
Abstract
Prior literature has suggested that following exposure to family violence, adolescents can develop internalizing and externalizing symptoms, including bullying perpetration and depressive symptoms. However, incongruities suggest that exposure to family violence is not a consistent precipitating event associated with bullying perpetration and depressive symptoms. Therefore, using latent growth models, the current study applied the intergenerational transmission of violence and emotional security theories to investigate the developmental co-occurrences of depressive symptoms and bullying perpetration and longitudinal effects of exposure to family violence on bullying perpetration and depressive symptoms across four time points in middle school (i.e., from grades 6 to 8; n = 1,585; Mage = 11.23 in grade 6; SD = .45). Consistent with expectations, results of the latent growth models indicated that exposure to family violence was positively associated with adolescents’ concurrent bullying perpetration and depressive symptoms. These effects were evident across the middle school years. Implications are discussed.
The adolescent developmental period is a critical time in which youth often develop externalizing and internalizing symptoms even if they did not display such patterns in childhood (Achenbach et al., 2016; Fleming & Offord, 1990; Moffitt, 1993). Externalizing symptoms include aggressive conduct such as bullying perpetration, which refers to repetitive intentionally aggressive behavior characterized by threatening to harm someone, and acts of physical aggression such as kicking, slapping, and punching (Bonanno & Hymel, 2013; Olweus et al., 2019; Smith et al., 2002). In contrast, internalizing symptoms include depression, mood disturbances, concurrent feelings of sadness, withdrawal, and lack of energy, as well as suicidal ideation, and sleep disturbances (Achenbach et al., 1987; Auerbach et al., 2011; Hughes & Gullone, 2010). Although bullying perpetration and depressive symptoms are typically viewed as distinct behavioral manifestations, reflecting unique disturbances in adolescents social and emotional development, they may also co-occur during the early adolescence developmental period (e.g., ages 10–13), and subsequently exacerbate and influence adverse outcomes including academic difficulties, loneliness, juvenile delinquency, social withdrawal, and substance use (Arango et al., 2016; Katz et al., 2011; Lahtinen et al., 2020; Willner et al., 2016).
Despite substantial individual differences in rates of bullying perpetration and depressive symptoms among adolescents, researchers have been interested in investigating normative developmental trends of depressive symptoms and bullying perpetration in early adolescence, as they may be related to typical emotional and physiological changes during this period (Reinke et al., 2012). For instance, Prince et al. (2023) found that normative hormonal changes and fluctuating emotional maladjustment to daily stressors may contribute to the development of increasing levels of depressive symptoms (e.g., chronic sadness, fatigue, and insomnia). There is also evidence that suggests during the early adolescent period, youth undergo cognitive changes and seek peer approval for identity formation, which are often connected to emotional disturbances and eventual depressive symptoms (Hamilton et al., 2014; Prinstein & Aikins, 2004). Pertaining to bullying perpetration, literature has highlighted that bullying perpetration often peaks during early adolescence due to attempts to establish a high peer status (Pellegrini & Long, 2002), fear of rejection (Boulton, 2013), and self-control difficulties (Kretschmer et al., 2017). These patterns can be considered normative and an adaptive mechanism to enhance status with peers who witness bullying and, unfortunately, often reinforced by peers in school settings (Salmivalli et al., 2011). Although these patterns appear to be typical in early adolescence, prior literature has noted that depressive symptoms and bullying perpetration tend to subside over time (Ellis et al., 2017; Espelage et al., 2018).
Prior studies have highlighted the potential co-occurrence of depressive symptoms and engaging in bullying perpetration (Lawrence et al., 2025; Siennick & Turanovic, 2024). Considering their co-occurrence, it may be informative from an etiological perspective to identify potential common risk factors. Consistent with principles of multifinality such that one risk factor may lead to multiple distinct outcomes (Cicchetti & Rogosch, 1996); a common risk factor is considered here to be one that may be predictive of both bullying perpetration and depressive symptoms. Scholars have suggested that environmental stressors, including adverse home (e.g., neglect, parental incarceration, rejecting and neglecting parenting styles) and school (e.g., bullying victimization and peer rejection) experiences may be common risk factors associated with the co-occurring development of adolescents internalizing and externalizing behaviors (Holfeld & Mishna, 2019; Jung et al., 2017; Shi et al., 2020). While the etiology of bullying perpetration and depressive symptoms are multifaceted, in the current study, we examined whether exposure to family violence, which refers to witnessing or hearing violent acts and behaviors within the home, may be a robust predictor of both outcomes (Hawkins et al., 2019; Lawrence, 2022b). During the transition to adolescence, not only are early adolescents facing biological changes associated with pubertal development, they are also encountering social and academic challenges as they are transitioning to a new middle school environment in which they are exposed to a more departmentalized classroom structure, and larger peer groups which are also becoming more influential. Family dynamics may be particularly important during this transitional period, as adolescents are navigating potentially unfamiliar and stressful, peer and school contexts.
Although having a secure family environment may be an important resource for adolescents to navigate these complex changes, exposure to family violence taxes adolescents’ emotional coping abilities and disrupts the sense of safety within the home (Chester & Joscelyne, 2021). These stressors subsequently elicit emotions such as anger and fear and create a hypervigilance schema that guides the ways in which adolescents navigate their social and interpersonal relationships (Lawrence, Hong, Sopchak, & Voisin, 2023; Moses & Villodas, 2017; Reyes et al., 2015). Thus, exposure to family violence may create a context of stress and insecurity which may exacerbate adolescents’ maladjustment and contribute to increasing rates of bullying perpetration and depressive symptoms across the middle school grades.
Theoretical Framework
According to the Intergenerational Transmission of Violence (ITV) model, following exposure to family violence, children and adolescents develop aggressive scripts that shape and guide subsequent behavior in unrelated situations (Black et al., 2010; Widom, 1989; Widom & Wilson, 2015). Due to the socially reinforcing tenements that underlie this model, existing scholarship often explains this framework through the social learning model, which suggests that while individuals are exposed to violence, they learn that aggressive behavior is an acceptable tactic in resolving conflict (Chapple, 2003; Dunlap et al., 2002; Mihalic & Elliott, 1997). There is widespread support for the ITV model (Carr & VanDeusen, 2002; Heyman & Slep, 2002; Milletch et al., 2010), such that adolescents’ exposure to family violence has been associated with aggressive behavior consistent with bullying perpetration (Baek et al., 2019; Grant et al., 2019). Although the ITV model has robust empirical support linking exposure to family violence to bullying perpetration, this model does not adequately explain the pathogenesis of internalizing symptoms. Therefore, to explain the link between exposure to family violence and depressive symptoms, we drew on the Emotional Security Theory (EST).
Under the tenements of the EST, familial discord, including exposure to family violence disrupts the sense of safety among children and adolescents. These adverse family experiences contribute to increased emotion dysregulation and elicit intense anger and fear that undermines the sense of security in the home, negatively impairing the parent-child relationship (Cummings & Davies, 1996). A substantial body of research has demonstrated that these psychologically distressing events are likely to increase the risk for adolescents to develop both externalizing and internalizing symptoms, (Alegre et al., 2014; Cummings et al., 2013; Cummings & Miller-Graff, 2015; Davies et al., 2016a, 2016b).
