
Abstract
There have been few studies on the bidirectional interaction between the parental and the offspring’s psychological symptoms. It is important to fill in this lacuna to understand the development and vicious cycles of psychological symptoms in the familial context. The objective was to study the bidirectional relationships between parental anxiety, early adolescents’ internalizing symptoms, and peer victimization and aggression. 288 early adolescents (54% girls) between 9 and 15 years (
Introduction
Children of parents who present with internalizing symptoms are at greater risk of developing internalizing and externalizing symptoms during childhood, early adolescence, and adolescence (Kim et al., 2009). The terms “internalizing symptoms” and “externalizing symptoms” have been widely used to refer to a group of symptoms related to emotional symptoms and behavioral problems, respectively (Achembach, 2016). Among others, internalizing symptoms include psychosomatic symptoms, anxiety symptoms, and depression symptoms. Externalizing symptoms include aggressiveness, impulsiveness, and disruptive behaviors, which are commonly expressed by both the victims and perpetrators of bullying (Lebrun-Harris et al., 2019).
Based on the intergenerational transmission of internalizing and externalizing symptoms (Capaldi et al., 2012), most studies have focused on studying how parental internalizing and externalizing symptoms affect their offspring’s symptoms, concluding that parents with symptoms are at an increased risk of transmitting such symptoms to their offspring (Goodman, 2020; Kim et al., 2009). However, in recent years, there has been growing interest in analyzing how offspring who exhibit internalizing and externalizing symptoms affect parental internalizing symptoms. For instance, it has been reported that internalizing and externalizing symptoms in offspring precede parental internalizing symptoms (McAdams et al., 2015). Despite the fact that parents and offspring affect one another, few studies have provided information on the bidirectionality between the parental and the offspring’s symptoms. Therefore, the main objective of this study was to analyze the bidirectional relationships between parental internalizing symptoms and their offspring’s internalizing and externalizing symptoms. Specifically, this study focused on the bidirectional relationships between parental anxiety, and early adolescents’ internalizing symptoms, peer victimization, and aggression.
Intergenerational Transmission: Parents to Early Adolescents
Most studies based on the intergenerational transmission of psychopathology have focused on analyzing the relationship between parental psychological symptoms and their offspring’s, assuming the multifinality principle (Cicchetti & Rogosch, 1996). This principle suggests that parental internalizing and externalizing symptoms are not only domain-specifically associated with their offspring’s symptoms (i.e., parental internalizing symptoms with their offspring’s internalizing symptoms), but are also generically related (i.e., parental internalizing symptoms with their offspring’s externalizing symptoms) (Schulz et al., 2021). For example, cross-sectional studies have observed that parental anxiety is associated with both internalizing children’s symptoms and externalizing symptoms (Gamliel et al., 2018).
Longitudinal studies attempting to analyze the transmission of parental psychological symptoms to their offspring have produced divergent results, which makes it difficult to draw clear conclusions regarding whether parental symptoms precede their offspring’s. Studies conducted with adolescents and parents have concluded that internalizing symptoms in adolescents are preceded by maternal depression (Côté et al., 2018; Vismara et al., 2022) and anxiety symptoms (Goodman et al., 2011; Johnco, 2021). In addition, paternal depression symptoms preceded their adolescent’s externalizing symptoms (Reeb et al., 2015; Vismara et al., 2022). Other studies came to the opposite conclusion, finding that parental anxiety and depression symptoms did not predict adolescents’ internalizing and externalizing symptoms (Schulz et al., 2021). Anxiety symptoms are rarely explored compared to depression symptoms; therefore, the previous literature highlighted the need to explore parental anxiety (Gamliel et al., 2018).
At the same time, little is known about whether parental anxiety may be related to peer victimization and aggression. It has been demonstrated that aggressive parental behavior and depression predict peer victimization and aggression in adolescents (Davis et al., 2020). In addition, a longitudinal study concluded that parental stress is a predictor of peer victimization and perpetration among adolescents (Zhang et al., 2021). However, further research is needed to determine the relationship between parental anxiety and peer victimization and aggression among early adolescents (Nocentini et al., 2019). In fact, the highest peaks of peer victimization and aggression occur in early adolescence (Rettew & Pawlowski, 2016), so it is important to analyze the risk factors, such as parental anxiety symptoms, that trigger these bullying behaviors (Davis et al., 2020).
Transactional Theory of Development: Early Adolescents to Parents
As mentioned above, there has been a trend in the literature toward studying the effect of an offspring’s symptoms on their parents based on the transactional theory of development (Sameroff, 2009). This theory emphasizes that because the environment surrounding children affects their development, children, at the same time, also produce a change in their environment. Thus, it is understood that because parental internalizing symptoms affect their offspring’s internalizing and externalizing symptoms, it is also the case that the offspring’s symptoms impact parental symptoms (Hou et al., 2020). For instance, it was found that adolescents’ internalizing symptoms predicted maternal anxiety (Schulz et al., 2021) and depression symptoms (Hou et al., 2020).
Bidirectional Relationships between Parental Anxiety and Symptoms among Early Adolescents
Taking into account this assumption, some studies have analyzed bidirectional relationships between the parental and the offspring’s internalizing and/or externalizing symptoms, but inconclusive results have been found in this regard. On the one hand, in the study conducted by Schulz et al. (2021), in which a six-wave longitudinal design was implemented, no bidirectional relationships were found between parental anxiety and depression symptoms and their offspring’s internalizing and externalizing symptoms. In other studies, bidirectional relationships were found between maternal anxiety symptoms and their offspring’s internalizing symptoms (Hughes & Gullone, 2010), and between maternal depression symptoms and their offspring’s internalizing symptoms (Hou et al., 2020; Johnco et al., 2021). Regarding the relationship between parental anxiety symptoms and peer victimization and aggression, to the best of our knowledge, no bidirectional studies have yet been carried out.
Previous studies have indicated the importance of analyzing the bidirectionality between parental symptoms and early adolescents’ symptoms because of its impact on the individual and on familial functioning (Johnco et al., 2021). This bidirectionality is compatible with a vicious circle in which the offspring’s and the parental symptoms increase reciprocally (Schulz et al., 2021). Thus, a mild symptom could lead to psychopathologies, such as anxiety, depression, or conduct disorders, in both offspring and parents (Hou et al., 2020). Therefore, worsening parental and offspring symptoms could affect family functioning (Pérez et al., 2018; Wiegand-Grefe et al., 2019).
