
Abstract
We examined the impact of Routines-Based Interview (RBI) training on the quality of Individualized Family Service Plans (IFSPs), comparing the IFSPs of providers trained to fidelity in RBI with those who had not received RBI training. We employed a quasi-experimental design, analyzing 163 IFSPs across six Local Education Agencies (LEAs) in one mid-Atlantic state, focusing on family engagement, outcome specificity, and compliance with recommended practices. Results indicate that IFSPs developed with families by RBI-trained providers scored statistically significantly higher in areas such as family resources, priorities, and concerns, as well as in the quality of child outcomes. These findings highlight the critical role of fidelity in RBI implementation and underscore the need for expanded training to ensure consistent improvements across settings. Implications for practice include using the RBI process to strengthen caregiver engagement in the IFSP process, develop meaningful and measurable outcomes, and guide professional development.
The Individuals with Disabilities Education Act (IDEA) ensures that children with disabilities receive appropriate early intervention, special education, and related services. Part C of the law outlines the provision of early intervention services to eligible infants and toddlers with developmental delays or disabilities from birth to age three. Services provided under Part C aim to enhance children’s development during their critical early years, reduce the future need for special education, and improve long-term outcomes through building collaborative partnerships with families (IDEA, 2004).
One of the most critical elements to accessing early intervention services is the Individualized Family Service Plan (IFSP). The IFSP is a legal document that outlines the early intervention supports and services a child will receive. It is developed to address the specific needs, concerns, and priorities of children from birth to age three and their families. The IFSP includes the family’s desired outcomes for their child and describes the early intervention services that will help achieve those outcomes. Additionally, it specifies when, where, and how these services will be delivered. High-quality IFSPs are essential in early intervention as they promote positive developmental outcomes for children with delays or disabilities by ensuring that services are tailored to their unique strengths, needs, and family priorities (Early Childhood Technical Assistance Center, 2021). These plans also empower families by enhancing their ability to support their child’s development, ultimately improving the child’s long-term educational and social outcomes (Hebbeler & Spiker, 2016). Given this, state and Local Education Agencies (LEAs), or other administrators of state Part C services, have a vested interest in improving the quality of IFSPs by adopting research-based methods that also enhance the IFSP process for children, families, and practitioners.
The Routines-Based Interview
The Routines-Based Interview (RBI) is a semi-structured interview process which is designed to assess overall child and family functioning; to establish a positive relationship between early intervention providers and the family; and to develop more functional, high-quality outcomes as part of a child’s IFSP (McWilliam et al., 2009). The RBI provides a useful framework for identifying functional and routines-based outcomes, helps to align a family’s priorities with the IFSP process, and supports the development of meaningful outcomes (McWilliam, 2010). The RBI is both a method and a process designed to foster increased investment between providers and families, as well as other adults who play critical roles in the life of the young child and family, such as childcare providers (McWilliam, 2010).
Since it was originally introduced 30 years ago, the RBI has evolved into a set of well-defined steps. Implementation of the RBI follows a six-step protocol designed to help families identify priorities for their child’s early intervention plan (McWilliam et al., 2009). The process begins with beginning statements, where the professional facilitating the RBI explains the purpose of the interview to initiate a positive, collaborative relationship which centers the family’s concerns and priorities in the IFSP development process. In the second step, functional routines are used to frame the discussion agenda, allowing the family to describe their typical daily activities, which sets the stage for detailed discussions. During the third step, the interviewer gathers information about a family’s routines and the child’s current functioning within those routines by asking open-ended questions to learn how the child participates in various activities and interacts with family members. For the fourth step, the interviewer assesses the family’s satisfaction with their existing routines using a scale to identify which routines are going well and which are challenging. The fifth step focuses on identifying concerns and priorities, where the family shares what they want to focus on, and the interviewer helps them articulate meaningful outcomes. Finally, for the sixth step, the family’s priorities are translated into specific, functional outcomes that guide the child’s IFSP (McWilliam, 2010; McWilliam et al., 2009).
Evidence Base of RBI
The RBI has gained widespread adoption, including within the United States and internationally (McWilliam et al., 2020), with implementation research showing both successes and challenges associated with the model. Studies show that implementation of the RBI in the IFSP development process leads to greater establishment of family-centered priorities as well as the development of more functional and routines-oriented outcomes (McWilliam et al., 2009). RBI has been shown to provide an accessible way for a provider to develop a working knowledge of the way a child and family functions in the context of meaningful routines. This, in turn, allows providers to support a family in identifying their key priorities and their child’s current competencies in order to develop more functional and meaningful outcomes (Pereira et al., 2022).
To date, few studies have explicitly examined the relationship between the fidelity of RBI implementation and IFSP quality, with most having relatively small sample sizes (e.g., McWilliam et al., 2009). Existing RBI studies tend to focus primarily on qualitative methods, program evaluations, or single-site implementations (e.g., Pereira et al., 2022; Ridgley et al., 2011). That said, there is research which compares IFSP quality across sites using a quasi-experimental document review or comparative analysis of archival IFSPs (e.g., Boavida et al., 2016); however this research often does not include measures of RBI fidelity, making it difficult to determine whether differences in IFSP quality are due to the RBI itself or to variations in how it was implemented. Thus, the absence of rigorously designed quantitative designs (i.e., randomized-controlled trials and quasi-experimental designs) which also measure RBI fidelity of implementation leaves unanswered questions about whether differences in IFSP quality can be attributed to the implementation of RBI training across contexts, particularly given that few studies account for the fidelity with which the RBI was delivered. Given the existing evidence base, RBI is not formally designated as an evidence-based practice by major clearinghouses such as the What Works Clearinghouse (United States Department of Education, n.d.), but the model is well aligned with the Recommended Practices established by the Council for Exceptional Children’s (CEC) Division for Early Childhood (DEC, 2016). Namely, the approach supports practices within the area of assessment, such as working with families to “obtain information about the child’s skills in daily activities, routines, and environments . . .” (DEC, 2016, p. 12) and to “provide services and supports in natural and inclusive environments during daily routines and activities to promote the child’s access to and participation in learning experiences” (DEC, 2016, p. 14). The process also assists early intervention practitioners to “build trusting and respectful relationships with the family” and to be “responsive to the family’s concerns, priorities, and changing life circumstances” (DEC, 2016, p. 16).
