
Abstract
We examined the effectiveness of coaching on caregiver implementation of responding to joint attention (RJA) intervention for toddlers with autism. We used a nonconcurrent multiple-baseline across participants single-case research design to examine the relation between coaching practices and caregivers’ RJA intervention implementation behaviors. Results indicated caregiver coaching that incorporated a behavioral skills training model was an effective approach for coaching caregivers on RJA intervention and resulted in caregivers’ improved use of intervention procedures. All three toddlers with autism demonstrated an increased number of correct RJA behaviors; however, the level of behavioral change varies across children.
Keywords
Joint attention (JA) is defined as the coordination of visual attention to a target object with another individual by sharing interests and social engagement while understanding that the other individual is sharing the same focus (Bakeman & Adamson, 1984). Successful JA skill development involves appropriately responding to JA bids (e.g., looking at where someone points) and initiating a bid for JA (e.g., pointing at an object to get someone to look; Tomasello, 1995). The emergence of JA in typically developing children occurs between the ages of 8 and 15 months, and responding to JA develops earlier than initiating JA (Bakeman & Adamson, 1984; Jones et al., 2006). Early signs of JA develop in a sequential manner; infants engage in face-to-face interactions in the early months, then shift toward engaging with objects around the mid-year, start responding to attempts by caregivers to share attention and focus together by the last few months, and finally initiating JA by showing or pointing to objects in later development (Adamson & Bakeman, 1991). JA development at an early age is highly associated with later communication development (Mundy et al., 1990; Nowell et al., 2020). For example, children can learn new vocabulary and form a sentence (e.g., “car goes down the ramp”) by using JA skills to link objects or events with their environment (Bruner, 1995). JA skills also facilitate children’s social initiations with adults and peers (Mundy & Sigman, 2015).
However, JA skill development is noticeably delayed and different in many children with autism compared to typically developing children and children with other developmental delays (Adamson et al., 2019; Mundy et al., 1990). Although the cause of this delay remains unknown, it stands out as a prominent characteristic in young children with autism (Johnson & Myers, 2007). JA is crucial not only as an indicator for diagnosing autism but also for its significance in early language learning for children with autism (Salo et al., 2018; Toth et al., 2006). Delayed JA development in autism plays a pivotal role in restricting social interactions, which subsequently contributes to developmental delays in various areas, such as social and academic skills (Freeman et al., 2015).
JA Interventions for Young Children with Autism
Studies examining JA interventions for young children with autism have shown improved child outcomes (Murza et al., 2016; White et al., 2011). Interventions for JA development include studies focusing on child–adult interactions with JA development as a collateral outcome and studies directly targeting JA skills (Paparella & Freeman, 2015). Different teaching procedures and programs have been used to improve JA skills, including discrete trial training (DTT) and pivotal response training (PRT; Jones & Feeley, 2009; Rocha et al., 2007); JA Mediated Learning (JAML; Schertz et al., 2013); JA, Symbolic Play, Engagement, and Regulation (JASPER; Kasari et al., 2006); and Improving Parents As Communication Teachers (Project ImPACT; Ingersoll & Dvortcsak, 2010). Across studies, behavior analysis principles are commonly applied despite variations in instructional approach, targeted behaviors, and the agents delivering interventions and coaching (Isaksen & Holth, 2009; Paparella & Freeman, 2015).
More recently, researchers have been combining both behavioral and developmental approaches to leverage their individual contributions (Tiede & Walton, 2019). For example, JASPER is a manualized intervention that uses a combination of behavioral and developmental procedures (Kasari et al., 2006). The environmental setup for JASPER facilitates children’s motivation with developmentally appropriate materials, and behavioral strategies such as reinforcement, modeling, and prompting procedures are used to help children learn JA and other social communication skills. This intervention has been tested across toddler- to preschool-age children with or at a high likelihood for autism and generally proved effective in improving JA development. However, outcomes varied across specific behaviors that were measured, which may have been influenced by the individual implementing the intervention or delivering coaching (Waddington et al., 2021). Similarly, Project ImPACT, an evidence-based developmental behavioral intervention that promotes social communication development, including teaching JA skills to children from 18 months to age 8 (Ingersoll & Wainer, 2013). Reinforcement and prompting procedures are used when teaching new skills, such as responding to parents’ JA bids at home. Only recently have the studies on Project ImPACT been tested in community settings, in which the goal is to equip early intervention (EI) providers, behavior therapists, or teachers to work with families (e.g., Stahmer et al., 2020). There is a general consensus that more research is needed to have sufficient evidence to suggest the generalizability of the intervention targeted in promoting the development of JA skills across people, settings, and contexts (Bruinsma et al., 2004; Jones et al., 2006; Murza et al., 2016).
