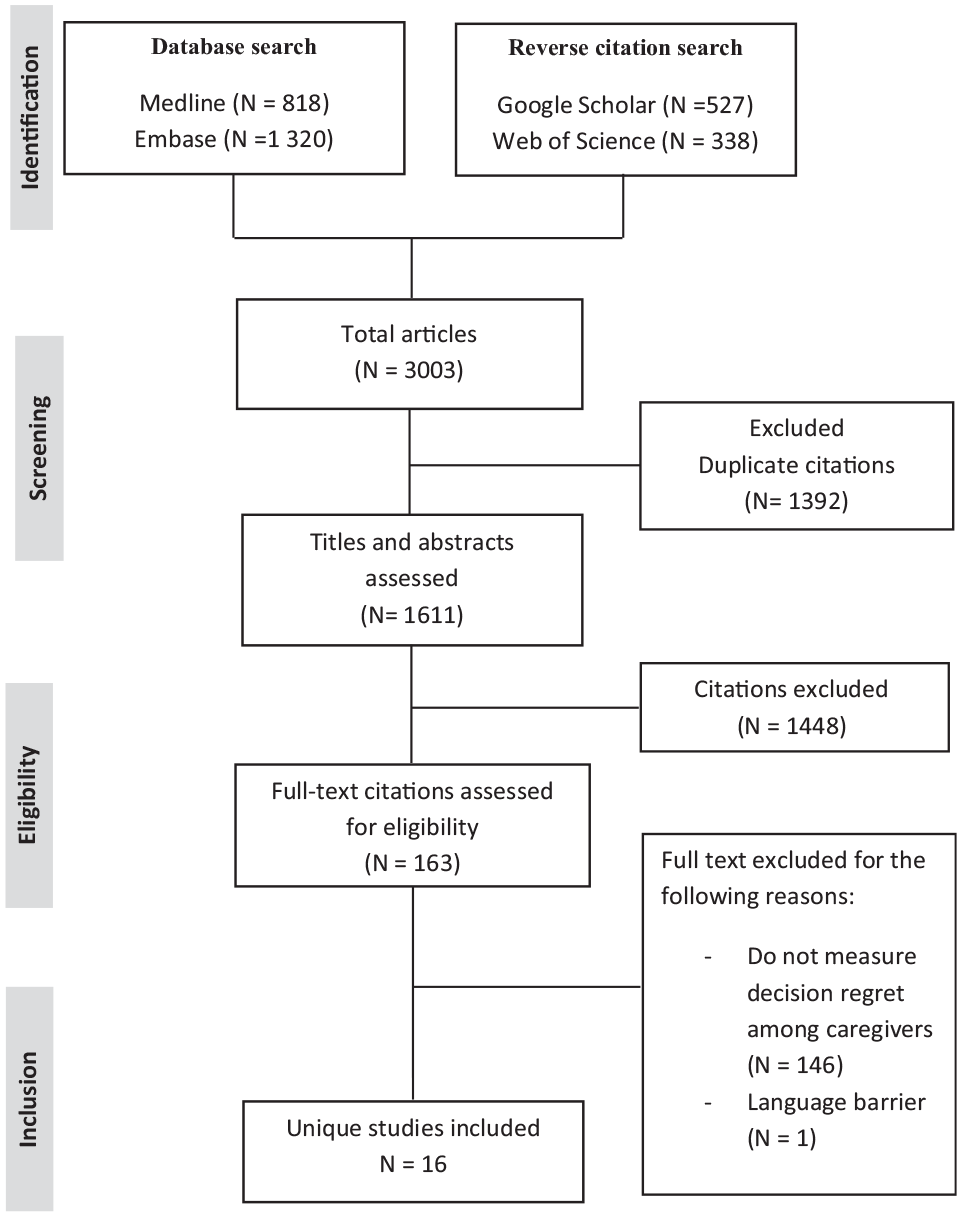
Flow chart of study inclusion process.
