
Abstract
Keywords
Physicians are morally and legally obligated to obtain informed consent when initiating medical therapies. It should be expected that patients understand their condition, and the recommended treatment’s benefits, harms, and alternatives. 1 However, patients often make decisions regarding complex medications with incomplete knowledge 2 and may have a limited ability to comprehend complex risk-benefit information.3,4
Rheumatoid arthritis (RA) is a chronic inflammatory disease that causes joint pain, functional impairment and irreversible joint damage. Etanercept is an injectable protein that targets and blocks the pro-inflammatory cytokine tumor necrosis factor-α (TNFα). Etanercept is utilized as a disease modifying anti-rheumatic drug (DMARD), which reduces joint swelling and pain as well as slows the development of joint damage.5,6
When physicians propose a new high-risk medication, like etanercept for RA, it is common practice for them to provide patients with a medication decision guide created by a pharmaceutical company in accordance with Food and Drug Administration (FDA) guidelines. These pharmaceutical industry decision guides (Pharm Booklet) are a form of direct-to-consumer communication that are required by the FDA to provide a balanced presentation of the risks and benefits. Medication guides only describe the drug’s indication for usage, not the specific benefits, and present side effects in long lists, which may not distinguish between clinically important and unimportant side effects. 7 They have been criticized for not providing data on how well a drug works, leading consumers to over-estimate disease risk, treatment benefits, and side effects.7-9 The full effects of this information architecture are not fully known but could include biased appraisals of drug benefits and risks, reduced participation in decision making (i.e., accepting the default physician recommendations), and increased decisional conflict about the use of effective therapies.9-11
Patient decision aids (PtDA) are an alternative approach to make information accessible, increase patient understanding of complex risk information, and facilitate patient participation, which can lead to more value-concordant medication decisions. The International Patient Decision Aids Standards Collaboration (IPDAS) promulgates a set of criteria for a good PtDA. 12 Despite recognition that PtDA could broadly improve healthcare, their adoption has been slow due to cultural, professional, and regulatory barriers.7,13, 14 The purpose of this study is to directly compare the effects of a Pharm Booklet with IPDAS-compliant PtDAs 15 on decision making.
Methods
Design and Setting
We conducted a single-blind, randomized controlled study of 3 educational interventions to support RA patients who had not previously taken a biologic DMARD, in making a simulated decision about intensifying medical therapy by adding etanercept to their current regimen (see Figure 1). The Michigan State University Institutional Review Board determined that the research protocol was exempt from review. The study population was men and women with RA 16 treated in a community rheumatology practice. The sample frame was created from the practice electronic health record registry (EHR). All subjects received care between July 24, 2012 and July 23, 2013, and were billed under the ICD-9 code 714.0 (RA). From the records, 1,637 adult patients were identified. All patients were considered for inclusion in the study. Inclusion criteria were assured by electronic search and manual review of the EHR, to confirm both the diagnosis of RA and that there was no past use of biologic DMARDs. Of the patients identified, 797 biologic DMARD-naïve RA patients were selected and included in a 3-contact mail survey using the methods described by Dillman. 17 Mailings and cover letters were addressed from each patient’s rheumatologist. The first question of the survey instrument inquired if the patient had RA and if they had previously taken a TNF blocking DMARD, like etanercept. In accordance with the research provision of the practice HIPAA statement, patient records were reviewed and the most recent summary scores of the Health Assessment Questionnaire 2 (HAQ2) 18 and Clinical Disease Activity Index (CDAI) 19 were extracted and written on the last page of the questionnaire. Although the questionnaire was anonymous, demographic characteristics of the survey sample were recorded in a separate database to permit comparison of the demographics of responders and non-responders.
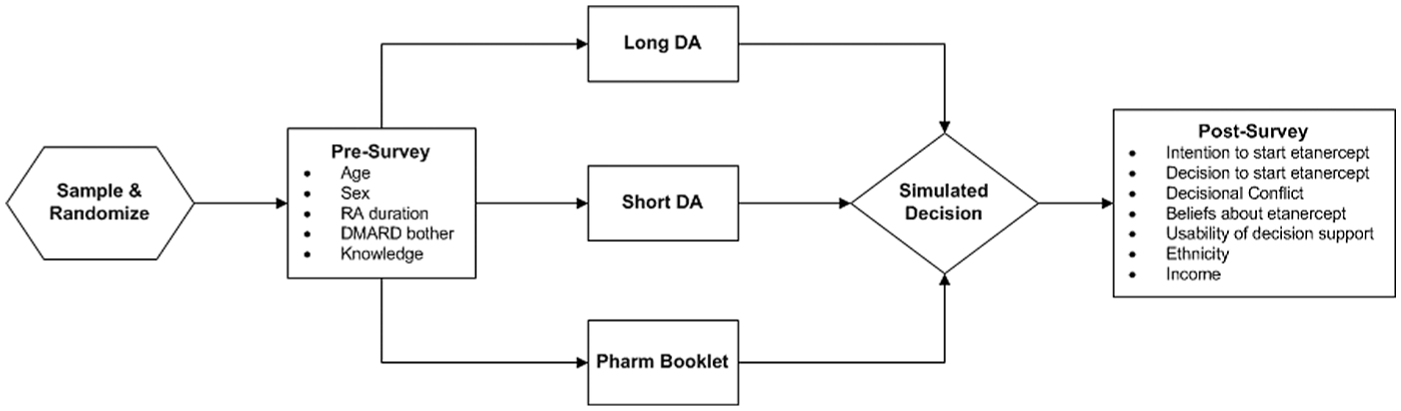
Study Design.
