
Abstract
Adolescent anhedonia is a multidimensional construct defined as the loss of enjoyment or pleasure across multiple domains of life. Anhedonia is concurrently associated with substantial impairment and distress, and it prospectively predicts the onset, severity, and treatment of depression. Despite its demonstrated importance, a limited number of anhedonia measures are validated for adolescents. The current study assessed the psychometric properties of the Dimensional Anhedonia Rating Scale (DARS) in 400 English-speaking, 12- to 19-year-old adolescents. Overall, the DARS demonstrated good convergent and discriminant validity, but sub-optimal concurrent validity. The strengths and limitations of the DARS and its utility as a measure of adolescent anhedonia are discussed. Furthermore, future directions for the construction of measures of adolescent anhedonia are outlined.
Introduction
Anhedonia, the loss of pleasure when anticipating or engaging in pleasurable activities, plays an integral role in the development and presentation of adolescent depression (Bennett et al., 2005; Forbes & Dahl, 2012; Kouros et al., 2016; Watson et al., 2020). Indeed, adolescent anhedonia predicts the onset of later major depressive disorder (MDD; Kouros et al., 2016; Wilcox & Anthony, 2004), more severe depressive episodes (Gabbay et al., 2015), and poor treatment response amongst adolescents with depression (McMakin et al., 2012). Despite being implicated in numerous deleterious outcomes, anhedonia remains an understudied phenomenon in adolescents (Forbes & Dahl, 2012; Kouros et al., 2016; McCabe, 2018; Watson et al., 2020), partially due to challenges in comprehensively detecting and measuring anhedonia in adolescents. Assessment of adolescent anhedonia is made difficult by its multidimensional nature (e.g., the anticipation vs. consummatory reward experience; Rizvi et al., 2015; 2016; Watson et al., 2020), and the broad number of domains adolescent anhedonia can disrupt (e.g., physical, social, sensory; Watson et al., 2020). Given the importance of anhedonia in adolescence, there is a need for reliable, valid, and comprehensive questionnaires that can accurately detect and measure anhedonia in this vulnerable demographic.
One shortcoming of existing tools for adolescent anhedonia assessment is that, despite anhedonia being a multidimensional construct, many of the available measures for adolescent anhedonia are unidimensional. Theoretical and empirical work suggests that anhedonia is driven by at least two dimensions: (1) consummatory anhedonia, the lack of immediate pleasure or enjoyment; and (2) anticipatory anhedonia, the inability to foresee oneself enjoying or gleaning pleasure from various activities (Gooding et al., 2016; Rizvi et al., 2016; Watson et al., 2020). Importantly, these dimensions predict distinct outcomes. For example, consummatory anhedonia predicts poor psychosocial functioning (Vinckier et al., 2017), whereas anticipatory anhedonia has been associated with depressive symptoms (Ho et al., 2015). Furthermore, anticipatory anhedonia, but not consummatory anhedonia, predicts reductions in effort and motivation (Sherdell et al., 2012). Therefore, assessing only one dimension of anhedonia does not fully capture adolescence experience in response to rewarding stimuli. Despite the importance of assessing various dimensions of anhedonia, however, many of the current measures of anhedonia for adolescents focus on just one dimension. For example, two of the frequently used measures of anhedonia, the Snaith Hamilton Pleasure Scale (SHAPS; Snaith et al., 1995; Leventhal, 2015) and the anhedonia subscale of the Child Depressive Inventory (CDI; Kovacs, 1985) specialize in assessing consummatory anhedonia exclusively.
Researchers also note the importance of examining the impact of anhedonia on domains of life relevant to adolescents. Adolescents with anhedonia experience diminished interest in various life domains, including social activities (Gooding et al., 2016; Watson et al., 2020) and sensory pleasures (e.g., hobbies, eating/drinking, and sensory experiences; Watson et al., 2020). Although measures have been validated in adolescent samples, they either include items unrelated to adolescents’ daily experiences or assess the effect of anhedonia in only one domain of adolescent life. For instance, Watson et al. (2020) criticizes the SHAPS (Snaith et al., 1995) and Temporal Experience of Pleasure Scale (TEPS; Rzepa & McCabe, 2019) because they assess engagement with experiences more commonly enjoyable to adults than adolescents, such as taking a warm bath/refreshing shower, the scent of flowers, or the sound of crackling wood in the fireplace. Thus, these measures may not tap into pleasurable or desirable experiences relevant to adolescents. Alternatively, other measures (e.g., the Anticipatory and Consummatory Interpersonal Pleasure Scale – Adolescents [ACIPS-A]; Gooding et al., 2016) focus on the anhedonic experience within the social domain specifically, despite evidence that other domains of anhedonia (e.g., physical anhedonia) are also relevant to the development, maintenance, and severity of depression (e.g., Loas et al., 1992; Shankman et al., 2010). Thus, although the existing adolescent anhedonia measures may provide valuable snapshots into dimensions or domains of anhedonia, they were not designed to capture the multidimensional nature of anhedonia and the multiple domains that it can influence in adolescence.
One measure that may fill this gap is the Dimensional Anhedonia Rating Scale (DARS; Rizvi et al., 2015). The DARS assesses different dimensions of anhedonia, including consummatory anhedonia and anticipatory anhedonia, across four domains: Hobbies, Food/Drinks, Social Activities, and Sensory Experiences. In each domain, participants generate examples of pleasurable activities from their own life; thus overcoming concerns we outlined earlier about age differences in interests and rewards (McCabe, 2018). Participants then rate how much they agree with a set of statements that assess their interest, motivation, effort, and liking of their listed activities on a 5-point Likert scale. The DARS was developed and validated in three separate samples of adult participants, and it demonstrated good convergent validity with other measures of anhedonia (r = .5 - .8), good concurrent validity with depression (r = .4 - .5), and good discriminant validity with measures of physical activity and behavioral inhibition (Rizvi et al., 2015). Furthermore, DARS demonstrated exceptional utility in distinguishing between healthy individuals and individuals with treatment-resistant depression (Rizvi et al., 2015). Since publication of the DARS, its validity in adults has been assessed and established in different languages, including Spanish (Arrua-Duarte et al., 2019), Chinese (Ching et al., 2021), and German (Wellan et al., 2021). The DARS has also been validated in a sample of Chinese adolescents (Xiao et al., 2022); however, its psychometric properties have not yet been assessed in a sample of English-speaking adolescents. Given the importance of cross-cultural validity (Souza et al., 2017), we aimed to assess the validity of DARS in English-speaking adolescents residing in North America.