Two potential reasons for the lack of generalization of children’s JA behaviors after successful skill acquisition are (a) limited opportunities to practice JA skills in diverse contexts during structured interventions and (b) restricted opportunities provided by untrained adults (Kasari et al., 2010). Children may excel in using JA skills in structured one-to-one teaching environments with clear discriminative stimuli but struggle in naturalistic settings such as typical routines or activities. Additionally, adults may not be prepared to offer appropriate JA bids in unstructured environments potentially affected by many other variables. Thus, utilizing natural contexts with familiar interaction partners during JA interventions can enhance children’s ability to generalize JA skills to typical interaction environments (White et al., 2011).
Caregiver-Implemented Intervention
Caregiver-implemented instruction is a promising approach to developing JA skills for young children with autism (e.g., Schertz et al., 2018). As an evidence-based practice, caregiver-implemented intervention has been mandated within the EI system (Individuals with Disabilities Education Act, 2004). In addition, involvement of caregivers in the intervention implementation has been emphasized, considering young children under the age of 3 spend the majority of their time with caregivers at home. Therefore, caregivers can provide maximized social learning opportunities throughout daily interactions and routines at home, which may also contribute to children’s generalization of newly acquired skills (Tait et al., 2004). Moreover, given that JA is first observed during child and caregiver interactions, involving caregivers as the direct JA instruction implementers in EI services for young children with autism can be an effective way to intervene as early as possible.
Coaching caregivers to implement JA interventions has occurred through a variety of methods. Schertz and Odom (2007) conducted 1-hour in-person home visits for 11 to 16 sessions over 9 to 26 weeks, providing coaching to caregivers. Coaching involved various strategies such as modeling, verbal and written instruction, prompting, rehearsal, and in-situ feedback by EI providers. Another study (Jones et al., 2006) involved hour-long in-person coaching sessions for 19 to 35 sessions throughout the study period. Preschool teachers verbally described intervention procedures, and used modeling, prompting, and feedback strategies to coach caregivers. Similarly, Rocha et al. (2007) used instruction, modeling, rehearsing, and feedback strategies during 1-hour and 15-minute sessions held 3 days a week for up to 50 sessions on average across three caregivers. These coaching approaches, although effective in enhancing caregivers’ implementation of JA teaching skills, demand a considerable time commitment.
Caregiver-implemented interventions for teaching JA skills during activities and routines often involve extensive coaching in multi-step instructional procedures such as PRT (e.g., Rocha et al., 2007) and JAML (e.g., Schertz et al., 2013). These types of coaching spanned multiple weeks (e.g., 15-week coaching; JAML; Schertz et al., 2013), involved multiple standardized assessment tools (e.g., ADOS, Mullen Scales of Early Learning, Autism Observation Scale for Infants, Preschool Language Scale; Brown & Woods, 2015), and occurred at clinical settings instead of at home (e.g., therapy center; Gengoux et al., 2019). Although many procedures have been effective in improving JA skills (Brown & Woods, 2015; Gengoux et al., 2019), the considerable time and resources required may not be accessible for all caregivers. Therefore, some families may prefer less time and resource-intensive coaching procedures.