Decision Support Interventions
LONG DA
We previously developed a prototype patient decision aid for patients considering initiating the synthetic DMARD methotrexate to treat their RA.4, 20, 21 The decision aid followed the steps involved in the Ottawa Decision Support framework 22 and adhered to the design specifications of the IPDAS. 15 This produced a 24-page, 21.5 cm × 14 cm (8.5- × 5.5-inch) booklet. Pre-testing demonstrated this was acceptable to RA patients and significantly increased relevant knowledge. Appraisal with the IPDAS instrument disclosed a quality score of 74 (0 to 100), which is in the range of existing benchmark decision aids. 20 We adapted the content of this methotrexate PtDA to be appropriate for patients considering initiating etanercept to treat their RA. For example, information was added on the potential adverse events from etanercept, which are not encountered with methotrexate therapy: injection site reactions, risk of reactivation of tuberculosis or other latent infections, and induction of immunological reactions. Sections elaborating the risks of methotrexate liver and lung toxicity were deleted. The LONG DA was 24 pages and contained the decision/choice set, and the following information: RA and Its Treatments, Information on Enbrel, Chance of Improving RA, Slowing Joint Damage, Chance of Serious Infection and Other Possible Harms, a Summary of Possible Benefits and Harms. It also included a decision matrix, a values clarification rating table, and a brief reflection on decision quality (see Appendix).
SHORT DA
We developed a 2-page SHORT DA based on the LONG DA. The first page presented the decision/choice set, brief information on Enbrel, visual representations of the sections on Chance of Improving RA, Slowing Joint Damage, Chance of Serious Infection and Other Possible Harms. The second page contained a Summary of Possible Benefits and Harms, a decision matrix, a values clarification table, and brief self-reflection on decision quality (see Appendix).
Pharm Booklet
The third decision support was a 35-page, 23 cm × 10 cm (9.0- × 4.0-inch) Amgen Enbrel Treatment Guide pharmaceutical material. This provided qualitative information on efficacy, safety, and administration procedures. Distributed through the medication information, there were 6 photos of RA patients linked to a brief, personal testimonial about their use of etanercept. In addition, the Enbrel Treatment Guide contained the FDA-mandated Prescribing Information, Medication Guide and Instructions for Use, which were folded in a back-cover pocket. When unfolded, the Prescribing Information and Medication Guide were a 2-sided, 76 cm × 53 cm (30- × 21-inch) leaflet. The complete content is available online. 23
Decision Scenario
In the hypothetical decision, patients were instructed to:
“Imagine that your RA has become more active than you want to tolerate. You approached your doctor about switching to a new disease-modifying drug. Your rheumatologist suggested adding Enbrel to your current regimen of medication. He has given you a treatment guide to read and asked you to call him tomorrow with your decision about whether or not you would like to start it.”
The patient was then instructed to open the sealed “medication information envelope” and to pause and read the enclosed “Treatment Guide”. Below the instructions, there was an image of the decision support to which the patient was randomized (see Appendix). Patients allocated to receive the Pharm Booklet, were shown a picture of the location of the “Medication Guide”. They were instructed, “Be sure to pull out and read the ‘Medication Guide’ tucked in the back pocket of the booklet, too.” This was followed by the instructions; “When you have finished reviewing the materials, please place them back in the envelope until you finish the questionnaire.”
On the next page, they were asked, “If you had to decide today, what would your decision be?” and choose between “I would call to request a prescription to start Enbrel now” or “I would choose not to start Enbrel now.” Patients were then instructed to turn the page and finish the questionnaire without looking back at the decision support materials.
Study Measurements
The survey instrument assessed the following patient variables:
Demographics
Age, sex, ethnicity, education, and household income were elicited. Participants who reported having less than a high-school graduation were classified as having low education. Participants who reported Hispanic, African, or Native American ethnicity were classified as having minority status. Low income was defined as total household income <$25,000, which is 106% the 2013 Federal Poverty Level for a family of 4. 24
RA- and DMARD-related Experience
RA disease duration, past, and current DMARD usage was elicited. We assessed the level of current (traditional) DMARD-related side effects with the item, “Think about the RA disease modifying drug you most recently started. Are you having any side effects from it that bother you now?”. 2
RA Disease Status
The HAQ2, 15 a validated measure of functional impairment, was utilized as an indicator of RA severity. The Clinical Disease Activity Index (CDAI) is a single, continuous, composite measure of RA disease activity that ranges from 0 to 76. 16 A score of 0 to 10 is classified as low, 11 to 22 as moderate, and ≥23 as high disease activity.
Decisional Conflict
We used O’Connor’s 16-item statement format of the Decisional Conflict Scale (DCS) 25 to evaluate the quality of the decision made about etanercept. This has 4 subscales: Informed, Values Clarity, Support, and Effective Decision. When combined, this yields a standardized score in the range of 0 to 100. The DCS can discriminate between groups who make and defer decisions, with an effect size of 0.4 or more. DCS scores of less than 25 are associated with implementing decisions, and scores greater than 37.5 are associated with uncertainty or delaying a decision. 26
Etanercept-related Knowledge
We created a test of patient knowledge that would be relevant to a patient considering intensifying their RA therapy by adding etanercept to their current treatment regimen. We began by comparing the content of 5 instruments previously reported for assessing patient knowledge in RA.20, 27-30 Within this pool of test items, we identified 37 relevant educational domains. From this, we generated 12 single-answer, multiple-choice knowledge test items. Using the Enbrel package insert and medication guide as our primary reference document, we modified these items to cover content relevant to etanercept (see Appendix): the RA disease process and consequences of untreated RA (2 items), basic information about etanercept therapy (2 items), the potential benefits (2 items) and harms of etanercept (6 items). Two investigators independently crosschecked the 3-decision support interventions to ensure that the content of the test items was representative of the educational domains and that the content needed to correctly answer all questions was present in all 3-decision support interventions. Items were modified as needed to meet this requirement. The usability of the test items was evaluated by 4 rheumatologists and 4 allied health professionals and revised. The same items were used in the pre-test and post-test, differing only in the arbitrary re-ordering of the multiple-choice foils in the post-test. Results are reported as the proportion of correctly answered items (possible range, 0.00 to 1.00).