The current study was designed to test the psychometric properties and validity of the DARS in a convenience sample of English-speaking adolescents in the United States and Canada. Toward this goal, the DARS and a battery of questionnaires were administered to adolescents 12–19 years of age (cf. World Health Organization, 2022; definition of adolescence). It was hypothesized that the DARS and its subscales (Hobbies, Food/Drinks, Social Activities, and Sensory Experiences) would demonstrate good reliability as evidenced by good internal consistency (i.e., within the range of α = .70 - .95; Taber, 2018). Furthermore, it was hypothesized that the DARS and its subscales would demonstrate good convergent and concurrent validity. Convergent validity reflects how much the DARS is related to other measures that assess the same or similar constructs. Thus, consistent with validations of other anhedonia measures (Gard et al., 2006; Gooding & Pflum, 2011; Rizvi et al., 2015), convergent validity of the DARS was assessed by examining its association with measures of social anhedonia and behavioural activation system. Concurrent validity reflects how much the DARS can predict a related criterion (e.g., a related construct or relevant behavior) that is happening concurrently. Thus, consistent with other validations of anhedonia measures (Gooding & Pflum, 2011; Rizvi et al., 2015; Winer et al., 2014), concurrent validity of the DARS was assessed by examining its association with measures of depression and affect. Correlation coefficients higher than .45 generally indicate good convergent and concurrent validity (DeVon et al., 2007). Finally, it was hypothesized that the DARS and its subscales would demonstrate good discriminant validity. Discriminant validity assesses whether the DARS measures constructs less related to or unrelated to anhedonia. Thus, consistent with previous validation of DARS (Rizvi et al., 2015), discriminant validity of the DARS was assessed by examining its association with measures unrelated to anhedonia (e.g., intelligence, physical activity, anxiety). Correlations smaller than .45 are generally thought to indicate good discriminant validity (DeVon et al., 2007), though negligible correlations (r < .1) are expected with constructs that are completely unrelated to anhedonia (e.g., intelligence) and small to medium correlations (r = .1 - .45) are expected with constructs with some, albeit small, overlap with anhedonia (e.g., anxiety).
Methods
Participants
Demographic Information of participants. Mean and SD are Presented for Continuous Variables, and Frequency and Percentage are Presented for the Categorical Variables.
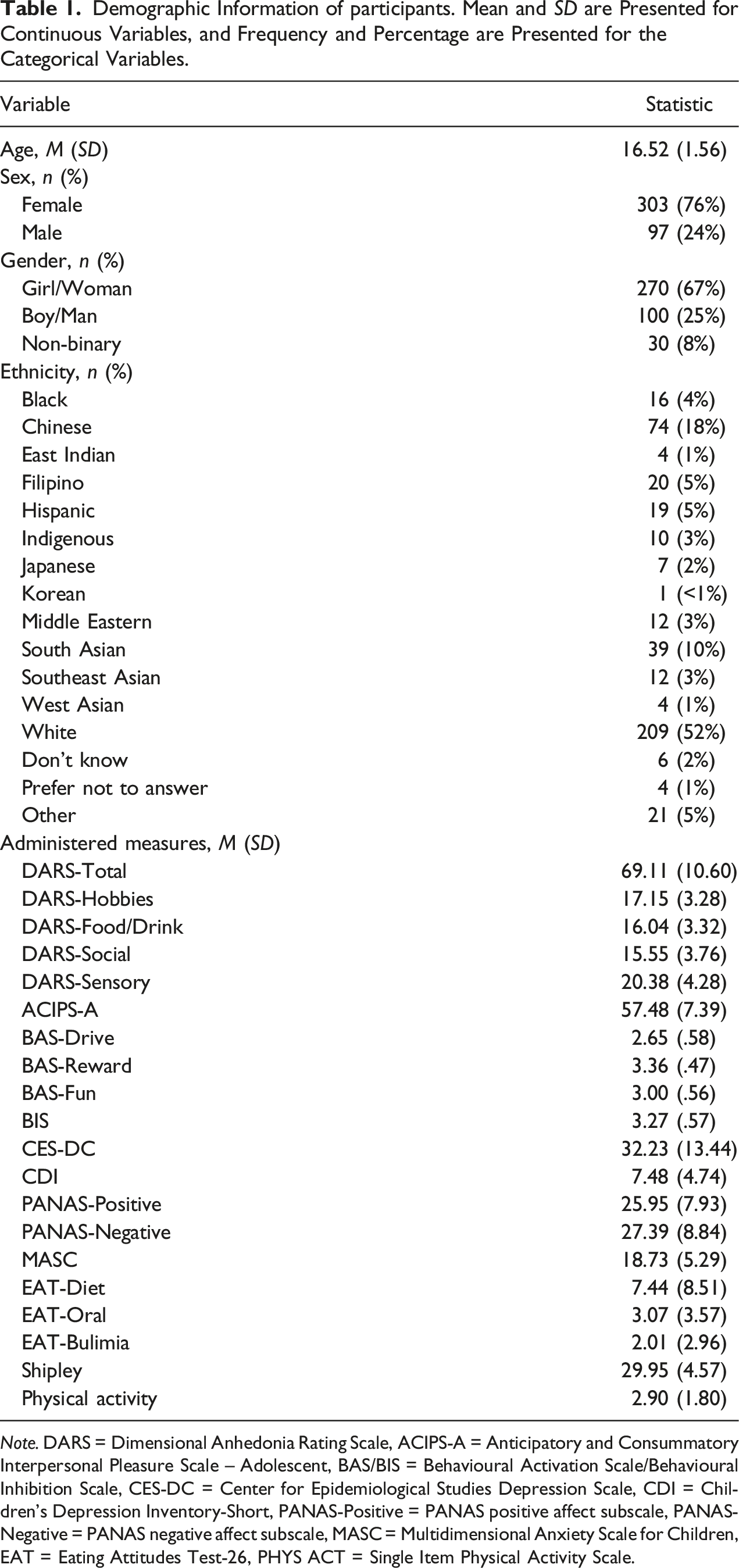
Note. DARS = Dimensional Anhedonia Rating Scale, ACIPS-A = Anticipatory and Consummatory Interpersonal Pleasure Scale – Adolescent, BAS/BIS = Behavioural Activation Scale/Behavioural Inhibition Scale, CES-DC = Center for Epidemiological Studies Depression Scale, CDI = Children’s Depression Inventory-Short, PANAS-Positive = PANAS positive affect subscale, PANAS-Negative = PANAS negative affect subscale, MASC = Multidimensional Anxiety Scale for Children, EAT = Eating Attitudes Test-26, PHYS ACT = Single Item Physical Activity Scale.