Studies were published in English between 2011 and 2018 and conducted in 5 countries: the United States (n = 11),23,24,37–45 Canada (n = 2),35,45 the United Kingdom (n = 1), 46 Italy (n = 1), 47 , and South Korea (n = 1) 48 (Table 1). Study designs included 7 cross-sectional,24,35,37,38,44,46,47 3 mixed methods,39,40,43 2 cohorts,23,41 2 randomized clinical trials (1 randomized cluster trial),48,49 and 2 nonrandomized clinical trials.42,45 Studies included from 16 to 444 individuals in total (caregivers and care recipients). They included from 15 to 444 caregivers (median = 83) of both sexes, except for 1 study conducted exclusively with women. 23 The mean age of the caregivers ranged from 30.9 to 62 y (median age = 54 y). Decisions were made in a variety of contexts: intensive care,24,37,41,42 oncology,43,46,48 surgery or urology,44,45,47 genetics,23,38 pediatrics, 39 geriatrics, 49 cardiology, 40 and primary care. 35 The most frequently reported psychometric characteristic of the DRS was the Cronbach’s alpha coefficient, which ranged from 0.44 to 0.92 (median = 0.75). Only 3 studies assessed the decisional regret score longitudinally over a 6-mo period,41,42,48 finding no significant change overall. One of these, a randomized controlled trial comparing a letter of condolence (control) to the letter and storytelling (intervention), showed some decrease in the DRS score in some patients in the intervention group. 42
Study and Participant Characteristics (n = 16 Studies)
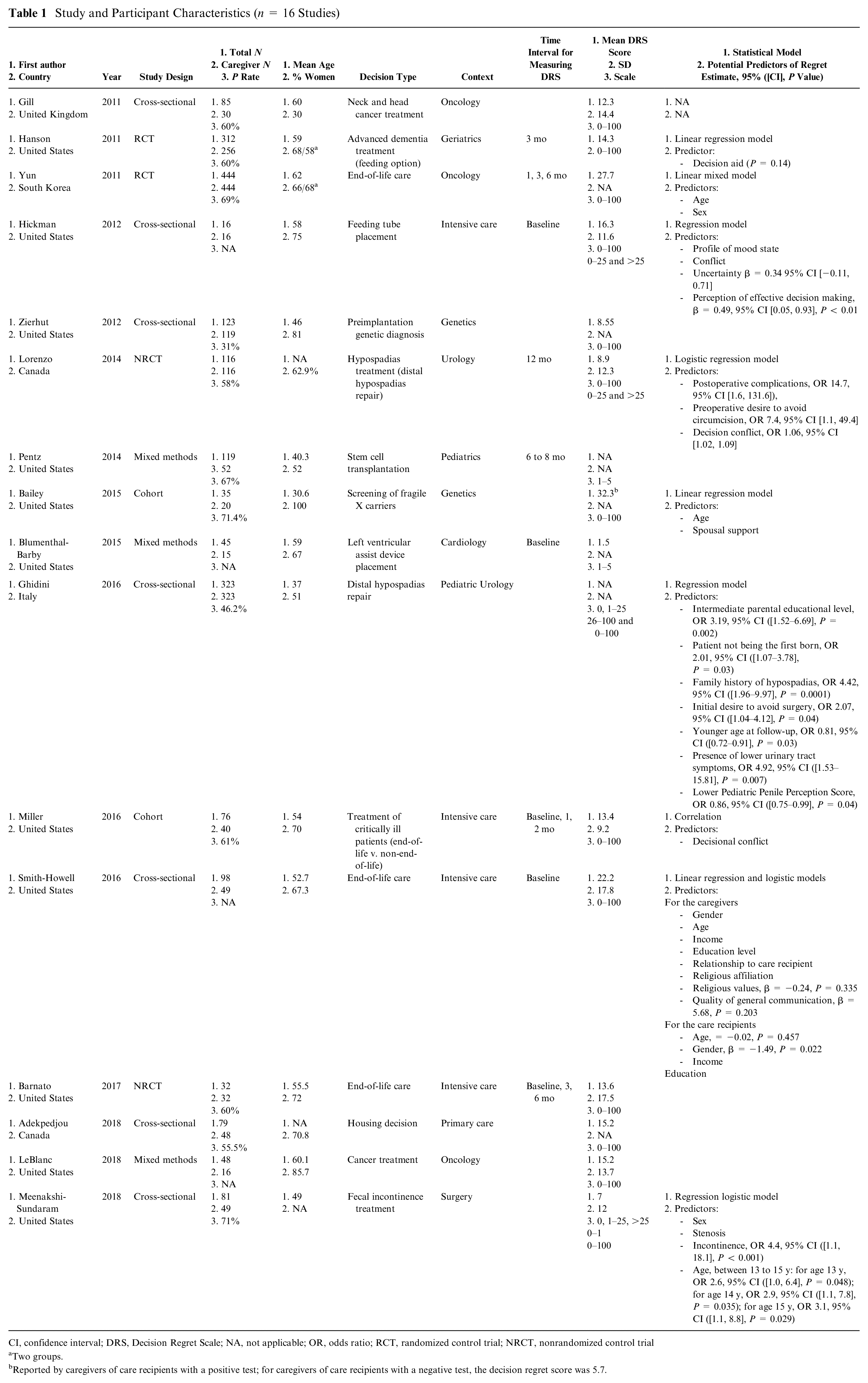
CI, confidence interval; DRS, Decision Regret Scale; NA, not applicable; OR, odds ratio; RCT, randomized control trial; NRCT, nonrandomized control trial
Two groups.
