
Abstract
Seasonal influenza is a significant health threat that circulates in all parts of the world. According to the World Health Organization, it leads to an estimated 3 to 5 million cases of severe illnesses and between 290,000 to 650,000 deaths globally each year. 1 In the United States alone, it causes more than 200,000 hospitalizations and more than 8000 deaths each year.2,3 It is also associated with increased general practice consultation, 4 lost days of work, 5 impaired academic and work-related performance,6,7 and overall pressure on the health care system during the winter months. 3
The influenza vaccine has been shown to reduce morbidity and mortality rates8–10 and is available at low cost. Nevertheless, many individuals who are recommended by their local health care authorities to receive the vaccine fail to do so.11,12 Even health care workers’ compliance rates are relatively low.13,14 Reasons for refusing the shots and the determinants of compliance rates vary across countries and social groups. Family background, age, and health status play an important role in the decision 15 as do health insurance coverage16,17 and advice within the household. 18 Many psychological factors, such as risk perceptions and social norms, have also been shown to affect the decision regarding vaccination. 19
A large body of literature has examined different interventions to increase the rate of compliance with the seasonal flu shot. Among those, one can find more traditional interventions, such as education and financial incentives20–23 as well as behavioral approaches that draw from the psychology and behavioral economics literature (also known as behavioral nudges). These include setting a default appointment to receive the shot, 24 emphasizing the benefits of the vaccine through invitation messages,25,26 reminders,27,28 personal invitations,29,30 asking patients to make an active choice during their visit to the clinic,31,32 and creating planning prompts, also known as implementation intentions. 33 Recently, it has been found that some of these behavioral interventions compare favorably with traditional ones in terms of their impact-to-cost ratio. 34
This article suggests and measures the effect of a new intervention that uses the seasonal nature of the flu and splits the option to receive the flu shot into an early (recommended) shot and a late one. The late option is quite clearly inferior to the early one and is therefore likely to generate comparisons that highlight the advantages of the more attractive shot. This suggested comparative channel is similar to the one that emerges as one of the psychological explanations underlying the well-known decoy effect. i One advantage of our approach is that it allows the natural integration of more standard tools—providing additional information, recommendations, and financial incentives—that have been shown to have positive effects on flu vaccine uptake, into the design. Using a survey held in Israel, we found that this intervention has the potential to significantly increase influenza vaccination uptake rates. Moreover, it can lead those who intend to receive the vaccine to do so early in the winter season, which has been shown to be more cost-effective.41,42 The suggested approach may be implemented at low costs and on a large scale.
Participants in our survey received a questionnaire in early September and were asked to imagine that on October 1, they will receive an invitation from their health maintenance organization (HMO) to get vaccinated against seasonal influenza. As in the standard protocol used by most HMOs in Israel today, all invitations began with an introduction that includes basic information about the disease and the vaccine. ii In the control group, the invitation continued to follow the standard protocol and stated that the vaccination is recommended by the Ministry of Health and is free and available until March 31. Participants in the control group were then asked whether they plan on getting the shot or not.
Our treatment groups added the timing dimension to the standard invitation by splitting the option to get vaccinated in two. The invitations started off with the exact same basic information as in the control. At this point, however, the invitation went on to describe 2 options to receive the shot: in early winter, until December 31, which is recommended by the Ministry of Health, or later in the season, from January 1 until March 31. Introducing vaccinations in this manner creates the basis for an early attractive flu shot option and a late inferior flu shot option. In our first treatment, the early shot was made attractive by the mere recommendation of the Ministry of Health alongside a brief explanation of the advantage of getting the shot early. The other treatments added an extra layer of attractiveness to the early shot compared with the late one. Here is the full list of treatments followed by a short description of their content:
Recommendation: The Ministry of Health recommends to get the early shot in order to increase its effectiveness.
Stock: As in the Recommendation treatment, and the invitation states that there is a higher chance that the vaccine will run out of stock after December 31.
Cost: As in the Recommendation treatment, and the early shot is free while the late one costs a fee of 20 ILS. iii
Benefit: As in the Recommendation treatment, and the early shot carries a benefit of 20 ILS that may be used for future doctor visits within the HMO. No benefit is offered for a late shot or for not getting vaccinated. iv
Following the invitation and the description of the vaccination options, we asked our participants whether they plan on 1) getting the shot early, 2) getting the shot late, or 3) not getting the shot at all. Our main interest was in comparing reported intentions to get the shot in each treatment to the intentions reported in the control. Participants in all groups were also asked how certain they are regarding their willingness to get the flu shot (with the answer reported on a 5-point Likert-type scale), whether they received the shot last year, and how many times they received the shot in the past 5 years (to the best of their memory).