Impact of RBI on IFSP Quality
Previous research has shown improvements in IFSP quality as a result of RBI training. For example, Boavida et al. (2014) described and evaluated an RBI professional development program aimed at enhancing the quality of IFSP outcomes; IFSP quality was measured using the Goal Functionality Scale III (GFS III), with scores increasing from 8.94 to 19.77, reflecting a large effect size (d = 3.04). Although fewer outcomes were developed, those which resulted were found to be more focused and functional, reflecting a shift toward relevance and practicality in the IFSP (Boavida et al., 2014). Similarly, Boavida et al. (2016) examined the perceptions of participants who attended an in-service RBI training program as well as the IFSPs they developed. Participants who demonstrated stronger baseline skills initially showed further improvement in their outcome development after training, with RBI training shown to make a positive impact on their outcome quality, overall (Boavida et al., 2016).
Implementation fidelity must be established before the effects of the intervention can be meaningfully evaluated. Previous studies have been conducted to measure and evaluate the construct of RBI fidelity. For instance, Boavida et al. (2015) investigated the psychometric properties of the RBI Implementation Checklist (McWilliam, 2010), a 36-item instrument designed to measure fidelity of implementation. The instrument measures both RBI structures and interviewing behaviors of professionals and was shown to have a very high level of internal consistency (Boavida et al., 2015). Additionally, group differences tests showed that the instrument can detect differences between professionals from various program types.
Although some studies have investigated the impact of RBI on IFSP quality, few have examined the influence of fidelity of implementation on these outcomes. This gap is substantial, as higher fidelity is often associated with better results in early intervention practices (McWilliam et al., 2009). There is a need for research that explicitly compares IFSPs written by providers who have achieved fidelity of RBI implementation with those written by providers who have not received RBI training. This study addresses critical gaps in the literature by providing a quasi-experimental comparison of IFSP quality across multiple districts, with a focus on fidelity of implementation thresholds. Using a state’s compliance monitoring tool, this study examines IFSPs from both RBI-trained and untrained providers across six LEAs.
Method
We identified how training and implementation of the RBI process impacted the quality of IFSPs across one mid-Atlantic state, by comparing IFSPs developed collaboratively with families by providers who met a pre-established threshold for RBI fidelity of implementation with the IFSPs associated with providers who had not received training in RBI. This study employs an ex post facto quasi-experimental design (QED) study, with average ratings of IFSPs from LEAs that received RBI training compared to IFSP ratings from LEAs that did not receive the training. The overarching research question in this study was: How does training in the RBI process impact the quality of IFSPs developed by families and early intervention providers?
Study Context
In partnership with the state’s department of education, a university partner has been funded over time to deliver training in the RBI to interested LEAs. As part of this ongoing, multi-year effort, LEAs voluntarily identified personnel to attend the state’s RBI Institute, a 2-day, in-person training focused on the philosophy, structure, and implementation of the RBI process. The training includes direct instruction, modeling, and peer practice, and concludes with a written assessment to verify participants’ understanding of key concepts.
After the Institute, providers receive individualized coaching to support implementation. This coaching is flexible and paced based on the needs of each provider, typically lasting between 3 and 12 months. Providers begin by working in teams of two or three to complete guided practice interviews (GPIs) with immediate feedback from a coach. Team members rotate roles, and most complete two to three GPIs before transitioning to independent practice. During independent practice, providers continue to receive coaching (usually two to three 45-minute sessions) with written feedback as needed.
We assessed fidelity using the RBI Implementation Checklist in combination with a review of recorded interviews, RBI notes, ecomaps, and IFSP outcomes. Providers became eligible to submit materials for fidelity review once they had completed the required steps on the Implementation Checklist: attending the training institute, participating in guided practice with coaching feedback, and engaging in independent practice with self-reflection. In consultation with their coach, providers could then elect to submit materials for review, with repeated attempts permitted until the fidelity threshold was achieved.
Overall, the extent of RBI implementation varies across districts in the state. Some LEAs have fully integrated the RBI into their early intervention processes, while others have only partially adopted it or chosen not to participate. This variation creates a unique opportunity to compare IFSP quality across settings with differing levels of RBI use. In this study, we compared LEAs that fully adopted the RBI with those that had no training or implementation support.
Sampling
The university’s Institutional Review Board (IRB) consent was obtained prior to the start of the study to ensure ethical compliance and the protection of participant data. Participants were divided into two groups for comparison: an intervention group consisting of providers who were trained in the RBI process and a comparison group of providers who had not received RBI training.
In the state where this study was conducted, IFSPs are developed collaboratively by teams that include the family, the Service Coordinator, and other service providers. Service Coordinators are early intervention professionals who hold primary responsibility for facilitating the IFSP process, coordinating services across disciplines, ensuring compliance, and finalizing the IFSP document. For the purposes of this study, IFSPs were selected when the Service Coordinator had completed RBI training, and when possible, when other team members supporting the child had also completed RBI training. In cases where multiple team members contributed to the IFSP, the Service Coordinator remained the primary responsible party for the development and activation of the IFSP.
Intervention Group Selection
The intervention group was constructed by first identifying LEAs that had implemented RBI with at least 80% of their early intervention providers either fully trained in the intervention or actively engaged in a process to achieve this threshold over time. Within these LEAs, we identified providers who had met the fidelity of implementation criteria, defined as achieving a score of 80% or higher on the RBI Implementation Checklist (McWilliam, 2010). Only providers who had met this fidelity threshold within the last calendar year were included in the intervention group.
To ensure that RBI implementation was well-supported within the LEA, we verified that the LEA itself had maintained fidelity of having at least 80% of early intervention providers trained over the course of the year. Providers who met the selection criteria were assigned unique codes for confidentiality, with a minimum of 30 different providers randomly selected to comprise the intervention group. Using the state’s online IFSP platform, we selected up to three IFSPs developed in collaboration with families by each provider within the last calendar year. All personally identifiable information was removed from the IFSP documents prior to review, and the child referenced in each IFSP was assigned a code for tracking purposes.
Comparison Group Selection
The comparison group was constructed by identifying LEAs that had not participated in the state’s RBI training opportunities. LEAs were verified as non-participating to confirm that their staff had not received RBI training. Within these non-trained LEAs, we randomly selected a minimum of 30 providers who comprised the comparison group. For each of these providers, we selected up to three IFSPs developed within the last calendar year from the state’s online IFSP platform. Personally identifiable information was removed, and each child was assigned a unique code for tracking purposes.
Matching Process and Final Sample
Overall, this sampling process yielded 163 IFSPs, with 82 in the intervention group and 81 in the comparison group. Prior to sampling, an a priori power analysis was conducted using G-power to determine the minimum required sample size. Using a minimum detectable effect size (MDES) of .75, power of .8, and alpha of .05, we determined that the minimum required sample size across both conditions was 58. Thus, this study was adequately powered to detect meaningful differences in IFSP quality between the two groups, especially as prior research (i.e., Boavida et al., 2014, 2016; McWilliam et al., 2009) has consistently shown effect sizes of greater than one standard deviation.