Reported by caregivers of care recipients with a positive test; for caregivers of care recipients with a negative test, the decision regret score was 5.7.
Types of Decisions Made
Informal caregivers were involved in 6 types of decisions for their loved ones (Figure 2): 1) decisions about a treatment other than cancer (e.g., surgery), reported in 4 of 16 studies39,44,45,47; 2) decisions about end of life, in 4 studies24,41,42,48; 3) decisions about the implementation of an assistive device (e.g., cardiac device), in 3 studies37,40,49; 4) screening or diagnostic decisions, in 2 studies23,38; 5) decisions about cancer treatment, in 2 studies43,46; and 6) a housing decision, in 1 study. 35 All studies were focused on decision making and more than half on shared decision making (see Table 1).
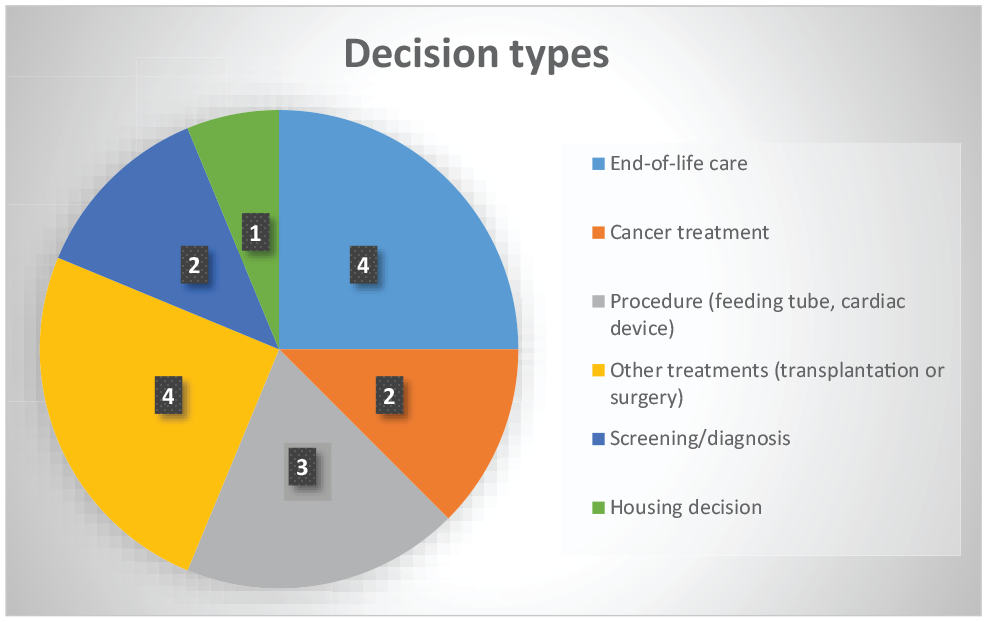
Distribution of decisions faced by informal caregivers (n = 16 studies).