We suggest that, while the inferior flu shot option would be rarely chosen, introducing it would increase the likelihood of picking the attractive flu shot option, that is, getting vaccinated by the end of the calendar year. In addition, the informational content regarding the advantage of the early shot and the extra recommendation by the Ministry of Health are likely to shift preferences in the same direction. v Since not all types of dominated options may be expected to increase the choice frequency of the dominating alternative, 43 we explored 4 different types of inferior options and examined whether they shift preferences toward accepting vaccination and which type of inferior flu shot generates a stronger effect. In choosing dominated (and dominating) options for the different treatments, we sought to vary the range of the suggested policy tools that maintain the freedom of choice of the individuals and are relatively easy to implement.
Our survey was completed by a sample of the Israeli adult population between the ages of 18 and 65 years and consisted of 3271 participants. All treatments led to increases in intentions. These ranged from 2.6 percentage points in the Recommendation treatment through 5.3 and 6.4 in the Cost and Stock treatments, respectively, to 9.4 percentage points in the Benefit treatment. A logistic regression that controls for the reported number of vaccinations in the past 5 years and other demographic variables showed that treatment effects are positive and that all of them are significant except for the one generated by the Recommendation treatment. Additional analysis showed that the treatments mostly affected those who received the vaccination at most once in the past 5 years, a finding that carries practical policy implications for HMOs and health care policy makers. vi
We also found that in all 4 treatments, the vast majority of participants who reported that they would receive the flu shot intended to do so by the end of the calendar year (only 3.3% of the participants in the treatment groups intended to receive the shot after December 31). In other words, the late option (in all treatments) was indeed perceived as an inferior option that was not attractive in its own right. Thus, our design nudges those who are willing to vaccinate to do so in early winter, a finding that has important policy implications: early vaccination assists in preventing the flu from spreading in the population, and it has been shown to be more cost-effective.41,42 By analyzing participants’ explanations of their choices, we provide evidence for the psychological comparative procedure triggered by the domination relation between the early shot and the late one.
Earlier, we mentioned the wide array of interventions that the behavioral literature has suggested over the past years to increase influenza vaccination uptake rates. These may be categorized and ordered according to their level of coercion, a ranking that has sometimes been referred to as an “intervention ladder.”45,46 Interventions along this ladder range from doing nothing through soft interventions, such as providing information, to more aggressive options, for example, default appointments. The ladder reflects a tradeoff that is well known to researchers studying this topic: more aggressive policies (higher on the ladder) are often more impactful in increasing vaccination rates,31,33 but their implementation is often not feasible on a large scale, and they are prone to stronger ideological objections because of their relative aggression. Lower on the ladder, the softer interventions are easier to implement on a large scale but suffer from small effect sizes.26,46 Our attractive flu shot approach has the potential to break this tradeoff and succeed on both fronts. While it is a relatively soft intervention that is easy to implement on a large scale, it has significant and substantial effects on vaccination intentions.
Methods
We conducted a survey among a sample of the Israeli adult population aged 18 to 65 years consisting of 3271 participants (136 additional respondents did not complete the entire survey and were excluded from the analysis). vii The survey was run by a professional survey company via an online panel that has about 30,000 registered panelists, out of which the sample was drawn. The mean age of the sample was 40.08 years, with a standard deviation of 12.05 years (for a comparison of the relevant age distribution between the sample and the Israeli population, see Supplementary Material E). The sample was slightly biased toward women due to the difficulty of reaching an accurately representative sample of the required size via an online panel: 1423 were male (43.5%) and 1848 were female (56.5%) versus 49.5% males in the population. Participants who completed the survey (which took, on average, 2 min), received a compensation of 1 ILS (about 0.3 USD). The survey was distributed during the first week of September 2019.
Participants were randomly assigned into either 1 of the 4 treatment groups or the control with an equal probability of 0.2. They were asked to imagine that on October 1, they will receive a message from their HMO inviting them to receive the seasonal influenza vaccine. The information included in the invitations in the control and treatment groups is described in the introduction section.