Patient Beliefs about Etanercept
To evaluate patient beliefs about taking etanercept from the perspective of the Integrated Model of Behavioral Prediction (IMBP), 31 we developed 5-point Likert scale questions, as follows:
Beliefs about outcomes of therapy
Three questions probed the patients’ beliefs about the likely consequences of taking etanercept. ‘If I take Enbrel, it will improve my pain and stiffness enough to make a difference in my life’ (anchors: strongly disagree, strongly agree). ‘If I take Enbrel, it will slow the progression of the RA joint damage’ (anchors: strongly disagree, strongly agree) ‘If I take Enbrel, how likely would it be that I would have a serious side effect in the next year’ (anchors: no risk, absolutely certain I would have a serious side effect).
Normative beliefs
Patients’ normative beliefs about Enbrel were assessed by asking about their perception of the beliefs of other people who are important to them, and how likely they would be to take etanercept. ‘Most people, like me, who have active RA despite taking a DMARD like methotrexate, would choose to try Enbrel’ (anchors: unlikely, very likely).
Perceived behavioral control
Patients’ perceived ability to successfully act on their decision, which is an indicator of self-efficacy, was assessed with one item. ‘I’m confident I could do all that would be needed to take and monitor Enbrel’ (anchors: not at all confident, totally confident).
Intention to Take Etanercept
The integrative model of behavioral prediction proposes that people act on their intentions when environmental factors do not interfere. 31 We measured patients’ intention to take etanercept with the Likert item: ‘What is the likelihood that you would consider taking Enbrel today.’ (0 = would never take, and 9 = absolutely would take).
Formative Evaluation of Interventions
We used three 5-point Likert scale questions to compare patients’ perceptions of the acceptability, effectiveness, and efficiency of each of the interventions as a decision support. 32 ‘The materials had the information I needed to make a decision.’ ‘The materials were helpful in preparing me to make a decision about Enbrel.’ ‘The materials were well organized, easy to read, and contained the right amount of information.’
Analysis
Descriptive analyses were performed to provide information on the characteristics of the respondents. Bivariate relationships were evaluated with Pearson correlation coefficients, independent samples t tests, and Chi-squared tests, as appropriate. The effect of the 3-decision support interventions on continuous patient outcomes was evaluated with a one-way analysis of variance of variance (ANOVA) or 2-way repeated ANOVA, as appropriate. Multivariate predictive models of the decision to intensify care by initiating etanercept were created with binomial logistic regression. 33 Continuous independent variables were mean-centered. Finally, we evaluated the causal hypothesis that patients’ beliefs about the outcomes of therapy and normative beliefs mediate the effects of decision support on choice to intensify therapy using methods described by Baron and Kenny. 34 All analyses were performed with IBM SPSS Statistics version 21.0. 35
Results
We surveyed 797 patients with RA. All participants were randomized and allocated to an intervention. Subjects were blinded to the allocation. Data were analyzed for 402 respondents. In addition to 387 non-respondents, 4 patients had died and 4 had changed address and could not be reached. The overall response rate was 52.0%. Data from all study completers were included in the analysis. In the completed sample, all patients had RA. See Consort Diagram (Appendix).
Patient Characteristics
We compared the demographic and RA-related disease characteristics between the overall sample and the respondents. The overall sample was similar in age (mean, 63.7 y), sex (69% female), ethnicity (7.5% minority), HAQ2 disability (0.818) and CDAI (10.8). The proportion of the sample randomized to each intervention and the completed sample varied by less than 2% in response rates across groups. A description of the respondents is presented in Table 1.
