
Abstract
This study aimed to assess differences in emotion and elaboration quality between clinical and community child cohorts in both past reminiscing and future worry conversations. We analyzed 54 Australian parents (46 mothers, 8 fathers) and their 8- to 12-year-old children (M = 9.63, SD = 1.29; 28 boys, 26 girls) in reminiscing interactions. Dyads were recruited from local schools (community cohort, n = 26) or a children’s psychology clinic waitlist (clinical cohort, n = 28). Clinical cohort children engaged in less emotion exploration in both past and future conversations, as did parents for future conversations. Elaboration quality did not differ. Parent-son dyads differed in the clinical cohort, exhibiting significantly lower emotion resolution than the community cohort, or parent-daughter dyads when discussing past events. These findings suggest that discussing anticipated negative events may be a relevant point of family-based intervention for anxious children. Additionally, this study highlights the importance of parent-son emotional discussion.
Introduction
Parent-child emotion conversation is central to children’s socio-emotional and cognitive development. Parents and children engaging in emotion focused conversations about the past, known as reminiscing, provides opportunity for emotion processing and understanding outside of the emotional ‘heat of the moment’ (Salmon & Reese, 2016). Decades of reminiscing research demonstrates how reminiscing supports positive socio-emotional development for children within community samples (see Fivush et al., 2006 for review). However, there is a gap in the research for those most at risk of socio-emotional and cognitive difficulties. Diagnostic frameworks have limitations when applied to children and there is substantial overlap, both concurrently and longitudinally, in symptom presentation (Finsaas et al., 2020). As a result, childhood difficulties are often conceptualized as internalizing (emotion-based symptoms including anxiety and depression, directed inwards) or externalizing (behavioral symptoms expressed outwards) (Eisenberg et al., 1998). Pre-adolescent children are particularly prone to comorbid anxiety and depression symptoms (Melton et al., 2016). Internalizing difficulties affect 8.7% of Australian children aged 4–17 years old; almost 7% of Australian children have a diagnosed anxiety disorder, and more than half of the 2.8% with diagnosed major depressive disorder also have comorbid anxiety disorders (Lawrence et al., 2015). Outside of diagnosis, one in seven (14.8%) of all Australian children accessed a health service for emotional or behavioral problems in the past 12 months (Lawrence et al., 2015). While the current study recruited a clinical sample of children with a primary referral for anxiety symptoms, many of these children also experienced depression and other internalizing symptoms. There is limited research examining reminiscing among child clinical samples or examining clinical symptoms, with some studies focusing on anxiety and others on internalizing symptoms. While the term anxiety will be predominantly used throughout, we acknowledge that any differences may also reflect children with either concurrent or future depression comorbidity and a vulnerability towards internalizing difficulties more generally.
The goal of this paper was to identify areas for intervention to empower parents to support their children with internalizing difficulties in everyday dyadic interactions. Typically, children accessing mental health services for internalizing difficulties receive Cognitive Behavior Therapy (CBT), which has long been the gold standard intervention (Wergeland et al., 2021). However, parental involvement in CBT is typically skills coaching (Breinholst et al., 2012), which has mixed findings regarding efficacy (Carnes et al., 2019; Kreuze et al., 2018; Manassis et al., 2014). Similarly, parenting programs with preadolescents typically focus on behavioral approaches to externalizing behaviors rather than relational focused approaches (Burke et al., 2010). Parent training emotion coaching interventions have also been successful, but are targeted at moments of high emotion, rather than reflective reminiscing (Kehoe et al., 2014). Although a small number of studies suggest that reminiscing is a modifiable dyadic interaction, including for ‘at risk’ children (see Corsano et al., 2019 for a review), further understanding of areas for intervention for this population is needed (Behrens et al., 2022; Van Bergen et al., 2009). Reminiscing may be a modifiable dyadic that could support parent emotion socialisation for children at risk of internalising difficulties.
Parent-Child Emotion Reminiscing
Past events are discussed with children frequently in daily life from as early as 18 months of age (Miller, 1994). In reminiscing, experiences are co-constructed after the event where the child theoretically has more capacity to reflect (Kucirkova & Tompkins, 2014; Salmon & Reese, 2016). This may be an especially important emotion socialization context for children with anxiety or internalizing difficulties, as more intense emotional reactions experienced in the moment may hinder processing or integration of the experience (Siegel, 2020). For typically developing children, parents use of an emotion-rich elaborative style – characterized by open-ended questions, encouragement, and novel information - is associated with a range of positive socio-emotional factors (Fivush et al., 2006). This style of reminiscing about negative emotional events appears to be more consistently associated with child outcomes compared with elaborative and open discussions about positive emotions (Bird & Reese, 2006; Laible, 2011; Leyva & Nolivos, 2015; Lunkenheimer et al., 2007; Reese et al., 2019).
Understanding Coding Approaches
There are a variety of methods to assess differences in emotion reminiscing conversations. Typically, these consider either elaboration and/or the quality of emotion discussion. Traditionally elaboration has been coded at the proposition, frequency level and more recently, scale-based coding has been developed to capture the overall quality of elaboration across the conversation as a whole. Leyva et al. (2020) found that the scale-based coding of elaboration was uniquely related to children’s emotion regulation, whereas frequency-based coding of elaboration was related to child memory recall (Leyva et al., 2020). Different coding approaches have also been used to capture the quality of emotion discussion in reminiscing. Emotion coaching, and reminiscing literature highlight the importance of parent’s attuned emotion discussion, validation and explanation of the causes and consequences of the child’s emotions as important (Bird & Reese, 2006; Eisenberg et al., 1998). Emotion explanations appear to be more salient than emotion attributions alone (i.e., emotion word counts), or other emotion references (Bird & Reese, 2006; Van Bergen & Salmon, 2010). Differences in emotion explanation may be particularly important in middle childhood, as advanced emotional skills develop and children are able to examine the why behind a situation on a deeper level (Pons et al., 2004). Moreover, learning to hold and resolve negative feelings is an adaptive emotional skill related to children’s mental health (Compas et al., 2017). Reminiscing conversations have also been coded for emotion resolution type (Bird & Reese, 2006) and quality (Koren-Karie et al., 2003; Russell et al., 2023). As reminiscing occurs out of the emotional context, there is enhanced potential for nuanced emotion learning to occur, where the child is regulated enough to hold the content in mind (Siegel, 2020). Parents scaffold and model resolving difficult emotions, which may generalize to regulating difficult emotions in other contexts as the child matures.
Reminiscing in the Community
The majority of reminiscing research has focused on the preschool and early childhood years, with some studies extending into middle childhood and examining associations of reminiscing quality with child functioning. In a community sample, Sales and Fivush (2005) found mothers who verbally expressed more emotion and provided more emotion explanations had children (aged 8–12 years old) with fewer internalizing and externalizing difficulties. Again, using a predominantly community sample, Brumariu and Kerns (2015) observed mother-child reminiscing in a conflict discussion with children aged 10–12 years old. Using a scale-based coding approach, more anxious children had mothers who were significantly less elaborative and less warm, after accounting for child gender. Moreover, more anxious children showed less engagement and more intense affect. Dyadic references to emotion words were also coded and were not significantly associated with child anxiety symptoms (Brumariu & Kerns, 2015). It appears that for community samples in middle childhood, child anxiety and internalizing symptoms are associated with less elaborative and less emotional-rich parent reminiscing.