Despite the theoretical utility of these models in explaining developmental pathways of bullying perpetration and depressive symptoms following exposure to family violence, there are several limitations that warrant further exploration. That is, these models have typically examined the consequences of exposure to family violence among early adolescents separately, which presents as a potential conceptual limitation. It is possible these theoretical frameworks provide competing or alternative viewpoints on the underlying processes or mechanisms by which family violence may exert an effect. For instance, because the ITV primarily focuses on how adolescents may model aggressive behaviors after exposure to family violence, this perspective may not adequately explain how family violence exposure could also trigger internalizing disturbances (e.g., depressive symptoms).
Applying this perspective, it could be the case that family violence is likely to have a stronger and more consistent effect on adolescents’ bullying perpetration compared to their depressive symptoms. Alternatively, when applying perspectives drawn from the EST, this model underscores how family violence exposure may also undermine adolescents’ affective regulation, which is likely to exacerbate their internalizing symptoms (e.g., depressive symptoms). Thus, in the current study we sought to simultaneously examine the effects of family violence on the co-occurring development of adolescent’s externalizing and internalizing behaviors to further assess whether its effects are potentially stronger on either of these outcomes, while controlling for their co-occurrence. This approach would allow us to make inferences in terms of whether the ITV model and EST provide complementary versus competing perspectives pertaining to the potential associations of family violence on changes in early adolescents’ internalizing and externalizing symptoms.
Empirical Evidence on the Associations of Family Violence With Adolescents’ Bullying Perpetration and Depressive Symptoms
As previously mentioned, literature has noted that exposure to family violence is a common risk factor for depressive symptoms and bullying perpetration. For example, Lawrence et al. (2022c) found that exposure to family violence positively predicted bullying perpetration. These results were further corroborated and extended by Gao et al. (2025), suggesting that exposure to family violence increases internal hostility and peer conflicts, which leads to externalizing conduct such as bullying perpetration. Furthermore, meta-analytic literature indicated that adolescents who were exposed to family violence were significantly more likely to engage in bullying perpetration than their non-exposed counterparts across various studies (Nocentini et al., 2019). Lee et al. (2022) found that across 12 studies, adolescents who were exposed to family violence were more likely to engage in bullying perpetration over time. In contrast, the current literature also suggests that exposure to family violence leads to emotional disturbances consistent with depressive symptoms (LaMontagne et al., 2023; Rivers et al., 2022). These studies were further supported by meta-analytic literature that shows exposure to family violence subsequently leads to a developmental pathway of depressive symptoms (Chen et al., 2023; Wang et al., 2025). More specifically, across fifty-three studies, adolescents who were exposed to some form of family violence, including witnessing physical fights and chronic screaming and yelling in the home, were more likely to endorse depressive symptoms (Whitten et al., 2024).
Overall, although the literature has highlighted the detrimental effects of exposure to family violence on subsequent depressive symptoms and bullying perpetration, there are inconsistencies in the literature. For instance, some previous studies suggest that exposure to family violence does not significantly predict bullying perpetration and depressive symptoms (Chen et al., 2017; Sternberg et al., 2006). Additionally, Knous et al. (2012) suggested that after controlling for prior internalizing and externalizing symptoms, exposure to family violence did not statistically predict bullying perpetration. Some attribute these inconsistencies to measurement differences (e.g., cross-sectional, and longitudinal designs; Ingram et al., 2020). In addition to these inconsistencies, one central gap exists in the literature. More specifically, few studies have investigated how the relative onset and growth rate of depressive symptoms and bullying perpetration in early adolescence may be associated with family violence exposure. This is an important gap to address because prior literature has shown that as early adolescents undergo psychological and physical changes, they are susceptible to engaging in bullying behavior and endorsing depressive symptoms (Iyer et al., 2013), and family violence exposure may function as a common risk factor which undermines their capacity to effectively handle these changes. Furthermore, given that adolescents’ bullying perpetration and depressive symptoms are likely to co-occur, it may be important to examine the simultaneous associations of family violence exposure on both aspects of adjustment.
Study Aims and Hypotheses
The current study aims to estimate the predictive effects of exposure to family violence on the onset and rate of change of bullying perpetration and depressive symptoms in early adolescence as youth were progressing through middle school. Towards this end, we undertook three interrelated objectives. First, we examined the normative development (trajectories) of adolescents’ bullying perpetration and depressive symptoms across the middle school years, grades 6 to 8. We hypothesized that both bullying perpetration and depressive symptoms would exhibit a normative increase in early adolescence as youth adjusted to middle school, and would subsequently subside during this period (i.e., by Grade 8). Second, we examined the co-occurrence of adolescents’ bullying perpetration and depressive symptoms during this time. More specifically, we hypothesized that initial levels of adolescents’ bullying perpetration and depressive symptoms (i.e., intercepts in Grade 6) would be positively correlated. We also expected that rates of growth (i.e., slope effects) would be positively correlated (i.e., adolescents who exhibited an increase in bullying perpetration over time would be more likely to have an increase in depressive symptoms). Third, we examined the predictive effects of family violence exposure on adolescents’ bullying perpetration and depressive symptoms. Consistent with the ITV and EST perspectives, we posited that higher levels of family violence exposure would be disruptive for adolescents’ adjustment across the middle school years and that these experiences would create persistent challenges during this time. Consequently, we hypothesized that family violence exposure would be positively associated with both initial levels and increasing rates of change (i.e., intercept and slope effects, respectively), of bullying perpetration and depressive symptoms.
Method
Participants
Data for the current study came from a program evaluation of the Second Step program conducted in two Midwestern states in the United States (Espelage et al., 2013). Students from 36 middle schools were recruited into the longitudinal study, and schools were matched and randomly assigned into treatment (intervention) and control schools. For the purposes of the current study, we used data from the 18 schools which were part of the control condition. The current study relied on secondary data analysis using publicly available data from Inter-university Consortium for Political and Social Research (ICPSR; https://www.icpsr.umich.edu/web/ICPSR/studies/36726). The publicly available dataset included 4,718 cases. This included 3,616 students who were recruited into the longitudinal study in Grade 6 (see Espelage et al., 2013), as well as additional children who were added to the study in subsequent grade levels over the course of the longitudinal project. For the purposes of the current study, and given the longitudinal design, we used data for students who were recruited into the study in Grade 6, and part of the control condition. More specifically, at the baseline assessment (Wave 1 conducted in Fall of Grade 6), there were 1,697 students who were identified as being in the control condition. Over the course of the longitudinal project, some students (n = 112) changed schools and were reassigned to the intervention condition, and these students were excluded from the current analyses due to having exposure to the intervention program, resulting in 1,585 students as the sample size for the current study (at the baseline assessment, Mage = 11.23; SD = .45). The sample was evenly distributed in terms of gender (51.2% boys and 48.8% girls), and consisted of 26.3% African American, 19.6% White, 38.2% Hispanic/Latino, 3.4% Asian American, and 12.4% identified as biracial or other.