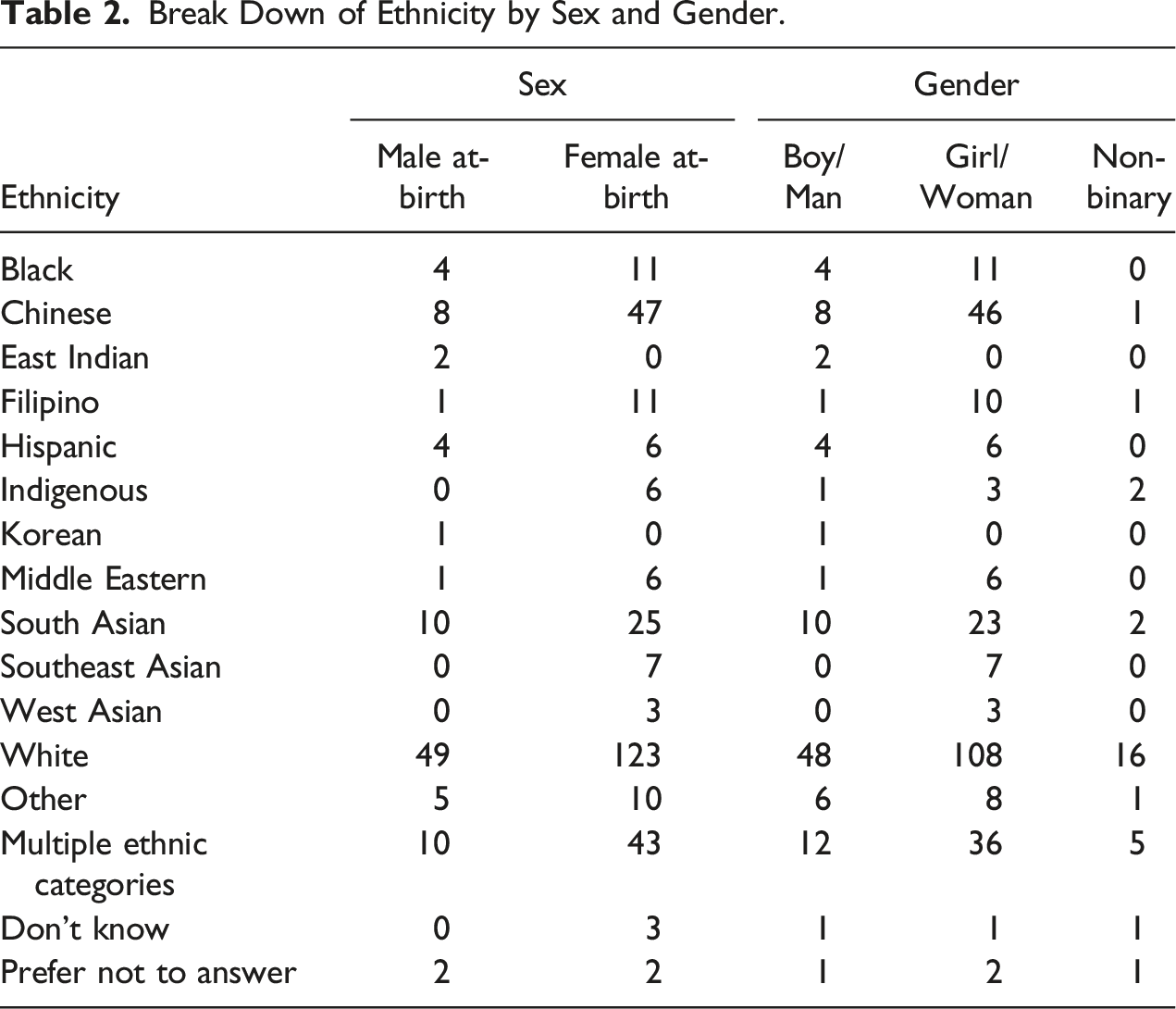
Break Down of Ethnicity by Sex and Gender.
Procedures
The study was approved by the University of British Columbia Behavioral Research Ethics Board and was conducted online. Adolescents between 12 and 16 years old provided assent, and a parent/guardian provided consent. Adolescents older than 16 provided consent for themselves. After consent (and assent) was provided, participants completed a series of questionnaires and reported their demographic information.
Measures
Dimensional Anhedonia Rating Scale
The DARS (Rizvi et al., 2015) is a 17-item self-report anhedonia measure that assesses anhedonia across four domains: Hobbies, Food/Drinks, Social Activities, and Sensory Experiences. Participants were asked to generate examples of enjoyable activities or stimuli in each domain and rate them on a 5-point Likert scale. Sample items include “I would enjoy these activities” and “I would actively seek out these experiences.” Consistent with Rizvi et al. (2015), responses were summed to create subscale scores and a total score. Higher scores indicate lower levels of anhedonia. The DARS full scale demonstrated good internal consistency in our sample (α = .89), as did the subscales: Hobbies (α = .89), Food/Drinks (α = .77), Social Activities (α = .86), and Sensory Experiences (α = .88).
Convergent Validity
Convergent validity of the DARS was assessed by examining its association with another measure of anhedonia (the ACIPS-A; Gooding et al., 2016) and a measure of behavioral activation (the Behavioral Activation Scale of the Behavioral Inhibition Scale-Behavioral Activation Scale [BIS-BAS]; Carver & White, 1994). The ACIPS-A was selected as it is the only multidimensional measure of anhedonia modified and validated in an adolescent population. The behavioral activation scale (BAS scale) of the BIS-BAS was selected as it, especially the BAS-Reward subscale, has been extensively used to validate different measures of anhedonia (e.g., Gard et al., 2006; Gooding & Pflum, 2011), including the DARS (Rizvi et al., 2015).
Anticipatory and Consummatory Interpersonal Pleasure Scale- Adolescent
The ACIPS-A (Gooding et al., 2016) is a 17-item self-report adolescent anhedonia measure that assesses social anhedonia across two dimensions: consummatory and anticipatory. Sample items include “I enjoy looking at photographs of my friends and family” and “I like talking with others while waiting in line.” Participants rated each ACIPS-A item on a 4-point Likert scale, and responses were summed. Higher scores indicate lower social anhedonia. The ACIPS-A demonstrated good internal consistency in our sample (α = .83).
Behavioral Inhibition Scale/Behavioral Activation Scale
The BIS-BAS (Carver & White, 1994) is a 24-item self-report measure that assesses the motivational system. The behavioral inhibition scale (BIS) measures motivation to avoid unpleasant or aversive outcomes, and the behavioral activation scale (BAS) measures motivation to seek or pursue positive or goal-oriented outcomes (Carver & White, 1994). A sample BIS item is “criticism or scolding hurts me quite a bit,” and a sample BAS item is “I go out of my way to get things I want.” The BIS-BAS consists of four subscales, the BIS subscale and three BAS subscales that measure reward sensitivity (BAS-Reward), drive (BAS-Drive) and fun seeking (BAS-Fun). Participants rated each BIS-BAS item on a 4-point Likert scale, and responses were averaged. Higher scores reflect increased activation of the respective system. The BIS-BAS demonstrated acceptable internal consistency in our sample: BIS (α = .80), BAS-Drive (α = .75), BAS-Fun (α = .63), and BAS-Reward (α = .68).