Most of the studies did not include a multi-informant design in their method (for exceptions, see Hughes & Gullone, 2010; Reeb et al., 2015; Schulz et al., 2021). This kind of design helps in gaining a more representative vision, one in which the mother’s, father’s, and offspring’s perspectives are included. Additionally, in those studies in which parent – child dyads have been analyzed, a very high percentage of the parental figure (around 95%) was represented by mothers (Côté et al., 2018; Goodman et al., 2011; Johnco et al., 2021). Studies that include balanced samples in terms of mothers and fathers are scarce. For example, in Schulz et al.’s (2021) study, the sample was composed of 53% mothers and 47% fathers, and in Hughes & Gullone's (2010) study, 58% of the sample were mothers and 42% fathers.
The unbalanced mother–father samples make it difficult to analyze whether there are differences between girls and boys in the development of internalizing and externalizing symptoms based on the symptoms presented by their mothers and fathers. Some longitudinal studies have reported no gender differences between adolescents in terms of the relationship between parental internalizing symptoms and internalizing symptoms among adolescents (Hou et al., 2020; Reeb et al., 2015). Nonetheless, Schulz et al. (2021) found small gender differences in their study. A bidirectional relationship was found between maternal internalizing symptoms and adolescent girls’ internalizing symptoms, and maternal internalizing symptoms were predicted by adolescent boys’ internalizing symptoms. No gender differences were detected related to paternal internalizing symptoms. Although longitudinal studies are inconclusive, some authors have suggested that maternal internalizing symptoms contributed to both girls’ and boys’ internalizing symptoms and that paternal internalizing symptoms contributed to boys’ internalizing (Reeb et al., 2015) and externalizing symptoms (Goodman, 2011).
On the other hand, a large number of publications have focused on the early stages of life (early and middle childhood), demonstrating the impact that parental symptoms have on the psycho-emotional development of their babies (Filed, 2018; Parsons et al., 2012). However, concurrently, two meta-analyses (Möller et al., 2016; Van der Bruggen et al., 2008) have suggested that the effect of parental symptoms on children’s symptoms intensifies as age increases; thus, this effect is more visible in early adolescence and adolescence. This may be due to the fact that older adolescents have been exposed to their parental symptoms for longer; thus, the effect of this exposure on adolescents’ symptoms is stronger compared to children’s. However, little is known about the role of age in this regard. Hence, these meta-analyses highlighted the importance of continuing to advance the study of these effects during the transition from childhood to adolescence, paying special attention to early adolescence, which refers to the period between 10 and 14 years of age (Blum et al., 2014).
The Present Study
Considering the aforementioned points, the present study aimed to evaluate the bidirectional relationships between parental anxiety symptoms and early adolescents’ internalizing symptoms, peer victimization, and aggression through a multi-informant (mother, father, and child) bidirectional design comprised of two waves. In this study, early adolescents were included because previous investigations have highlighted the need to understand the impact of this reciprocal effect between parents and offspring in the transition from childhood to adolescence (Möller et al., 2016).
Thus, through this study, based on what transactional theory indicates (Sameroff, 2009), it was expected that we would find bidirectional relationships between parental anxiety symptoms and their offspring’s internalizing symptoms, peer victimization, and aggression. Furthermore, differences between mothers and fathers were analyzed with regard to these bidirectional relationships, resulting in two hypothesized models: one related to maternal anxiety and the other to paternal anxiety. In this sense, no hypothesis was put forward, because there was not much evidence regarding the differences that can be expected between mothers and fathers.
Finally, whether gender and age moderated the above-mentioned bidirectional relationships was examined. To achieve this aim, multigroup comparisons were conducted to evaluate whether the hypothesized models were invariant across gender and age groups (younger early adolescents ranged between 9 and 12 years, and older early adolescents between 13 and 15 years). For gender differences, it was hypothesized that girls’ and boys’ internalizing and externalizing symptoms would predict both maternal and paternal anxiety. In addition, we hypothesized that maternal anxiety would predict girls’ but not boys’ internalizing symptoms, and that paternal anxiety would predict boys’ but not girls’ externalizing symptoms. Regarding age-group differences, it was expected that the models would differ due to the fact that the reciprocal effect between parents and offspring intensifies over time. Therefore, it was hypothesized that this effect would be more intense for older early adolescents than for younger ones.
Method
Participants
Of the initial sample, 288 adolescents and at least one parent participated in both waves. Specifically, in 221 of the 288 cases, both the mother and the father answered the self-report questionnaires, in 58 cases only the mother did, and in 9 cases only the father did. The sample for Wave 1 (W1) was recruited in May 2021, and that for Wave 2 (W2) was recruited in November 2021. The early adolescents were aged between 9 and 15 (
Measures
Peer Aggression and Victimization
Peer aggression and victimization were measured by the Spanish adaptation (Ortega-Ruiz et al., 2016) of the European Bullying Intervention Project Questionnaire (Brighi et al., 2012). This questionnaire is composed of 14 items, of which seven referred to peer victimization and the remaining seven referred to peer aggression. Participants indicated how often they experienced these bullying situations, with answers ranging from 0 (never) to 4 (always). Recent studies have reported good internal consistency for both the victimization (α = .79) and perpetration (α = .79) subscales (Pichel et al., 2021). The Cronbach’s alphas for the current sample were acceptable as well:
Internalizing Symptoms among Early Adolescents
The Spanish adaptation (Ortuño-Sierra et al., 2015) of the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) was applied to measure internalizing symptoms. This questionnaire consists of 25 items used to assess five factors: hyperactivity/inattention, emotional symptoms, conduct problems, peer relationship problems, and prosocial behavior. For the present study only, the emotional symptoms subscale was used to represent internalizing symptoms. The emotional symptoms items (e.g., “Many worries or often seems worried”; “Often unhappy, depressed or tearful”; “Nervous in new situations, easily loses confidence”) were answered through a three-point Likert scale (0 = not true, 1 = somewhat true, 2 = absolutely true). Regarding the Spanish version of the SDQ, previous studies have shown good psychometric properties (Rodríguez-Hernández, 2014). In the present study, the Cronbach alpha of the emotional symptoms’ subscale was .73 in both W1 and W2.