Procedure
Parents of all students received a consent letter explaining the purpose and risk of the study. Youth whose guardians had not granted consent were removed from administration rooms once surveys were presented. Furthermore, for students who had received parental consent, an assent form was also signed and returned to trained assistants. School based data collection occurred over a period of three years, as students progressed through middle school (Grades 6 to 8). Data collection occurred across 4 waves including assessments conducted in Fall (Wave 1) and Spring (Wave 2) of Grade 6, Spring of Grade 7 (Wave 3) and Spring of Grade 8 (Wave 4). Prior publications with this current dataset (e.g., Espelage et al., 2018) appear to indicate that portions of this sample were also followed into high school (with three additional waves of data collection conducted); however, due to changes in the sampling design and availability of measures made after youth transitioned into high school, it was not possible in the current study to utilize data beyond the middle school years. Thus, the current study utilized waves 1 through 4 in which students completed several survey questionnaires with consistent (repeated) measures of adolescents’ bullying perpetration and depressive symptoms.
Measures
Exposure to Family Violence
Exposure to family violence was measured at Wave 1 using 3 items from the Family Conflict and Hostility Scale which were drawn from the Rochester Youth Development Study (Thornberry et al., 2003). This scale measured the degree to which adolescents’ perceived conflict and hostility in the household by assessing loss of temper, frequent arguing, and physical violence by family members at home. Items included, “How often are there physical fights in the household?”, “How often is there yelling, quarreling, or arguing in your household?”, and “How often do family members lose their temper or blow up for no good reason?”. Responses were scored on a 5-point Likert scale ranging from 0 (never) to 4 (always), and this measure exhibited adequate internal reliability within the current sample (α = 79).
Depressive Symptoms
Depressive symptoms were measured in Waves 1 to 4, using nine items from the Orpinas Modified Depression scale (Orpinas, 1993). This scale measured the frequency of various depressive symptoms including irritability, sadness, worrying, hopelessness, and nervousness within the past 30 days. Example items included, “Did you feel hopeless about the future?”, “Did you worry a lot?”, Were you very sad?”, and “Did you feel nervous or afraid that things won’t work out the way you would like them to?”. Items were scored on a 5-point Likert scale ranging from 0 (never) to 4 (almost always), with higher scores reflecting more depressive symptoms. This measure exhibited adequate internal reliability within the current sample (αs ranged from .81 to 86 in Waves 1 to 4).
Bullying Perpetration
Bullying perpetration was measured in Waves 1 to 4 using 7 items from the Illinois Bully Scale (Espelage & Holt, 2001). This measure assessed how often in the past 30 days students engaged in various forms of physical, relational and verbal bullying. Example items included, “I spread rumors about other students”, “I excluded other students from my clique (group) of friends”, “I helped harass other students”, and “I threatened to hurt or hit another student.” Items were scored on a 5-point Likert scale ranging from 0 (never) to 4 (seven or more times). Prior literature has supported the construct validity of this instrument, which was strongly correlated with peer nominations of bullying perpetration (Espelage et al., 2003). This measure exhibited adequate internal reliability within the current sample (αs ranged from .79 to .83 in Waves 1 to 4).
Data Analysis Plan