Following the invitation, participants in the treatment groups had to indicate whether they intend to 1) get the shot early, 2) get the shot late, or 3) not get the shot at all. viii They were then asked to answer 4 more questions. First, they were asked to provide a brief explanation of their intention (an open-ended question). Then, we asked how certain they feel regarding their willingness to get the shot on a 5-point Likert-type scale ranging from 1 (not certain at all) to 5 (very certain). Finally, they were asked whether or not they received the shot last year and how many times they received the shot in the past 5 years (to the best of their recollection). The full surveys are available in Supplementary Material D. ix
Results
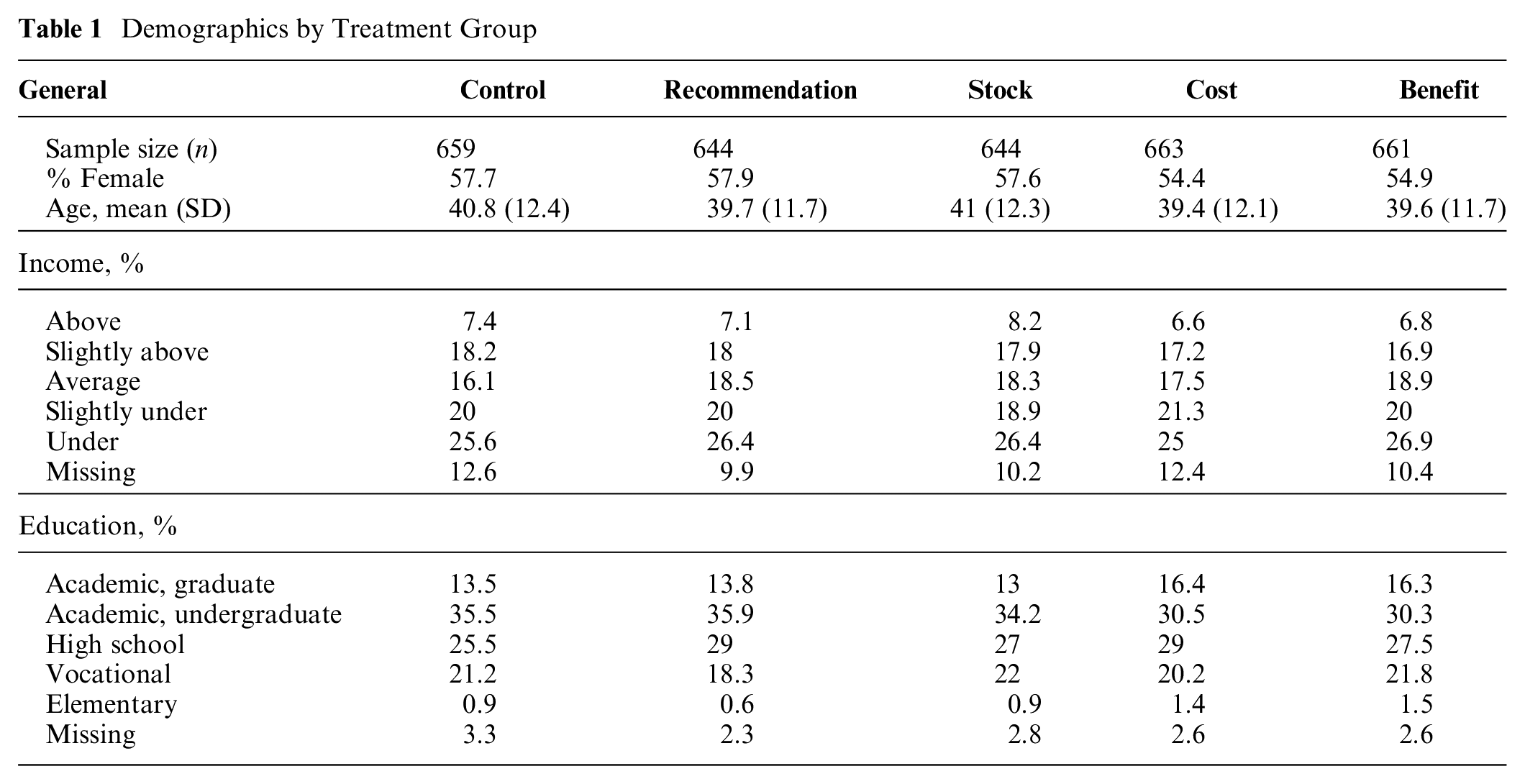
A general overview of our participant pool’s demographic characteristics is given in Table 1. As expected in a randomly controlled study, no significant differences appeared across treatments and control. An assessment of the quality of our data, based on 2 validation checks, showed that responses of our participants were highly consistent (see Supplementary Material C for details).