Level of Decision Regret and How It Was Reported
In total, 13 of 16 studies reported the DRS score on a continuous scale of 0 to 100, with scores ranging from 7 to 32.3 (median = 14.3)23,24,35,37,38,41,43–46,48,49 (Table 1; Supplementary File 3). In a randomized controlled trial, intervention groups showed slightly lower DRS scores than control groups did. 42 One study reported the score on a continuous scale of 1 to 5 (mean 1.5). 40 One study divided DRS scores into 3 categories (0, 1–25, 26–100) 47 and reported the percentages for each (0: 8.1%, 1–25: 52.3%, and 26–100: 39.6%). Another study used 3 forms to treat DRS scores (0, 1–25, >25; 0–1; 0–100), 44 reporting DRS mean scores of 7 out of 100. Two studies dichotomized DRS (0–25 and >25),37,45 reporting DRS mean scores of 16.5 points 37 and 8.9 points. 45 These studies mixed nonregret (DRS = 0) with presence of regret (DRS > 0). Two studies used both continuous and categorical approaches to DRS scores.37,45
Methodological Quality of Studies
With regard to the methodological quality of individual studies, randomized controlled trial designs48,49 did not meet criteria regarding the completeness of outcome data, participants’ adherence to the assigned intervention, 48 or blinded outcome assessors 49 (Figure 3; Supplementary File 4). Nonrandomized designs23,24,37,42,44–47 did not meet participants’ representativeness criteria regarding42,47 completeness of outcome data criteria45,47 or accountability for confounders in the design.37,46 Descriptive study designs35,38,41 did not meet criteria regarding the risk of nonresponse 35 or sample representativeness criteria. 38 Lastly, mixed-methods designs39,40,43 did not provide adequate rationale for using mixed-method designs39,43 or meet the criteria for effectiveness integration. 40
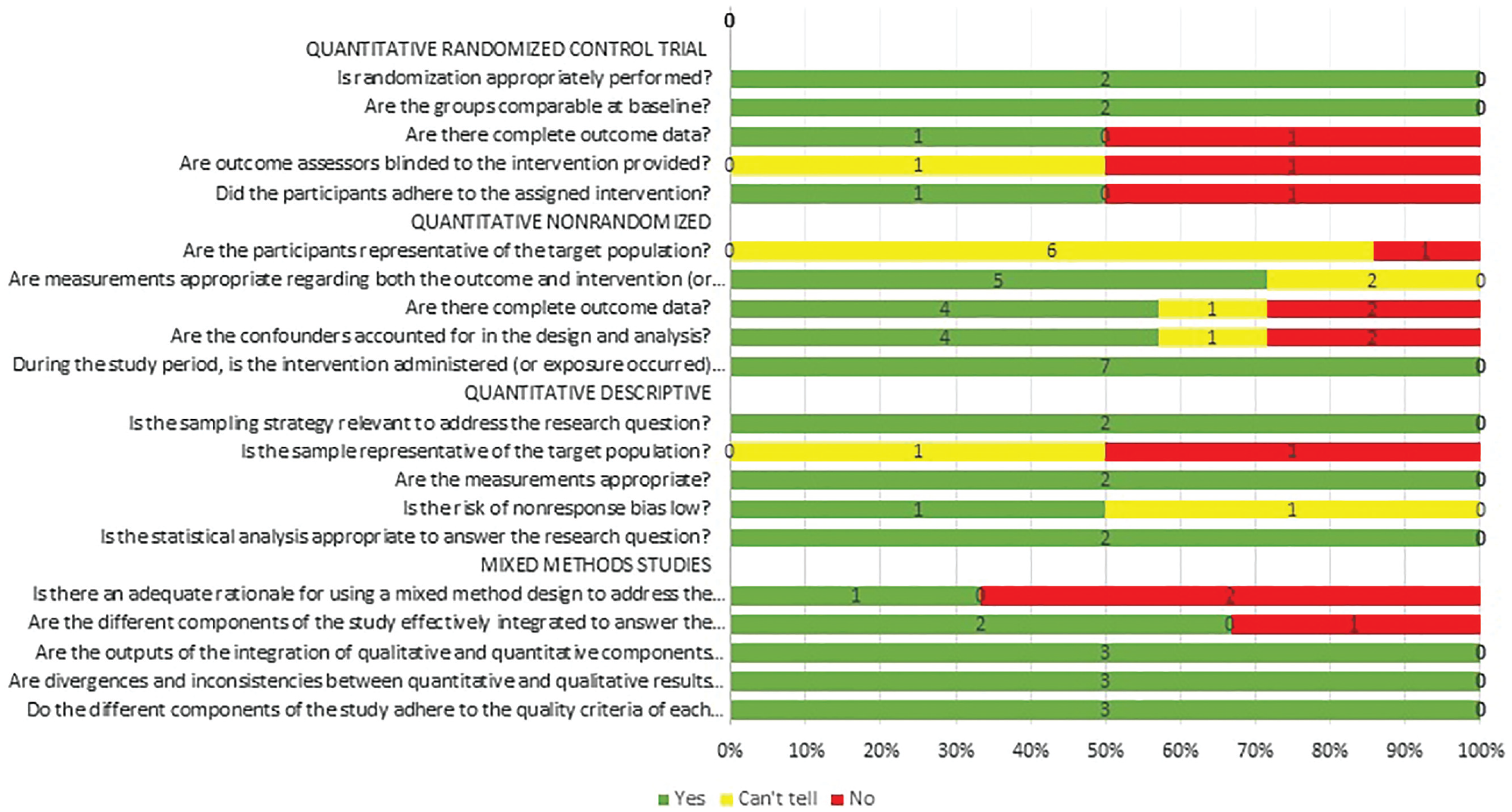
Assessment of the methodological quality of the studies (N = 16 studies).