Data Collection and Instrumentation
The Process Performance Indicators (PPI) for IFSPs is a tool developed by the state education agency in collaboration with the university partner. The DEC’s Key Principles and Recommended Practices (DEC, 2014) are aligned with each item in the measure. In practice, it is used to ensure that IFSPs in the state meet the compliance standards for the IDEA Part C, the state’s regulations, and that IFSPs reflect current recommended practices in the field. The PPI evaluates key areas such as family priorities, concerns, present levels, and child outcomes, helping to improve the overall quality of IFSPs. Items from this instrument were used to rate IFSPs included in study analyses. Items from the PPI focused on the following areas: family resources, family priorities, family concerns, present levels, compliance, and quality of child outcomes. Items on the PPI were identified by the state educational agency as either Best Practice Indicators or Compliance Indicators. Best Practice Indicators were scored on a 3-point scale while Compliance Indicators were scored dichotomously. Measures of total outcomes, total child outcomes, and total parent outcomes were counted data. Appendices A and B show each of the items measured within the PPI, including their alignment to DEC Key Principles and Recommended Practices.
Within the state where the study was conducted, the term “present levels” is used to refer to a child’s present levels of functional development. In the state’s IFSP, there are three sections of the IFSP which include statements describing developmental skills. This language includes the following three areas: (1) Developing Positive Social Skills and Relationships, (2) Acquiring and Using Knowledge and Skills, and (3) Using Appropriate Behavior to Meet Needs. For each, the IFSP includes an easy-to-understand description designed to help families interpret the information provided in these fields. These descriptions appear on the state’s IFSP form and were taken directly from the Early Childhood Technical Assistance Center (ECTA, 2021, 2025, 2026):
(1) Developing positive social skills and relationships: This refers to how children relate to those around them—their parents, caregivers, brothers and sisters, and other young children. This includes many different skills such as communicating, showing emotions appropriately, and controlling their own behavior. Having positive social relationships also requires young children to follow rules for how to interact, such as waiting one’s turn or sharing.
(2) Acquiring and using knowledge and skills: This refers to thinking, learning, reasoning, memory, and problem-solving skills, general knowledge that children acquire about their world, such as concepts of more and less, colors and shapes, stories and books, and using this knowledge to participate in everyday activities. It is about early learning and how children come to understand their world and acquire the skills they need to be successful in school and beyond.
(3) Using appropriate behavior to meet needs: This refers to children being able to take care of themselves and to use appropriate ways to get what they need and want. This includes everyday activities like eating, dressing, playing with toys, making choices, and getting from one place to another, as well as how they respond to challenges or delays in getting what they want. It also refers to children being aware of and responding to situations that may be dangerous. This ultimately focuses on emerging independence.
Steps were taken to improve the consistency and reliability of scoring using the PPI. Prior to rating all IFSPs, four research team members engaged in a norming process to ensure consistent application of the scoring criteria. Each of the scorers is a subject matter expert in special education and early intervention. Five IFSPs were independently rated by all four scorers, after which the team met to compare scores and identify any discrepancies. Through this process, inconsistencies in scoring were discussed, and consensus was reached on the interpretation of specific items. As a result of these discussions, additional scoring guidelines were developed to accompany the PPI and were used in the scoring of all remaining IFSPs to improve scoring reliability. This process was undertaken to strengthen the reliability of the scores in the absence of a formally defined scoring protocol. After these processes were undertaken, PPI scores were estimated to have a reliability (alpha) coefficient of .81, indicating acceptable levels of score reliability across all PPI items.
To further address inter-rater reliability, we conducted a post hoc reliability check after initial scoring was completed. Each rater was randomly assigned 10 IFSPs originally scored by another rater, with selection conducted by the data analyst. The IFSPs selected for this process were ones the secondary rater had not previously reviewed. Prior to this process, raters revisited the scoring guidelines developed during the norming process to ensure consistent application. Inter-rater reliability was calculated using percent agreement across all PPI items.
Analytical Approach
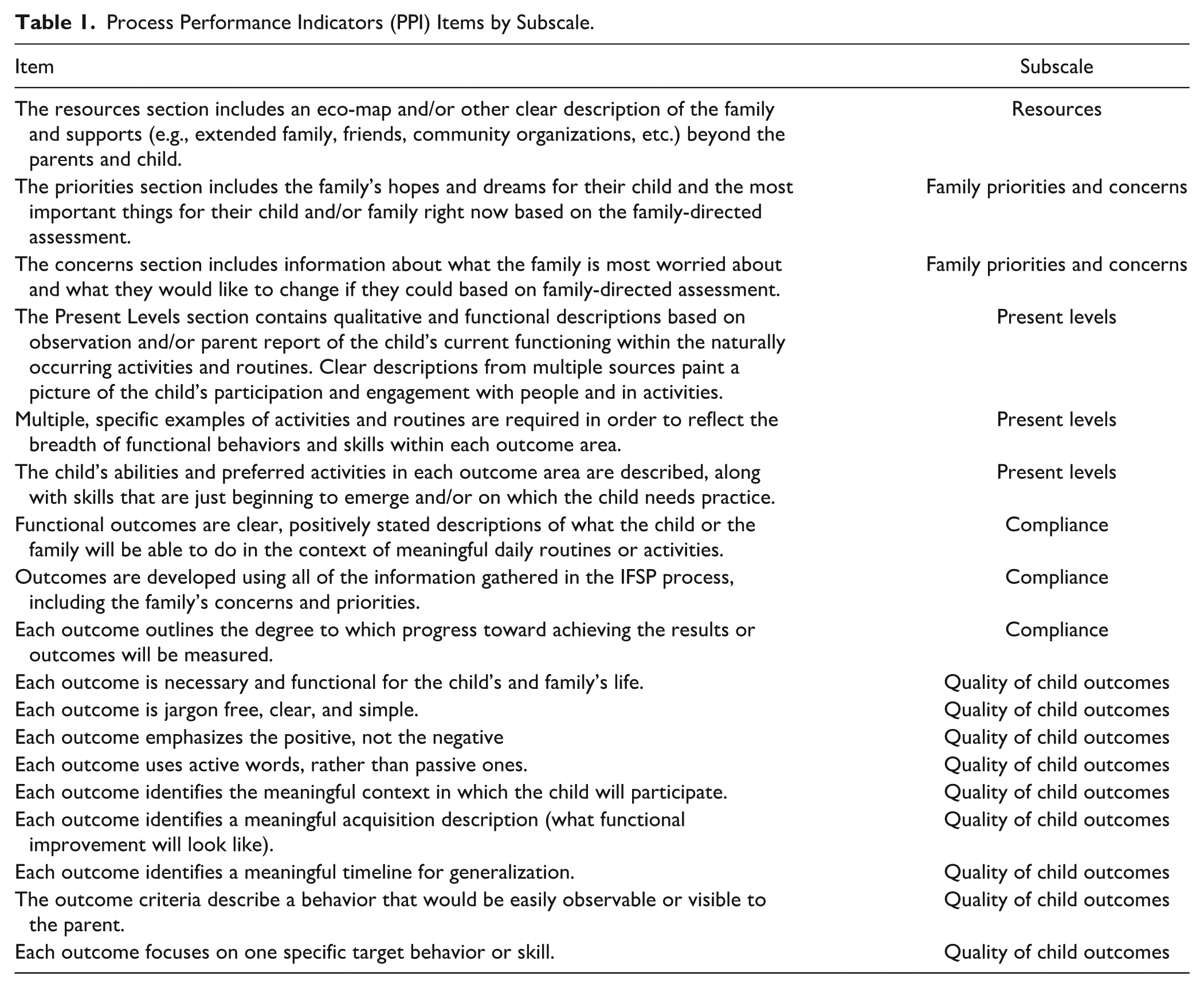
Average ratings by item were summarized descriptively. As most rating items were 3-point scales, non-parametric Mann–Whitney U tests were conducted to compare average ratings between conditions. Pearson chi-square tests of independence were conducted to examine differences in ratings between conditions on dichotomous items. Subscale scores were constructed by averaging together all items on the scale, with independent t-tests conducted to compare average subscale scores by condition. Subscale average scores were also summarized by LEA. An overview of the items that comprised each subscale can be found in Table 1.