Demographics by Treatment Group
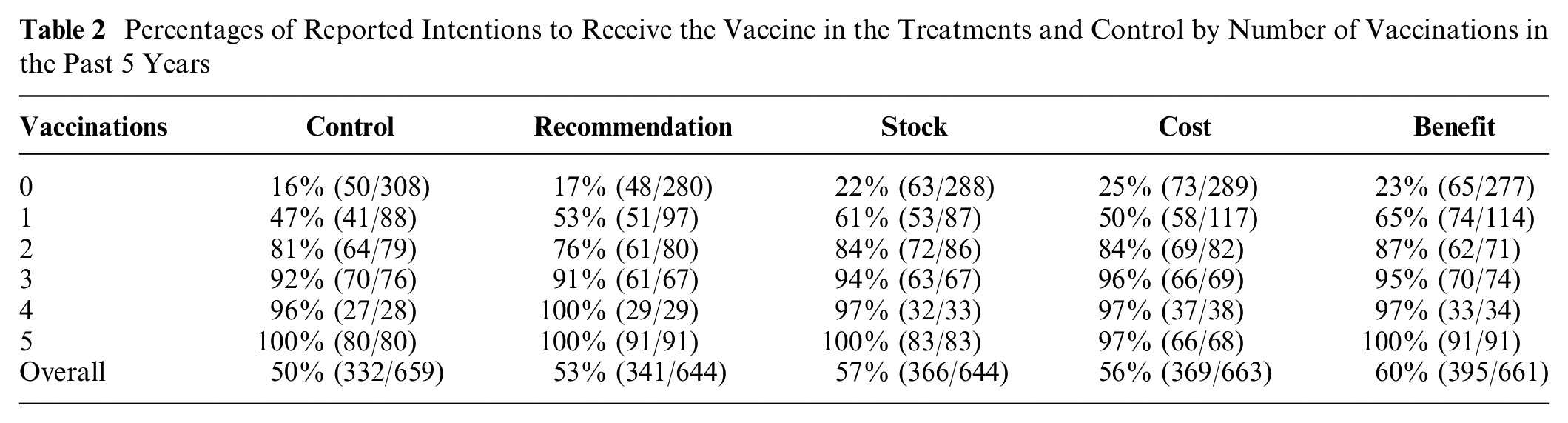
In Table 2, we provide an overview of vaccination intentions by treatment, broken down by number of vaccinations in the past 5 years. Starting with the overall effects (bottom row), we observed that all treatments had a positive effect on intentions, ranging from 2.6 to 9.4 percentage points. We used Pearson’s chi-square test (with false discovery rate correction for multiple comparisons 47 ) to examine whether vaccination intentions were independent of the treatments. The null hypothesis that overall intentions are not affected by treatments may be rejected (χ2 = 13.8003, df = 4, adjusted P value = 0.034). The table also shows that our design mostly affected those who received at most 1 vaccination in the past 5 years (top 2 rows). Once again, we used Pearson’s chi-square test to examine whether intentions to vaccinate were independent of the treatments for participants with the same number of vaccinations in the past 5 years. We can reject (with marginal significance) the null hypothesis that vaccination intentions of those who did not get any vaccinations in the past 5 years and those who got the shot only once in that time period are not affected by treatments (zero vaccination group: χ2 = 11.079, df = 4, adjusted P-value = 0.067, one vaccination group: χ2 = 9.8959, df = 4, adjusted P-value = 0.091). Looking at the table, it is quite obvious that our treatments did not affect those who received 2 vaccinations or more in the past 5 years. For those with 2 vaccinations in the past 5 years, we obtained χ2 = 3.656, df = 4, and an adjusted P-value of 0.537. Almost all individuals in the remaining groups (3 or more vaccinations in the past 5 years) intended to receive the shot (899/928, 97%), and for these groups, the treatments had no effect on intentions. x
Percentages of Reported Intentions to Receive the Vaccine in the Treatments and Control by Number of Vaccinations in the Past 5 Years
It seems somewhat surprising that our intervention affected those who received at most 1 vaccination in the past 5 years, since it is reasonable to think of this group as having strong preferences against the vaccine (especially those who did not comply even once in that period). Our results show that this is not necessarily the case. It may be that their attitude toward the vaccine is actually quite ambiguous and that this ambiguity leads them to behave passively (i.e., not vaccinate) especially considering the time cost associated with getting the shot. The tendency to remain passive and stick to the default (even when the costs of acting are much lower than those associated with getting vaccinated) is a well-known phenomenon in the psychology and behavioral economics literature.48–50 If their attitude is indeed ambiguous, they may be prone to behavioral nudging.
To further examine this potential explanation, we checked the correlation between the number of vaccinations in the past 5 years and the level of certainty regarding the vaccine (on a scale of 1 to 5) and found that it is equal to 0.39 (medium-low correlation). xi Thus, it seems that the strength of preferences may be partially responsible for the lift in intentions among those with a low number of vaccinations in the past 5 years, but it is certainly not the only factor. Future research may shed more light on the relationship between recent compliance rates and the potential to be affected through nudging.