Clinical Comparisons
In studies with clinically recruited families, similar results have been observed. Van der Giessen and Bögels (2018) compared parent-child conflict discussions for children with and without anxiety disorders and found no differences in emotional expressivity. However, dyads with children with anxiety disorders showed lower emotional flexibility: the ability to move freely between emotions. Suveg and colleagues compared the emotional content of reminiscing conversations between 8- to 12-year-old children and a parent, for children with and without anxiety disorders (Suveg et al., 2005). Mothers of children with anxiety disorders tended to discourage negative emotional expression and used fewer positive words in comparison to non-clinical mothers. No differences were observed in emotion explanations for the mothers or children. However, another study examining children (again 8–12 years old) with anxiety diagnoses found parents of clinical children were less likely to explain emotions than parents of non-clinical children (Suveg et al., 2008). Contrary to their predictions, neither study found evidence that clinical children were less likely to explain their emotional experiences. One reason may be that neither study controlled for children’s language ability, which is typically correlated with reminiscing quality (Bird & Reese, 2006; McDonnell et al., 2016; Reese et al., 2007; Reese & Newcombe, 2007; Valentino et al., 2013), and has been suggested as an important mechanism underlying child psychopathology (Salmon et al., 2016). Research has consistently observed parents of children with anxiety difficulties to be less open and explanatory in relation to emotions. However, further research is needed to understand child differences, particularly within clinical samples.
Middle Childhood and Mental Time Travel
Parent emotion socialization has been shown empirically to continue into middle childhood, defined typically as ages 8 through 12 years old (Zeman et al., 2010). By middle childhood, children are developing nuanced reflective skills, exploring the social landscape, and experiencing the social and emotional consequences of conflict and resolution (Nelson, 2003; Siegel, 2020; Zeman et al., 2010). Moreover, it is a period of rapid brain development, as the neurological foundations of emotion regulation patterns are built (Zeman et al., 2010). At around age 8, children develop deeper thinking skills, abstract thought, and social awareness (Pons et al., 2004). These social, cognitive, affective, and neural changes are also mirrored in changes in psychopathology, with increased expression of internalizing and externalizing difficulties (Leve et al., 2005). Middle childhood may therefore be a critical period for prevention of psychopathology, and development of adaptive coping skills through parent scaffolded emotion discussion. Middle childhood may also be an important age to study future cognition and discussion, which requires complex ‘mental time travel’ (Atance & Meltzoff, 2005). Difficulties with imagined future thinking has been linked with mental health difficulties (Hallford et al., 2018). In fact, some have gone so far as to suggest that difficulties in mental health “may all actually boil down to negative future thinking” (Roepke & Seligman, 2016, p. 24). Predicting and anticipating future events is an important developmental leap (Fivush & Nelson, 2006). Parent-child future talk has been linked to episodic memory and planning ability (Hayne et al., 2011); however, conversations about the future have received relatively little attention in the emotion socialization literature. Two studies have examined educators and mother reminiscing and future talk among preschoolers (Andrews et al., 2019, 2020). Hollenstein et al. (2015) examined verbal and non-verbal emotions for 14- to 18-year-olds (with and without depression) and their parents. Families planned a future vacation alongside several other conversation tasks. There was some evidence that parents did not match the expressed negative emotions of their adolescents with depression during the planning task, although this was considered together with a past event discussion. Further research is needed to understand the specific role of parent-child future conversations for children with internalizing difficulties and in particular, anxiety.
As anxiety is defined as a perceived anticipated threat, emotion conversations about anticipated events may be especially important for children with anxiety presentations (Percy et al., 2016). The way in which parents prepare, or fail to prepare, children and the specific aspects of these anticipated events that are emphasized, may have implications for children’s internalized coping strategies and their overall appraisal of threats. Moreover, future focused conversations provide insight into how children and parents use coping skills ahead of time. Research has demonstrated that talking about an event beforehand alters children’s memory outcomes (Salmon et al., 2016). Life story research from Ramsgaard et al. (2019) identified that anxious youth appraised past events less positively, and expected fewer positive outcomes in the future, despite describing equivocal events as typically developing youth from the community. If past conversations are a potential avenue for gaining emotional awareness, and making meaning, future focused conversations may be an avenue where these skills are both applied, and an uncertain future might learn to be tolerated. It is therefore important to understand how children with anxiety and their parents engage in future event conversations.
The Current Study
This study examines parent-child worry conversations about past events and future anticipated events. Parent-child dyads were recruited from either local community schools (community cohort), or a child mental health clinic prior to treatment for the child’s anxiety symptoms (clinical cohort). Due to high levels of comorbidity, depression and internalizing symptoms were also measured. This study aims to examine potential differences in conversations about both past and future worry events for children (aged 8–12 years) who experience anxiety and their parents. It is hypothesized that in comparison to the community cohort: (1) children clinically referred for anxiety and their parents would demonstrate less emotion exploration (Siegel, 2020; Suveg et al., 2008); (2) parents of children clinically referred for anxiety would have lower quality elaboration (Leyva et al., 2020; Waters et al., 2019); and (3) clinical dyads would demonstrate poorer quality emotion resolution during emotion reminiscing, in line with emotion regulation research (Siegel, 2020).
Finally, child gender may also be important to consider. Gender differences in anxiety and internalizing symptoms begin to emerge during middle childhood, with increased rates consistently observed for girls (Zahn-Waxler et al., 2008). There is some evidence of main gender effects on emotion reminiscing, with a greater emphasis on discussion of anxiety and sadness with daughters compared with sons (Bird & Reese, 2006; Fivush et al., 2000). However, other research shows no main effect (Brumariu & Kerns, 2015) and a recent meta-analysis concluded no overall gender differences in maternal elaboration (Waters et al., 2019). It will be important to understand whether gender effects for reminiscing and future conversations within both clinical and community samples. Due to the mixed findings regarding child gender and reminiscing no specific predictions were made.
Methods
Participants
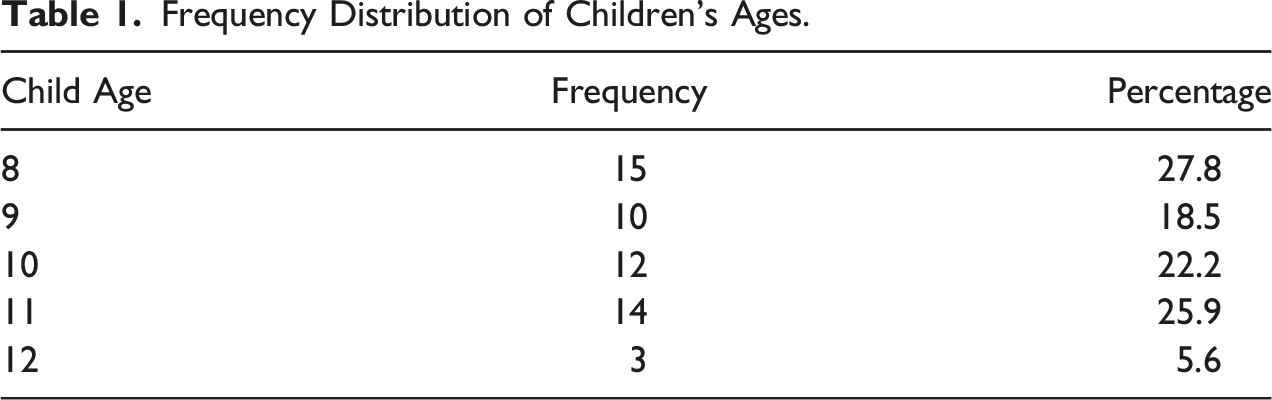
Frequency Distribution of Children’s Ages.