Predictors of Decision Regret, Models, and Measures Used
Predictors of decisional regret were explored in 9 of the 16 included studies23,24,37,41,44,45,47–49 (Table 1). The authors of 4 of these studies evaluated predictors of the DRS score using a linear regression model,23,24,48,49 4 studies used a logistic regression model,37,44,45,47 1 study used both models, 24 and one study did not mention which model was used. 24 Our model35,36 allowed us to organize predictors of regret into 3 main stages of the decision process: 1) decision antecedents (e.g., age, gender), 2) decision-making process (e.g., decisional conflict), and 3) decision outcomes (e.g., complications; Figure 4).
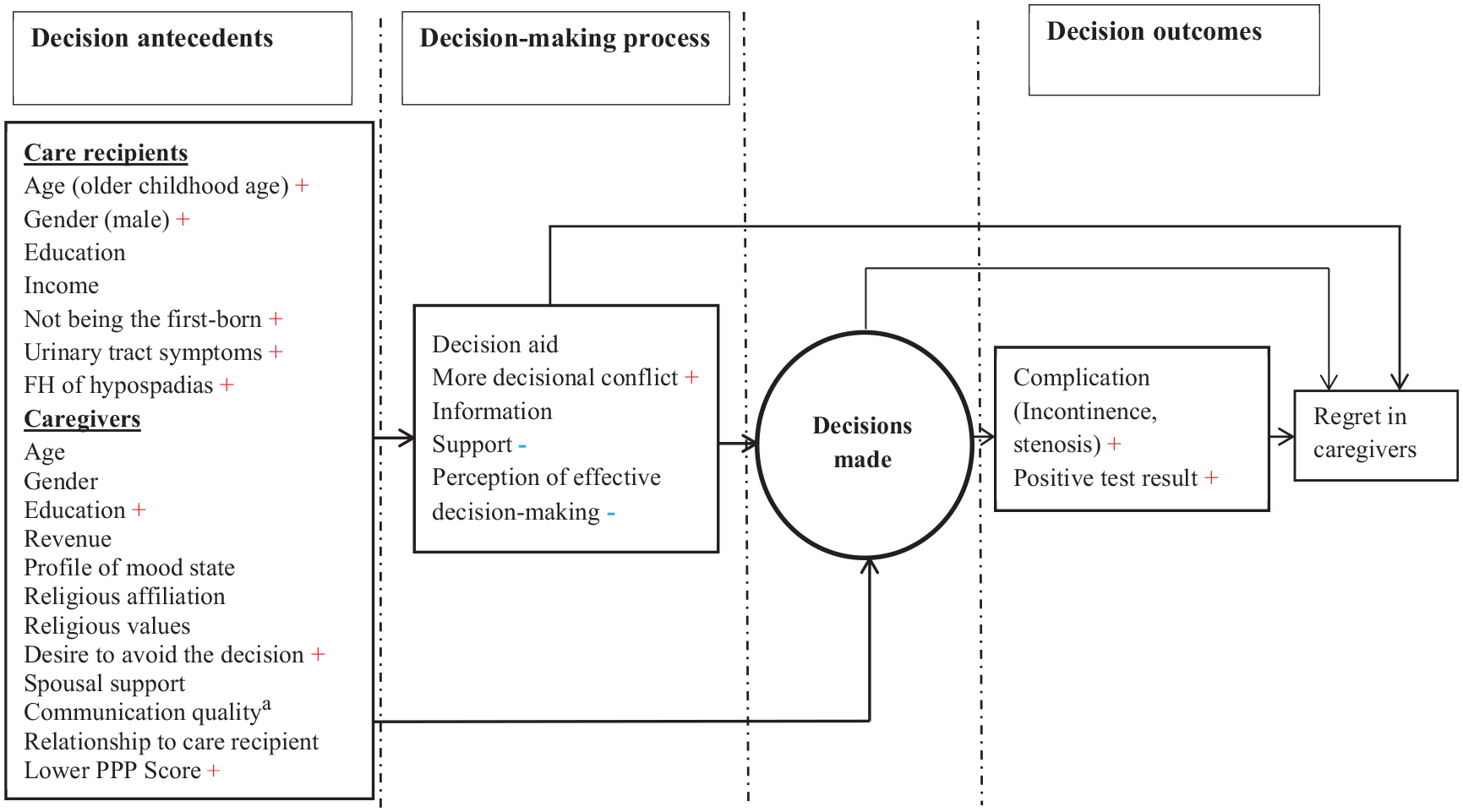
Predictors of decision regret. PPP, Pediatric Penile Perception; FH, Family history; aCommunication quality between caregivers and care recipients; +, the predictor increased regret; −, the predictor decreased regret. No sign means no significant association was found.