Next, we ran 3 logistic regression models in which the dependent variable equals 1 if the individual reported an intention to receive the shot and 0 otherwise. The results are reported in Table 3. The first model includes only treatment dummies as explanatory variables and therefore represents the overall treatment effects. All treatments (except for Recommendation), generated a positive effect on intentions with varying significance levels (the Cost treatment is significant only at the α = 10% level). The odds ratios of the Stock, Cost, and Benefit treatments are 1.297, 1.236, and 1.462, respectively. In the second column, we controlled for vaccination history (number of vaccinations in the past 5 years) as well as demographic variables. This strengthens the effects of the Stock, Cost, and Benefit treatments: The odds ratios are 1.513, 1.461, and 1.662, respectively, and all coefficients are significant at the 5% level (Stock and Benefit are significant at the 1% level). As may be expected, vaccination history is an important predictor of intentions to receive the shot (odds ratio of 4.03). This column provides 2 additional interesting findings that are unrelated to our study’s main focus: men were more willing to receive the shot than women, and age had a negative (albeit small) effect on intentions (see Schmid et al. 19 for a recent systematic review of findings relating these demographic variables to influenza vaccination). In the third column, we added the interaction between treatments and vaccination history and found that although the treatment effects change very slightly, the interaction variables are not significant.
Logistic Regression Models a
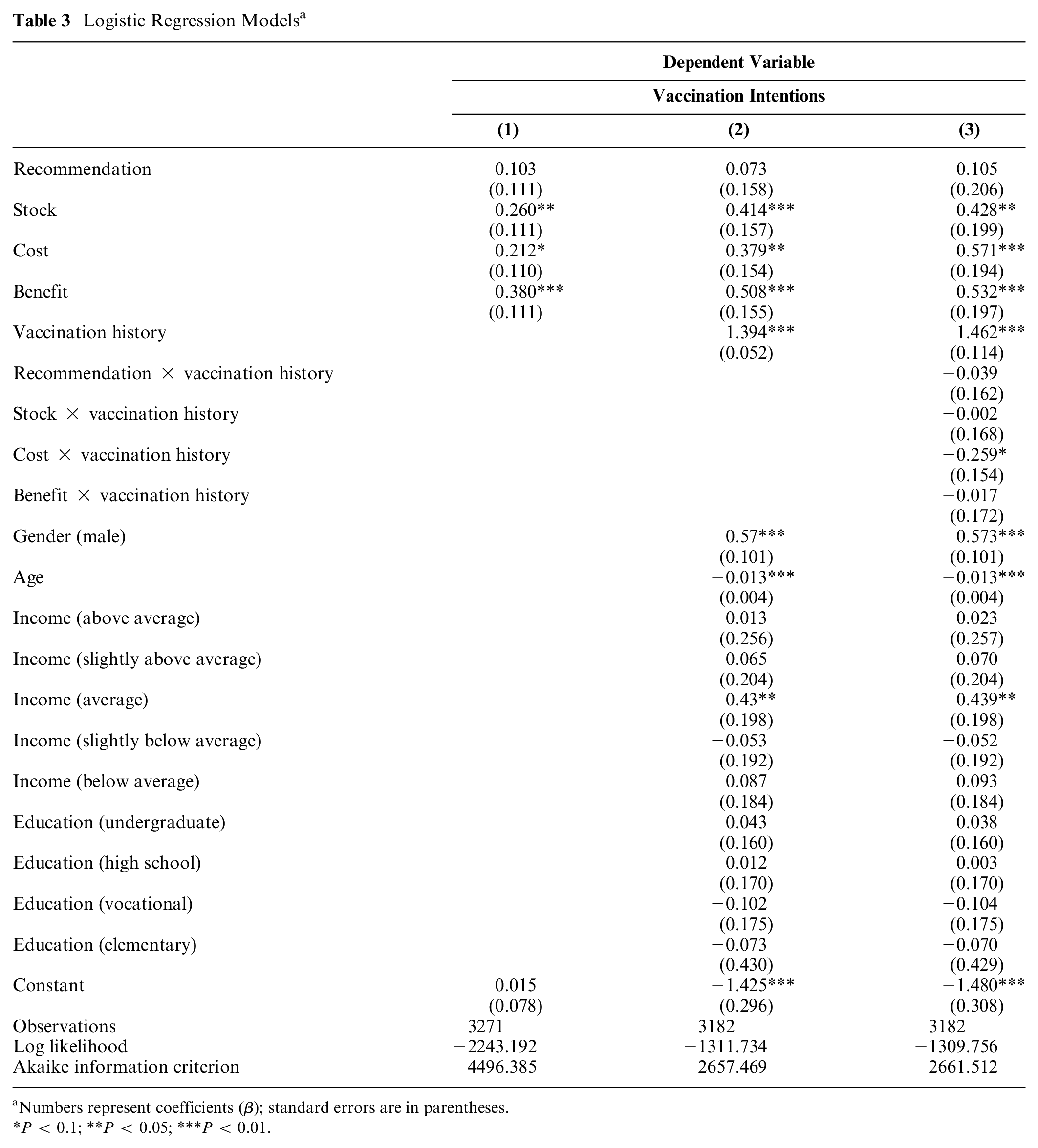
Numbers represent coefficients (β); standard errors are in parentheses.