Procedure
The University Human Research Ethics Committee (2018/492), and the State Department of Education (19/184120) granted ethics approval for this research. Each dyad attended the University developmental lab for approximately 90 minutes as a part of a broader study which examined different parent-child interactions with parent mental health (Russell et al., 2023) and conflict discussion (Bird et al., 2021). Informed consent and assent were obtained from the dyad prior to data collection. The research session was scheduled after initial intake assessment but prior to commencement of therapy to not interfere with the child’s therapeutic care. Parents and children completed individual questionnaires on iPads (approximately ten minutes), which were presented in the same order for all participants. The dyad then completed a series of tasks including the reminiscing and future conversation tasks and the children’s language ability task.
For the conversation tasks, parents chose two negative events where the child felt worried or scared: one from the recent past (e.g., getting lost at the mall) and another anticipated in the future (e.g., an upcoming dentist appointment). The researcher consulted with the parent to ensure topics were contained to everyday difficult events rather than highly traumatic incidents such as abuse or death. Two positive emotion events, where the child felt happy or excited, were also selected and set to follow the worry conversations to provide containment for the child before leaving the research session. During the conversation tasks, dyads sat comfortably on a couch together, and were instructed to discuss the selected topics “as you usually would, for as long as you usually would”, and were then given privacy to complete the task. Conversations were audio-recorded for later transcription and coding. Dyads were debriefed following the tasks to ensure co-regulation prior to leaving and were offered a $20 gift voucher and children a small stationary gift in appreciation.
Measures
Demographic Questionnaire
Demographic variables collected included the parent’s gender, ethnicity, age, family structure and level of education. Collected children demographics included their gender, age and number of siblings, school grade, and ethnic background.
Peabody Picture Vocabulary Test – Fourth Edition (PPVT-4)
To measure children’s receptive language ability, the PPVT-4 was utilized (Dunn & Dunn, 2007). The PPVT-4 is validated for ages 2 ½ years through 90 years (Dunn & Dunn, 2007). Test items are presented as four images, and the individual is asked to select the image that matches the spoken word by pointing. Standardized scores are calculated from total scores based on age-based norms. Dunn and Dunn (2007) report a test–retest reliability of r = .92.
Revised-Child Depression and Anxiety Scale (RCADS)
The RCADS is a 47-item self-report measure of youth anxiety and depression symptoms aged eight to 18-years-old, with youth and parent report versions (Chorpita et al., 2000). A four-point Likert scale from 0 (never) to 3 (always) indicates how often the child experiences the symptom listed (e.g., “I feel sad or empty”). The RCADS has good test-retest reliability (Chorpita et al., 2000) and good concurrent validity with other validated measures (Chorpita et al., 2005). The RCADS produces six subscales measuring anxiety and major depression symptoms (MDD), as well as overall scores and an internalizing symptom score. Cronbach’s alpha for the current sample for child report was anxiety at .93, MDD at .76 and total internalizing at .94. The parent report had a Cronbach’s alpha of .92 for internalizing total, .88 for MDD symptoms and .96 for anxiety symptoms.
Child Anxiety Life Interference Scale (CALIS)
The CALIS is a measure of the interferences of anxiety symptoms on a child’s day-to-day life (Lyneham et al., 2013). The child version (CALIS-C) and a parent version (CALIS-P) of the measure were utilized, which both use a 5-point Likert scale from not at all to all the time. The measure is scored into categories of interference with at home, outside of home, and parent impact (parent report only). Lyneham et al. (2013) found test-retest reliability to be moderate (r = .66 to .87) and an acceptable level for intraclass correlations (r = .38 to .74). Cronbach’s alpha for this sample surpassed the acceptable level .95.
Strengths and Difficulties Questionnaire (SDQ)
The SDQ was completed by parents to measure the emotional and behavioral difficulties of the child (Goodman, 2001). There are five subscales including prosocial behaviors, emotional, conduct, hyperactivity, and peer relationship problems. Subscale scores can be summed to provide broader internalizing (emotional problems and peer relationship problems) and externalizing (conduct problems and hyperactivity) scores (A. Goodman et al., 2010). Test-retest reliability and internal consistency reliability has been demonstrated in past research (Goodman, 2001). The internalizing difficulties score was used in the current analyses. Cronbach’s alpha for internalizing symptoms in the current sample was .85.
Conversation Coding
The parent-child worry conversations were transcribed verbatim and any identifying information was removed prior to coding. One coder made two passes over the transcripts, firstly for emotion exploration content coding, and secondly for emotion resolution quality coding. Off-topic talk (e.g., asking for the time, etc.) was not coded. A second researcher coded elaboration on the quality scale. A third researcher conducted reliability for both the emotion and elaboration codes. Reliability was conducted on 25% of the transcripts. Conversation duration was calculated by totaling all propositions, excluding off-topic talk, to quantify amount discussed, not confounded by speed of speech.
Parent and Child Emotion Exploration
Based on past reminiscing research, frequency codes of emotion aspects were tallied and then summed to create a composite code. The causes of emotion are explanations or explanation of an emotional state, for example “you were worried because…” (Bird & Reese, 2006; Suveg et al., 2005). Consequences of emotions are statements that describe or explore the occurrences after an emotional state or as a consequence of the emotion for example “you covered your face when you were scared” (Bird & Reese, 2006; Suveg et al., 2005). General emotion talk describes references to emotion that do not attribute or explain the emotion, rather they may describe the meaning of emotions or more broad applications, for example “where do you feed scared in your body?” For parents only, validation of the child’s emotion was also included. Validation was coded as statements that clearly verbally confirm a child’s emotion statement, for example, “Yes, it was really scary” (Suveg et al., 2005). The third researcher coded 25% of the transcripts for reliability. Cohen’s Kappa was calculated for each component and averaged. Mean Cohen’s Kappa was .74, within the acceptable range of k > .70 (McHugh, 2012). Codes for emotion exploration, validation and general emotion talk were then summed to create the total emotion exploration construct. Not included in this construct were emotion attributions (e.g., “You were scared”) and factual talk (e.g., “It was close to Christmas”, “Who else was there?”).
Dyad Emotion Resolution
The emotion resolution coding was adapted from Koren-Karie et al. (2003) Autobiographical Emotional Events Dialogues (AEED) coding scale for emotion closure. This scale was adapted to include efforts for meaning making or emphasis on the child’s strengths or a lesson learned. Emotion resolution was rated for parent and child separately however were highly correlated (Past, r = .558, p < .01; Future, r = .687, p < .01) and as such were totaled for a dyad resolution score, per conversation type. Scores ranged from 1 to 9, with higher scores indicating higher quality attempts of resolution of emotion and meaning made, and lower scores indicated poor attempts, including emphasis on negative aspects (Bird & Reese, 2006; Koren-Karie et al., 2003). Reliability on 25% of the sample was tested through a two-way random, single measure intraclass correlation coefficient (ICC) with absolute agreement (Syed & Nelson, 2015). The emotion resolution ICC was .79.
Parent Elaboration
Parent’s elaborative quality was measured using a 1 to 5 quality-based scale (Fivush & Fromhoff, 1988; Laible, 2004; Leyva et al., 2020). Higher scores indicate mostly elaborative and open-ended questions with minimal repetition and depth of information. Lower scores indicate primarily factual and closed questions, a repetitive style, where they may negate the child’s emotions (Brumariu & Kerns, 2015; Fivush & Fromhoff, 1988; Laible, 2004; Leyva et al., 2020). The elaboration reliability ICC was .82 (Syed & Nelson, 2015).