Parental Anxiety Symptoms
To measure parental anxiety symptoms, the Spanish adaptation (Daza et al., 2002) of the Depression, Anxiety, and Stress Scale (DASS-21; Lovibond & Lovibond, 1995) was used. The scale is composed of 21 items, with seven for each subscale (anxiety, stress, and depression symptoms), and answered using a four-point scale from 0 to 3: 0 (did not apply to me at all), 1 (applied to me to some degree, or some of the time), 2 (applied to me to a considerable degree or a good part of time), and 3 (applied to me very much or most of the time). For this study, only the anxiety subscale was included. In previous studies, a high reliability on the part of this scale has been observed (Ruíz et al., 2017). Similarly, in the present study, the Cronbach alpha values for each subscale were acceptable in both waves for mothers (
Procedure
Seven out of eleven Biscayan schools, which were randomly selected for this study, agreed to participate. All fourth to eighth grade classes in those seven schools participated in the study. After receiving an information letter describing the main objectives of the study, headteachers sent an informed consent form to parents, and 98% of them allowed early adolescents to participate.
A group of psychologists went to the schools on two occasions to conduct both waves (W1 and W2), which were separated by 6 months. Once in the classrooms, early adolescents were informed about the study, emphasizing that their participation was voluntary, that their responses would be kept confidential, and that they were allowed to stop participating at any time during the process. They spent around 30 minutes in completing the questionnaire individually. Once this was completed, each student took home a letter, along with two questionnaires, one for their mother and one for their father. In order to match the answers of the students with those of their parents, a numerical code was used. After 6 months, the same sample recruitment procedure was conducted, and another numerical code was used to match answers from W1 and W2. This study was approved by the ethics committee of [masked for review] University.
Data Analysis Plan
Firstly, IBM SPSS 27 was used to analyze the descriptive data and Pearson correlations among study variables. Secondly, bidirectional relationships between study variables were tested by using LISREL 10.20, conducting one hypothesized model with maternal anxiety and another with paternal anxiety. The models included cross-sectional paths between variables belonging to the same wave, autoregressive paths from the study variables in W1 to the same variables in W2, and bidirectional paths from each study variable in W1 to each study variable in W2. The goodness of the model fit was evaluated with the root mean square error of approximation (RMSEA), the standardized root mean square residual (SRMR), the comparative fit index (CFI), and the nonnormative fit index (NNFI). Following Little’s (2013) recommendation, a good fit is indicated by RMSEA and SRMR values lower than .08 and CFI and NNFI values higher than .90.
From the dataset, only 3% of the values were missing from the hypothesized model with maternal anxiety, and 1.2% of the values were missing from the hypothesized model with paternal anxiety. Little’s missing completely at random (MCAR) test was nonsignificant in the hypothesized model with maternal anxiety (χ2 = 20.08, p = .86) and the hypothesized model with paternal anxiety (χ2 = 13.79, p = .88). Finally, it was determined whether the hypothesis models were equivalent across gender (girls and boys) and age (younger and older early adolescents) via multigroup analysis.
Results
Descriptive Data
Means, Standard Deviations, and Correlation Coefficients between Study Variables.
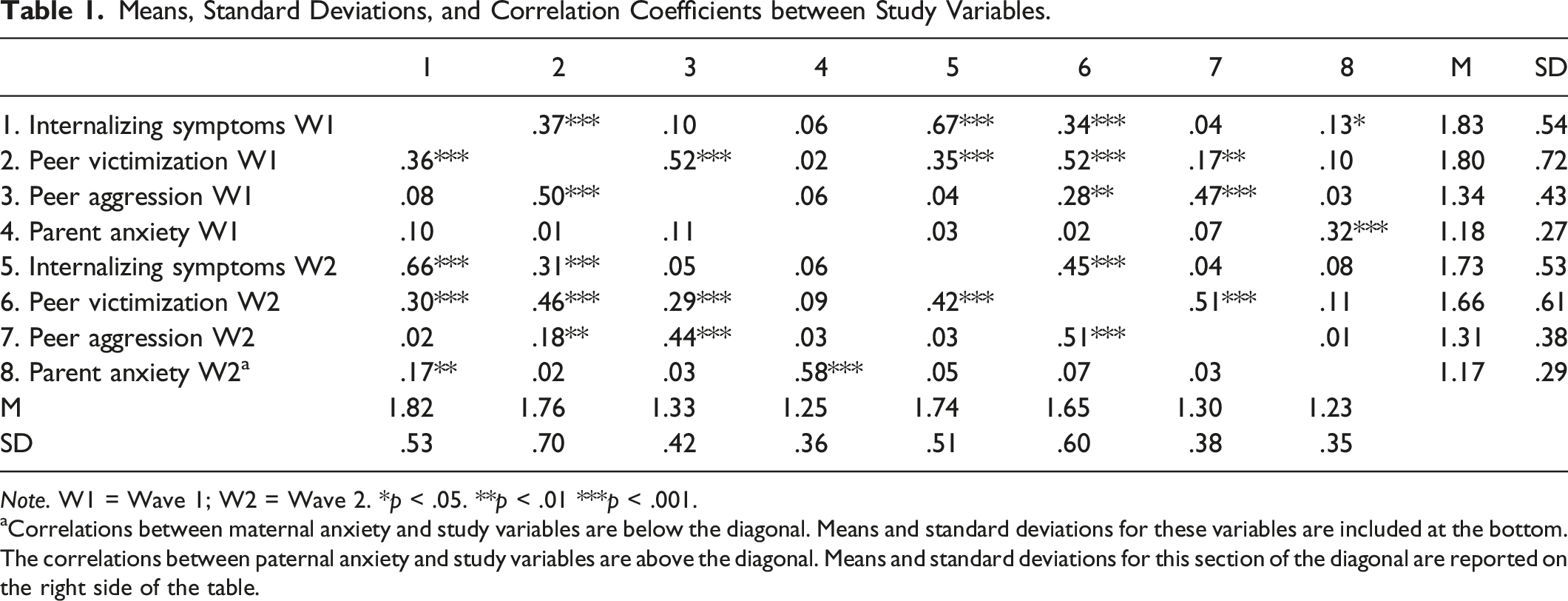
Note. W1 = Wave 1; W2 = Wave 2. *p < .05. **p < .01 ***p < .001.
aCorrelations between maternal anxiety and study variables are below the diagonal. Means and standard deviations for these variables are included at the bottom. The correlations between paternal anxiety and study variables are above the diagonal. Means and standard deviations for this section of the diagonal are reported on the right side of the table.