Brief caregiver coaching on instructional procedures can utilize an effective adult teaching model such as behavioral skills training (BST; Schaefer & Andzik, 2021). BST, an empirically supported training package, is used to teach teachers, staff, caregivers, and preservice therapists a variety of skills (DiGennaro Reed et al., 2018). It comprises instruction (verbal or written descriptions of teaching), modeling (demonstration of correct performance), rehearsal (opportunities for trainees to practice skills), and feedback (encouragement for correct responses and correction for incorrect responses; Miltenberger, 2015). Caregivers benefit from BST as it offers explicit, structured, and systematic applications (Miles & Wilder, 2009). Although BST has effectively taught caregivers novel skills in a short time period (Toelken & Miltenberger, 2012), it has not been used to teach them JA instructional strategies for toddlers with autism. Despite the availability of these effective adult teaching strategies, current professional training in EI settings focuses on directly implementing interventions with children but is not designed to equip EI providers to coach caregivers effectively (Fleming et al., 2011; Romano & Schnurr, 2022). Training professionals to support early signs of autism in children, including JA development, and providing skills in coaching families using evidence-based adult teaching procedures (e.g., BST model) is essential.
Purpose and Research Questions
The purpose of this study was to examine the effectiveness of coaching on caregiver implementation of responding to JA (RJA) intervention for young children with autism. RJA is defined as an individual responding to a gesture or the eye gaze of another individual by attending to the object (Bruinsma et al., 2004). Specifically, the study investigated whether brief coaching during ongoing EI activities could teach caregivers to implement RJA intervention with fidelity for their child with autism. Additionally, we aimed to examine the impact of caregiver-implemented RJA intervention on the JA skills of children with autism. The research questions addressed in the study were: (1) Does coaching that incorporates components of BST result in increases in caregiver RJA intervention implementation accuracy during typically occurring activities and routines at home? (2) Do levels of child RJA behavior increase when RJA intervention is implemented by the caregiver? (3) To what extent do behavior therapists report that online training is sufficient to coach caregivers to implement RJA intervention at home? (4) To what extent do caregivers report coaching that incorporates components of BST was sufficient to implement RJA intervention for their child with autism?
Method
Participants
Behavior therapists
A total of three behavior therapists in the United States providing at-home services to toddler-age children with autism and their families were recruited. Behavior therapists met the following inclusion criteria: (a) hold an active Board Certification in Behavior Analysis (BCBA©) from the Behavior Analysis Certification Board©; (b) provide at least 30 min of services weekly to a toddler (age 18–30 months) with autism in their home; (c) provide family coaching as part of their ongoing services in family homes; (d) willing to receive online training; and (e) anticipate continuing their caseload for at least 6 months.
Three behavior therapist participants were recruited from private clinics offering behavioral services to children with autism at home. Recruitment involved actively distributing research flyers within professional networks, conferences, workshops, and autism-related social media platforms. The first author, a doctoral student in special education, met with behavior therapists, described study criteria, and obtained signed consent if they met the criteria. Then, behavior therapists provided information about their role and caseload, describing their typical sessions with children and families. We provided them with a brief description of the caregiver-implemented RJA intervention and caregiver coaching model. Next, each behavior therapist contacted eligible caregivers and children on their caseload who needed caregiver coaching on implementing RJA intervention in home settings for participation.
Caregiver-child dyads
The target child participants were three toddler-age boys with autism who were receiving behavior therapy through home visits; these children were recruited with the assistance of their behavior therapists (see Appendix A). The target caregivers were adults who primarily interacted with the child at home (e.g., the mother). Caregiver–child dyads met the following inclusion criteria: (a) the child did not engage in JA as reported by the behavior analyst, (b) the child was between 18 and 30 months old, (c) the child had an autism diagnosis as reported by the parents, (d) family received at least 30 minutes weekly of home-based services from the consented behavior analyst, (e) child was not currently receiving RJA intervention as reported by caregivers and the behavior analyst, and (f) family reported access to the internet at their home. The first author met with the caregivers of each prospective child to obtain informed consent, and the child assent procedure was followed through in every session. To obtain a child’s assent, the caregiver approached them saying, “It’s time to play with me. Please come here to play.” If the child verbally agreed, nodded, or approached, they were considered to have assented. If the child verbally refused, shook their head, or moved away, it indicated not wanting to participate. Following a 1- to 3-minute wait, the caregiver repeated the same statement. The session was terminated if the child refused to assent after three attempts in one session. If the child consistently refused assent over three sessions, they were dismissed from the study. Study procedures, data collection, and forms for participant consent were approved by a university Institutional Review Board.