Process Performance Indicators (PPI) Items by Subscale.
Results
Post hoc inter-rater reliability analyses indicated acceptable levels of agreement across raters. Percent agreement averaged 80% across all PPI items, with 14 of 21 items showing greater than 80% agreement. These findings support the consistency of scoring across raters in addition to the internal consistency of the instrument (Cronbach’s α = .81).
Item-Level Analyses
The first set of analyses examined differences in IFSP ratings on individual items by condition. Table 2 shows the results of Mann–Whitney U tests on each of the 3-point rating scale items.
Process Performance Indicators (PPI) Item-Level Comparisons.
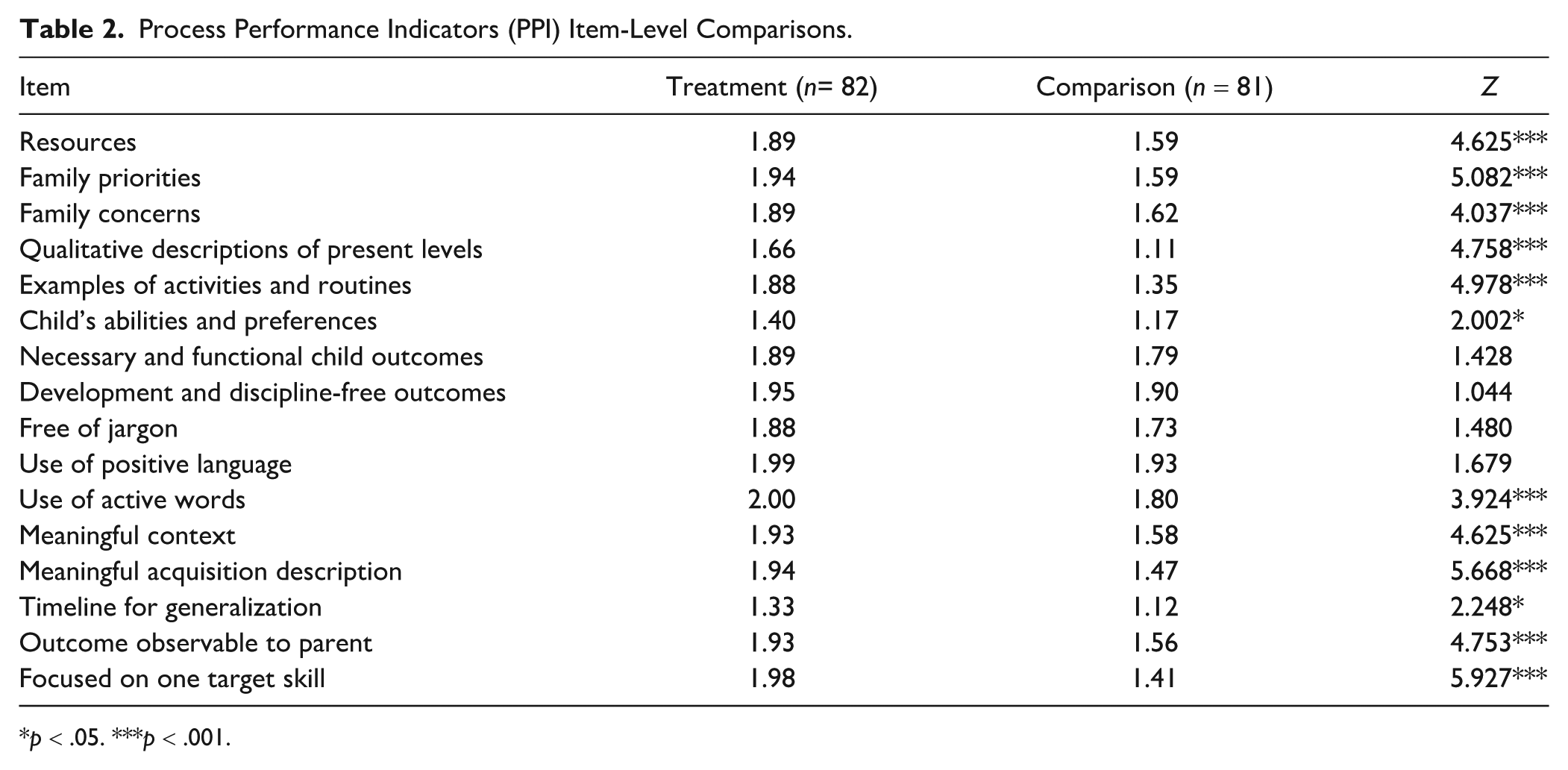
p < .05. ***p < .001.
Average ratings were statistically significantly higher for IFSPs developed with RBI-trained providers and families, compared to those from the comparison group. Intervention group IFSPs were rated higher in areas including family resources, family priorities, and family concerns, along with outcomes relating to present levels and some child outcomes. Non-significant comparisons were found on items relating to components of developing high-quality child outcomes. In general, IFSPs written by RBI-trained providers received statistically significantly higher ratings than did those from non-RBI-trained providers.
The next set of ratings examined differences in ratings on three compliance measures. As these were dichotomous ratings, Pearson chi-square tests of independence were used to determine if there were statistically significant differences in ratings between conditions. The results of these analyses are found in Table 3.