Bidirectional Relationships between Study Variables
Via path analysis, the bidirectional relationships between the study variables were estimated, differentiating between two hypothesized models: one including maternal anxiety and the other one including paternal anxiety.
The hypothesized model with maternal anxiety obtained excellent fit indexes, χ2 (4, n = 271) = 1.07, p = .899, RMSEA = .00 (90% Confidence Interval [0.00, 0.04]), CFI = 1, NNFI = 1, SRMR = .0007. The autoregressive paths for each variable were significant, indicating the stability of study variables over 6 months. Moreover, early adolescents’ internalizing symptoms in W1 predicted peer victimization and maternal anxiety in W2. A more parsimonious model was estimated in which non-significant paths were excluded. This new model also obtained excellent fit indexes, χ2 (14, n = 271) = 11.50, p = .646, RMSEA = .00 (90% Confidence Interval [0.00, 0.05]), CFI = 1, NNFI = 1, SRMR = .03. In Figure 1, the paths of this new model were presented. Hypothesized model with maternal anxiety. Note. W1 = wave 1; W2 = wave 2. **p < .01. ***p < .001.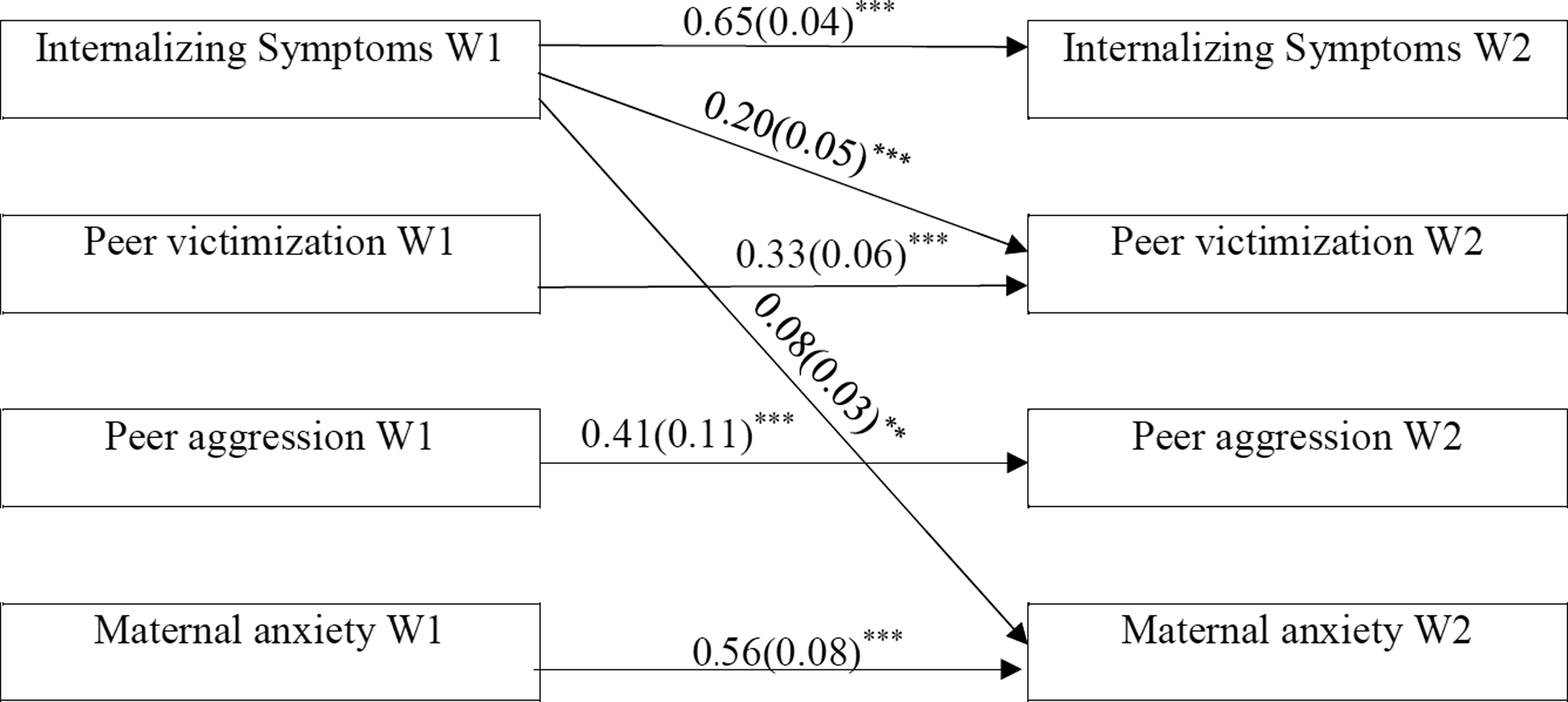