First, preliminary analyses were conducted in SPSS (version 28) to assess patterns of missing data, descriptive statistics, and bivariate correlations. Second, latent growth curve modeling was conducted in Mplus (version 8) to examine the longitudinal associations of family violence on adolescents’ bullying perpetration and depressive symptoms. To handle missing data, full information maximum likelihood (FIML) estimation was used which includes all cases with available data, and the maximum likelihood robust (MLR) estimator was used which accounts for non-normality when estimating standard errors. Model fit was assessed using the recommendations of Hu and Bentler (1999), such that models were deemed to have adequate fit if the RMSEA <.06, SRMR <.08, and CFI >.95.
Growth modeling was conducted in two parts. First, unconditional latent growth models were specified for bullying perpetration and depression to assess the growth patterns for each construct separately, across Waves 1 to 4. For each construct, a series of linear and non-linear (quadratic) growth models were specified, and nested model tests were used to compare models. Given the use of MLR, nested model comparisons consisted of Satorra-Bentler adjusted chi-square difference tests (Satorra, 2000). After determining the optimal growth pattern for each construct, a parallel process growth model was estimated for bullying perpetration and depressive symptoms simultaneously, across Waves 1 to 4. The latent growth parameters included estimates for the intercept factor, which reflected baseline (Wave 1) scores for bullying perpetration and depressive symptoms, and slope and quadratic factors which estimated linear and non-linear changes in bullying perpetration and depressive symptoms from Wave 1 to 4. These growth parameters were correlated with each other to account for co-occurring changes in bullying perpetration and depression over time. Family violence was specified as a predictor (exogenous variable) and included path estimates to the growth parameters for bullying perpetration and depressive symptoms. Race, age and gender were included as control variables predicting the growth factors and correlated with family violence. An example of the complete path model based on the parallel process growth model is illustrated in Figure 1. Illustrative example of conditional growth model examining associations of family violence on adolescents’ bullying perpetration and depressive symptoms trajectories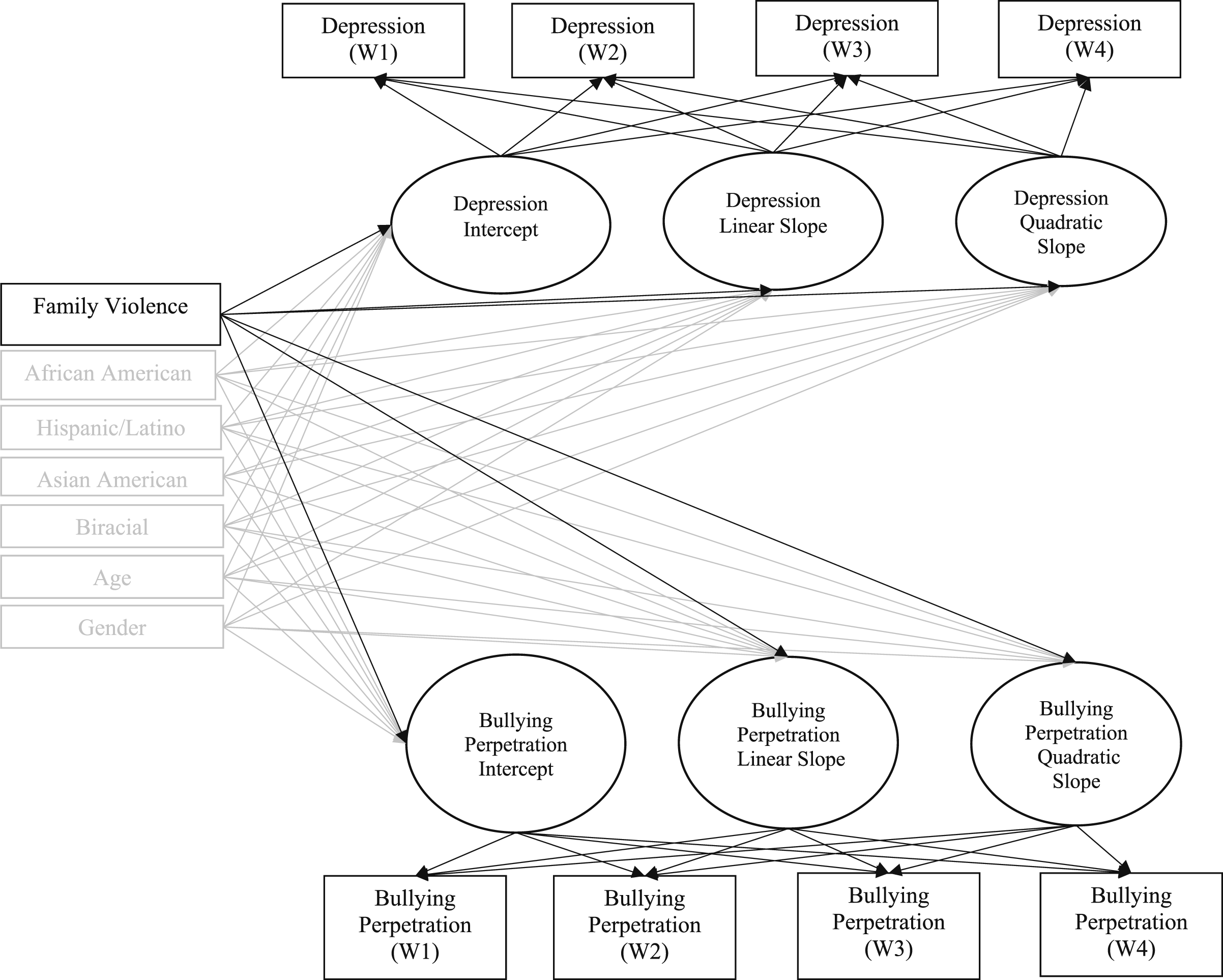
Results
Preliminary Analyses (Missing Data, Descriptive Statistics, and Bivariate Correlations)
Missing data analyses were performed to assess patterns of attrition over the course of the longitudinal project. Results indicated that missing data increased over time, with an average of 4% missing data at Wave 1, 15% at Wave 2, 32% at Wave 3, and 42% at Wave 4. To assess whether there were observable patterns of attrition, a series of univariate t-tests were performed to examine whether rates of missing data differed by students’ gender, and ethnicity. Results indicated some significant differences across demographic groups, but the findings were inconsistent. More specifically, Hispanic students had significantly more missing data and Black students had significantly less missing data on the depression measure in Wave 1, but not on bullying perpetration. In Waves 2, 3, and 4, Hispanic students had significantly less missing data, and in Waves 3 and 4, Black students had significantly more missing data. Although these findings were inconsistent, to account for these demographic differences, race and ethnicity were included as covariates in all subsequent growth models.
Descriptive Statistics and Bivariate Correlations Among the Study Variables
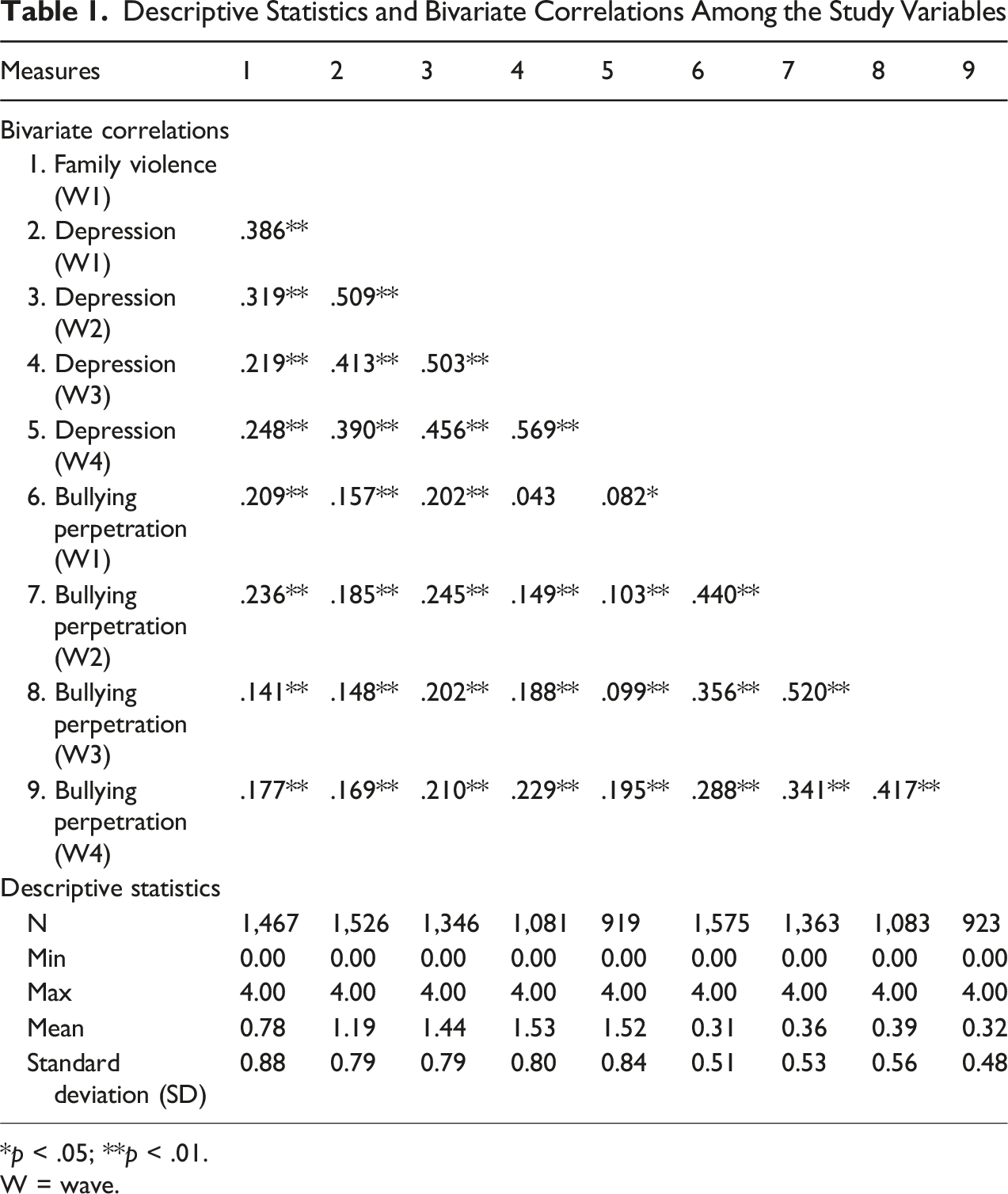
*p < .05; **p < .01.