Analyses Plan
Correlations Between Continuous Demographics, Mental Health, and Conversations.
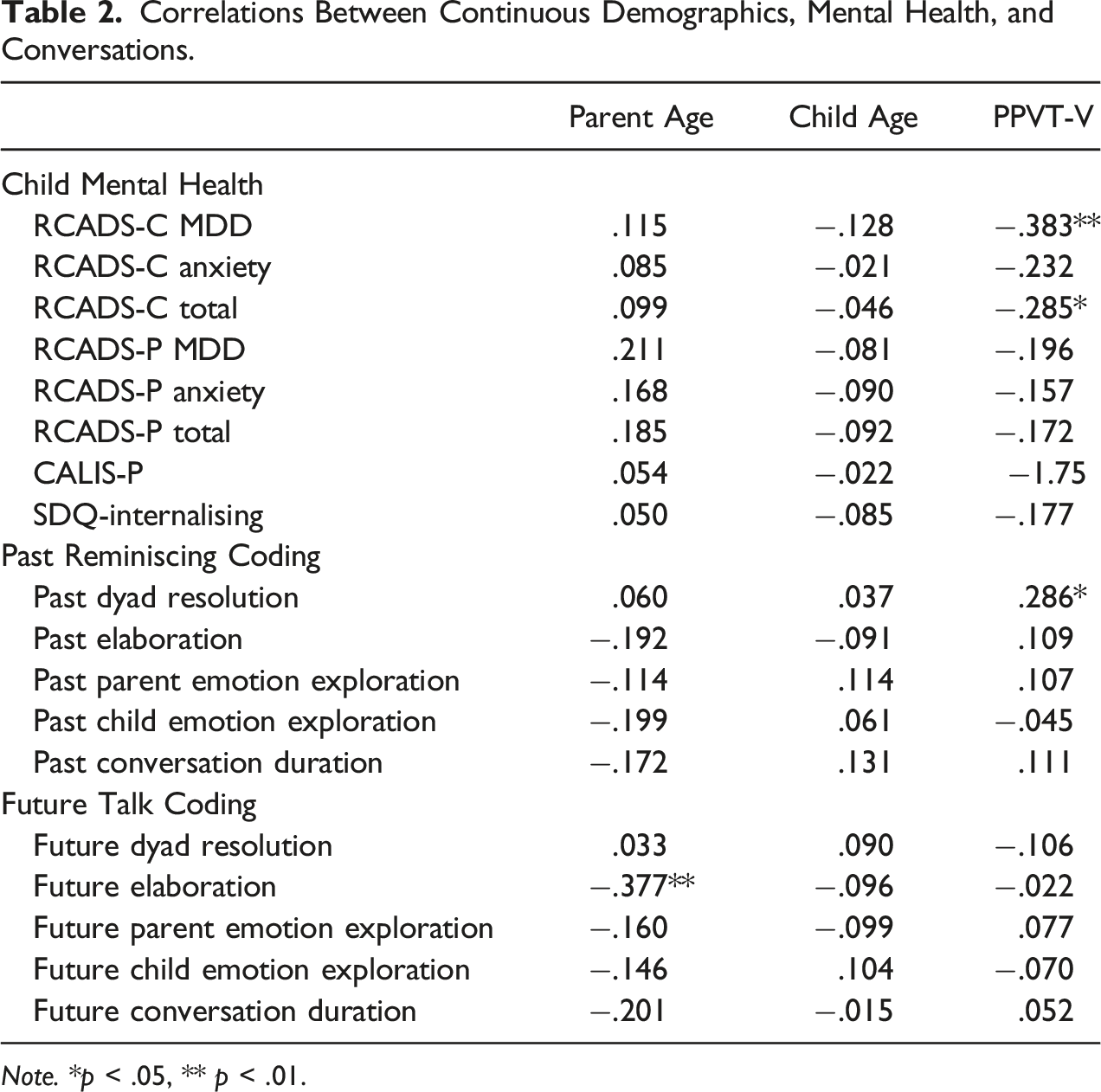
Note. *p < .05, ** p < .01.
Demographic and Mental Health Data by Cohort Statistics and Comparisons.
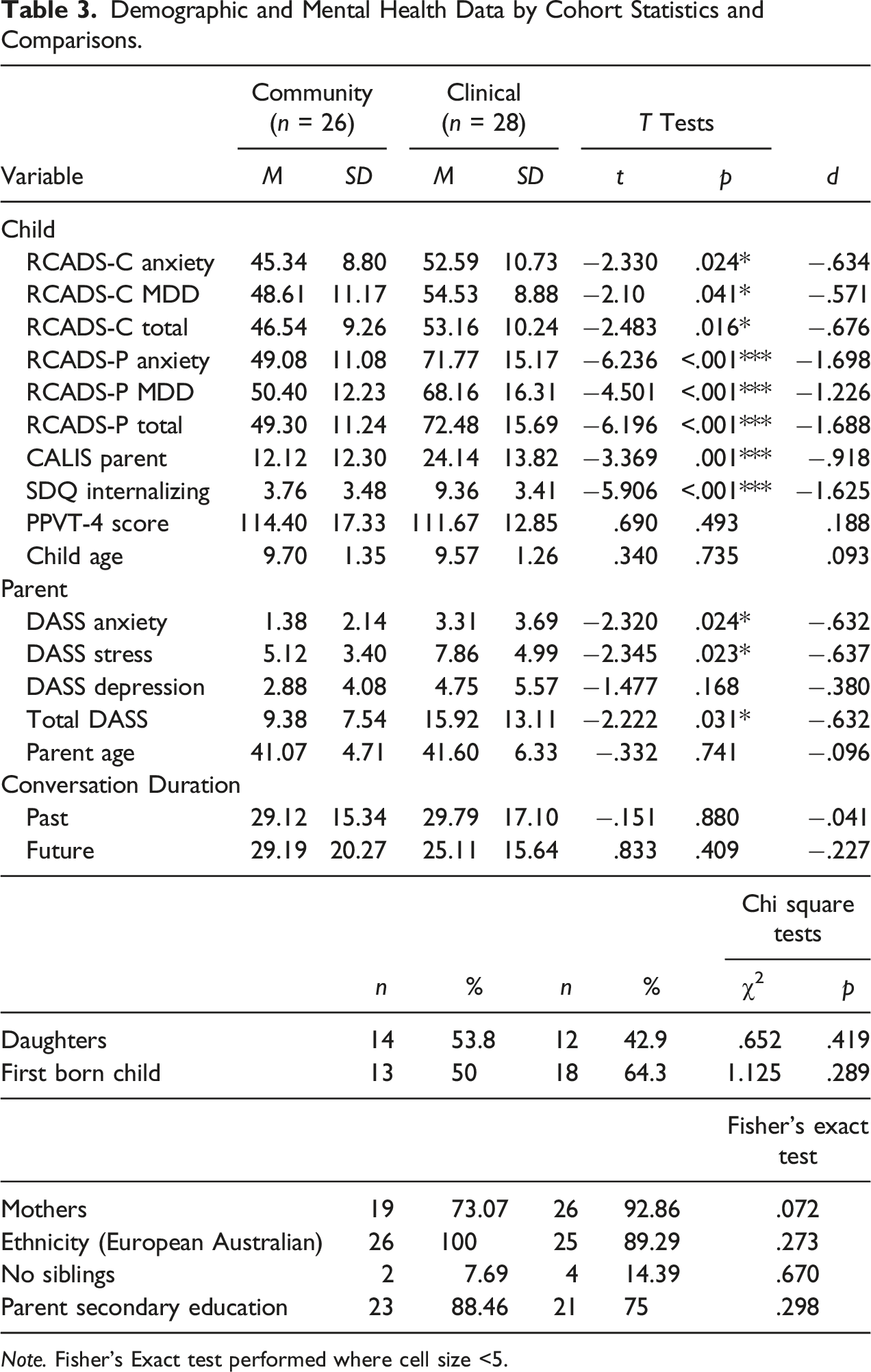
Note. Fisher’s Exact test performed where cell size <5.