Patient Characteristics
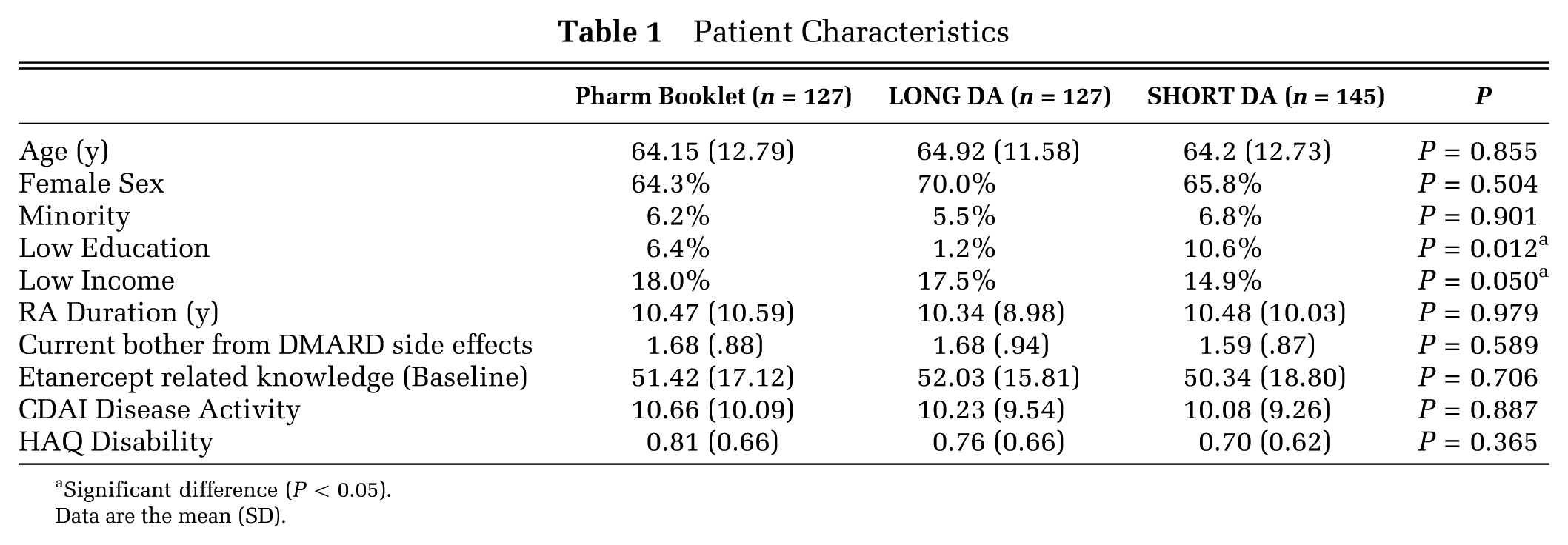
Significant difference (P < 0.05).
Data are the mean (SD).
Decision to Intensify Therapy
We found that 31.3% of patients randomized to receive decisional support from the Pharm Booklet, chose to intensify therapy by adding etanercept to their current regimen, as compared with 14.6% of LONG DA and 14.0% of SHORT DA (χ2 (2,394) = 15.68; P < 0.001).
Formative Evaluation of Decision Support Interventions
Patients rated perceived acceptability, effectiveness, and efficiency of each of the interventions above the mean on each of the 5-point Likert rating scales; there was no statistically significant difference in mean ratings among interventions.
Etanercept Related Knowledge
Test Reliability and Validity
The mean item difficulty for the pre-test was .51 (range, 0.08 to 0.89) and post-test .61 (range 0.20 to 0.88). Reliability of the combined index was adequate with a Cronbach α = 0.70. The item-total index correlations ranged from 0.28 to 0.46. Post-test knowledge correlated negatively with decisional conflict (r = -0.139, P < 0.02) suggesting modest construct validity.
Effect of Intervention
Results of pre- and post-intervention etanercept related knowledge tests are summarized in Figure 2. We evaluated change in pre-test to post-test etanercept knowledge as a function of intervention by utilizing a 2-way, mixed model ANOVA, with time (pretest and posttest) as the within-subjects variable, and intervention (Pharm Booklet group, LONG DA group, and SHORT DA group) as the between-subjects variable. The main effects were found for time (F (1,399) =125.454; P < 0.001), and intervention (F (2,399) = 3.209; P = 0.016). This significant interaction was further explored with follow-up one-way ANOVAs and post-hoc t tests. First, a one-way ANOVA on pre-test etanercept knowledge showed that, as expected, for each level of intervention, these groups did not significantly differ (F (2,399) = 0.335, P = 0.715; 51.429 [17.127] for Pharm Booklet group; 52.034 [15.808] for LONG DA group; 50.343 [18.797] for SHORT DA group). Next, a one-way ANOVA was conducted to determine whether the level of intervention influenced the post-test etanercept knowledge means. This effect was significant (F (2,399) = 9.809; P < 0.001). Tukey HSD post-hoc t tests indicated that the mean post-test knowledge for the Pharm Booklet group (54.849 [18.712]) was significantly lower than that for both the LONG DA (62.530 [18.889]) and SHORT DA (65.811 [23.340]) groups, with no significant difference between the LONG DA and SHORT DA groups. All interventions resulted in an increase in etanercept knowledge but the LONG DA and SHORT DA materials were significantly more effective in increasing knowledge than the Pharm Booklet.
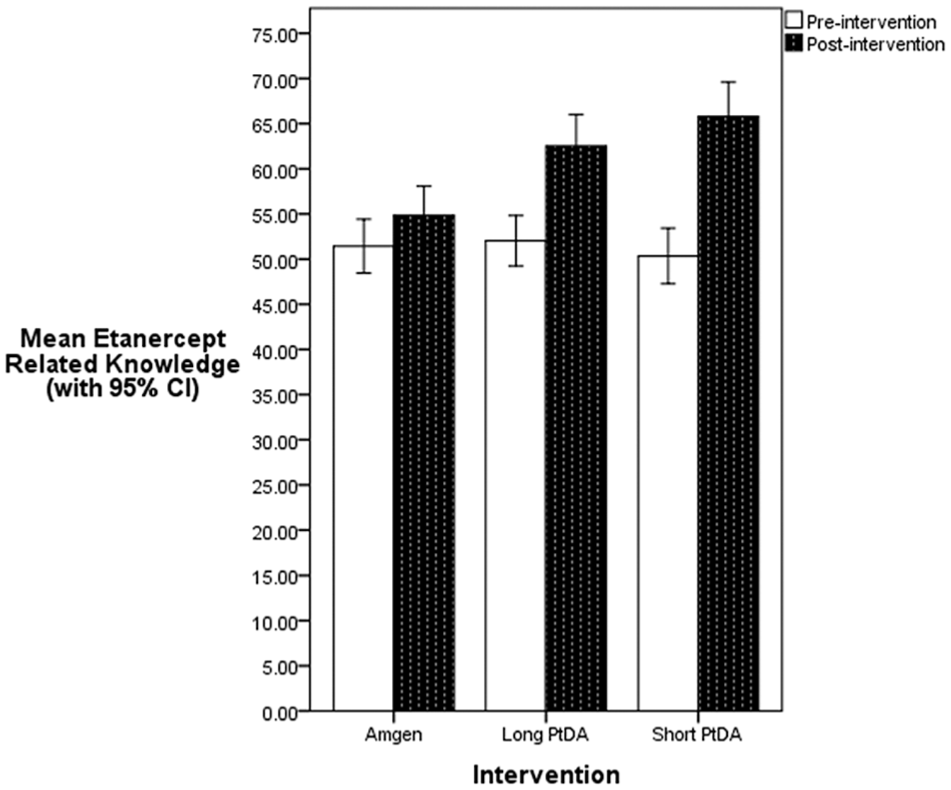
Change in etanercept related knowledge with decision support.