W = wave.
Unconditional Latent Growth Model Results
Unconditional growth models were specified for bullying perpetration and depressive symptoms separately. For bullying perpetration, the model comparisons indicated that the non-linear growth model including a quadratic effect had adequate overall model fit (χ
2
= 2.60, df = 1, p = .11; RMSEA = .03, SRMR = .01, CFI = .995), and significantly better fit compared to the linear growth model (χ
2
= 39.46, df = 5, p < .001; RMSEA = .07, SRMR = .05, CFI = .884; scaled Δχ
2
= 34.23, df = 4, p < .001). Considering the mean estimates for the growth parameters, (M
intercept
= .30, p < .001; M
slope
= .13, p < .001; M
quadratic
= −.04, p < .001), it appeared that bullying perpetration exhibited a significant increase over time with a sharper increase in earlier waves, peaked in Wave 3 (Grade 7), and then had a slow declining effect by the final wave (see Figure 2(a)). Unconditional growth models examining adolescents’ bullying perpetration (a) and depressive (b) trajectories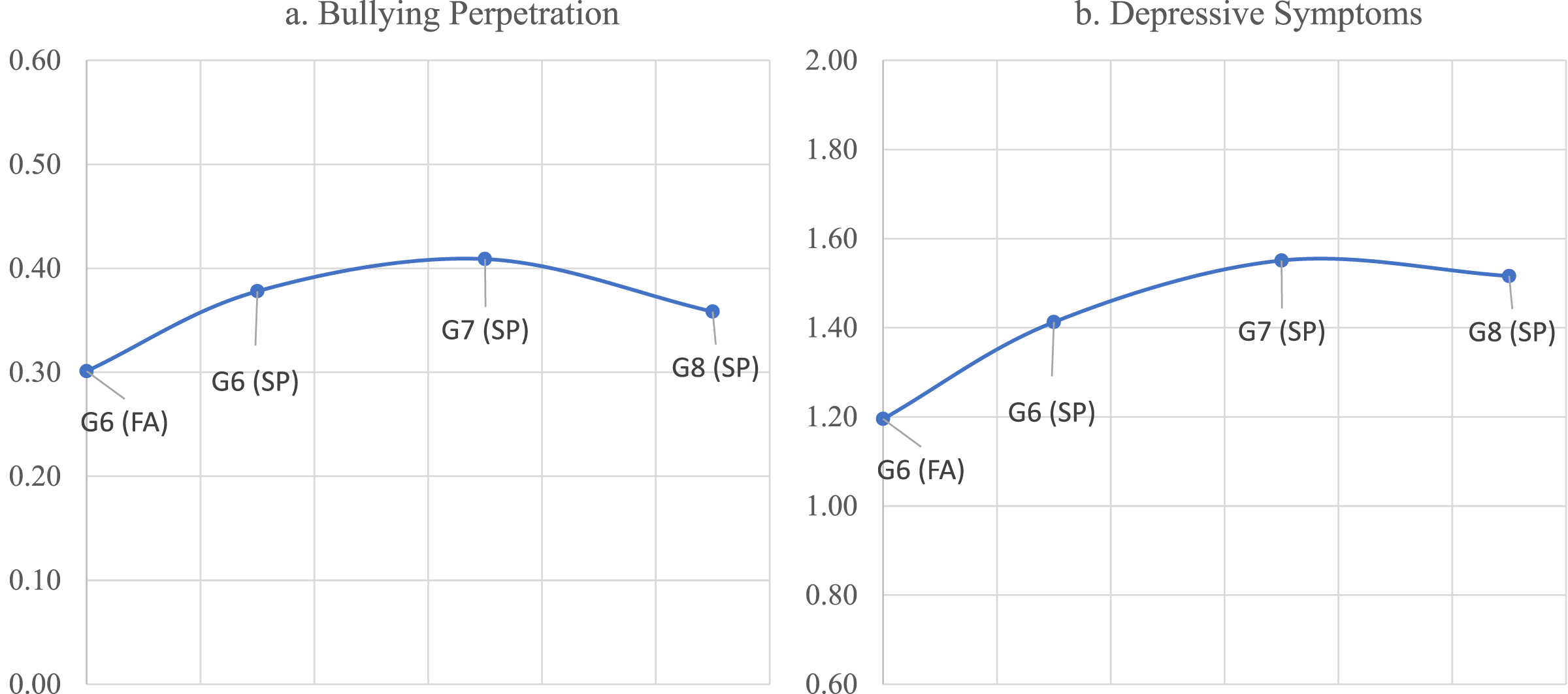
For depression, the model comparisons indicated that the non-linear growth model including a quadratic effect had adequate overall model fit (χ 2 = 3.11, df = 1, p = .08; RMSEA = .04, SRMR = .01, CFI = .997), and significantly better fit compared to the linear growth model (χ 2 = 67.87, df = 5, p < .001; RMSEA = .09, SRMR = .05, CFI = .916; scaled Δχ 2 = 62.47, df = 4, p < .001). Considering the mean estimates for the growth parameters, (M intercept = 1.20, p < .001; M slope = .36, p < .001; M quadratic = −.09, p < .001), it appeared that adolescents’ depressive symptoms exhibited a significant increase over time (from Waves 1 to 4), however the rate of change varied over time with a sharper increase in earlier waves, followed by a tapering effect in later waves (see Figure 2(b)).
Parallel Process Latent Growth Model Results
Based on the unconditional growth modeling results, the non-linear (quadratic) models for both bullying perpetration and depression were included in the parallel process growth model that was subsequently estimated. Model results indicated that the parallel process latent growth model exhibited adequate model fit (χ 2 = 43.30, df = 24, p < .01; RMSEA = .02, SRMR = .01, CFI = .99). To more closely evaluate the model results, we examined the effects of family violence on the bullying perpetration and depression growth parameters, the covariate effects of age, race, ethnicity and gender on the growth parameters, and the covariances (correlations) among the growth parameters.