Results
Preliminary Analyses
Table 2 presents Pearson’s r correlations. Table 3 presents means and standard deviations, and independent samples t-tests between cohorts to assess for potential covariates. Categorical variables were tested between cohorts using Chi-Square for those with adequate cell sizes, and Fisher’s Exact Test for categorical variables with cell sizes smaller than 5. Significant demographic variables were then included as covariates in the main analyses. Parent age was included for analyses of future elaboration. The PPVT-4 was significantly related to RCADS-C MDD and total internalizing as well as dyad emotion resolution (Table 3). Based on past research that suggests children’s language ability is highly associated with both reminiscing and child mental health outcomes, we elected to include this as a covariate in the main analyses (Salmon & Reese, 2016). All child mental health variables were significantly different between cohorts (Table 3). All fell within the acceptable range of fell within the acceptable range of +/− 2 for Skewness and Kurtosis (George & Mallery, 2010).
Main Analysis
A series of four 2 (cohort) × 2 (child gender) ANCOVA were conducted for both past and future conversation types with the reminiscing dependent variables; dyad emotion resolution; parent emotion exploration; parent elaboration and child emotion exploration. Children’s language ability as measured by the PPVT-4 was included as a covariate in all analyses.
Past and Future Conversation Differences Across the Community and Clinical Samples.
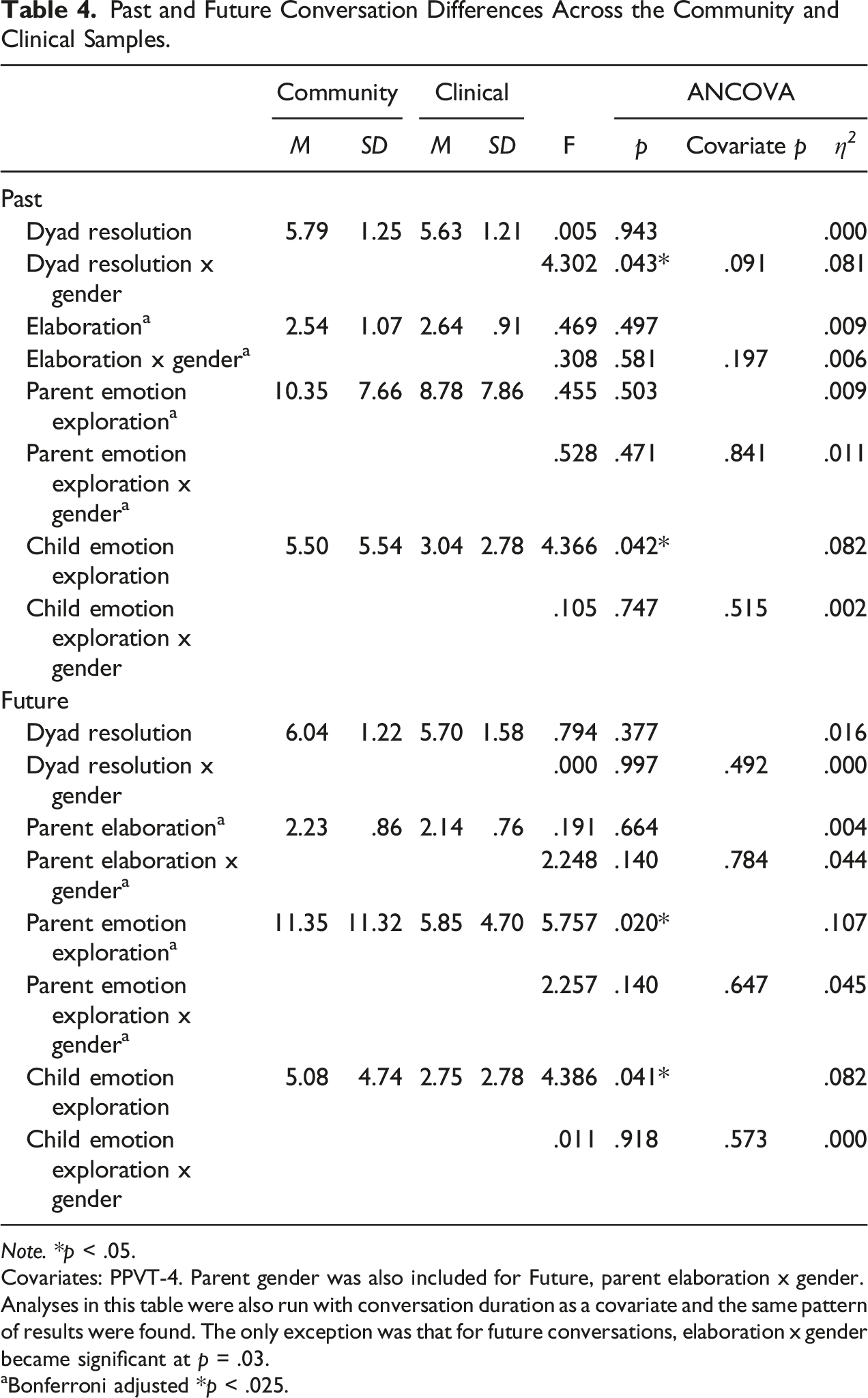
Note. *p < .05.
Covariates: PPVT-4. Parent gender was also included for Future, parent elaboration x gender.
Analyses in this table were also run with conversation duration as a covariate and the same pattern of results were found. The only exception was that for future conversations, elaboration x gender became significant at p = .03.
aBonferroni adjusted *p < .025.