Regarding the hypothesized model with paternal anxiety, excellent fit indexes were also reported, χ2 (6, n = 227) = 3.11, p = .796, RMSEA = .00 (90% Confidence Interval [0.00, 0.05]), CFI = 1, NNFI = 1, SRMR = .016. All the autoregressive paths were significant, and also, internalizing symptoms in W1 predicted peer victimization in W2. Including only the significant paths, a more parsimonious model was estimated, which also showed excellent fit indexes (Figure 2), χ2 (10, n = 227) = 10.02, p = .439, RMSEA = .002 (90% Confidence Interval [0.00, 0.07]), CFI = 1, NNFI = 1, SRMR = .038. Hypothesized model with paternal anxiety. Note. W1 = wave 1; W2 = wave 2. *p < .05. ***p < .001.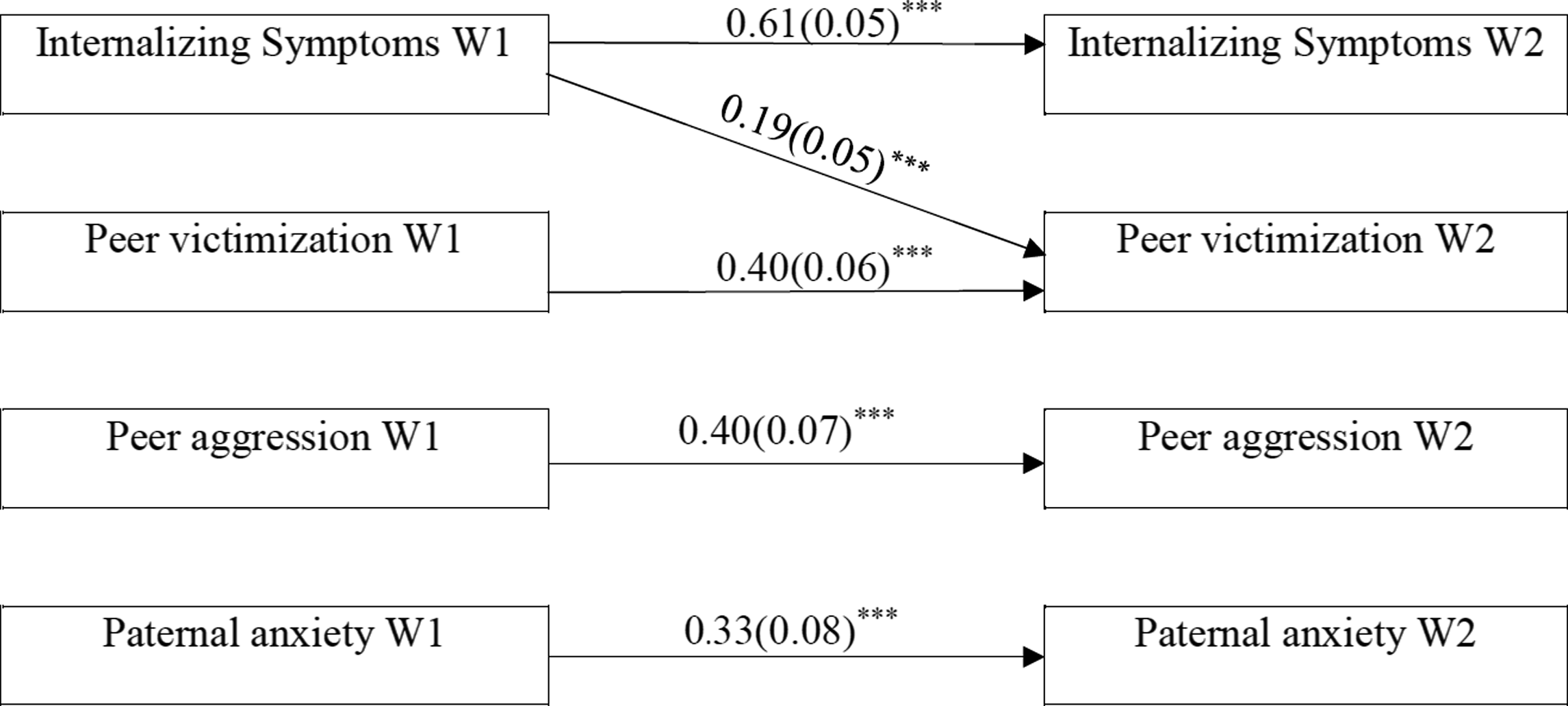
Gender and Age Differences in Early Adolescents
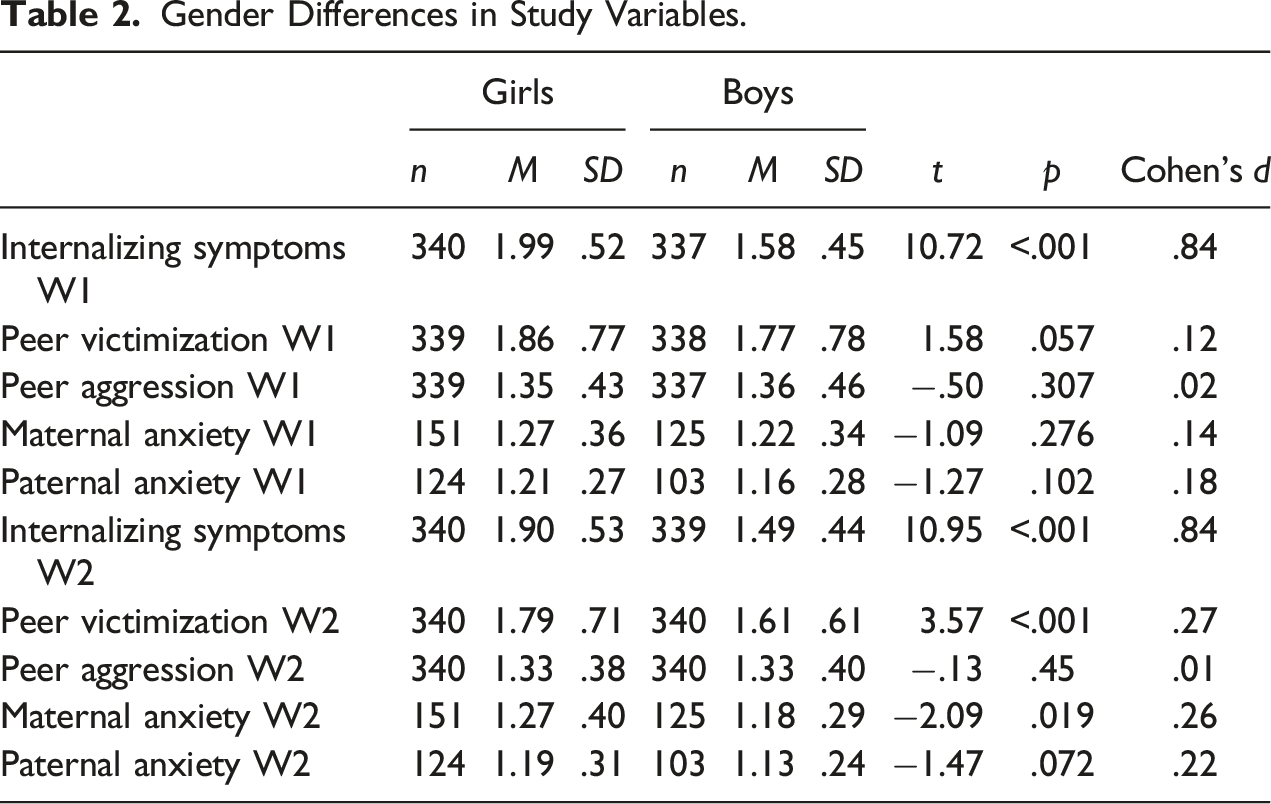
Gender Differences in Study Variables.