Concurrent Validity
Concurrent validity of the DARS was assessed by examining its association with measures of depression (the CDI, Kovacs, 2003; the Center for Epidemiological Studies Depression Scale [CES-DC], Faulstich et al., 1986) and a measure of positive and negative affect (the Positive and Negative Affect Scale Short Form [PANAS-SF], Watson et al., 1988). The CES-DC was selected as the adult version (CES-D; Radloff, 1977) was used to assess the concurrent validity of the DARS when its psychometric properties were assessed in an adult sample (Rzivi et al., 2015). The CDI and PANAS were selected as they have been used to validate other measures of anhedonia (Gooding & Pflum, 2011; Winer et al., 2014). The two measures of depression were both included because one, CES-DC, assesses the frequency of depressive symptoms, and the other, CDI, assesses the severity of depressive symptoms.
Center for Epidemiological Studies Depression Scale
The CES-DC (Faulstich et al., 1986) is a 20-item self-report measure that assesses the frequency of depressive symptoms in adolescents. Sample items include “I felt down and unhappy” and “I was more quiet than usual.” Participants rated each CES-DC item on a 4-point Likert scale, and responses were summed. Higher scores reflect more severe depressive symptoms. The CES-DC demonstrated good internal consistency in our sample (α = .93).
Children’s Depression Inventory-Short
The CDI (Kovacs, 2003) is a 10-item self-report measure that assesses the severity of depressive symptoms in adolescents. Participants rated each CDI item on a 3-point scale, and responses were summed. Higher scores reflect more severe depressive symptoms. The CDI demonstrated good internal consistency in our sample (α = .87).
Positive and Negative Affect Scale Short Form
The PANAS (Watson et al., 1988) is a 20-item self-report measure of affect, with two subscales: a 10-item positive affect subscale (e.g., excited, interested) and a 10-item negative affect subscale (e.g., upset, guilty). Participants rated each PANAS item on a 5-point Likert scale, and responses were summed. Higher scores reflect higher levels of the respective affect. The positive affect subscale (α = .87) and the negative affect (α = .88) subscale both demonstrated good internal consistency in our sample.
Discriminant Validity
Discriminant validity of the DARS was assessed by examining its association with measures unrelated or minimally related to anhedonia: intelligence (Shipley Verbal Intelligence Test; Shipley et al., 2009), physical activity (Single Item Physical Activity Scale; Scott et al., 2015), behavioral inhibition (BIS scale of BIS-BAS; Carver & White, 1994), anxiety (Anxiety Scale for Children [MASC]; March et al., 1997), and disordered eating (Eating Attitudes Test-26 [EAT-26]; Garner et al., 1982). The Shipley intelligence test was included because we expected no correlation between a measure of anhedonia and intelligence. Therefore, the correlation with Shipley could act as a benchmark to assess the discriminant validity of DARS against other constructs that DARS should be unrelated or minimally related. The measure of physical activity and the behavioral inhibition (BIS) scale of the BIS-BAS were selected as they have both been used previously to validate the DARS (Rizvi et al., 2015). A measure of anxiety (MASC) was included to assess whether the DARS distinguished anhedonia in the social domain from general anxiety, and a measure of disordered eating (EAT-26) was included to assess whether the DARS distinguished anhedonia in the food/drink domain from disordered eating more broadly.
Shipley Verbal Intelligence Test
The Shipley Verbal Intelligence Test (Shipley et al., 2009) is a 40-item measure of verbal intellectual capacity. Participants were asked to find the best synonym of each reference word among the four options. The Shipley demonstrated good internal consistency in our sample (α = .78).
Single Item Physical Activity Scale
This 1 item physical activity scale measured how many days in the past week adolescents exercised for at least 1 hour and was designed for and validated in adolescents (Scott et al., 2015).
Multidimensional Anxiety Scale for Children
The MASC (March et al., 1997) is a 10-item child and adolescent measure of anxiety. Participants rated each MASC item on a 5-point Likert scale, and responses were summed. Higher scores indicate more severe anxiety symptoms. MASC demonstrated good internal consistency in our sample (α = .73).
Eating Attitudes Test-26
The EAT-26 (Garner et al., 1982) is a 26-item self-report measure that assesses disordered eating behaviors and cognitions across three subscales: dieting, bulimia, and oral control. Sample items include “I avoid foods with sugar in them” and “I am terrified about being overweight.” The EAT-26 was scored on a 6-point scale, and responses were summed. Higher scores indicate greater severity of symptoms. EAT-26 subscales demonstrated acceptable reliability in our sample: EAT-Dieting (α = .90), EAT-Bulimia (α = .69), and EAT-Oral control (α = .68).