Beliefs about Etanercept
The results of the post-intervention testing of patient beliefs about etanercept are summarized in Table 2. We explored differences in patients’ beliefs about the outcomes of intensifying therapy with etanercept as a function of the intervention groups through a series of one-way ANOVA tests. First, the effect of the intervention group on belief about outcome of therapy was significant (F (2,387) = 5.454, P = 0.005). Tukey HSD post-hoc analyses revealed that the Pharm Booklet group (3.28 [1.125]) had a significantly higher belief that etanercept would improve RA symptoms than did the SHORT DA group (2.85 [1.039]), whereas the LONG DA group (3.16 [1.125]) did not significantly differ from the others. Second, the effect of the intervention on normative beliefs was also significant (F (2, 386) = 5.926; P = 0.003). Tukey HSD post-hoc analyses revealed a pattern of differences similar to that found for beliefs about outcome of therapy: the Pharm Booklet group (3.04 [1.042]) had a significantly higher belief that other patients with RA in a similar situation would take etanercept than did those in the SHORT DA group (2.58 [1.76]), while the LONG DA group (2.79 [1.125]) did not significantly differ from the others. Finally, no differences were found among the intervention groups for patient beliefs about how much etanercept would slow RA disease progression (F (2, 388) = 2.020; P = 0.134), for belief that etanercept would cause a serious adverse event in the next year (F (2, 388) = 0.017; P = 0.984), and for patients’ self-efficacy to take the new medication (F (2, 388) = 1.756; P = 0.174).
Beliefs about Etanercept
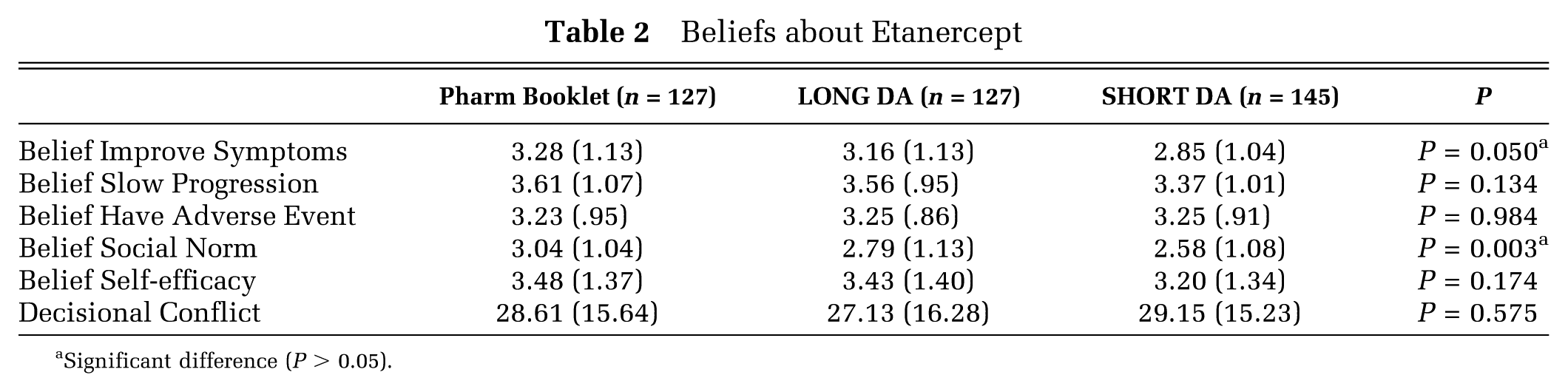
Significant difference (P > 0.05).
Decisional Conflict
Decisional conflict was assessed immediately after patients were asked to make a choice regarding intensifying therapy. The mean overall DCS score was 28.45 (15.79) with a range of 0 to 100. We evaluated the mean overall DCS score and DCS subscale scores by decision support intervention with one-way ANOVA and found no significant differences. We also found no significant differences in the proportion of patients with DCS scores >37.5 or DCS scores <25.0 (χ2(2) = 3.06, P = 0.22; χ2(2) = 0.483, P = 0.79).