Settings and Materials
Online training for behavior therapists on caregiver coaching strategies and the RJA intervention protocol occurred via Zoom. All intervention sessions (i.e., caregiver coaching and follow-up coaching) occurred at the child’s home. Caregiver coaching sessions took place based on the area where the child preferred to stay (e.g., living room, bedroom) during the behavior therapist’s home visits. While the behavior therapist provided in-person coaching to the caregivers, the first author joined via Zoom to video record the session for data collection purposes. The first author turned off the video and microphone throughout the visit to prevent any potential distractions to the behavior therapist’s session with the caregiver and the child.
Online training, pre-coaching, caregiver coaching, and follow-up sessions were video recorded for data collection purposes via the Zoom video recording function. The online coaching fidelity, behavior therapist’s caregiver coaching implementation fidelity, caregiver RJA intervention implementation accuracy, and the child RJA behaviors were collected via paper and pencil recording forms. The timer on Zoom recordings was used to monitor session length. RJA intervention materials included five toys that were available at the child’s home (e.g., blocks, toy cars, books, etc.) that were identified as the child’s moderately preferred items and one highly preferred item that had a lower likelihood of children engaging in challenging behavior when the item was removed from the child’s hand.
Response Definitions and Measurement System
The primary dependent variable was caregiver RJA intervention implementation accuracy, and the secondary dependent variable was the child’s independent RJA behaviors. The same response definitions for caregiver RJA intervention implementation accuracy and child RJA behavior were used across participants, with examples and nonexamples of each variable specific to the context in which the caregiver selects intervention. Child choice behaviors were measured during preference assessments prior to the study and every 2 weeks.
Caregiver RJA implementation
Caregiver RJA intervention implementation was measured via video using direct observational recording (Ayres & Ledford, 2014). All RJA intervention sessions included 10 trials with 9 steps each (90 total steps each session). Data on caregivers’ correct implementation of each step in the RJA intervention that each caregiver learned through caregiver coaching were collected on a trial-by-trial basis and were aggregately reported at the session level. The percentage of steps a caregiver accurately implemented was calculated using the following formula: dividing the number of correctly implemented behaviors by the total number of expected behaviors and multiplying the quotient by 100.
Child RJA behavior
Child RJA behaviors were measured via video using direct observational recording (Ayres & Ledford, 2014). RJA behaviors were defined respectively for each stage of RJA intervention. For RJA to items within the reach stage, RJA behavior was defined as manipulating or looking at the newly presented toy for at least 3 seconds. Examples include rolling a toy car for 5 seconds and looking at the book the caregiver is holding for 3 seconds. Non-examples include facing toward the book the caregiver is holding for 1 second and facing back to the toy the child was originally playing with. During RJA to items out of reach intervention, child RJA behavior was defined as looking at or showing gestures to reach for a newly presented toy for at least 3 seconds (e.g., reaching for the block caregiver is pointing to for 4 seconds).
The child’s accurate RJA responses were collected for each trial for a total of 10 opportunities in each session. Child independently engaging in the correct response “I,” correct response with caregiver’s prompt “P,” and no response “NR” were recorded.
Choice during preference assessment
Children’s choice during the preference assessment was defined as the participant touching, grasping, and/or mouthing the item with one or both hands for at least 3 seconds, crawling or walking toward the item, or pointing or trying to reach to an item with the finger(s) or hand(s). Any of these actions could occur with or without eye gaze. Data were collected in situ. Choice responses during the preference assessment were measured on a trial-by-trial basis using a paper and pencil data recording sheet. The item selected by the child was recorded for each trial; if no selection was made, the response “NR” was recorded.