Data Analytic Plan
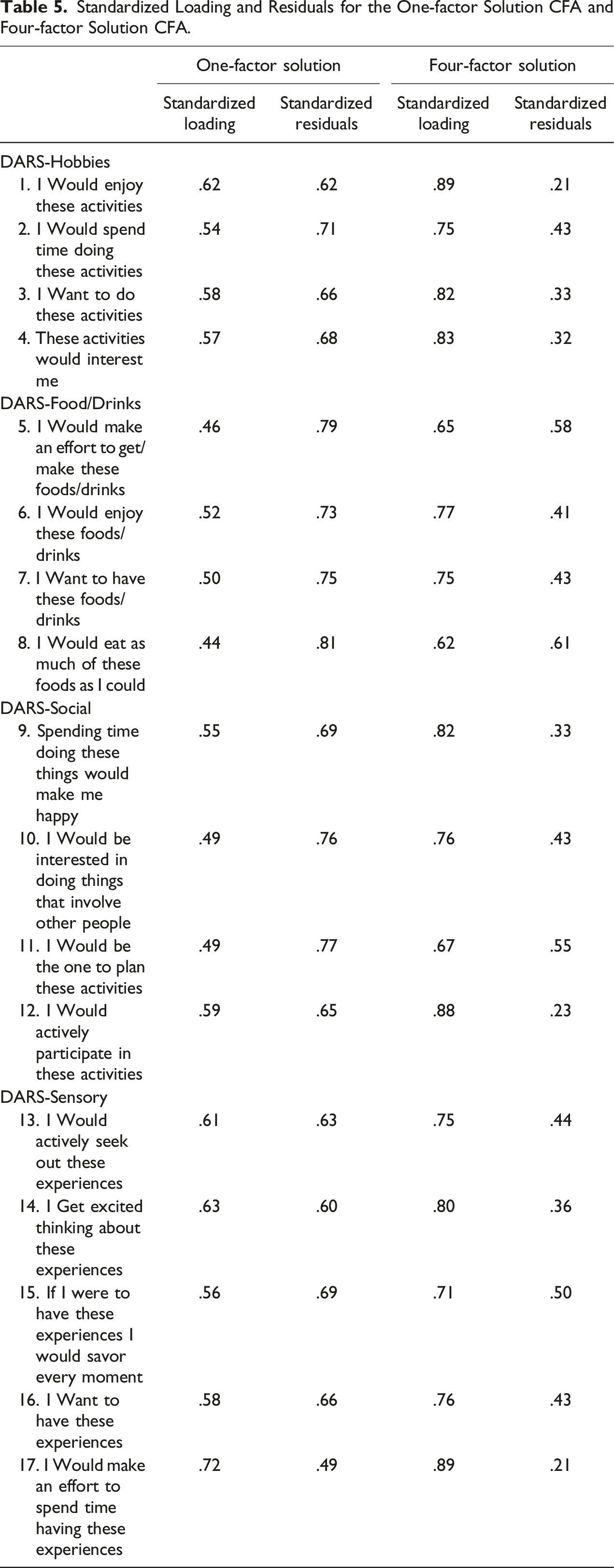
All analyses were conducted in R 4.3.0 (R Core Team, 2023). We ran the CFA with maximum likelihood using the Lavaan package (Rosseel, 2012). We assessed two models using CFA. The first model is a first-order CFA with one latent variable that corresponds to the total score on the DARS and the items as the indicator variables. The second model is a second-order CFA with a second-order factor corresponding to the total score on the DARS, four first-order factors corresponding to the four DARS subscale scores (i.e., the Social Activities, Hobbies, Sensory Experiences, and Food/Drinks subscales), and the DARS items as indicator variables. We interpreted the acceptability of the factor loadings as follows: excellent (∼.71), very good (∼.63), good (∼.55), fair (∼.45), and poor (∼.32; Comrey & Lee, 1992). We assessed model fit using the non-incremental fit indices, including the Comparative Fit Index (CFI), the Tucker Lewis Index (TLI), the root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR). CFI and TLI above .95, SRMR below .08, and RMSEA below .06 indicate good model fit (Hu & Bentler, 1999).
To assess the internal consistency of the DARS, we calculated Cronbach’s alpha and McDonald’s ω using the psych package (Revelle, 2015). Cronbach’s alpha measures the degree of correlation between items in a given measure (Cronbach, 1951). The value of Cronbach’s alpha depends on various factors such as the number of items in a measure, the interconnectedness of the items, and the consistency of the responder (Vaske et al., 2017). Although from a theoretical perspective, a cutoff value for Cronbach’s alpha is not recommended (Agbo, 2010), both previous academic work (see Tavakol & Dennick, 2011) and common practices in reporting Cronbach’s alpha in scientific papers (see Taber, 2018) suggest that values between .70 and .95 reflect acceptable internal consistency, with higher values generally indicating better internal consistency.
Given that Cronbach’s alpha is not adequate to assess the unidimensionality of a measure (Agbo, 2010), we also assessed McDonald’s ω. Omega coefficients take the multidimensionality of the measures into account; Omega Total (ωt) estimates the variance accounted for by all DARS factors, and the Omega Hierarchical (ωh) estimates the variance explained by the general factor (Revelle & Condon, 2019). Higher ωt suggests that the measure likely has multiple factors, whereas higher ωh (>.8) suggests that the measure is likely unidimensional (Rodriguez et al., 2016).
To assess the DARS’s convergent, concurrent, and discriminant validity, we calculated correlations using the stats package (R Core Team, 2013). Specifically, we assessed convergent validity based on the association between the DARS and its subscales with other measures of anhedonia (the ACIPS-A) and a measure of behavioral activation (the BAS subscale). To assess the concurrent validity of the DARS, we assessed its association with measures of depression (the CES-DC and CDI) and affect (the PANAS positive and negative subscales). Finally, to assess the discriminant validity of the DARS, we assessed the association of the DARS with measures of vocabulary (the Shipley), behavioral inhibition (the BIS subscale), physical activity (the Single Item Physical Activity Scale), anxiety (the MASC), and disordered eating (the EAT-26). Given that the DARS Total score and subscale scores were not normally distributed, we calculated Spearman correlations (r s ). Given that 75 correlations were conducted to assess the validity of the DARS, we emphasize the magnitude of the associations rather than their significance level. The following cutoffs were used to evaluate the magnitude of correlations: small (rs <.30), medium (.30 ≤ rs <.50), and large (rs ≥ .50; Cohen, 1988). In addition, a Bonferroni correction was used (Bonferroni, 1936), and only p-values less than .001 were considered significant.
Finally, we assessed the relationship between DARS and demographic variables. Given that both sex and gender did not meet the assumption of homogeneity of variance as assessed by Levene’s test for equality of variances (p < .05), we used the Mann–Whitney U test to assess the association of the DARS with sex at-birth, and we used the Kruskal–Wallis test to assess the association of the DARS with gender. Ethnicity met the assumption of homogeneity of variance (p > .05). Therefore, we used one-way analysis of variance to assess the association between DARS and ethnicity. Mann-Whitney U and Kruskal-Wallis, were calculated using the stats package (R Core Team, 2013), and the post-hoc test for the Kruskal-Wallis, the Dunn test (Zar, 2010), was conducted using the FSA package (Ogle et al., 2023).
Results
Descriptive Information
Intercorrelation Between DARS Subscales. The Spearman Correlations Between DARS Subscales are included in this Table.
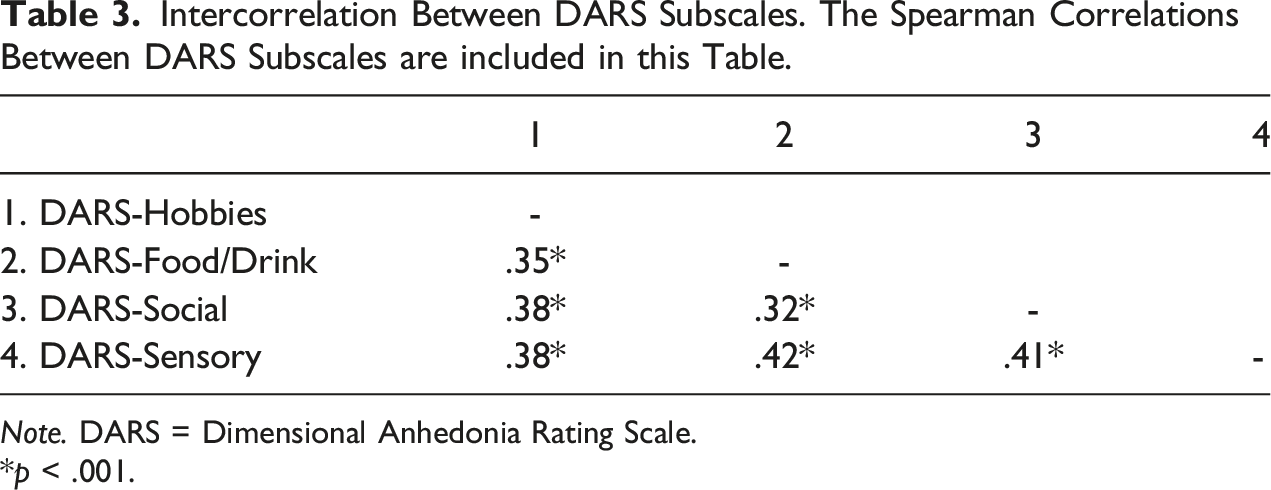
Note. DARS = Dimensional Anhedonia Rating Scale.