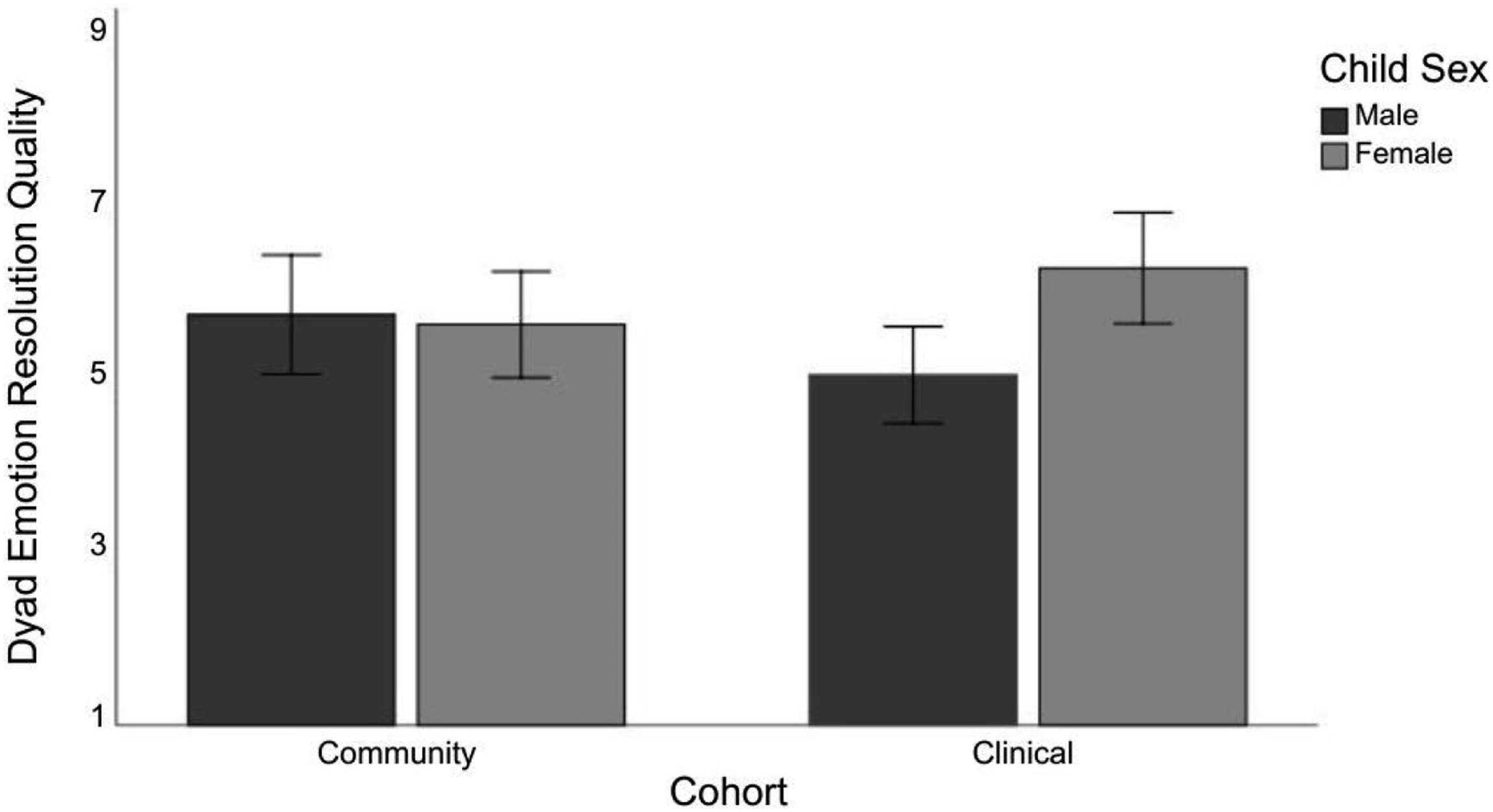
ANCOVA dyad resolution quality interaction effect cohort by child gender for past reminiscing.
Discussion
The current study aimed to expand understanding of parent-child past and anticipated future worry conversations among children clinically referred for anxiety difficulties, compared with a community sample. This study focused on middle childhood, and considered the emotion content, emotion resolution and elaborative aspects of conversations. Children referred for anxiety engaged in less emotion exploration compared with community peers in past conversations, and both parents and children in the clinical sample engaged in less emotion exploration during future conversations. There was also a significant cohort by child gender interaction, with poorer quality emotion resolution for clinical boys but not girls, and no gender difference for the community sample. These findings suggest reminiscing differs meaningfully in families of children with internalizing difficulties and could provide an avenue for clinical intervention.
A novel aspect of this study is the observation of future worry conversations, which show significantly lower emotion exploration for both parents and children in the clinical cohort. Due to the cross-sectional design, the direction of this relationship is unknown. Past research demonstrates the unhelpful nature of avoidance in perpetuating emotional difficulties (Fialko et al., 2012; Hayes et al., 1999). A bi-directional relationship may occur, which cyclically reinforces the avoidance of emotion discussion and narrows the child’s (and parent’s) window of tolerance to difficult emotions. As these conversations occur outside the intensity of the emotional event, it may be that as less attention is placed on exploring difficult emotions, children have fewer opportunities to learn to tolerate the negative affect, and thus fewer opportunities for learning how to cope with the anticipated event. Over time, this avoidance may contribute to not only increased anticipatory fear about future events, but also provide children less opportunity to prepare and cope with realistic negative experiences; further reinforcing - to both the child and parent - the child’s limited capacity to cope. In addition, although these conversations occur outside of the event, children with anxiety are likely to be more emotionally activated within these conversations. Although not measured here, there may be multiple contributing mechanisms for both the parent and child in this potential avoidance cycle. For example, parents may engage in less emotion rich conversation about anxiety-provoking events for their concern of distressing the child, their own difficulties in regulating emotions, or other transdiagnostic mental health factors.
Greater emotion exploration was observed in the community cohort. In turn, this system of communicating with rich emotion exploration may reinforce the child and parent’s own capacity to hold difficult feelings. Moreover, this may provide greater opportunities for children to mentally prepare for future events, to be soothed if distressed, and in discussing the event learn that they can manage, even if it is scary. Supporting research comes from Ramsgaard et al.’s (2019) study of adolescent’s life stories, which found adolescents with anxiety tended to have less clear and coherent imagined futures, even those with more positive outcomes. This suggests that young people with anxiety may not be adequately preparing for inevitable difficult events, through the avoidance of difficult feelings (Ramsgaard et al., 2019). Our findings provide the first evidence that parent-child conversations about anticipated future negative events may be an emotion socialization context with relevance for the developing mental health of children.
Future focused conversations may be a way children apply skills and problem solve whilst tolerating difficult emotions, whereas past conversations may offer a way that children learn lessons and make meaning about events. Children in the clinical cohort used significantly less emotion exploration in past event reminiscing as predicted, whereas parent emotion exploration did not differ significantly between groups. Again, the lower level of emotion exploration by children in the clinical cohort may reflect children utilizing a more avoidant strategy to reduce their experience of negative affect, which in turn may exacerbate internalizing symptoms (Fialko et al., 2012; Hayes et al., 1999; Wilson & Hughes, 2011). Overall, past research has found mixed results for parent and child explanatory language as related to anxiety symptoms (Sales & Fivush, 2005; Suveg et al., 2005, 2008). Although there are some inconsistencies amongst whether it is the parent, child or both who differ in explanatory and emotion exploration, the overall trend appears to show families with anxiety symptoms tend to have shorter, less emotionally laden conversations. This is supported by the conflict discussion findings of Van der Giessen and Bögels (2018), which observed less emotional flexibility in dyads where children had an anxiety disorder, in comparison to healthy controls. The excerpts below illuminate the difference in which two mother-son dyads from our study discuss a future worry event. Dyad A’s excerpt shows a parent and child from the community cohort with low anxiety symptoms, who are discussing the child’s upcoming speech. The parent opens and holds an emotional conversation with the child, curiously demonstrating the exploration of emotion around the event.