Experimental Design
A nonconcurrent multiple-baseline (NCMB; Watson & Workman, 1981) design across caregiver-child dyads was employed to evaluate the effectiveness of BST coaching on caregiver-implemented RJA intervention for toddlers with autism. The NCMB design was appropriate for this study because collecting baseline data nonconcurrently across the participants allowed the participants to begin intervention relatively quickly after the baseline data met the condition change criterion. Additionally, the NCMB design was suitable for the current study because participants were independent of each other and not influenced by shared environmental factors, minimizing the likelihood of covariation. Data were graphed daily after participant behaviors were measured via video recordings. Visual analysis was used to examine the relation between BST coaching practices and the caregiver’s RJA implementation accuracy (Ledford & Gast, 2018). Specifically, level, trend, and variability were analyzed between and across conditions, and immediacy of effect, overlap, and consistency of data patterns was analyzed across conditions and tiers.
Initiation of caregiver coaching was staggered across three individual caregivers provided by each behavior therapist to demonstrate a treatment effect. Decisions regarding condition changes were made based on the caregiver’s RJA intervention implementation accuracy. However, consistent with guidance for using NCMB designs, baseline lengths were randomized (Watson & Workman, 1981). If the caregiver’s RJA intervention implementation accuracy data were not stable at the end of the randomly assigned number of baseline sessions, one additional session was continued, and the last three data points in the baseline condition were visually analyzed for data stability. The coaching intervention began when the baseline data were stable.
Once the first caregiver demonstrated stable baseline data, the behavior therapist paired with the first caregiver participant began coaching (the first stage of RJA intervention; RJA to items within reach). While the first caregiver participant began caregiver coaching, the baseline data for the second caregiver participant were collected to have varied lengths of baseline data to visually demonstrate the minimization of the threats to internal validity. The second caregiver accessed coaching once the condition change criterion was met. Coaching on the second stage of RJA intervention, RJA to items out of reach, was introduced contingent on the child’s 80% correct response on RJA for three consecutive sessions. This design allowed a systematic examination of the relation between caregiver coaching and the caregiver’s RJA intervention implementation accuracy. The last caregiver participant’s baseline data were collected after the first caregiver participant began the coaching session and during the second caregiver participant’s baseline data collection. Baseline data lengths differed from the other two caregiver participants’ baseline data to adequately evaluate threats to internal validity. The third caregiver participant’s coaching was delivered once the baseline data points remained at a low level.
Within the caregiver coaching condition, the change of the RJA intervention stage (i.e., 'RJA to items within reach’ to 'RJA to items out of reach’) depended on the child’s RJA behavior. If the child’s response did not reach 80% correct RJA behavior for two consecutive trials during RJA to items within-reach intervention stage, the caregivers were not asked to implement RJA to items out of reach teaching procedure and were asked to continue implementing RJA to items within-reach intervention. Decisions on condition change and RJA intervention stage change within the treatment phase were dynamic processes that allowed data-based decision-making with respect to the implementation effects of the intervention through continuous examination of raw data on the dependent variable (Ledford & Gast, 2018).
Procedures
Sessions occurred during the behavior therapist’s home visiting sessions scheduled two to three times a week. For each behavior therapist–caregiver–child triad, there were three main research activities: (a) online training for the behavior therapists, (b) caregiver coaching on RJA intervention delivery, and (c) caregiver independently implementing RJA to the child (i.e., follow-up sessions). Online training for behavior therapists occurred at any time during the baseline phase of the caregiver participants. Caregiver coaching sessions lasted 25–35 minutes each across participants. At the start of each session, verbal assent was obtained from the child following the child assent procedure (described above). If the child participant indicated a willingness to participate, the session was conducted. The first 15–20 minutes focused on didactic teaching of the procedural steps and techniques for RJA intervention. The remaining 10–15 minutes allowed caregivers to implement RJA intervention with their toddler with autism for 10 trials. Two weeks after the caregiver coaching sessions ended, three follow-up sessions occurred.