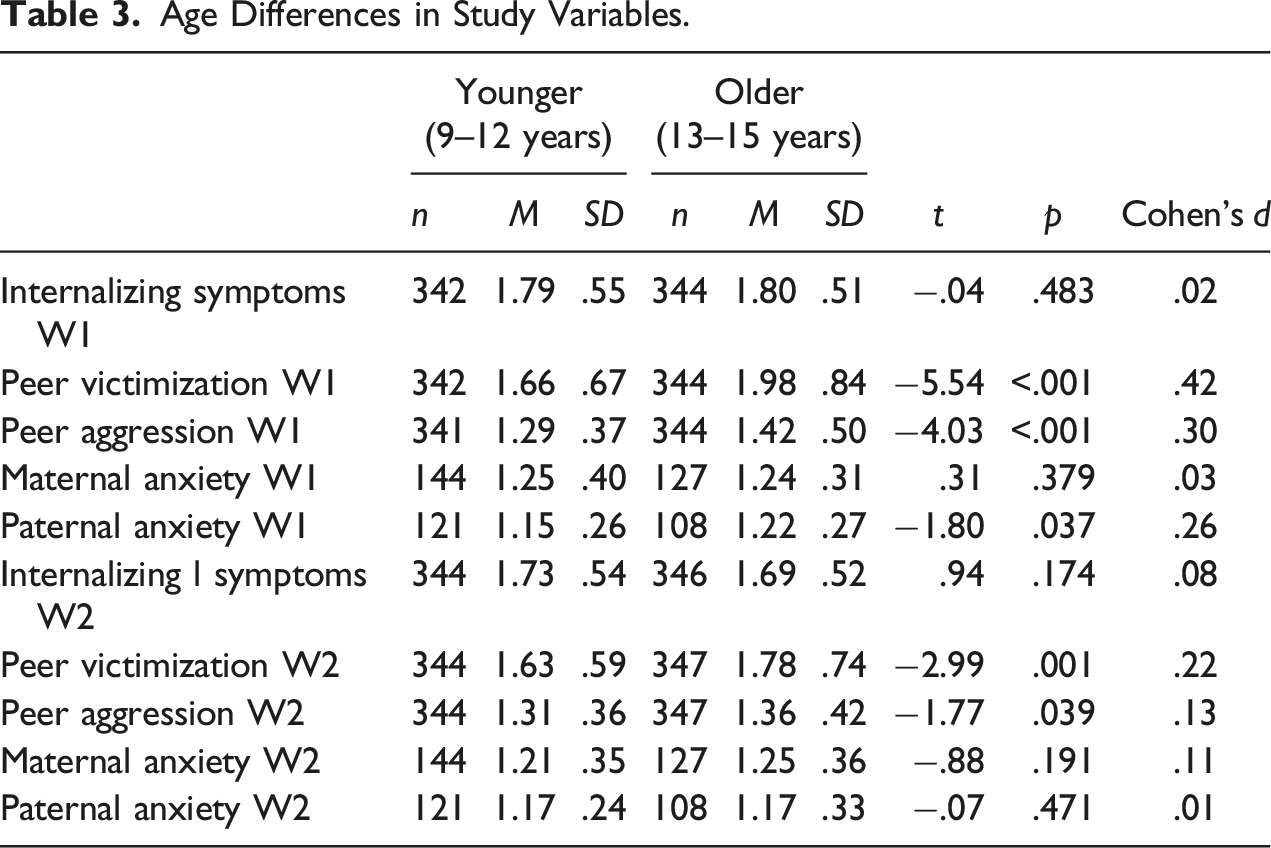
Age Differences in Study Variables.
Multigroup Analysis Across Gender.