Dyad A – Future Worry Conversation
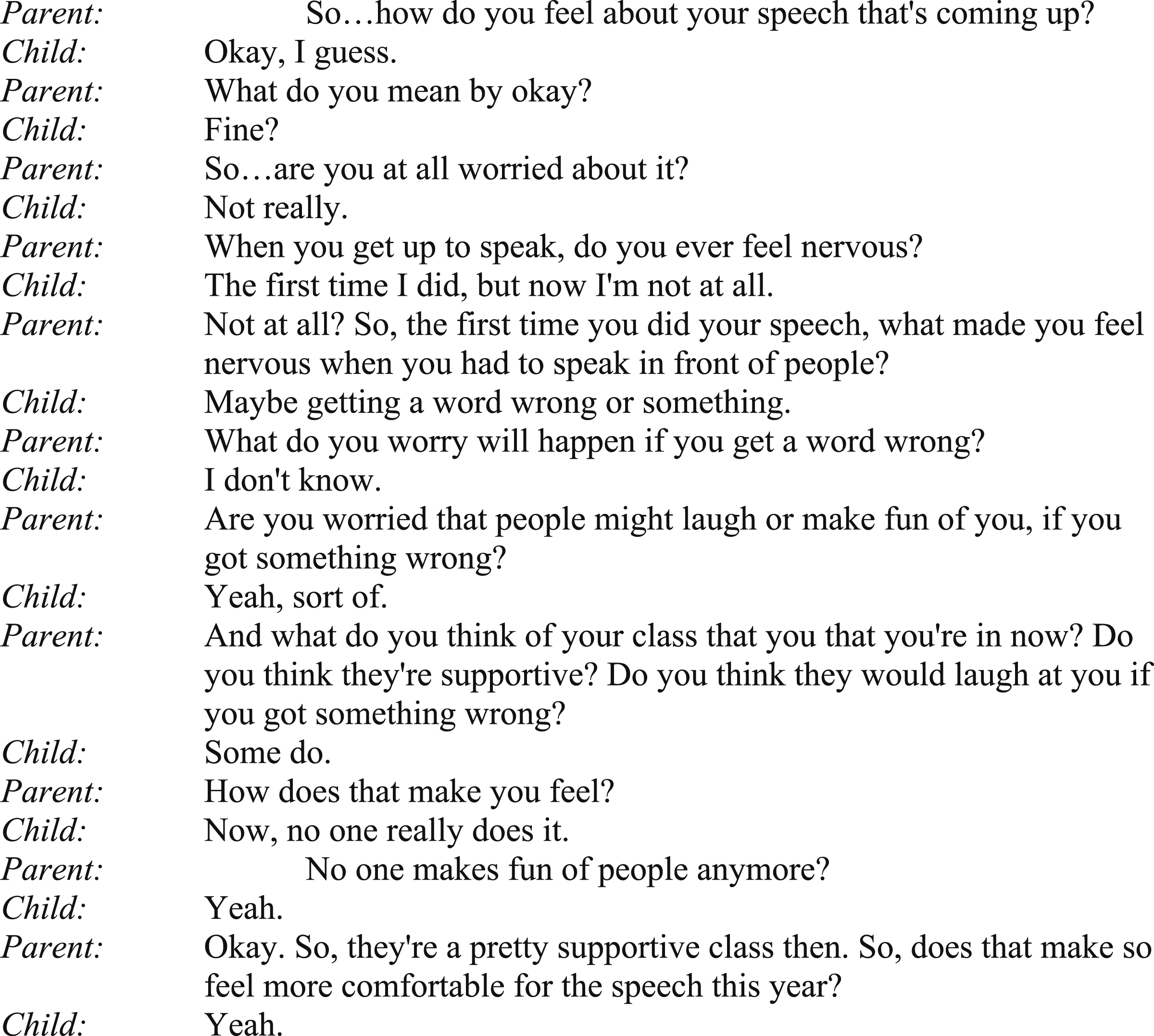
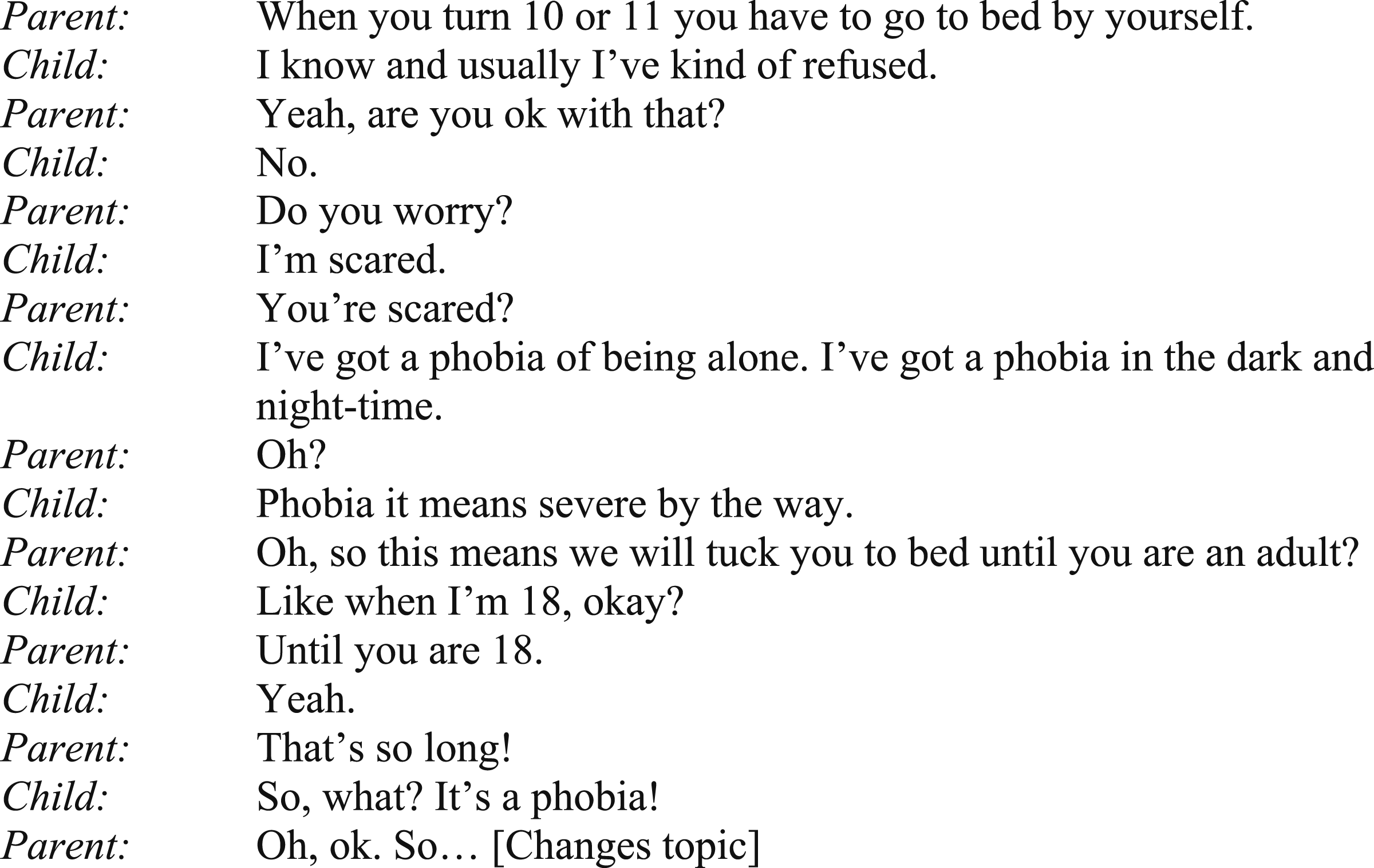
In Dyad B’s discussion, despite the child using exaggerated language about fear, the exploration and discussion of emotion is avoided and moved past quickly.