Process Performance Indicators (PPI) Compliance Item Comparisons.
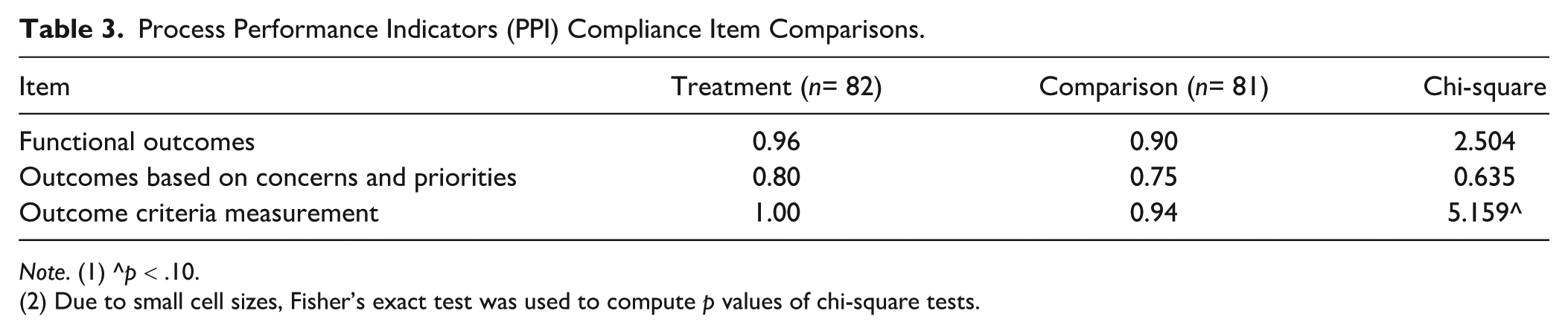
Note. (1) ^p < .10.
(2) Due to small cell sizes, Fisher’s exact test was used to compute p values of chi-square tests.
No statistically significant differences in ratings were found on any of these three compliance items, with intervention group ratings slightly larger on average than comparison ratings in all three cases.
Rating Subscale Comparisons
The next set of analyses consisted of independent t-tests that compared subscale average ratings between intervention and comparison IFSPs. The first five t-tests examined the subscales of Family Resources, Family Priorities and Concerns, Present Levels, Compliance, and Quality of Child Outcomes; these scales were averages of the individual items in each subscale and ranged from 0 to 2 in possible scores. The last three t-tests examined counts of total outcomes, child outcomes, and family outcomes for intervention and comparison IFSPs. The results of these analyses can be found in Table 4.
Process Performance Indicators (PPI) Subscale Comparison Results.
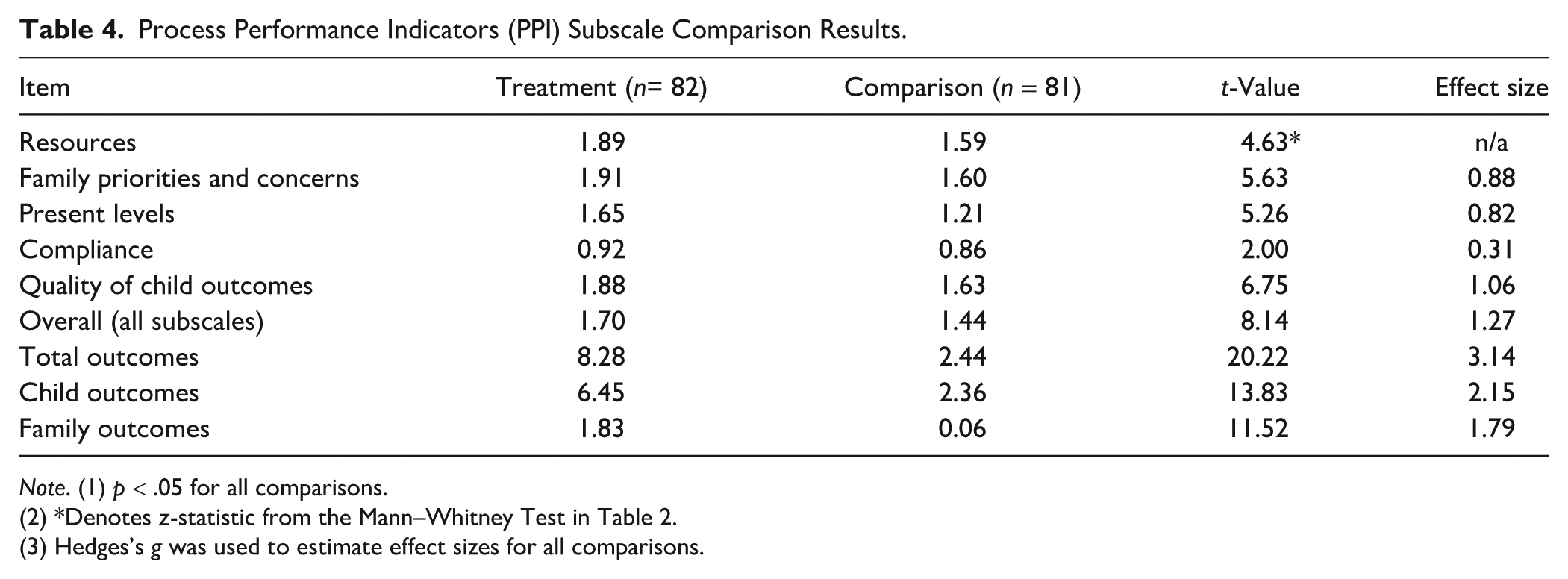
Note. (1) p < .05 for all comparisons.
(2) *Denotes z-statistic from the Mann–Whitney Test in Table 2.
(3) Hedges’s g was used to estimate effect sizes for all comparisons.
Statistically significantly higher intervention ratings were observed across all subscales relative to comparison ratings, as evidenced by the first five t-tests presented in Table 4. Effect sizes of these comparisons range from .31 to 1.06 SDs across subscales, indicating large practical impacts. In terms of counts of IFSP outcomes, IFSPs written by RBI-trained providers contained considerably larger numbers of total outcomes than did IFSPs written by comparison providers, with intervention group IFSPs containing nearly six more outcomes than did comparison IFSPs. When broken down by type of outcome, intervention group IFSPs contained four additional child outcomes and nearly two additional family outcomes than did comparison outcomes, on average. Effect sizes on counts of outcomes were very large, with an effect size of more than 3 SDs observed for total counts of outcomes.