Effects of Family Violence and Control Variables on Adolescents’ Bullying Perpetration and Depressive Trajectories
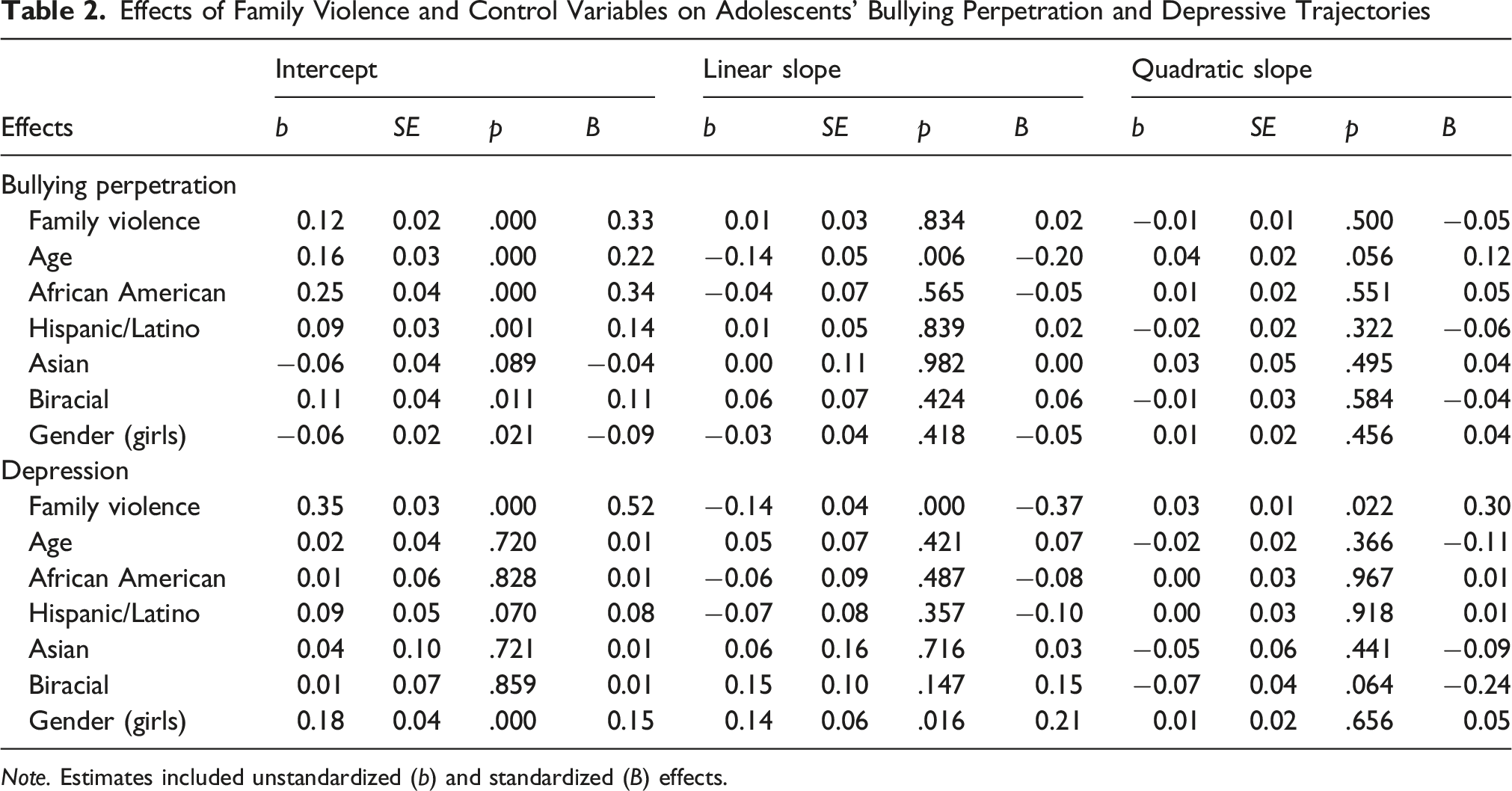
Note. Estimates included unstandardized (b) and standardized (B) effects.
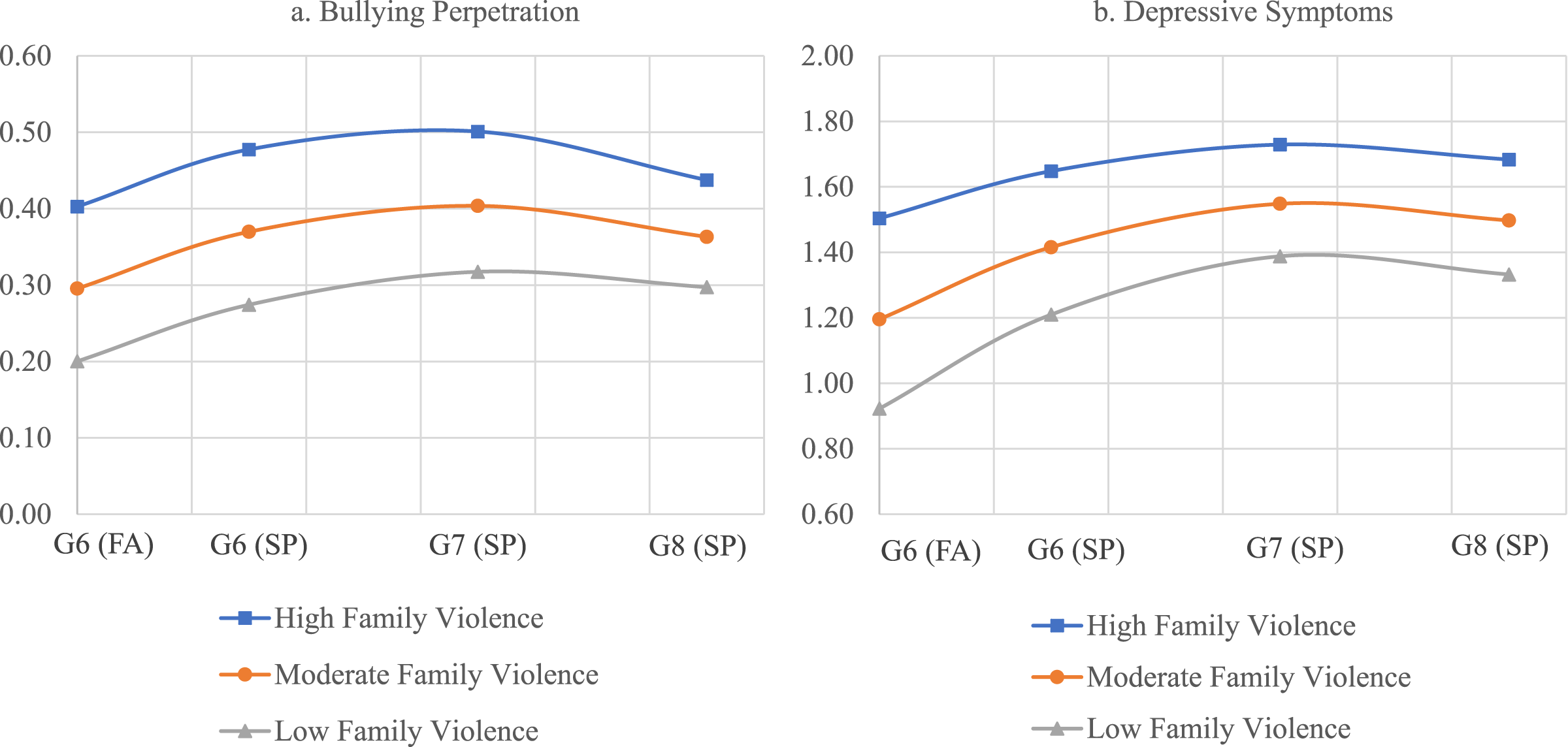
Conditional growth models examining effects of family violence on adolescents’ bullying perpetration (a) and depressive (b) trajectories
With respect to the covariate effects (see Table 2), the model results for bullying perpetration indicated a significant gender effect, such that girls had significantly lower baseline levels than boys. The significant intercept effects indicated that age was positively associated with higher baseline levels of bullying, and race and ethnicity effects indicated that Black/African American, Hispanic/Latino and biracial youth had higher baseline levels of bullying perpetration compared to White youth. The model results for depressive symptoms indicated a significant gender effect, such that girls had significantly higher intercept and slope effects than boys. Covariate effects for race, ethnicity and age were not significantly associated with depressive symptoms.