Decision antecedents
At this stage, 4 studies assessed the association between care recipients’ or caregivers’ characteristics and decision regret in caregivers by estimating an odds ratio (OR) or β with 95% confidence interval (CI) and P value.24,44,45,47
Among care recipients, the association between age and DRS among caregivers was examined in 3 studies,24,44,47 including 2 studies in a pediatric population. The first showed a steady increase in parental decision regret with their children’s age, increasing from 13 to 15 y: for age 13 y, OR 2.6, 95% CI ([1.0, 6.4], P = 0.048), and for age 15 y, OR 3.1, 95% CI ([1.1, 8.8], P = 0.029). 44 The second pediatric study revealed that higher DRS scores were associated with a younger age at follow-up, OR 0.81, 95% CI ([0.72–0.91], P = 0.03). 47 The third study, conducted among caregivers of adults, found no association between age and DRS (β = −0.02, P = 0.457) but found that being male was significantly associated with regret (β = −1.49, P = 0.022). 24
In one study conducted among parent caregivers, the following factors showed significant association with regret: intermediate parental educational level, OR 3.19, 95% CI ([1.52–6.69], P = 0.002 47 ; care recipient not being the first born, OR 2.01, 95% CI ([1.07–3.78], P = 0.03) 47 ; family history of the disease, OR 4.42, 95% CI ([1.96–9.97], P = 0.0001) 47 ; and presence of clinical symptoms, OR 4.92, 95% CI ([1.53–15.81], P = 0.007). 47
Among caregivers, 3 factors were found to be significantly associated with more decision regret: an intermediate educational level, OR 3.19, 95% CI ([1.52–6.69], P = 0.002) 47 ; an initial desire to avoid surgery, OR 2.07, 95% CI ([1.04–4.12], P = 0.04) 47 ; and a lower surgical outcome appraisal score, OR 0.86, 95% CI ([0.75–0.99], P = 0.04).47,50
Decision-making process (only in caregivers)
Four studies24,37,41,49 examined factors related to the decision-making process that were associated with decision regret among only caregivers. Whereas increased decisional conflict (OR 1.06 [1.02, 1.09]) 45 was associated with more decision regret, caregivers’ perception of effective decision making (β = 0.49 ([0.05, 0.93], P < 0.01) 37 was significantly associated with less decision regret among caregivers.
Decision outcomes (only in care recipients)
Two studies examined the influence of a bad health outcome or complication (e.g., stenosis, incontinence [OR = 4.4 {1.1, 18.1}, P < 0.001])23,44 on decision regret experienced by caregivers.23,44 Both studies found that poor health outcomes were positively associated with decision regret.
Discussion
This review sought to assess the extent and predictors of decision regret among informal caregivers who made health decisions on behalf of a loved one. The methodological quality of the studies was low to moderate overall (Figure 3) but better among mixed-methods studies. Four main conclusions emerged. First, decision regret in caregivers was low overall but high for some decisions. Second, measuring decision regret among informal caregivers appears to be a recent outcome of interest. Third, results suggest that supporting caregivers who are parents is called for, as studies report higher levels and many predictors of regret. Finally, predictors for decision regret emerged mostly from the first stage of the decision-making process (i.e., decision antecedents).