*p < .001.
Demographic Differences in DARS and its Subscales.
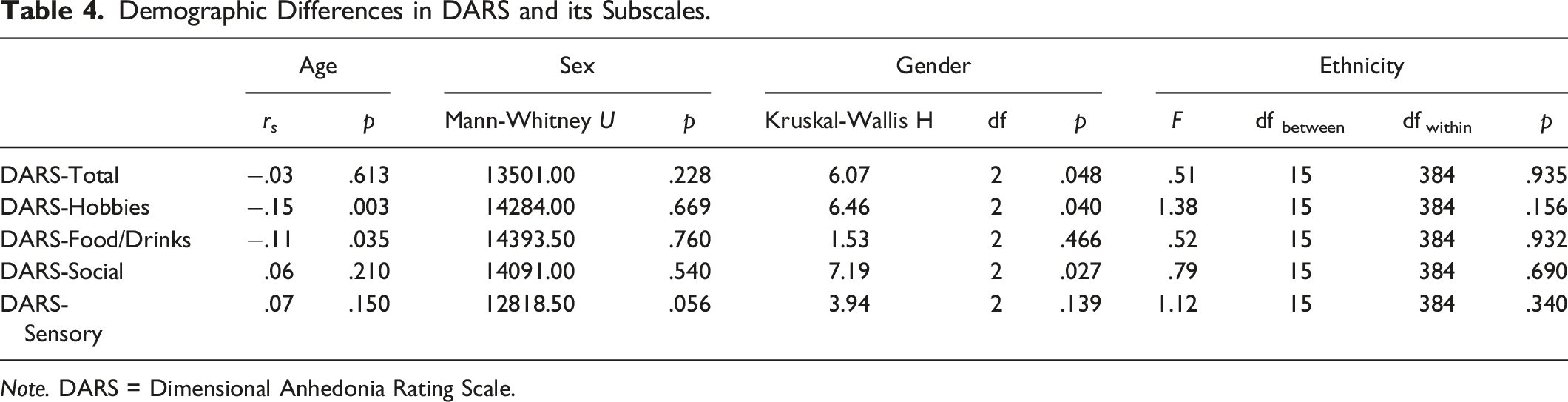
Note. DARS = Dimensional Anhedonia Rating Scale.
Confirmatory Factor Analysis
Standardized Loading and Residuals for the One-factor Solution CFA and Four-factor Solution CFA.
Internal Consistency
The McDonald’s Omega coefficients provided further evidence for the multidimensionality of DARS, evidenced by a ωh below .80: (ωh = .66), which suggests separate dimensions of anhedonia measured by the DARS. Furthermore, DARS and its subscales demonstrated acceptable Cronbach α: Total scale, α = .89, Hobbies, α = .89, Food/Drinks, α = .77, Social Activities, α = .86, Sensory Experiences, α = .88.
Convergent Validity
Convergent, Concurrent, and Discriminant Validity of DARS and its Subscales. Spearman Correlation Between DARS and its Subscales and Measures of Convergent, Concurrent, and Discriminant Validity are Included in this Table.
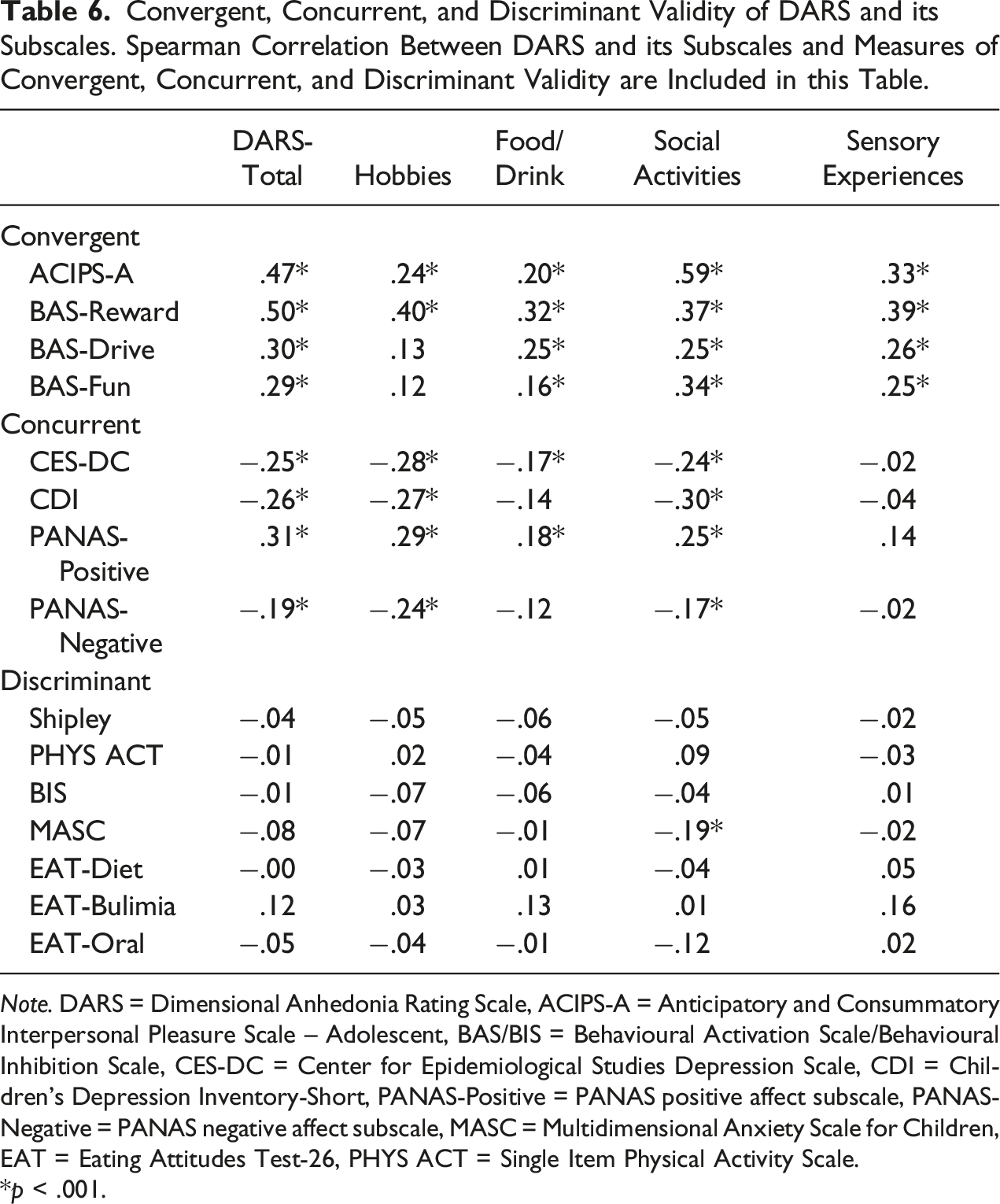
Note. DARS = Dimensional Anhedonia Rating Scale, ACIPS-A = Anticipatory and Consummatory Interpersonal Pleasure Scale – Adolescent, BAS/BIS = Behavioural Activation Scale/Behavioural Inhibition Scale, CES-DC = Center for Epidemiological Studies Depression Scale, CDI = Children’s Depression Inventory-Short, PANAS-Positive = PANAS positive affect subscale, PANAS-Negative = PANAS negative affect subscale, MASC = Multidimensional Anxiety Scale for Children, EAT = Eating Attitudes Test-26, PHYS ACT = Single Item Physical Activity Scale.