With respect to the correlations among the growth factors, the model results indicated that the latent intercept factors for bullying perpetration and depressive symptoms were positively correlated with each other (r = 23, p = .01). The intercept factors for depression and bullying perpetration were not significantly correlated with the slope and quadratic factors.
Discussion
The present study estimated the longitudinal onset and growth, and the co-occurrence, of bullying perpetration and depressive symptoms while applying the ITV and EST models to understand the pernicious effects of exposure to family violence on the developmental trajectories of depressive symptoms and bullying perpetration across four-time points. Our findings provided novel information and advanced the literature by highlighting normative trends in the developmental onset and growth rate of bullying perpetration and depressive symptoms in early adolescence and underscoring the detrimental effects of exposure to family violence during this developmental period. More specifically, youth with higher levels of family violence exposure in grade 6 exhibited higher concurrent levels of bullying perpetration and depressive symptoms, and these deleterious effects persisted across the middle school years (through grade 8).
Development and Co-Occurrence of Bullying Perpetration and Depressive Symptoms
Our first aim was to investigate the normative developmental growth patterns of bullying perpetration and depressive symptoms as adolescents progressed through middle school. The results were mostly consistent with our hypotheses regarding normative developmental trends but also underscored the differential developmental trajectories of bullying perpetration and depressive symptoms among early adolescents. More specifically, with respect to bullying perpetration, adolescents exhibited a significant increase during the early stages of measurement (i.e., from grades 6 to 7), with a peak in bullying perpetration in Grade 7, followed by a declining pattern thereafter (from grades 7 to 8). With respect to depressive symptoms, adolescents exhibited a significant increase during the early stages of measurement (i.e., from grades 6 to 7), followed by a tapering effect in which it appeared that rates of depression stabilized. These findings support the notion that during the early adolescent developmental period, there is a normative onset of both bullying perpetration and depressive symptoms in that both increased and declined or stabilized thereafter (Ellis et al., 2017; Espelage et al., 2018). These findings highlight how the simultaneous developmental transition to adolescence and contextual transition to middle school may serve as an important period in which there are significant shifts in adolescents’ behavioral and emotional adjustment. Although the biological and social changes that are occurring during this time can be viewed as being normative, they may also present challenges and introduce stressors to adolescents that may compromise their healthy adaptation. Toward this end, prior literature has shown that during the transition to middle school, adolescents often experience stress related to adjusting to the new environment and may experience anxiety about their social status among peers, which could lead to bullying behaviors (Shell et al., 2014; Wei & Chen, 2012).
Expanding on these normative developmental patterns, the results also revealed a positive correlation between the bullying perpetration and depressive symptoms intercept factors. This finding indicated that bullying preparation and depressive symptoms were co-occurring among adolescents, and that adolescents who were engaging in higher levels of bullying perpetration were also exhibiting higher levels of depressive symptoms, relative to other youth. Unlike prior studies that have separately examined bullying perpetration and depressive symptoms, these results advance previous findings by suggesting that these two particular forms of externalizing (bullying perpetration) and internalizing behaviors (depressive symptoms) are likely to co-occur as youth are transitioning into middle school. Notably, within the parallel process growth models, this correlation reflected a residual correlation, after accounting for the effects of family violence and other potential confounding demographic effects including gender, age, race, and ethnicity. This suggests that the co-occurrence of bullying perpetration and depressive symptoms was beyond what could be accounted for by family violence. On the one hand, it is possible that the social-contextual changes that are occurring during this period may exacerbate adolescents’ adjustment across multiple developmental outcomes. That is, adolescents who are having challenges adapting to middle school are likely to exhibit a combination of emotional disturbances characterized as irritability and psychomotor agitation and bullying perpetration behavior, such as name calling and physical violence. On the other hand, it is possible that there are underlying biological or dispositional factors (e.g., a general psychopathology or p factor) that are associated with the co-occurrence of multiple forms of externalizing and internalizing factors (Allegrini et al., 2020).
Exposure to Family Violence and Effects on Bullying Perpetration and Depressive Symptoms
We predicted that, following exposure to family violence, adolescents would be more likely to endorse depressive symptoms and engage in bullying perpetration. In general, the findings provided support for this assertion but also revealed insights with respect to the timing of these associations (i.e., differential effects on the growth parameters). More specifically, higher levels of family violence as adolescents were beginning middle school were associated with more elevated rates of bullying perpetration and depressive symptoms, which then persisted over the course of middle school. There are several possible theoretical and translational explanations for these associations. Theoretically, this result is consistent with the ITV model, which suggests that individuals who are exposed to family violence learn that violence and aggressive behavior are appropriate methods of handling conflict, which increases their chances of engaging in aggressive behavior (Black et al., 2010; Lawrence, 2022a; Tracy et al., 2018).
Consistent with the EST, these findings also indicated that exposure to family violence could have undermined the sense of safety and emotion regulation that creates the vulnerability for the onset of depressive symptoms. Translationally, these results highlight that as adolescents were exposed to high levels of family violence, they were more likely to engage in aggressive acts characterized as bullying perpetration at school while also endorsing depressive symptoms. Consistent with these findings, it is plausible that exposure to traumatic events (such as family violence) could impede self-regulatory practices that are necessary when navigating and maintaining interpersonal relationships (Evans et al., 2015; Kim et al., 2021; Lawrence, Hong, Espelage, & Voisin, 2023), and ineffective coping strategies and prolonged affective disturbances, which is consistent with prior studies (Espelage et al., 2014; Grant et al., 2019). Because adolescents who were exposed to family violence may exhibit increased hypervigilance, they may also misinterpret ambiguous situations and have difficulty recognizing emotional expressions (McCrory et al., 2011). Taken together, these findings highlight how exposure to family violence may be particularly detrimental for adolescents as it may compromise multiple developmental processes pertaining to adolescents’ self-regulatory mechanisms, coping strategies, attributional styles, and emotional security and functioning, which collectively appear to exacerbate their co-occurring externalizing and internalizing behaviors.