Subscales by LEAs
The final set of analyses descriptively examined average IFSP ratings by LEA. As noted earlier, six LEAs engaged in RBI training in writing IFSPs, while another six LEAs did not participate in training. While the overall target number of IFSPs was reached within both the intervention and comparison groups, the number of IFSPs selected from each LEA varied. In general, the number of IFSPs selected from each LEA reflected the size of the district, with fewer IFSPs selected from smaller LEAs and more from larger LEAs. In some smaller LEAs, the number of eligible IFSPs was limited because only IFSPs developed collaboratively with families by providers who met fidelity thresholds within the past 12 months were included. To maximize sample size, as many eligible IFSPs as possible were selected across LEAs. Within LEAs, the number of participating providers ranged from 3 to 32 per jurisdiction. Although the sampling target was three IFSPs per provider, the number of IFSPs selected per provider ranged from one to three, depending on the availability of eligible plans. This variability in provider representation and number of IFSPs should be considered when interpreting differences across LEAs. Table 5 shows average subscale scores by LEA for all 12 LEAs that participated in the study.
Process Performance Indicators (PPI) Average Subscale Ratings, by LEA.
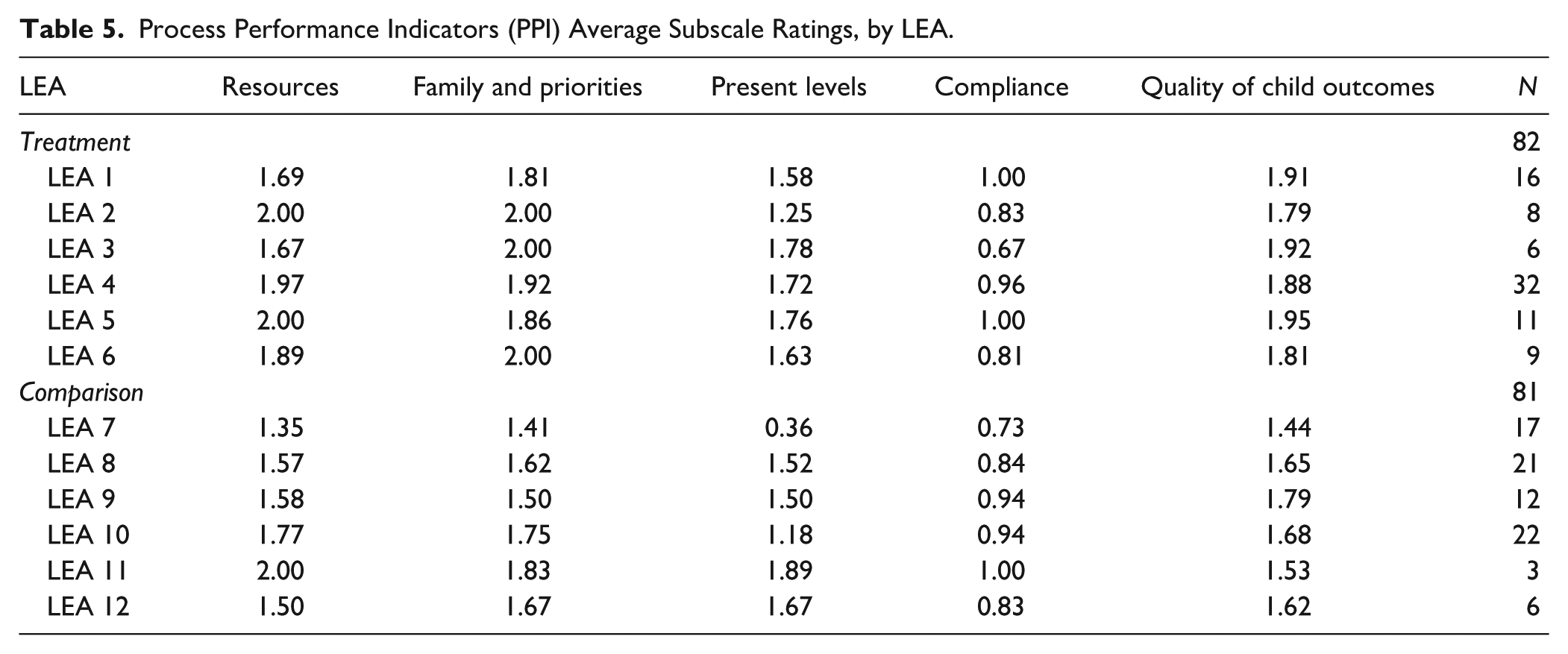
Consistent with prior results, average ratings for IFSPs in intervention LEAs tended to be higher than those of IFSPs in comparison LEAs. Ratings were consistently high across all six LEAs where the intervention took place, with LEAs 4 and 5 tending to have the highest ratings and LEAs 1 and 3 having the lowest (though still quite high). Ratings across comparison LEAs were more variable, with high ratings observed in LEA 11, for example (though only three IFSPs were written there), but lower ratings in LEAs 7, 8, and 12. Across all LEAs, the most variation was found in Present Levels and Resources ratings.
The results of the analyses in Table 5 showed that ratings of IFSPs from RBI-trained providers were statistically significantly higher, on average, than those of IFSPs from non-RBI-trained providers. Statistically significant differences in ratings were most prevalent on ratings relating to Family Resources, Family Priorities and Concerns, and Present Levels. Ratings on compliance and some facets of child outcome measures were more equivocal across IFSPs from both conditions. When examining ratings by LEA (Table 5), ratings in LEAs where the intervention took place tended to be higher and less variable than those in comparison to LEAs that did not receive RBI training.
Discussion
Implications for Practice
The findings of this study align with previous research (Boavida et al., 2014, 2016; McWilliam et al., 2009; Pereira et al., 2022) that shows a positive relationship between RBI implementation and IFSP development. In this study, all RBI-trained providers had achieved high fidelity on the process prior to IFSP development, so the results reflect differences between trained and non-trained providers rather than differences in fidelity levels. The results demonstrate that statistically significant improvements in IFSP quality were achieved by providers who were trained to implement the RBI and had reached fidelity. Because we did not include IFSPs from providers with lower fidelity, the study cannot determine whether the level of fidelity independently influenced IFSP quality, but future research should examine this relationship directly. Nevertheless, these findings are consistent with the broader literature suggesting that when RBI is implemented as intended, it can enhance the quality of information gathered from families and lead to higher quality IFSPs. This study has practical implications for quality IFSP development, specifically related to caregiver engagement, family outcomes, compliance, fidelity, and professional development.
This study highlights the importance of meaningfully engaging families and caregivers in the IFSP process. RBI-trained providers created IFSPs that scored higher in family resources, family priorities, and family concerns. Caregiver engagement is a critical element of the RBI process and of quality IFSPs. Families and other caregivers, such as child care providers who spend a substantial amount of time with children, play a crucial role in identifying family resources, priorities, and concerns. A high-quality IFSP extends the capacity of the family to support the needs of their child by centering their priorities within everyday routines.