Predictors of Decision to Intensify Therapy
We developed a preliminary logistic regression model to describe the relationships among patient characteristics, decision support intervention, and choice to intensify therapy. Dummy variables were created for Pharm Booklet and SHORT DA to allow the covariates to be included in the logistic equation. We used purposeful selection of covariates, including all potentially clinically relevant variables, to control for confounding. 36 In the first step, we created univariate logistic regression models for 18 potential predictor variables. Eleven variables were not predictive (P ≥ 0.25) and were excluded: female gender, low income, minority status, bother by side effects from current anti-rheumatics, RA disease activity (CDAI), functional disability (HAQ2), etanercept related knowledge, patients’ beliefs about how etanercept would slow RA disease progression, patients’ self-efficacy to take the new medication, values clarity, and overall decisional conflict.
Following this, we created a multivariate model by entering the 7 remaining variables, into a backward, stepwise logistic regression. We opted to retain low education in the final model regardless of its association as an important control variable. The final model fit was excellent in predicting treatment choice in 83.6% of cases, with the Nagelkerke R2 explaining 44.2% of variation. The Hosmer and Lemeshow Test P value was high (P < 0.752), indicating all systematic variance has been accounted for in the model. The Hosmer and Lemeshow Contingency Test showed close agreement between the expected and observed frequencies of the model across deciles in classifying patients into choice groups. Tolerances were >0.2, suggesting the absence of significant multicollinearity of covariates. We also evaluated inclusion of the 2-way interactions among age, low education, and the Pharm Booklet and SHORT DA dummy variables, but no interaction terms contributed significantly to the model, and we retained only the main effects.
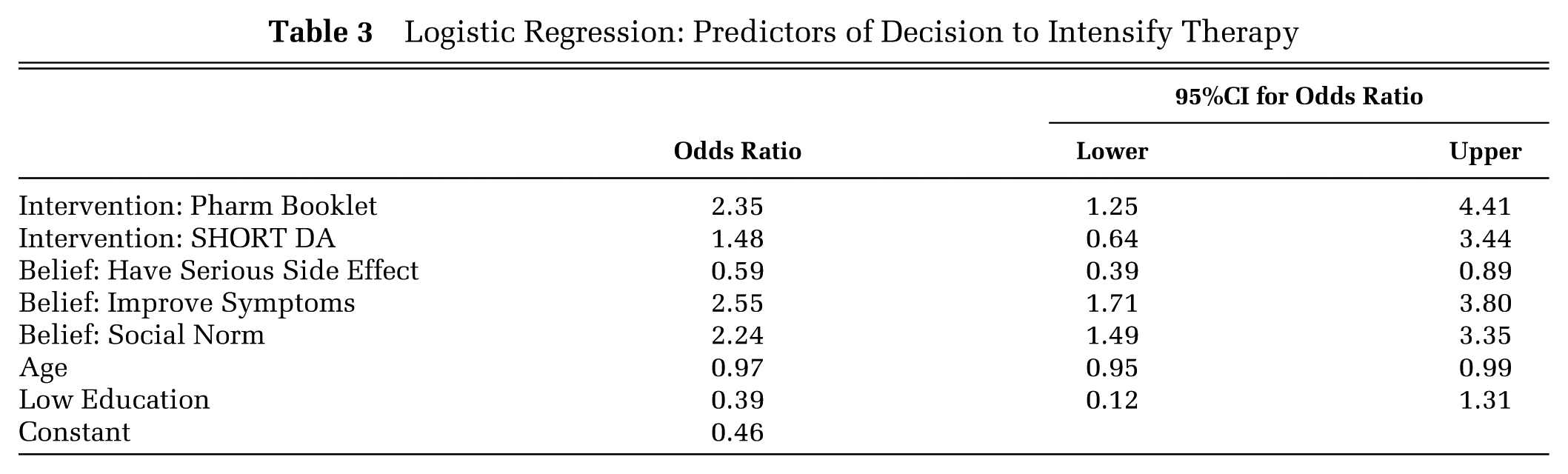
The results are summarized in Table 3. The odds ratios of covariates predicting choice to intensify therapy were: Belief: Improve Symptoms, 2.55, 95%CI = 1.71 to 3.80; Intervention: Pharm Booklet decision support 2.35, 95%CI = 1.25 to 4.41; Belief - Social Norm 2.24 95%CI = 1.49 to 3.35; Belief: Have Serious Side Effect, 0.59, 95%CI = 0.39 to 0.89; and Age, 0.97, 95%CI = 0.95 to 0.99. The regression coefficients for low educational level and SHORT DA were not significant.
Logistic Regression: Predictors of Decision to Intensify Therapy
Mediation Analysis
We next performed a mediational analysis to examine whether the decision support intervention’s effect on the intention to take etanercept was mediated by patient beliefs about etanercept. As can be seen in Figure 3, the decision support intervention had a significant relationship with the intention to take etanercept (0 to 9 scale), such that patients given the Pharm Booklet indicated a higher intention of taking the drug than those given the Decision Aid. The intention to take etanercept was strongly related to the decision to take etanercept in a single factor logistic regression model (R2 = 0.582). In terms of patient beliefs, the decision support intervention only had a significant effect on the belief that symptoms would improve and the normative beliefs about etanercept, so only these were used as mediators. The Pharm Booklet group was more likely to believe that their symptoms would improve and that most people like themselves would choose to take etanercept compared to the Decision Aid group. Increases in both patient beliefs were then associated with increases in the patients expressed intentions of taking etanercept. Once we accounted for the mediators, the direct effect of the decision support intervention was no longer significant. Furthermore, the indirect effect of decision support intervention was significant through both mediators. Taken together, this suggests the effect of the decision intervention on patients’ intention to take etanercept was mediated by patients’ beliefs about the medication.