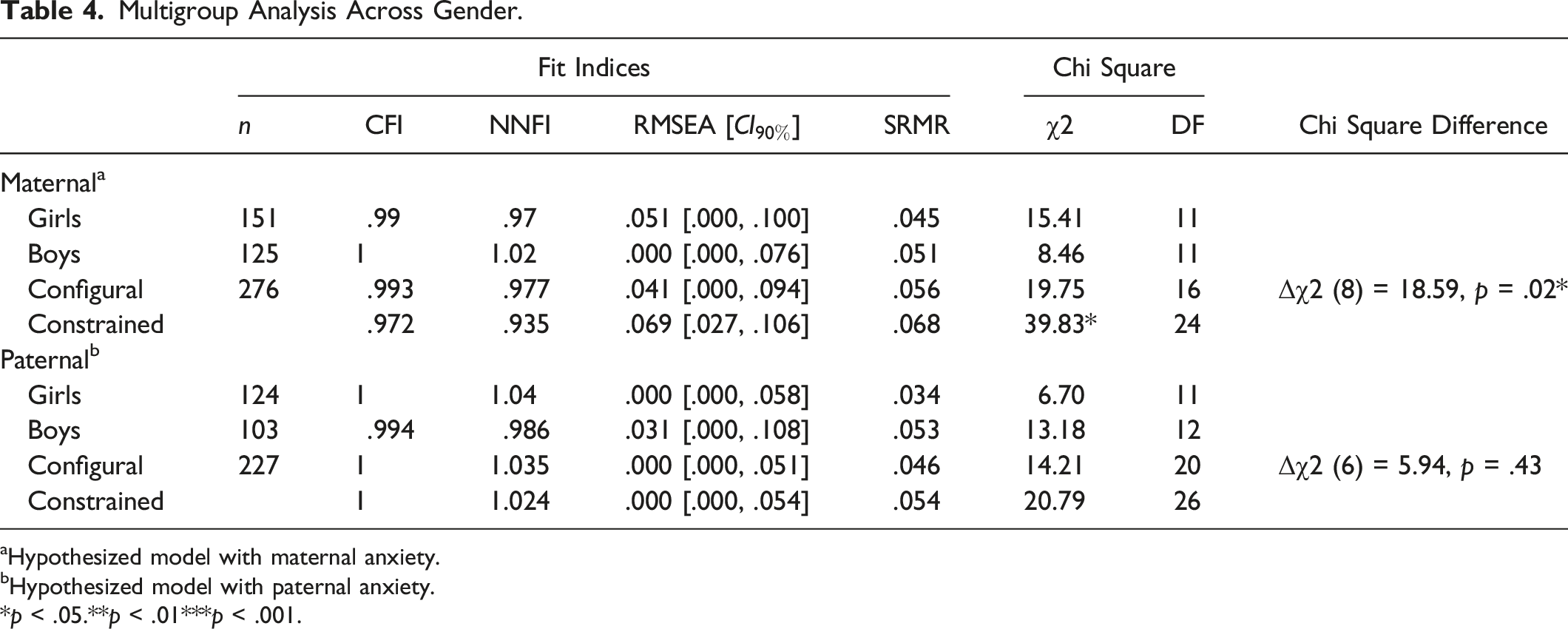
aHypothesized model with maternal anxiety.
bHypothesized model with paternal anxiety.
*p < .05.**p < .01***p < .001.
Multigroup Analysis Across Age.
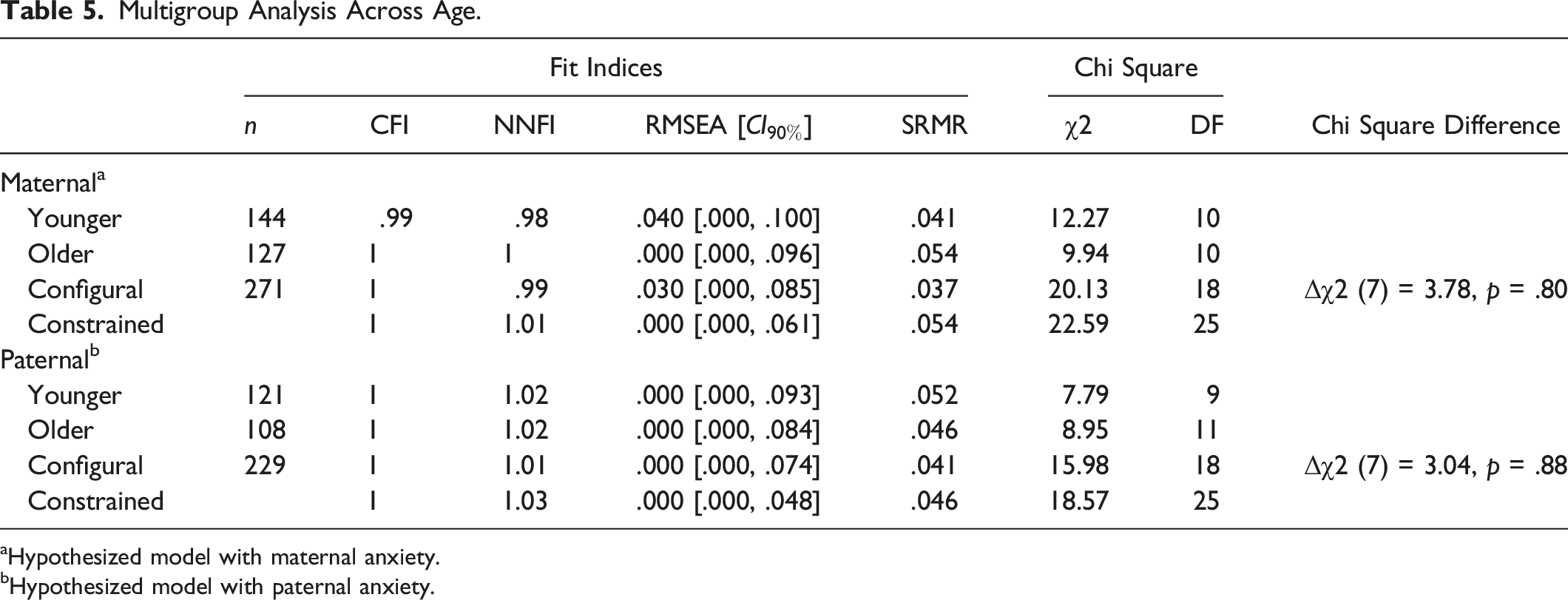
aHypothesized model with maternal anxiety.
bHypothesized model with paternal anxiety.
Discussion
The main objective of this study was to analyze the bidirectional relationships between parental anxiety symptoms and their offspring’s internalizing symptoms, peer victimization, and aggression. Unexpectedly, no bidirectional relationships were found between these variables. However, some interesting findings emerged when analyzing the relationship between parental anxiety symptoms and their children’s internalizing symptoms, peer victimization, and aggression.
First, regarding the correlations between the study variables, early adolescents’ internalizing symptoms in W1 were not associated with parental anxiety in W1, but were related to parental anxiety in W2. Therefore, it seems that parental anxiety symptoms do not co-occur with early adolescents’ internalizing symptoms, but are preceded by internalizing symptoms in early adolescents. Indeed, this predictive association was reflected in the hypothetical model with mothers, in which early adolescents’ internalizing symptoms significantly predicted maternal anxiety.