Two hypotheses could explain the low level of regret observed overall. First, many decisions took place in a shared decision-making context, which may have contributed to clarifying values and reducing regret.40,43,49 However, it was not possible to confirm whether or not SDM reduced decision regret, given that we did not collect data that compared studies taking place in a shared decision-making context with those that did not and given that we identified few studies that made this comparison. Second, few studies reported negative outcomes as a result of the decision-making process, so it is possible the others reported outcomes that were mostly satisfactory and led to lower levels of regret.23,44,45 For example, one study reported a significantly higher level of regret following screening decisions when the result was not satisfactory. 23 In addition, some studies reported categorical values that may lead to confusion between no regret (DRS = 0) and a low level of regret. It should be mentioned that while included studies reported low levels of regret, consistent with previous reviews examining the extent of decision regret, DRS scores were difficult to interpret clinically because there is no significant clinical cutoff point for DRS scores.4,51 However, because a DRS score of 30 or higher (out of 100) means people agree that they have experienced some level of regret, 30 of 100 could be considered as a minimal point for clinical concern.2,4 Nevertheless, research is needed to establish a more reliable and meaningful clinical cutoff score.
In our review, we found few studies measuring regret longitudinally at multiple time points, and none measured regret over more than 6 mo. One study reported that even with no significant change between groups, the intervention was beneficial in some cases but only to patients who initially presented highest regret. Furthermore, another study specifically on values clarification showed that regret significantly decreased over time (>1 y) when values were clarified. 52 Our study did not give us much insight into repeated measurement of regret over a long period. Further research is required to better understand the evolution of regret over time.
Measuring decision regret among informal caregivers appears to be a new outcome of interest, as studies are few and recent. Moreover, the topic has been studied exclusively in high-income countries. This finding may be explained by the fact that in low-income countries, it is taken for granted that the burden of caring for the incapacitated is mainly carried by family members and caregivers.53,54 In high-income countries, where the proportion of the population that is older is increasing, policy makers are beginning to notice family caregivers as playing a crucial role in caring for older adults and often in making health-related decisions on their behalf. If these unremunerated caregivers are no longer able to play this role for some reason, their replacement with paid workers can pose significant problems for health care systems. The staffing problems due to the exclusion of informal caregivers from visiting long-term care facilities during the COVID-19 pandemic made this abundantly clear. Moreover, if family caregivers fail to receive the care they need, it is likely that they, too, will need additional health care services.16,35,55–58
In our review, most identified predictors of regret were evaluated in the context of a medical or surgical decision made by a parent caregiver for their child.44,45,47 The highest DRS scores were reported by a study conducted among parent caregivers. 23 Medical or surgical decision making in pediatric care is particularly psychologically burdensome for parent caregivers.59,60 Furthermore, pediatric decision making is complex because of the involvement of parents, health care professionals, and children.21,59–61 Providers must give specific attention and guidance to parent caregivers, especially when involving them in surgical decision making.
Our results reveal that although predictors of decision regret may emerge from different stages of the decision-making process, most predictors we found were in the first stage. Before decision making occurs, predictors of decision regret may derive from caregivers and/or care recipients. For example, in studies conducted among parent caregivers, increased decision regret was associated with older childhood age. 44 Furthermore, our results also show that caregivers’ increased decision regret is associated with an initial desire to avoid making a proxy decision. These caregivers not only regretted the choice they made but also may have regretted not following their initial desire to avoid making a decision altogether. 47 Before a decision-making process take place, it is thus important for providers to evaluate caregivers’ comfort regarding decision making and to empower them so they are more confident to face current and future decisions. During the decision-making process itself, the fact that caregivers’ perception of effective decision making was associated with decreased DRS scores is a clear indication that shared decision making that continues throughout the care path is an effective counterweight to decision regret. At the stage of decision outcomes, complications or a positive test result were associated with increased decision regret. But if a person has been empowered to make effective decisions beforehand, supported through the process, and finally reassured that the best path possible has been taken, the destructive and distressing spiral of decision regret may be averted. 62
Limitations
Our study had certain limitations. First, the heterogeneity of the studies, in terms of their clinical and methodological approaches, made it impossible to conduct a meta-analysis. However, we tried to provide a concise narrative summary of collected data comparing differences and similarities between studies. Second, this review may not reflect all factors influencing regret among caregivers, as we focused on studies using DRS. Finally, as we did not include unpublished studies, we may have omitted some in which caregivers reported high levels of regret.63,64
Conclusion
Our review found that studies conducted among informal caregivers reported a relatively low level of regret. We also identified factors that may influence decision regret, including older childhood age of care recipients, family or medical antecedents, adult care recipients being male, informal caregivers manifesting an initial desire to avoid the decision, decisional conflict, perception of effective decision making and support, and treatment complications. Further research could elucidate links between phases of decision making and the presence of decision regret and determine whether decision support can reduce or alleviate decision regret if provided at all phases of decision making: before, during, and afterward.