Online training
The behavior therapists individually received 30-minute online training for at least four sessions on coaching caregivers to implement RJA intervention for toddler-age children with autism. The online training sessions included (a) an overview and importance of JA for children (session 1); (b) the benefits of caregiver coaching (session 2); (c) the caregiver coaching model (i.e., BST), and specific strategies or techniques for coaching JA (sessions 3 and 4, respectively). A one-page handout was provided for each session. For sessions 3 and 4, videos modeling the BST and the RJA intervention procedures were provided along with the handouts. The behavior therapist had the opportunity to ask questions about the contents or procedures that were addressed throughout the online training. The online training sessions continued until the behavior therapists reported feeling confident in coaching the caregivers. Once the behavior therapists reported feeling confident, they demonstrated RJA intervention implementation procedures without the primary researchers’ prompt while the researcher coded the fidelity of the intervention implementation. The online training was terminated if the behavior therapist reached at least 80% fidelity of the intervention implementation.
Preference assessment
To determine toys for RJA interventions, an informal preference assessment adapted from Rocha et al. (2007) was conducted before baseline and every 2 weeks thereafter to assess child toy preference continuously. Each child was presented with 10 to 15 toys (e.g., toy car, block, etc.) selected based on the caregiver reports and previous preference assessments, if applicable. The items were interspersed within reach and visible distance of the child. Then, the children’s behavior in making choices during the preference assessment was observed and recorded following the response definitions described above. Once the child selected a toy, they were allowed 15 seconds of toy interaction; then, the toy was removed so the child could approach another toy freely. A preference hierarchy was established for each child. Five toys identified as moderately preferred were used in the order of least to most preferred for the following sessions. The behavior therapist and caregivers discussed and excluded toys or items that could potentially prompt the child to engage in challenging behavior contingent upon denied access.
Baseline
The behavior therapists provided an RJA intervention protocol and a written task analysis of the instructional procedure of RJA intervention and asked the caregivers to review it for 5 minutes. Materials (e.g., 4 moderately preferred toys and 1 highly preferred toy) were listed on the handout with the actual toys in a basket for the caregivers to use following the protocol. After 5 minutes, the caregivers were asked to implement RJA intervention procedures with the child without the handout. Handouts were not provided to caregivers in order to capture their existing RJA skills, if any. All sessions across baseline conditions were videotaped for data collection purposes, and no feedback was provided to the caregivers or the children. The baseline data were collected for both the caregiver and the child for at least three sessions until the caregiver’s RJA intervention implementation accuracy data (primary dependent variable) points were stabilized or demonstrated a counter-therapeutic trend.
Caregiver coaching
The four steps of the BST model (i.e., instruction, modeling, rehearsal, and feedback) were incorporated during the caregiver coaching procedure. Instruction and modeling procedures were used during the pre-coaching session, and rehearsal and feedback strategies were used during the main caregiver coaching sessions. Behavior therapists and caregivers jointly completed a coaching summary form after every coaching session, which was used to make adaptations to the following sessions as needed.
Pre-coaching
Prior to the main coaching session, pre-coaching was a 15–20 minutes didactic teaching focused on the specific procedural steps and techniques that were asked of the caregivers to use during their RJA intervention implementation. A one-page handout was provided with a written protocol of the RJA intervention procedure, including prompt fading and constant time delay (CTD; Wolery et al., 1992) procedural steps. The behavior therapist and caregivers reviewed the handout by (1) verbally explaining the procedural steps (instruction) and (2) modeling each of the task-analyzed steps. Modeling included showing how to initiate JA, how to use prompting procedures contingent on the child’s response, and how to provide praise and reward contingent on the child’s correct response. The caregivers were given the opportunity to ask questions they may have about the RJA intervention procedures or strategies after reviewing the handout.
Coaching
During the remaining 10–15 minutes of the coaching session, the caregivers had the opportunity to implement RJA intervention for their toddler-age child with autism for a total of 10 trials. The caregivers did not have access to the RJA intervention protocol handouts but had verbal feedback (i.e., constructive feedback, supportive feedback) from the behavior therapist. Constructive feedback was used to identify areas where caregivers’ teaching practices could be enhanced. For example, the behavior therapist might say, “During the initial trial, you pointed to the toy car and said, ‘Look, I have a car’, but the child was looking towards the door instead. You could try tapping him and saying ‘Look, I have a car’ and then wait for his response in the following trial,” to suggest caregivers effective prompting strategies when providing JA bids to the child. Supportive feedback was used to acknowledge and reinforce caregivers’ accomplishments by providing positive descriptions of their implementation behaviors. For example, the behavior therapist may say, “It was great to see you provide praise and the reward immediately to your child when he engaged in the correct response,” when the caregiver delivered the reward and praise with high fidelity.