At the same time, although the correlation between internalizing symptoms and paternal anxiety was significant, the predictive models indicated that early adolescents’ internalizing symptoms did not precede paternal anxiety, concluding that mothers may be at a higher risk than fathers of developing anxiety symptoms after their offspring have shown internalizing symptoms. This may occur due to the fact that mothers continue to be the principal day-to-day caregivers for their children (Ahmadzadeh et al., 2019). Therefore, mothers may be more exposed to their offspring’s internalizing symptoms than fathers, and subsequently, their anxiety may increase because these mothers are worried about their children (Hudson et al., 2008). In turn, other authors have suggested that there may be other intrapersonal and interpersonal variables that act as risk factors or protective factors in this relationship (Weijers et al., 2018). It has been shown that authoritative parenting works as a protective factor for bullying perpetration, victimization, and depression, whereas authoritarian and permissive parenting styles are risk factors for these outcomes (Luk et al., 2016). Moreover, children with insecure attachments are at the greatest risk of developing internalizing symptoms and difficulties in self-regulation and relating to their peers (Kerns & Brumariu, 2014). In addition, mindful parenting has been related to fewer parental internalizing symptoms (Moreira & Canavarro, 2018), and it has been shown to contribute to building healthier parent – child relationships and, consequently, reducing the risk of the development of externalizing and internalizing symptoms in children (Parent, 2021). Hence, future research should evaluate whether factors such as those described contribute to these differences in the development of maternal and paternal anxiety related to the internalizing symptoms among early adolescents.
Regarding the relationships between peer victimization and aggression and parental anxiety, they were not associated either transversally or longitudinally. Despite the fact that the literature (Schulz et al., 2021) indicates that the relationship between parental symptoms and their offspring’s follows the multifinality principle (Cicchetti & Rogosch, 1996), in this study, parental internalizing symptoms (maternal anxiety) were only domain-specifically associated with early adolescents’ internalizing symptoms. Future studies could therefore include parental externalizing symptoms in the hypothesized models to understand whether there is any association between parental externalizing symptoms and peer victimization and aggression.
Moreover, it is noteworthy that victimization was significantly associated with both internalizing symptoms and aggression toward peers. Likewise, in the hypothesized models, peer victimization was preceded by internalizing symptoms. As argued by other authors (Forbes et al., 2019), internalizing symptoms and peer victimization do not merely co-occur; rather, each produces a negative effect on the other. Although aggression toward peers has not shown any bidirectional relationships, the relationship between internalizing symptoms, victimization, and aggression toward peers through cascades (Masten & Cicchetti, 2010) or mediation/moderation analyses could be an interesting subject for future research because there seems to be a relationship between these variables (Christina et al., 2021).
The hypothesized model with maternal anxiety was only invariant between girls and boys in one of the paths, which indicated that victimization predicts aggression more strongly in girls than in boys. This difference was significant, but had a small effect size, which is in alignment with the results of other authors (Busch et al., 2015). In relation to maternal and paternal anxiety, no gender differences were found. These results were consistent with other longitudinal studies (Hou et al., 2020; Reeb et al., 2015), indicating that there were no gender differences in the hypothesized models. However, in the current study, separate models were run for mothers and fathers. Therefore, further research is needed to test gender differences using multigroup analysis, including both mothers and fathers in the same model.
In addition, the models were invariant between younger and older early adolescents. Nevertheless, age-group differences were detected with regard to peer victimization and aggression. Younger early adolescents scored higher regarding peer victimization and aggression than older early adolescents. These results partially agree with those obtained for Spanish populations in previous studies, which found that the peak of peer victimization occurs around 12 years of age (Pichel et al., 2021). However, in these studies, it was also found that peer aggression increases after the age of 12–13 years (Garaigordobil, 2015), which does not coincide with the results obtained in the present study. Likewise, in agreement with previous meta-analyses (Möller et al., 2016; Van der Bruggen et al., 2008), it was also found that fathers with older early adolescents scored higher on anxiety symptoms than those with younger early adolescents.
Limitations and Future Studies
This study has certain limitations. The most important limitation was the size of the subsamples that were used for invariance testing. As for the present study, data from various informants were combined, and the cases eliminated from the study were considerable in number. The small sample size may have limited the power to find significant relationships between the study variables. Consequently, future studies should test the proposed models in larger, multi-informant samples. Likewise, regarding the proposed models, it would be convenient to include a third wave so as to obtain a more complete perspective on this phenomenon, through which the cascade effect between the study variables and/or the mediating or moderating effect of other variables could be analyzed. In addition, early adolescents responded to questions about peer victimization and aggression, which could lead to high covariance due to shared method variance. Thus, future studies should consider using different methods to measure peer victimization and aggression. Finally, it would be very interesting to assess whether these models could be applied to other cultures and ethnic groups.
Strengths and Clinical Implications
Despite these limitations, the present study also has several strengths and clinical implications. First, a bidirectional design was included, which increased the understanding of not only the reciprocity of the study variables, but also their evolution over 6 months. Furthermore, as mentioned above, there are few longitudinal studies that have analyzed the relationship between parental psychological symptoms and early adolescents’ symptoms, so this study provides new evidence on these relationships. This could bring a new perspective to family interventions by understanding that the psychological symptoms presenting in early adolescents and/or in their parents should also be analyzed by considering the symptoms reported by the other party. Second, this study is one of the few that has been able to include very similar groups of mothers and fathers in its sample, whereas most previous studies have included much larger samples of mothers than fathers. This allows our study to respond to the gap detected in the literature regarding the mother – father imbalance in the samples. Studies with balanced samples of mothers and fathers may be valuable in providing a more representative view of the differences between mothers and fathers regarding issues related to the family context, such as the development of psychological symptoms in parents and offspring. Likewise, the models provided in the present study showed differences between mothers and fathers. For this reason, the present study leads to a new study approach in which the parallel evaluation of the influence between early adolescents and their mothers and fathers is highlighted. Finally, this study advocates a future line of research in which the evolution of maternal, paternal, and early adolescents’ psychological symptoms should be analyzed from a more complex perspective, one in which the family context and the relational dynamics that can be derived from these relationships can be considered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science, Innovation and Universities of the Spanish Government (Ref. PID2019-106162GA-I00 and Ref. PRE2020-094016) and the Basque Government (IT1532-22).
Ethics Approval
The Ethics Committee of the University of Deusto approved this study.
Consent
Informed consent was obtained from all parents, and assent was obtained from all adolescent participants.