Supplemental Material
Elidor_et_al._Revue_Decision_Regret_Supplementary_file_1_20200903.rjf_online_supp – Supplemental material for Extent and Predictors of Decision Regret among Informal Caregivers Making Decisions for a Loved One: A Systematic Review
Supplemental material, Elidor_et_al._Revue_Decision_Regret_Supplementary_file_1_20200903.rjf_online_supp for Extent and Predictors of Decision Regret among Informal Caregivers Making Decisions for a Loved One: A Systematic Review by Hélène Elidor, Rhéda Adekpedjou, HervéTchala Vignon Zomahoun, Ali Ben Charif, Titilayo Tatiana Agbadjé, Nathalie Rheault and France Légaré in Medical Decision Making
Supplemental Material
Elidor_et_al._Revue_Decision_Regret_Supplementary_file_2_20200903.rjf_online_supp – Supplemental material for Extent and Predictors of Decision Regret among Informal Caregivers Making Decisions for a Loved One: A Systematic Review
Supplemental material, Elidor_et_al._Revue_Decision_Regret_Supplementary_file_2_20200903.rjf_online_supp for Extent and Predictors of Decision Regret among Informal Caregivers Making Decisions for a Loved One: A Systematic Review by Hélène Elidor, Rhéda Adekpedjou, HervéTchala Vignon Zomahoun, Ali Ben Charif, Titilayo Tatiana Agbadjé, Nathalie Rheault and France Légaré in Medical Decision Making
Supplemental Material
Elidor_et_al._Revue_Decision_Regret_Supplementary_file_3_20200903.rjf_online_supp – Supplemental material for Extent and Predictors of Decision Regret among Informal Caregivers Making Decisions for a Loved One: A Systematic Review
Supplemental material, Elidor_et_al._Revue_Decision_Regret_Supplementary_file_3_20200903.rjf_online_supp for Extent and Predictors of Decision Regret among Informal Caregivers Making Decisions for a Loved One: A Systematic Review by Hélène Elidor, Rhéda Adekpedjou, HervéTchala Vignon Zomahoun, Ali Ben Charif, Titilayo Tatiana Agbadjé, Nathalie Rheault and France Légaré in Medical Decision Making
Supplemental Material
Elidor_et_al._Revue_Decision_Regret_Supplementary_file_4_20200903.rjf_online_supp – Supplemental material for Extent and Predictors of Decision Regret among Informal Caregivers Making Decisions for a Loved One: A Systematic Review
Supplemental material, Elidor_et_al._Revue_Decision_Regret_Supplementary_file_4_20200903.rjf_online_supp for Extent and Predictors of Decision Regret among Informal Caregivers Making Decisions for a Loved One: A Systematic Review by Hélène Elidor, Rhéda Adekpedjou, HervéTchala Vignon Zomahoun, Ali Ben Charif, Titilayo Tatiana Agbadjé, Nathalie Rheault and France Légaré in Medical Decision Making
Footnotes
Acknowledgements
We wish to thank Hubert Robitaille for his dedicated assistance with the conception of the review protocol and Louisa Blair and Thomas Mills for language revision and editing.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Tier 1 Canada Research Chair in Shared Decision Making and Knowledge Translation provided financial support for this study (No. 950-231200). FL holds this chair. This Chair and VITAM (Centre de recherche en santé durable) supported HE and RA. The Fonds de recherche en santé du Québec–Santé (FRQS) supported ABC. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. Only the authors are responsible for the information provided and the views expressed in this article.
Authors’ contributions
HE, HTVZ, and FL conceptualized and designed the review protocol with the support of NR. NR developed the search strategy that was revised by HTHZ, HE, and FL. HE, TTA, and RA conducted the study selection and data extraction. HE and RA performed the quality assessment. HE conducted data synthesis, which was revised by HTVZ, RA, and ABC. HE drafted the manuscript overseen by HTVZ, RA, ABC, and FL. All authors contributed to important results, revised the manuscript critically for key intellectual content, gave their consent of the version to be published, and agreed to be responsible for all aspects of this review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.