Caregiver-implemented RJA intervention
The RJA intervention was divided into two sequential stages (RJA teaching procedure is available in Appendix B): (a) RJA to items within reach and (b) RJA to items out of reach (Whalen & Schreibman, 2003). Intervention procedures across both stages utilized CTD to implement RJA intervention trials. However, the controlling prompt in each session was specific to each caregiver–child dyad and changed in each sequential phase. The controlling prompt for Child A was pointing, hand-over-hand for Child B, pointing during the items within-reach procedure, and tapping during the items out-of-reach procedure for Child C.
For example, all trials began with a 0-second delay interval and then moved to a 3-second terminal delay for delivering a controlling prompt. Finally, all trials ended with the caregiver providing a 3-second response interval and delivering praise contingent on the child engaging in RJA. The RJA intervention procedural steps for each stage (described below) were measured as present or absent. The caregivers were instructed to implement a total of 10 trials during the 10- to 15-minute coaching session. If the caregiver did not provide an appropriate JA bid for approximately 1 minute, the behavior therapist provided a verbal prompt to the caregiver to initiate an opportunity. The planned steps for correct implementation are described below.
RJA to items within reach
In RJA within reach, the caregiver handed the child one of their moderately preferred toys that were identified from the preference assessment. While the child engaged with the moderately preferred toys, the caregiver presented a new toy to the child by holding the toy in front of the child and saying, “Look, I have a __” (providing appropriate JA bids during caregiver-child interaction). Then the caregiver delivered the controlling prompt after an initial (0 second) or terminal (3 seconds) delay interval. The caregiver then initiated a 3-second response interval. If the child engaged with the newly presented toy (i.e., manipulating or looking at the toy for at least 3 seconds) before (independent response) or after (prompted response) the controlling prompt, the response was correct. If the child did not engage with a newly presented toy (i.e., manipulating or looking at the toy for at least 3 seconds) before (independent response) or after (prompted response) the controlling prompt, the response was incorrect—there is no contingent caregiver response to an incorrect child response. Contingent on the child’s correct response, the caregiver provided specific praise and a reward of having access to a highly preferred toy for 15 seconds (providing praise with a reward). A trial ended after (a) the 3-second response interval if the child delivered no response or (b) delivery of praise and the item contingent on a correct response.
The decision to move from teaching RJA to items within reach to RJA to items out of reach was contingent on the child’s RJA behavior. If the child demonstrated 100% of correct RJA behavior independently for three consecutive sessions on items within reach, teaching RJA to items out of reach was introduced. If the child did not respond, the caregiver implemented the planned prompting procedure for the child (following the CTD procedures). Children A and B remained in this phase for the duration of the intervention; Child C moved to the out of reach procedure listed below.
RJA to items out of reach
The procedural steps were the same as in the previous stage, except that the location of the newly presented toy was out of the child’s reach instead of in front of the child. Accordingly, the child’s correct RJA behavior included the gesture of reaching for the new toy or looking at the new toy for at least 3 seconds. Caregivers had the option to select either (a) pointing to the object with the caregiver’s finger or (b) shifting the eye gaze from child-toy-child without pointing as the prompting procedure.
Follow-up
In the follow-up sessions, the caregivers were asked to independently implement RJA intervention for their child, and the behavior therapist only provided verbal feedback during the follow-up sessions.
Interobserver Agreement
Secondary observer data were collected for at least 33% of sessions across conditions, participants, and behaviors to calculate interobserver agreement (IOA; Ayres & Ledford, 2014). Reliability data were collected on the caregiver RJA intervention implementation accuracy and child RJA behaviors at least every third session of each condition using video recordings and paper pencil recording forms. Reliability data collection occurred by observers who were masked to the study purpose and primary researcher hypothesis. IOA was calculated using point-by-point agreement for each dependent variable using the following formula [agreements/(agreements + disagreements) × 100)]. Average IOA across conditions for caregiver RJA intervention implementation fidelity was 87.22% for Caregiver A (range 83.33–93.33%), 87.22% for Caregiver B (range 83.33–93.33%), and 91.11% for Caregiver C (range 87.78–94.44%). The average agreement for toddlers RJA behavior data was 93.33% for Child A (range 90–100%), 90% for Child B (range 80–100%), and 91.67% for Child C (range 90–100%).