*p < .001.
Concurrent Validity
The concurrent validity of the DARS was assessed by examining its correlation with depression frequency (CES-DC), depression severity (CDI), positive affect (PANAS-Positive), and negative affect (PANAS-Negative). These findings are summarized in Table 6. The DARS-Total score demonstrated small to moderate correlations with measures of depression, CES-DC, r s = −.25, p < .001, CDI, r s = −.26, p < .001, a moderate correlation with positive affect (PANAS-Positive), r s = .31, p < .001, and a small correlation with negative affect (PANAS-Negative), r s = −.19, p < .001. The Hobbies and Social subscales of DARS also showed small to moderate correlations with measures of depression and affect, r s = |.17 - .30|, ps < .001, and the Food/Drink subscale of DARS showed small correlations with these measures, r s = |.12 - .18|, ps <.001 - .017 - (see Table 6). The Sensory subscale was not significantly correlated with any concurrent validity measures, r s = |.04 - .14|, ps = .005 - .655. The strength of the correlations between DARS and measures of concurrent validity all fell below the cutoff of r ≥ .45 recommended by DeVon et al. (2007).
Discriminant Validity
The discriminant validity of DARS was assessed by examining its correlation with intelligence (Shipley vocabulary score), behavioral inhibition (BIS), physical activity (single-item measure), anxiety (MASC), and disordered eating (EAT-Diet, EAT-Bulimia, and EAT-Oral). These findings are summarized in Table 6. The DARS total score and its subscales demonstrated very small, and primarily nonsignificant, correlations with intelligence, motivation to avoid negative outcomes, physical activity, anxiety, and disordered eating behaviors and cognitions. The only significant correlation was between the DARS-Social subscale and anxiety (MASC), r s = −.19, p < .001. Symptoms of bulimia (EAT-Bulimia) also showed a small, albeit nonsignificant, correlation with DARS-Total score, r s = .12, p = .042, DARS-Food/Drink, r s = .13, p = .027, and DARS-Sensory, r s = .16, p = .005. Eat-Oral also showed a small nonsignificant correlation with DARS-Social, r s = −.12, p = .046. All the other correlations between DARS and the measures of discriminant validity were negligible and nonsignificant, r s < |.1|, p = .117 – .999. The strength of the correlations between the DARS and measures of discriminant validity met the cutoff (r < .45) recommended by DeVon et al. (2007).
Discussion
Overall, the results of our study indicate that the DARS demonstrated good factor structure and reliability, consistent with results documented by Rizvi et al. (2015) in an English-speaking adult sample. The DARS and its subscales also demonstrated good convergent and discriminant validity, further supporting that the DARS is a reliable and valid measure of anhedonia in adolescents. However, the DARS demonstrated lower-than-expected concurrent validity in our sample, suggesting that the DARS did not consistently measure a construct associated with adolescent depression or affect.
Convergent validity was assessed by examining associations of the DARS with the ACIPS-A, BAS-Reward, BAS-Drive, and BAS-Fun. These associations were significant and in the small to strong range. For example, both the DARS-Social subscale and the DARS-Total score demonstrated a strong association with social anhedonia as measured by ACIPS-A, which replicates past adult research in both the magnitude and direction of associations (e.g., Wellan et al., 2021) and provides support for the DARS ability to detect anhedonia, particularly in the social domain. Although the DARS was also positively associated with behavioral activation subscales, the strength of these associations varied. Specifically, associations between the DARS and the reward sensitivity subscale (BAS-Reward) were moderate. Yet, associations of the DARS with a drive to achieve goals (BAS-Drive) and novelty-seeking (BAS-Fun) ranged from small to moderate. The moderate association between the DARS and BAS-Reward subscale replicates past research (Rizvi et al., 2015; Xiao et al., 2022), and ultimately supports the convergent validity of the DARS. Although associations of the DARS with the BAS-Drive and BAS-Fun subscales were weaker than expected, it may be because these BAS subscales assess externalizing symptoms less central to anhedonia (e.g., Taubitz et al., 2015). Indeed, other researchers have also found weak associations of the DARS with a drive to achieve goals (BAS-Drive) and novelty-seeking (BAS-Fun; Rizvi et al., 2015; Xiao et al., 2022). Thus, associations of the DARS with other measures of adolescent anhedonia and BAS subscales were reasonable given past research, and generally support its ability to detect deficits in reward responsiveness and reward processing in adolescents.