Additionally, the IFSPs developed collaboratively with families by RBI-trained providers had more child and family outcomes than those developed with families by non-RBI-trained providers. These outcomes were more functional, measurable, and aligned with family priorities than those created by non-RBI trained providers. Explicit, meaningful, and measurable IFSP outcomes are an essential element of early intervention. The strategies aligned with these outcomes must be practical and easily implemented by parents or other providers within the context of daily routines. To ensure families are equipped to support their child’s development, it is necessary for early intervention providers to ensure that all caregivers have a comprehensive understanding of the strategies discussed during visits. This includes a clear picture of what the strategy entails, actionable steps for implementation, and practical ways it integrates within their everyday routines or the child’s natural environment. Since the real learning and practice happen after the provider leaves, it is important that caregivers feel equipped to integrate these strategies seamlessly, ensuring ongoing skill development and meaningful progress for the child. RBI-trained providers can serve as a bridge between family input and outcome development. Although implementation plays a critical role in child progress, the central focus of this study is the quality of IFSP development. By equipping providers with a structured process for gathering and using family input, the RBI enhanced the clarity, relevance, and measurability of IFSP outcomes; this creates a strong foundation for effective, routine-based intervention.
This study also has implications for IFSP compliance and RBI fidelity. Both RBI-trained and non-trained providers performed similarly on compliance items, suggesting that baseline training and internal processes such as IFSP system audits are effective. However, the findings here underscore the value of going beyond compliance and demonstrate that investing in RBI training is key to improving the quality and substance of IFSP outcomes. Implementing the RBI process with fidelity can help to address inconsistencies in IFSP quality, particularly in areas related to caregiver engagement and outcome specificity. These findings point to the importance of not only offering initial RBI training but reinforcing that training over time to support trainees to reach fidelity. Without that continued emphasis, the potential impact of the RBI process on IFSP quality may be diminished.
Although this study focuses on IFSP quality, it also surfaces important professional development takeaways that reinforce the value of structured training and ongoing support to strengthen provider practice. Professional development for providers should focus on how to increase family and caregiver engagement during every stage of the IFSP process to develop measurable, functional outcomes that address all the child’s needs, family priorities and concerns, as well as the child’s developmental stage. Given this evidence and findings from related studies, states and jurisdictions not currently utilizing the RBI process should weigh the potential benefits of implementing training, coaching, and provider support to strengthen caregiver engagement and improve IFSP quality. Access to this training and support over time can help to sustain improvements in IFSP quality, particularly in crafting functional outcomes and enhancing family engagement.
Lastly, the PPI tool used in this study serves not only as a compliance measure but as a coaching instrument. By grounding this study in a practical framework utilizing the state’s compliance tool, the authors wish to emphasize the potential of existing tools in other states, which can be used to inform both policy and practice, advocating in favor of a more integrated perspective on IFSP quality assessment. As a bridge between compliance and IFSP quality, tools like the PPI can be used for reflective coaching and feedback to promote providers’ learning. While the PPI tool is state-specific, states may adapt the model or use their own state-developed measures for feedback and coaching as well as for compliance and quality checks. Evaluating IFSP quality requires more than theoretical rigor; it necessitates approaches within the real-world contexts where these plans are developed and implemented. Research, after all, does not occur in isolation from the systems it aims to inform. Employing state compliance monitoring tools not only underscores the relevance of these findings but also demonstrates how such tools can serve dual purposes, meeting immediate regulatory needs while also contributing to broader questions about what constitutes high-quality and effective early intervention services. By focusing on these actionable strategies, early intervention systems can foster the development of high-quality IFSPs that reflect both the family voice and recommended practices. The findings of this study emphasize the importance of gathering rich information from the RBI to inform the development of measurable, functional outcomes that support meaningful change for more children and families.
Implications for Future Research
These findings highlight several areas for further investigation. First, it is critical to explore the availability and validity of assessment tools for a more comprehensive understanding of how best to evaluate the quality of IFSPs, particularly within each state’s existing framework of forms, formats, and monitoring tools. Future research might also explore the benefits and challenges of using a validated tool developed by researchers as compared to a state-specific monitoring tool such as the one used in this study. As states aim to replicate studies like this one, partnerships between universities, researchers, and state departments of education can play a pivotal role in influencing both research and practice. Collaborative partnerships can support the identification of tools that align with state-specific constructs and objectives. This helps ensure that implementation efforts remain grounded in practical relevance while also advancing the broader goals of early intervention research.
In the present study, all RBI-trained providers had achieved high fidelity prior to IFSP development, and the comparison was between trained-to-fidelity and non-trained providers. As a result, the findings cannot speak to whether varying levels of fidelity independently influence IFSP quality. Future research should explicitly examine differences in IFSP quality across a range of fidelity levels, including low, moderate, and high fidelity, to determine whether incremental gains in fidelity translate into measurable improvement in IFSP quality and/or whether those gains are sustained over time. Such results could offer valuable insights into the scalability and long-term impact of fidelity-focused RBI training programs which would guide efforts to enhance early intervention practices.
Future research should also investigate how high-quality IFSP outcomes developed through the RBI translate into real-world developmental gains for children. While this study demonstrated improvements in the quality of IFSPs, it remains unclear whether these improvements lead to better developmental, social-emotional, or academic outcomes for young children over time. Longitudinal studies tracking child progress post-IFSP implementation could provide a clearer understanding of the long-term benefits of high-quality, routines-based intervention planning.
Limitations
Several factors serve as limitations in this study. First, the PPI is a state-created tool, used primarily for regulatory compliance, professional development, and coaching. Therefore, this tool has not been rigorously tested for validity which may impact the consistency and applicability of the findings. However, this limitation is not without justification. The selection of the PPI was guided by its alignment with the state’s priorities and its practicality within the existing system. By utilizing a tool already integrated within the state’s framework, this study sought to bridge the often distinct domains of research and practice in early intervention. Likewise, while formal validation of the PPI has not yet been conducted, the alignment between the PPI items and the state’s early childhood framework supports the face and content validity of the tool. Overall, this alignment between the PPI and the state’s framework also helps to alleviate concerns related to the lack of extant validation evidence. Similarly, the subject matter expertise of the raters who used the PPI in this study helps to address potential concerns over inter-rater reliability evidence.