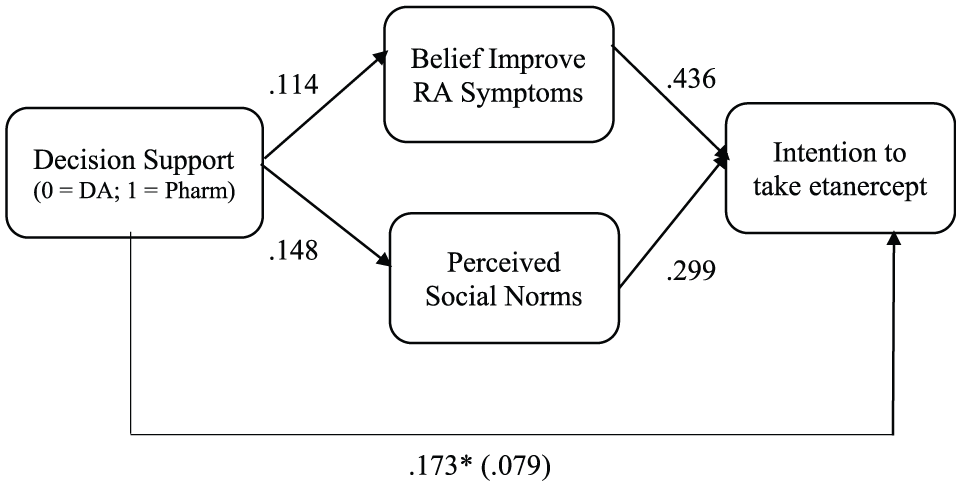
Mediational model of the intervention on patient intentions. Total indirect effect: b = 0.094*. Indirect effect through “Belief Improve RA Symptoms”: b = 0.050*. Indirect effect through “Perceived Social Norms”: b = 0.044. * Indicates P < 0.05. Indicators of significance for the indirect effects were obtained using 5,000 bootstrap resamples.
Discussion
Patients may face complex decisions when they consider a proposal to intensify medical therapy. To make an informed choice, patients should have accurate beliefs about the safety and efficacy of a proposed therapy. There is a renewed debate regarding the ethics of the content in direct-to-consumer pharmaceutical advertising, 37 which is relevant to pharmaceutical company “patient decision guides” distributed by industry representatives to physicians. The basis of the argument is that patients must be able to make decisions that are consistent with their personal values and that they are formed by a reliable method. 38 However, in addition to providing information, pharmaceutical advertisements construct persuasive messages aimed to induce a positive attitude about their product by pairing it to another object to which the patient already has a positive attitude. 39 The psychological term for this is evaluative conditioning. The product can be paired with: an image which evokes a hopeful, positive mood, 38 a celebrity testimonial, 40 or by describing a norm of how most people who choose in this situation (Social Norm); i.e., with a salient patient testimonial. 40
All 3 of these approaches are utilized in the Pharm Booklet used in our study. There are images of African-American, Hispanic and Caucasian adults participating in physical activities in beautiful outdoor settings making statements that include words like: “good”, “tremendous”, “manageable”, “well”, “healthier”, “relief”, and “active lifestyle”. In addition, there is a testimonial from the popular “Hall of Fame” golfer Phil Mickelson, who takes etanercept for psoriatic arthritis.
Overall, it is unknown how strong the effects of any of these methods of evaluative conditioning are on the formation of beliefs about medications and patients’ responses to a physician’s recommendation to intensify therapy. 38 An ethical conflict arises if the Pharm Booklet produces positive beliefs about drug safety and efficacy that are not fully accurate, yet shape the patient’s choice toward adopting the new therapy. In this case, the persuasive materials undermine patient autonomy, as the medication decision might be based on an emotional response rather than an appraisal of the facts about efficacy and safety. 38
Our study attempts to begin to unravel the question of what effects evaluative conditioning could have by comparing the Pharm Booklet to decision aids. PtDA are purposefully designed without using persuasive strategies, presenting benefits and harms neutrally, often supporting numerical information with visual aids to reduce the cognitive load and aid in the accurate understanding of the probabilities.41, 42
Exposure to the Pharm Booklet doubled the rate of patient choice to intensify therapy (increased absolute rate of adoption by 17%) as compared with the SHORT DA and the LONG DA. We demonstrated that both DAs produced a greater increase in relevant knowledge but that the greater knowledge and feeling of being informed did not have an impact on the patient’s beliefs about medication, decisional conflict, or their choice to intensify therapy.
The Integrative Model of Behavioral Prediction proposes that intention and ultimate adoption of a new therapy can be predicted by 3 types of beliefs: 1) expected outcomes of therapy, 2) social norms, and 3) self-efficacy to act on the intention. 31 In Figure 4, we conceptualize how patient characteristics, decisional support, and potential mediating medication beliefs could influence decisional outcomes. In the current study, predictive models demonstrate a stronger relationship between beliefs about outcomes of therapy and social norms on decisional outcomes than patient characteristics. In addition, it appears the mechanisms of the Pharm Booklet’s effects are partially mediated through persuasive communication techniques that influence patients’ belief symptoms: This will improve and increase social normative beliefs rather than by increase relevant knowledge, clarifying patient values about positive or negative treatment outcomes, or increasing their self-efficacy.