The discriminant validity of the DARS was assessed by comparing its association with intelligence (Shipley vocabulary score), behavioral inhibition (BIS), physical activity, anxiety (MASC), and disordered eating (EAT-Diet, EAT-Bulimia, and EAT-Oral). As expected, the DARS-Total or subscale scores was not significantly associated with intelligence (Shipley vocabulary score), behavioral inhibition (BIS), or physical activity. However, there was a significant, albeit small, association between the DARS-Social subscale and anxiety as measured via the MASC. However, this association was not entirely unexpected given that anxiety has been linked to social anhedonia (e.g., Barkus, 2021; Yang et al., 2022). Indeed, Yang et al. (2022) also documented a positive association between adolescent anhedonia (as measured by the ACIPS-A) and heightened levels of generalized and social anxiety (Yang et al., 2022). The DARS Total score and/or its subscales also demonstrated a small, but nonsignificant, correlation with disordered eating as measured via the EAT-Bulimia and EAT-Oral subscales. In particular, the DARS-Food/Drink subscale showed a small correlation with the EAT-Bulimia subscale. This finding is consistent with observations that individuals with eating disorder symptoms may experience less enjoyment, interest, and time spent eating/drinking (Dolan et al., 2022). Additionally, other research has documented associations between anhedonia and various alternative types of disordered eating, including heightened anhedonia and reward learning impairments in patients that recovered from bulimia nervosa (Dolan et al., 2022). Thus, despite some overlap of the DARS with the MASC and the EAT Bulimia and Oral subscales, the small magnitude of the correlations suggests the DARS does not function as a measure of these constructs. Rather, these findings may help explain the role anhedonia has as a transdiagnostic correlate or bridge between various types of psychopathologies (e.g., Conway et al., 2019; de la Torre-Luque & Essau., 2019; Dolan et al., 2022).
Despite evidence for convergent and discriminant validity, the DARS did not demonstrate consistent concurrent validity in this sample. Concurrent validity was assessed by examining the association of the DARS with the CDI, CES-DC, and PANAS. The majority of these associations were small, though there could be several explanations for our findings. First, anhedonia in adolescence can precede other depressive symptoms (e.g., Kouros et al., 2016). As a result, the concurrent association between anhedonia and depression might be weaker in adolescents than in adults, particularly in a general population sample. Future research should assess if the DARS demonstrates better predictive than concurrent validity with depression. Second, adolescent anhedonia may be composed of unique experiences such as chronic boredom (Watson et al., 2020), and as the DARS was developed for adults, it may not capture potentially unique adolescent experiences and, thus, fail to demonstrate strong associations with established markers of concurrent validity. Third, depression can cause difficulties with encoding past pleasurable experiences to memory (Heshmati & Russo, 2015; Jankowski et al., 2018), and while more emotionally salient experiences are better encoded and more easily accessible (Heshmati & Russo, 2015), the alternative is also true. Specifically, research into reward circuitry suggests that the dampened emotions or the loss of salient positive emotional experiences (as observed in depression and anhedonia; Jankowski et al., 2018; Watson et al., 2020), known as the positive blockade (Disner et al., 2011), diminishes reward experiences and weakens reward learning (Der-Avakian & Markou, 2012; Heshmati & Russo, 2015). This is to say that, for those with depression in our sample, these memory encoding difficulties may have impacted our sample’s ability to provide relevant pleasurable example activities for the DARS, possibly explaining the inconsistent convergent validity. In a similar vein, individuals with depression demonstrate poorer retrieval of positive autobiographical memories (as reviewed by LeMoult & Gotlib, 2019), and when individuals with depression are recounting positive memories, they report lower ratings of happiness (Söderlund et al., 2014). These difficulties with recalling and reporting past levels of enjoyment may suggest that, while anhedonia impacts the encoding of memories, it might also impact the recall of past pleasurable experiences and the extent to which the experiences are remembered as enjoyable. To this end, researchers are increasingly documenting that anhedonia can influence an additional temporal orientation: accurately recalling past experiences and levels of pleasure (i.e., recall anhedonia; Chentsova-Dutton & Hanley, 2010; Zareian et al., in prep). This possibility suggests that the need to recall specific pleasurable activities and events on the DARS may hinder accurate assessment of anhedonia when clinical levels of anhedonic or depressive symptoms are present in adolescents.
It is also important to note that, although the DARS measures various dimensions of anhedonia (e.g., consummatory, anticipatory), it does not allow differentiation between these dimensions. Instead, its subscales focus on the various domains adolescent anhedonia might disrupt (e.g., physical, social, sensory; Watson et al., 2020). As a result, the DARS does not allow researchers to assess the unique contribution each dimension of anhedonia makes to predicting a criterion (e.g., depression, reward processing). This is surprising given that measuring each dimension of anhedonia’s unique role in predicting outcomes may prove critical. Indeed, researchers have documented that each dimension can have a unique association with an outcome of interest (Buck & Lysaker, 2013; Gard et al., 2007). Shedrell and colleagues (2012), for example, found that anticipatory, but not consummatory, anhedonia predicted reductions in effort and motivation. Thus, future measures of anhedonia should assess anhedonia in all domains and allow subscale scores that measure each dimension of anhedonia.
There were several limitations associated with this study. First, our sample was predominantly girls and, as such, our results may be somewhat limited in their generalizability. Although we are unaware of gender differences in the experience of anhedonia, previous research has shown that male adolescents with depression are more likely to report anhedonia than their female counterparts (Bennett et al., 2005; Bennik et al., 2014). Therefore, future research should assess the generalizability of our data by recruiting a sample with more representations of boys and non-binary individuals. Second, although we recruited a large sample of adolescents, our sample is a convenience community sample of adolescents. Therefore future researchers should assess the DARS ability to distinguish between adolescents with and without clinical levels of psychopathology by recruiting clinical samples. An additional limitation was that our study relied exclusively on self-report measures. Future research should use multi-method approaches, including cognitive tasks or functional imaging to better establish the overlap between the DARS and objective measures of reward processing.
Overall, this study aimed to examine the psychometric properties of the DARS as a potential option for measuring anhedonia in English-speaking adolescents. A rigorous self-report measure appropriate for adolescents would allow researchers and clinicians to better detect the existence and assess the severity of adolescent anhedonia, provide a clear definition of this hedonic deficit, and facilitate further research and understanding of this pervasive construct (Watson et al., 2020). Although the DARS showed good convergent and discriminant validity in our sample, its sub-optimal concurrent validity raises concern and suggests additional research is needed to determine if the DARS detects features unique to the adolescent experience. Future researchers may seek to develop additional measures incorporating this adolescent-specific experience and address the multidimensionality of anhedonia, especially the temporal orientations of these deficits (e.g., Gard et al., 2006). Additionally, neuroscientific research on reward processing and memory, as well as qualitative research into the adolescent experience, suggest a dimension of anhedonia may be difficulty recalling past pleasurable experiences (i.e., recall anhedonia), possibly due to dampened emotional responses leading to poorer reward learning and memory retrieval (Der-Avakian & Markou, 2012; Heshmati & Russo, 2015; Watson et al., 2020). Researchers should consider recall problems, especially of past positive memories, as an essential component of anhedonia given the overlapping reward circuitry (Heshmati & Russo, 2015) and the demonstrated importance and impact of this temporal deficit in past quantitative and qualitative research (Chentsova-Dutton & Hanley, 2010; Watson et al., 2020). Finally, researchers should assess how these temporal dimensions of anhedonia uniquely contribute to the more severe, frequent, and treatment-resistant psychopathology associated with anhedonia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Psi Chi.