P < 0.1; **P < 0.05; ***P < 0.01.
Our questionnaire not only provides information regarding positive or negative intentions to vaccinate. It also contains information about individuals’ timing decision. The vast majority of participants in the treatment groups who intended to get the shot planned on doing so early in the season. Only 3.3% of participants in these groups (87 of 2612) planned to get the late shot. In Table 4, we ran a multinomial logit regression with participants from all treatment groups (excluding the control) in which the dependent variable takes 3 possible values: vaccinate early, vaccinate late, or not vaccinate at all. The benchmark group is taken to be the Recommendation treatment. The table shows that participants responded to the financial incentives introduced in the Benefit and Stock treatments: the Benefit treatment increased intentions to receive the early shot, while the Cost treatment lowered intentions to get the late shot.
Multinomial Logit Regression a
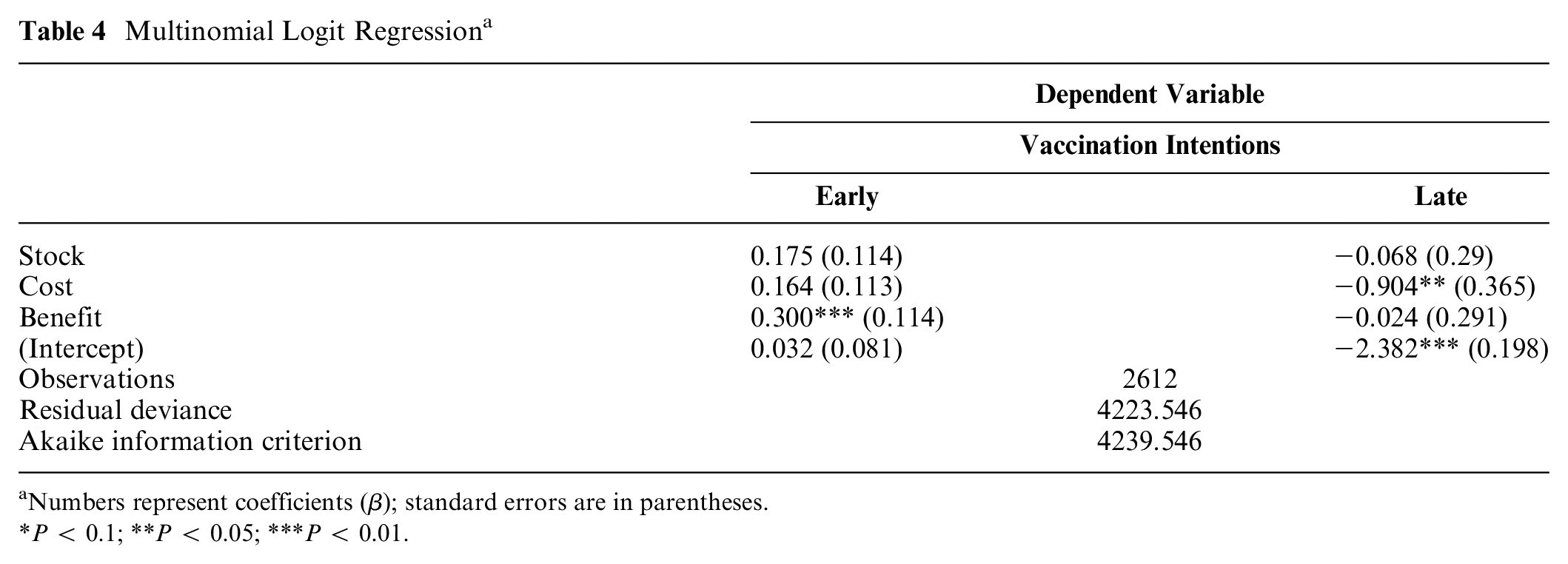
Numbers represent coefficients (β); standard errors are in parentheses.
P < 0.1; **P < 0.05; ***P < 0.01.