Dyad B - Future Worry Conversation
Contrary to our predictions, we found no differences in parent elaboration quality between cohorts, for either past or future focused conversations. We opted to use the scale-based coding of elaboration, rather than specific instance based, because past research suggests this has the strongest association with child socioemotional skills (Laible, 2004; Leyva et al., 2020). Although null findings such as this should be interpreted with caution, especially among a relatively small and specific sample, it may be that the way in which emotions are discussed and resolved are a more salient reflection of differences in clinical samples of children during middle childhood. Elaboration has been observed to differ in reminiscing where parents have mental health symptoms, although with mixed findings (Reese et al., 2019; Swetlitz et al., 2021). It may be that parent elaboration differences are more reflective of the parent’s mental health than the interaction with the child’s mental health.
We anticipated that clinical-community differences would be observed in emotion resolution. Specifically, we hypothesized that community cohort dyads would have higher quality resolution in both conversations in comparison to the clinical cohort dyads, however overall, no significant difference was observed. As the cohort is developmentally in middle childhood where conceptual skills are being developed (Siegel, 2020), these findings may be a result of our resolution coding reflecting both meaning making as well as attempts to close the emotion and end the conversation on a positive note. Meaning making describes how well the child and parent make sense of the event in the context of their autobiographical memory and identity, (e.g., “It taught me that I am brave”). Previous literature has found that meaning making about difficult life events that are still ongoing may not actually be helpful for young people. Sales et al. (2013) examined the personal narratives of 24 African American adolescent girls, where meaning making in the context of stressful lives was not found to be helpful when they continued to exist in the difficult context of their lives. They concluded that resolution attempts may have been ruminative rather than providing resolution. Of note, Sales et al.’s (2013) study assessed girls only, and there may be some parallels with our finding of a significant interaction for gender by sample.
Although no other main or interaction effects were observed for child gender amongst the analyses, there was a significant interaction between child gender and cohort for dyad emotion resolution in past conversations. Within the community cohort, there was no difference between child genders on emotion resolution, however within the clinical cohort parent-son dyads had significantly lower dyad emotion resolution than parent-daughter dyads. This cohort and gender effect highlights a potential pathway whereby emotion resolution quality may be related to the development or maintenance of anxiety for boys. As discussed above, Sales et al. (2013) found meaning making was potentially unhelpful and ruminative for female adolescents. These findings parallel the higher emotion resolution observed among girls from the clinical cohort in the current study, which could indicate a level of co-rumination. This observed difference in boys with anxiety is particularly important to understand given middle childhood signals a shift in gender differences for internalizing disorders, with boys tending to move towards externalizing difficulties (Leve et al., 2005). Past research has indicated that due to traditional gender roles and socialization, boys may lean towards avoidant strategies (e.g., “boys don’t cry”) (Vanderveren et al., 2020), which could influence the increase in externalizing disorders in adolescence (Leve et al., 2005). Comparatively, females tend to readily express emotion and work through the problem until a resolution is found (Fivush et al., 2007); however, this approach to resolving emotion could also promote rumination, which is linked with poorer coherence and wellbeing (Vanderveren et al., 2020). Of note, these findings reflect a difference in the quality of emotion resolution, rather than quantity of emotion, of which an interaction was not observed for emotion exploration and gender. It is important to note that these mechanisms are speculative, and that although there is a statistical difference observed for males in the clinical cohort, clinical significance has not been tested and further research is needed to identify the clinical utility of these differences.
This study is unique in its approach to reminiscing conversations, in addressing child mental health as the focus in middle childhood, as well as including future focused conversations. This study is the first to examine associations of past and future negative emotion conversations to child mental health outcomes. Other strengths include the coding of different aspects of emotion conversations. We also collected multiple measures of child mental health symptoms so although no diagnostic interviews were used, we were able to establish clear differences in the two cohorts; yet cohorts were also matched on language, gender, and ethnicity. Importantly, the current study also controlled for child language ability, which adds to the robustness of our findings.
Although our clinical recruitment and measurement of symptoms was sufficient, children had not yet received a formal diagnosis. McLeod et al. (2007) did note the strength that a formal diagnosis can provide in comparison to non-clinical samples. Percy et al. (2016) expanded on these approaches in a review, which compared either diagnosis comparison studies, or non-clinical community cohorts which used symptomology measures to split the cohort. Our study utilized a balanced approach; although it did not utilize formal diagnostic interviews, the clinical sample was recruited directly from a mental health clinic where an intake assessment by a clinician provided an informal diagnostic clarification of internalizing difficulties rather than a formal diagnostic interview. Not only did this recruitment process decrease demands on the children in the research session, but also ensured data collection prior to waitlisted therapeutic intervention where a formal diagnosis may occur. We did not account for the various levels of previous intervention the dyads may have had at an earlier time, which may or may not be reflected in parents’ conversational style. Moreover, the application of our findings may only be applied broadly to anxiety difficulties rather than the clarity a diagnosis would provide here.
Parent mental health should also be considered in interpreting these findings as a small body of research has observed differences in reminiscing as a function of parent mental health (Cimino et al., 2020; Reese et al., 2019; Swetlitz et al., 2021; Van der Giessen & Bögels, 2018). Exploring parent mental health symptoms was outside the scope of this paper and has been addressed in a parallel study (Russell et al., 2023). As discussed in Suveg et al. (2005), children of parents with high anxiety and stress symptoms may in turn choose to discuss emotional events in a different way to other children. Thus, differences may reflect parent as well as child mental health differences across the two groups. Moreover, examining the differences in parent mental health from a transdiagnostic lens would assist in understanding parent’s own difficulties in regulating, and mindfulness that may interfere with the ability to hold these difficult conversations, and attune to their child (Dalgleish et al., 2020). Following investigation of parent factors, future research should investigate the potential transmission of mental health from parent to child. These everyday emotion reminiscing conversations may be one way that intergenerational transmission of mental health symptoms occurs (Swetlitz et al., 2021).
As with much in-depth observational research, the sample size of this study is small. The sample is predominantly white and highly educated. We acknowledge this is a limitation of the study, making note of the sensitivity analysis, and as such the results should be considered preliminary and interpreted with caution. Furthermore, due to the cross-sectional nature of this research, direction of causality cannot be attained. We cannot be certain if what we have observed is contributing to their mental health difficulties, or if observed differences are the dyad’s attempts to resolve the current issues for which they have been referred. A follow up study utilizing longitudinal research would help clarify how reminiscing may be helpful in clinical interventions. Moreover, we did not exclude children with a prior diagnosis or treatment in the community cohort, which could have an impact on our findings. Despite this, children in the clinical cohort had reached a level of distress which required intervention, which likely reflects a meaningful difference in the lives of these families. Likewise, the past and future aspects of these decontextualized conversations parallel a need for further research of present moment emotion coaching to support parents supporting their children with anxiety.
In conclusion, this study has revealed a pattern of less emotion exploration in anticipated future worry conversations for families of children with anxiety. Clinical families past reminiscing conversations showed lower emotion exploration from parents, however children did not differ between cohorts. Neither elaboration nor emotion resolution quality differed between cohorts; however, a statistical interaction effect was observed with cohort and child gender. Boys with anxiety were more likely to have poorer resolutions than girls with anxiety or both genders in the community cohort. As parent-child emotion reminiscing has been found to be modifiable (Corsano et al., 2019; Van Bergen et al., 2009) with long-term benefits for children’s wellbeing (Mitchell et al., 2020), these findings may inform family-based interventions to support parents in emotion exploration during reminiscing. Future research should investigate longitudinal parent and child mental health with reminiscing as a potential mechanism of mental health transmission in families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Australian Rotary Health with a PhD Scholarship awared from Josephine Margaret Redfern and Ross Edward Redfern (Rotary Club of Granville); and the University of Wollongong Early Career Researcher Grant (2018).