Secondly, limitations to generalizability should be noted. The authors acknowledge that states and local jurisdictions utilize different IFSP forms and implement different measures for reviewing the quality of these forms and formats. This variation in IFSP documentation and review criteria may limit the ability to compare these findings across all states, jurisdictions, and other contexts. Although this study had an adequate sample size, the results may not be generalizable beyond the state in which the analyses occurred. LEAs who participated in RBI training did so on a voluntary basis and therefore may already have a stronger commitment to high-quality IFSP development. Additionally, variability in the number of providers and IFSPs selected across LEAs, due to differences in LEA size and provider eligibility, resulted in unequal sample sizes. While statistical analyses were conducted to examine IFSP quality, this variability should be considered when interpreting the results.
While Service Coordinators are primarily responsible for drafting and finalizing IFSPs in this state, the development of IFSPs is inherently a collaborative process involving input from families and other service providers. Although the sampling strategy prioritized IFSPs developed with families and RBI-trained Service Coordinators (and, when possible, supported by other RBI-trained providers), it is possible that contributions from non-RBI-trained team members influenced the content and quality of some IFSPs. This collaborative nature of IFSP development should be considered when interpreting the findings.
Lastly, this study focuses primarily on IFSP quality rather than long-term child and family outcomes. While improvements in IFSPs suggest stronger alignment with recommended practices, future research is needed to determine whether these improvements translate into meaningful developmental gains for children and increased family engagement in early intervention processes.
Conclusion
The findings from this study provide evidence that RBI training is associated with statistically significant improvements in IFSP quality at the state level. IFSPs developed collaboratively with families by providers who received RBI training consistently demonstrated higher ratings in important areas such as family resources, priorities, and concerns, indicating the benefit of this approach in developing meaningful and functional outcomes. Results indicated that training in RBI yielded more detailed family-centered plans that correspond to recommended practices in early intervention. The study, however, uncovered some areas where improvements were needed, particularly concerning the development of quality child outcomes and explicitly including family outcomes with action steps.
Findings from this study support the continued expansion of RBI training. Findings also indicate the need for professional development focused on writing measurable and developmentally appropriate outcomes, supporting families to implement strategies, and ensuring that learning extends beyond provider visits. Equipping families with clear, practical strategies that integrate into their daily routines and natural environment is essential to maintaining ongoing child progress and development.
These findings contribute to the broader discussion of early intervention practices by emphasizing the importance of fidelity in RBI implementation. Given the variability in IFSP quality across different LEAs, targeted feedback and support for agencies or programs not currently using RBI may help bridge gaps and ensure more consistent implementation across a state or jurisdiction.
Overall, this study supports that training and implementation of the RBI process can enhance the quality of IFSPs. By refining and expanding training efforts, strengthening provider competencies in outcome development, and ensuring that families are fully equipped to implement strategies at home, early intervention services can further optimize child development and family engagement. Continued research and investment in professional development is essential to advance the quality and effectiveness of IFSPs. By uniting research and practice through the thoughtful use of state tools, early intervention programs can benefit from practical, context-specific approaches that drive meaningful improvements in early intervention services.
Footnotes
Appendix
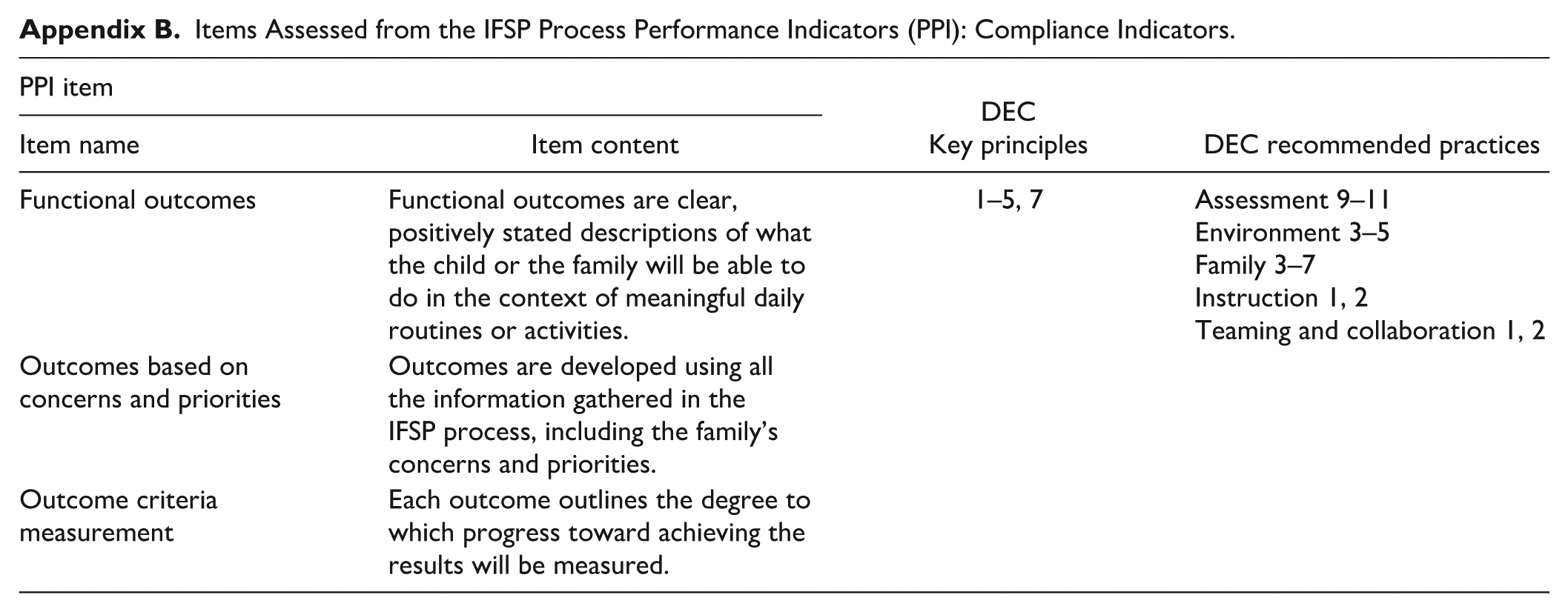
Items Assessed from the IFSP Process Performance Indicators (PPI): Compliance Indicators.
| PPI item | DEC |
DEC recommended practices | |
|---|---|---|---|
| Item name | Item content | ||
| Functional outcomes | Functional outcomes are clear, positively stated descriptions of what the child or the family will be able to do in the context of meaningful daily routines or activities. | 1–5, 7 | Assessment 9–11 Environment 3–5 Family 3–7 Instruction 1, 2 Teaming and collaboration 1, 2 |
| Outcomes based on concerns and priorities | Outcomes are developed using all the information gathered in the IFSP process, including the family’s concerns and priorities. | ||
| Outcome criteria measurement | Each outcome outlines the degree to which progress toward achieving the results will be measured. | ||
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Maryland State Department of Education.