One question in the survey recorded participants’ open-ended responses for their stated intentions, which allowed us to gain insight into their psychological decision-making procedure. Specifically, we examined whether the late option to receive the shot played a role and influenced their decisions. If many responses include a comparative argument between the early and late shots, this would support the conjecture that the late decoy option affects participants’ reasoning through a psychological mechanism that is similar to the one underlying the decoy effect. Indeed, we found that 41% of participants in the treatment groups made a comparative statement between the early shot and the late one based on the former’s relative attractiveness. It is possible that for some individuals, who perhaps would not have taken the shot given a standard invitation message, this reasoning (on top of all other supporting arguments that they have in mind) may be the extra nudge they need to get the shot. xii
Examining comparative arguments by treatments, we found that 29% made such arguments in the Recommendation treatment and that 40%, 47%, and 49% did so in the Stock, Cost, and Benefit treatments, respectively. These percentages show that all of our late vaccination options affected individuals’ reasoning to some extent. Notice the fact that the Recommendation treatment, which is the one that makes the weakest distinction between the early and late shots, had the lowest percentage of comparative arguments, followed by the Stock treatment, which creates a stronger distinction but one that is still not very tangible. The monetary treatments (Cost and Benefit) have the largest volume of comparative arguments, as they make the strongest distinction between the 2 shots, one that carries clear monetary consequences.
Discussion
We conducted a survey and measured how introducing two options to receive the flu shot—early and late—affects individuals’ intentions to get vaccinated. We designed 4 treatments that differed in the manner in which they enhanced the early shot compared with the late one. All treatments increased vaccination intentions compared with the control, 3 of them significantly so. If HMOs would like to use this design and concentrate their efforts on specific subgroups that can be identified, they should focus on those who received at most 1 flu shot in the past 5 years.
Our intervention combines the psychological behavior triggered by the presence of a dominated option with more rational effects on behavior due to added information, repeated recommendations, and financial incentives. We now briefly examine these factors and the potential roles they play in our findings.
The Dominated Option Effect and Other Potential Factors
The literature on the decoy effect highlights the potential of a dominated option to trigger comparisons that enhance the attractiveness of the dominating option, which may, in turn, shift preferences in its favor. As reported in the Results section, we found support for this psychological channel in our data, as a substantial percentage of participants made arguments based on the comparative advantage of the early shot over the late one. Furthermore, these arguments appeared most frequently in the Benefit and Cost treatments, followed by the Stock treatment and finally the Recommendation treatment. In other words, the starker the dominance relation between the early and late vaccination options, the more comparative arguments were made. This shows that, if our design is to be implemented, it is important to maintain a clear dominance relation between the early and late shots to generate the maximal effect of the psychological comparative channel.
We would like to suggest 3 more potential contributing effects. First, compared with the control, the treatments provided additional information regarding the advantages of receiving the shot early in the season. In the treatments’ invitations, it was stated that “the Ministry of Health recommends to get the shot early, in the beginning of the season, until December 31st, in order to increase its effectiveness for you and for the rest of the population.” Educating and providing information have been found to have positive effects on influenza vaccinations.20,22
Another potential effect may be due to the fact that the treatments’ invitations included 2 recommendations by the Ministry of Health, whereas the control included only one. The first recommendation appeared in all treatments and control and referred to influenza vaccination in general. The second recommendation appeared only in the treatment groups and referred to the early option. Some studies have already shown that individuals react to recommendations,51,52 and although we are not aware of studies examining the role of repeated recommendations, it is plausible that such repetitions may encourage higher compliance rates. It is important to note, however, that the informational content and the repeated recommendations are common to all of our treatment groups. Hence, while they may account for an overall positive lift of intentions compared with the control group, they cannot account for the heterogeneous effects of the different treatments. The heterogeneity of our treatment effects is, in our opinion, mostly due to the differences in the late options across treatments and the variation in their ability to trigger a comparison that favors the early shot.
Finally, in the Benefit treatment, the early shot carried a monetary reward that may be used to cover the copay for doctor visits within the HMO. This is the only treatment in which a financial incentive in the form of a bonus was used, and as prior research has shown, such incentives are likely to have a positive impact on vaccination uptake rates.20,21,53 It is therefore plausible that the incentive introduced in this treatment is responsible for at least part of its relatively large effect on intentions.
Policy Implications
Two of our treatments involved monetary transfers, that is, benefits to those who come early or a fee paid by those who arrive late. These transfers were relatively small and comparable with the fee associated with a visit to a specialist in most insurance plans available in Israel today. However, since monetary transfers may be problematic from a regulatory perspective, policy makers may prefer to consider the Recommendation and Stock treatments that generate substantial effects on intentions by simply conveying different information through their invitation messages.