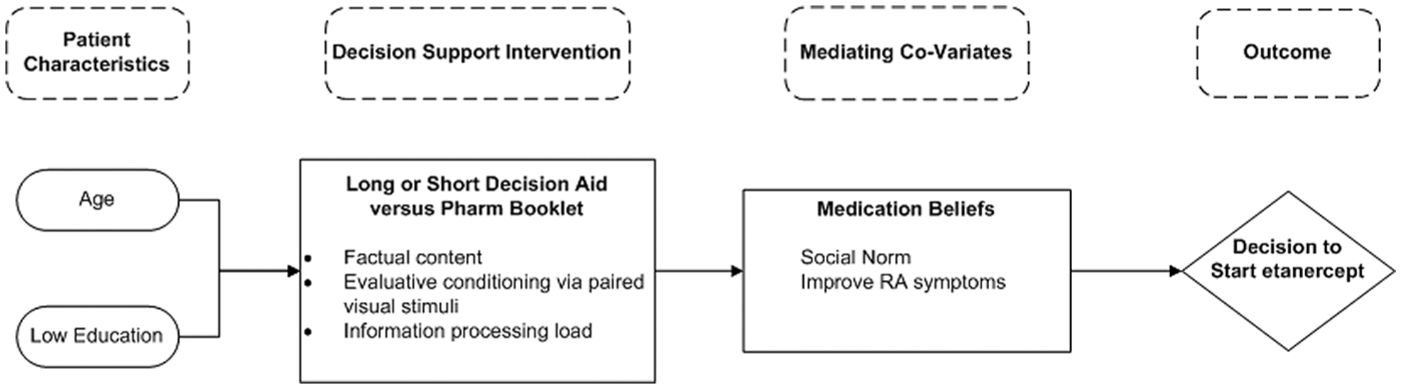
Simplified model of the effects of decisional support on the choice to intensify therapy.
Our study has several limitations. First, it was a simulated decision rather than a high-stakes, real-time clinical decision. In addition, it was conducted as a mail survey; thus, we cannot be sure how much time or effort patients expended in reviewing the decisional support materials. We expected some variation amongst patients, as the incomplete utilization of decision aids by patients has been previously reported and may relate to the salience of materials to the individual patient.43,44 Another uncertainty is the effect of the design of the decision/choice set in the PtDAs. The choice architecture of the LONG and SHORT DA directed the patient to consider 5 choices: take no treatment, continue current treatment, begin Enbrel now, ask doctor about other options, and defer choice for now. This reflects real-world conditions, where PtDA are often used as an adjunct to the medical office visit. It frames the decision as more than, “should I take or reject the proposed therapy now” to a broader starting point of “do I want to take any treatment for RA” and removes limits to the time of deliberation while considering “do I need other information or to consider additional options”. Because our simulated decision was an experiment, we forced subjects to make a choice “to call to request a prescription to start Enbrel now” or “choose not to start Enbrel now”. For this reason, our results may not fully reveal how decision support performs in the field. However, in some ways this may mimic real ambulatory practice where a physician introduces treatment options and send the patient home with support materials to reflect on their preferences and choose. Alternatively, by choice bracketing—i.e., reducing from a 5-choice set to 2 choices: 1. start Enbrel now v. 2. choose not to start Enbrel now (no treatment, continue current treatment, ask about other options, defer choice for now)—it is possible that we could have introduced a broad bracketing effect. 45 This could potentially result in different patient choices than in a clinical setting, where all 5 choice options are available. The direction and magnitude of this effect is context specific and could not be predicted with the current study design.
Given the respondent burden to read educational materials and complete a pre- and post-survey, we felt the response rate was excellent at 52%. We compared the demographics of the original sample frame with the completed sample and found them to be similar. When compared to a random sample of patients seen in Michigan community rheumatology practices, our completed sample contained a lower proportion of low-education patients (6.2% v. 14.2%) but a similar minority representation (6.3% v. 7.3%). 2 Together, these suggest that the results can be reasonably generalized to other community rheumatology practice populations, though additional study is needed in low education populations.
In conclusion, this study has several implications for practice and policy. Schwartz and Woloshin of the Dartmouth Center for Health Policy and Practice have lobbied the FDA and legislators to revise their policies to mandate providing medication efficacy data and create new standards for presenting side effect data in non-biased formats to patients.8, 9 Unfortunately, the FDA deferred action for an undisclosed 3- to 5-y study period. 7 The results of our study provide further evidence that the choice architecture in the Pharm Booklet contained powerful, persuasive content that may lead patients to develop inaccurate beliefs about the efficacy or safety of the treatment, and it undermines their decision making autonomy. From a societal viewpoint, these Pharm Booklets could lead to the overutilization of recommended medications by nudging patients toward adopting proposed commercial products without a critical consideration of the drug attributes. PtDA offer a balanced alternative that clinicians could use to structure complex medication discussions and support more informed patient choices. We believe patients would benefit from their use.
Footnotes
Acknowledgements
The authors would like to thank Michael Frisby of the Michigan State University Center for Statistical Training and Consulting for assistance with developing and interpreting the logistic regression models as well as Blake Riek, PhD of Calvin College Department of Psychology who conducted the mediation analysis. We would like to acknowledge past students including PJ Gallagher, EJ Turbergen, BM Martin and our research coordinator Dawn DeBois for their contributions to study. In addition, we are grateful to the many generous patients at West Michigan Rheumatology who participated in this study or other phases of the Rheumatoid Arthritis Shared Decision-Making Initiative. Finally, we would like to thank the reviewers and editors of MDM for their valuable feedback on the manuscript.
The investigators funded this work, which ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. They have no financial interest in any form that could create a potential conflict of interest or the appearance of conflict of interest with regard to this work. The Enbrel Decision Guide booklets were provided, for the study, at no cost, by Amgen. Amgen was not involved in patient selection, data collection, data analysis or writing of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.