Contrary to expectations, the effects of family violence on the bullying perpetration growth parameters were not significant, and family violence was negatively associated with the depressive symptoms linear slope parameter (although it was positively associated with the quadratic factor). These findings indicated that family violence was more consistently associated with adolescents’ initial levels of bullying perpetration and depressive symptoms but was not associated with increasing symptomology. Although the reasoning for these non-significant findings are unclear, we consider several possible explanations. These findings may speak to the importance of assessing family violence over time by including repeated (i.e., time varying) assessments. To the extent that there are fluctuations or changes in adolescents’ family violence exposure as they progress through middle school, it is possible that the effects of family violence exposure may have diminished, or not persisted as strongly, over time. Expanding on this point, the transition to early adolescence, and middle school, is a period in which early adolescents are likely to experience multiple contextual stressors which extend beyond the family structure (e.g., larger and more bureaucratic school structures; multiple teachers which may reduce their teacher-student relationship quality; changes in their peer groups and social hierarchies which may contribute to increasing peer victimization), and how adolescents’ adapt to these changes are likely to contribute to changes (e.g., increases) in their depressive symptoms and bullying perpetration. An interesting direction for future research may be to examine its potential moderating effects to assess whether family violence exposure exacerbates other contextual stressors that adolescents may encounter during this time.
Study Strengths and Limitations
Among the strengths of the current study were a diverse sample and multi-year (4 wave) longitudinal examination of the co-occurring developmental trajectories of depressive symptoms and bullying perpetration in early adolescence. This approach has several benefits over cross-sectional studies and provides a more nuanced lens for better understanding the effects of exposure to family violence on adolescent internalization and externalization of disturbances. Another strength is that this study supported the robustness of the ITV and EST models that could promote future studies to further examine the utility of these models using complex methods and diverse samples. Lastly, a notable strength is that our findings underscored the co-occurrence of bullying perpetration and depressive symptoms and the conditional effects of exposure to family violence on subsequent maladaptive adolescent externalizing and internalizing symptoms.
Despite these strengths, there were also several limitations. First, this study utilized data from self-reported measures, which could serve as a limitation because adolescents may omit relevant details that could be mitigated by gathering information from multiple sources, including parents, teachers, and peers. Therefore, future studies should include other sources of information, which could reduce threats to validity. Second, this study only measured two outcomes (i.e., depressive symptoms and bullying perpetration) of exposure to family violence. Because there are several consequences of exposure to family violence that were not included in this study, future research should include relevant internalizing and externalizing consequences of exposure to family violence, using standardized measures such as The Multidimensional Anxiety Scale for Children (March et al., 1997) Proactive and Reactive Aggression Questionnaire (Raine et al., 2006) and the Problem Behavior Frequency Scale (Farrell et al., 2016) amongst others.
Third, prior literature has shown that the typology of bullying perpetration often includes cyberbullying, which was not included in the current study (McField et al., 2023). Thus, future studies should incorporate additional forms of bullying perpetration when assessing its onset and growth. Fourth, prior literature has shown that the occurrence of family violence often co-occurs with parental psychopathology and influences adolescents’ internalizing and externalizing behavior (Ehrensaft & Cohen, 2012). However, the current study only estimated the effects of exposure to family violence, but not parental psychopathology, on the onset of internalizing and externalizing symptoms. Future studies could address this limitation by robustly estimating how family violence and various parental psychopathologies (e.g., anxiety, depression, antisocial behavior) impact adolescent maladaptive functioning. Lastly, prior literature has suggested that bullying victimization often associates with adolescent internalizing and externalizing symptoms (Lawrence, 2023a, 2023b), which was not included in the current study. Therefore, future studies can address this limitation by measuring whether prior bullying experiences could lead to bullying perpetration and depressive symptoms over time.
Practice Implications
This study provided preventive and therapeutic implications. The occurrence of family violence is often interwoven with parental psychopathology, environmental strain, substance use, and overall dysfunctional family patterns (Briggs-Gowan et al., 2010; Ehrensaft & Cohen, 2012). To disrupt this pattern, legislative efforts and financial support should be allocated to providing community mental health services aimed at preventing family violence in socioeconomically disadvantaged communities that are cost-efficient and gender-specific (Chan et al., 2009). Communities that have utilized evidence-based models, such as the Duluth and Domestic Abuse Intervention Project (DDAIP) have reported reduced family violence and the occurrence of domestic violence among families (Feinberg et al., 2016).
Practically, because the onset of family violence could lead to a strained parent-child relationship, which could subsequently associate with child-parent aggression, including verbal (e.g., yelling at parents) and physical aggression (e.g., slapping, kicking, punching), family clinicians could disrupt these patterns by using evidence-based family interventions including Solution Focused Family Therapy. Such therapeutic interventions consist of incorporating core values into desired outcomes to form realistic solutions to problems (Beyebach, 2009). Prior evidence has shown that families who participated in Solution Focused Family Therapy reported fewer child-parent aggression, and families felt empowered to resolve conflict using healthy communication strategies (Powell & Ladd, 2010).
Situations in which individual therapy is an appropriate approach compared to family therapy may encourage clinicians to use evidence-based interventions such as Cognitive Behavioral Therapy (CBT), to identify distorted thinking patterns that often lead to emotional dysregulation, which could lead to adolescent antisocial behavior (Persampiere et al., 2014). Additionally, CBT interventions provide guidance and psychoeducation on the overlap between thoughts and behaviors to help develop healthy coping strategies, such as reappraisal of emotions, problem-solving techniques, and seeking support from others (Simpson et al., 2012). The utility of CBT in schools is also evident. For instance, clinicians report reductions in bullying preparation and overall hostility among students who participated in CBT brief interventions, which utilize challenging distorted thinking patterns that lead to aggressive behavior (Powell et al., 2011). Lastly, because exposure to family violence is strongly correlated with the development of traumatic symptoms and dysfunctional sibling relationships (i.e., sibling aggression; Lawrence, Hong, Espelage, & Voisin, 2023; Saleem et al., 2020; Vickerman & Margolin, 2007), clinicians can use Cognitive Processing Therapy (CPT) to address trauma symptoms by specifically encouraging clients to write about their worst traumatic event while utilizing affective coping strategies to attenuate intense emotions (Iverson et al., 2011; Vogel & Rosner, 2020). Studies have shown the efficacy of using CPT among adolescents who endorse traumatic symptoms (Ahrens & Rexford, 2002; LoSavio et al., 2021).
Conclusion
Overall, the current findings contribute to the current literature by demonstrating that bullying perpetration and depressive symptoms increased in early adolescence after adolescents transitioned to middle school and peaked in Grade 7. Bullying perpetration subsequently declined, and depressive symptoms stabilized thereafter. Findings indicated that bullying perpetration and depressive symptoms are likely to co-occur during this developmental period, and that this co-occurrence is associated with higher levels of exposure to family violence. Exposure to family violence appeared to be a common risk factor which was significantly associated with both bullying perpetration and depressive symptoms, and youth who experienced higher family violence exposure in Grade 6 were more likely to exhibit persistently elevated rates of bullying perpetration and depressive symptoms across the middle school years (i.e., Grades 6 to 8). These findings highlight the importance of preventive interventions in thwarting family violence while providing evidence-based interventions that are effective in addressing the onset and co-occurrence of bullying perpetration and depressive symptoms.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Approval
The data are publicly available. The study utilized publicly available data with no identifiers and was exempted from the Institutional Review Board oversights.