In contemplating which attractive flu shot may be most appropriate to implement, it is important to note that the nonmonetary treatments may be less effective in practice since their separation between the early and late shots is less tangible than the separation made by the monetary treatments. In the Recommendation treatment, for example, there are actually no material consequences for receiving the late shot. In the other nonmonetary treatment (Stock), it is indeed more likely that the vaccine will run out of stock later in the season, but it is not likely that this will happen exactly on December 31, and individuals will most probably be aware of that. By contrast, in the Benefit and Cost treatments, getting the shot after December 31 carries the consequence of not receiving a bonus/paying a fee, which may more naturally resonate on people’s minds. Thus, the monetary treatments may be more effective, whereas the nonmonetary treatments may require more publicity to maintain their effectiveness. xiii
Limitations
This study examined intentions rather than actual vaccination uptake rates. However, it has been shown that positive intentions are associated with a much higher likelihood of actually receiving the shot.17,54,55 Moreover, it was pointed out that those with positive intentions are more likely to follow their provider’s recommendation to receive the shot. 54 Thus, influencing intentions is likely to have important and significant positive effects on actual uptake rates. To provide more accurate estimates of the effectiveness of our attractive flu shot design, it would be helpful to examine how actual vaccination rates respond to such an intervention, a task that remains to be explored in future work.
The participant pool we analyzed did not include elderly people (older than 65 years), who are considered a major high-risk population that is recommended to receive the flu shot (in fact, as the age distribution in the sample is representative of the age range that we were able to sample, only 26% of the participants were 50 years or older). Yet, it is important to keep in mind that although younger individuals may be less vulnerable to complications related to the disease than the elderly, an increase in the vaccination rates of the younger population has been shown to generate positive external effects for the elderly. 56 In addition, younger adults are less likely to receive the flu shot and less likely to follow standard health recommendations by providers. 57 This age group might require new approaches to increase its uptake rates, such as the one suggested in this study.
Supplemental Material
Appendix1_online_supp – Supplemental material for Attractive Flu Shot: A Behavioral Approach to Increasing Influenza Vaccination Uptake Rates
Supplemental material, Appendix1_online_supp for Attractive Flu Shot: A Behavioral Approach to Increasing Influenza Vaccination Uptake Rates by Amnon Maltz and Adi Sarid in Medical Decision Making
Supplemental Material
Appendix2_online_supp – Supplemental material for Attractive Flu Shot: A Behavioral Approach to Increasing Influenza Vaccination Uptake Rates
Supplemental material, Appendix2_online_supp for Attractive Flu Shot: A Behavioral Approach to Increasing Influenza Vaccination Uptake Rates by Amnon Maltz and Adi Sarid in Medical Decision Making
Supplemental Material
Appendix3_online_supp – Supplemental material for Attractive Flu Shot: A Behavioral Approach to Increasing Influenza Vaccination Uptake Rates
Supplemental material, Appendix3_online_supp for Attractive Flu Shot: A Behavioral Approach to Increasing Influenza Vaccination Uptake Rates by Amnon Maltz and Adi Sarid in Medical Decision Making
Supplemental Material
Appendix4_online_supp – Supplemental material for Attractive Flu Shot: A Behavioral Approach to Increasing Influenza Vaccination Uptake Rates
Supplemental material, Appendix4_online_supp for Attractive Flu Shot: A Behavioral Approach to Increasing Influenza Vaccination Uptake Rates by Amnon Maltz and Adi Sarid in Medical Decision Making
Supplemental Material
Appendix5_online_supp – Supplemental material for Attractive Flu Shot: A Behavioral Approach to Increasing Influenza Vaccination Uptake Rates
Supplemental material, Appendix5_online_supp for Attractive Flu Shot: A Behavioral Approach to Increasing Influenza Vaccination Uptake Rates by Amnon Maltz and Adi Sarid in Medical Decision Making
Footnotes
Acknowledgements
We thank Arie Melnik for helping us discover our interest in this topic. We also thank Ayala Arad and Moti Michaeli for important comments and fruitful discussions. Finally, we would like to thank 3 anonymous reviewers who invested from their time and efforts to significantly improve this article.
Authors’ Note
This research was approved by the Committee for Ethical Research and the Protection of Human Participants, the Faculty of Social Sciences, University of Haifa (approval number 260/16). This study has been preregistered on the AEA RCT Registry, and its unique identifying number is AEARCTR-0004584. All data and analysis code are available through this preregistration ID and on the following GitHub repository: ![]() .
.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.