The secondary observer, a master’s student in Special Education, was trained prior to beginning the study. The observer was provided with descriptions of the dependent variable. The criterion for training was at least 90% agreement for two videos for each behavior. Discussions about discrepancies occurred after each session, in which agreement was below 90% across the primary and secondary observers.
Procedural Fidelity
Procedural fidelity (PF) data were collected on behavior therapists’ online training and caregiver coaching. Specifically, caregiver coaching in PF data involved measuring the behavior therapist’s implementation of procedures in (1) setting up the environment for coaching sessions, (2) instructing and modeling RJA intervention, (3) repeating rehearsal and feedback process on RJA intervention, (4) providing opportunities for caregivers on implementing RJA intervention with their child, and (5) facilitating session reflection and feedback. Direct systematic observational recording via video was used for at least 33% of sessions across participants, conditions, implementers, and behaviors. Overall fidelity for each session was calculated by dividing the number of correctly implemented behaviors by the total number of expected behaviors and multiplying the quotient by 100. PF data were collected at least every third session; sessions in which data were collected were determined by a random number generator. Fidelity data were collected by an independent observer who was not implementing the session. The fidelity coder collected online training fidelity data on 33% of the sessions across the behavior therapist participants. The first author collected the coaching fidelity data during 100% of coaching intervention sessions across behavior therapist–caregiver dyads.
The first author trained the fidelity coder by (a) providing written definitions of expected implementer behaviors by condition and (b) evaluating PF in a mock video for each condition. The criterion for training was 100% agreement with the primary researcher across two videos per condition. Average PF for online training was 93.33% for Behavior Therapist 1 (range 86.67–100%), 100% for Behavior Therapist 2, and 91.15% for Behavior Therapist 3 (range 84.62–100%). The average PF for caregiver coaching was 92.38% for Behavior Therapist 1 (range 80.95–100%), 93.75% for Behavior Therapist 2 (range 90–100%), and 93.89% for Behavior Therapist 3 (range 90–100%).
Social Validity
A social validity questionnaire was provided to all behavior therapists and caregivers 2 weeks following study completion. The questionnaire assessed participant’s perceptions of the study procedures. The questionnaire included six questions with 5 Likert-style responses. The social validity questionnaires asked the following: (1) if the online training (behavior therapist)/coaching (caregiver) was helpful; (2) how confident they are in providing caregiver coaching using BST model (behavior therapist)/implementing the RJA intervention (caregiver); (3) how often participants use caregiver coaching practices (behavior therapist)/implement RJA intervention at home (caregiver); (4) how often they used the practices before study participation; (5) if they would continue using BST caregiver coaching (behavior therapist)/the RJA intervention (caregiver); and (6) if they are willing to recommend this practices to other behavior therapists (behavior therapist)/families (caregiver). The last section of the questionnaire was an open-ended question asking the participants to describe how participation in the study changed their interactions with the caregiver (behavior therapist)/child (caregiver) and to include any other information they would like to share (see Appendix C).
Results
Given an NCMB across participants design was used, all data are presented in three ways. Figure 1 displays data graphed by session number in which the nonconcurrent start is not represented on the graph. Figure 2 displays data by calendar date in which the nonconcurrent start can be seen, and the distance between each data point indicates the temporal space between the two sessions. Each graph represents a different way to capture the temporal nature of the sessions, while both graphs allow readers to conduct vertical analysis. Presentation of both graphs concurs with NCMB reporting guidelines, which suggest clearly showing nonconcurrence on graphs by including the dates on which each tier’s data points were collected and/or adding session numbers and describing nonconcurrence on the figure (Carr, 2005; Kratochwill et al., 2022; Ledford & Zimmerman, 2022).
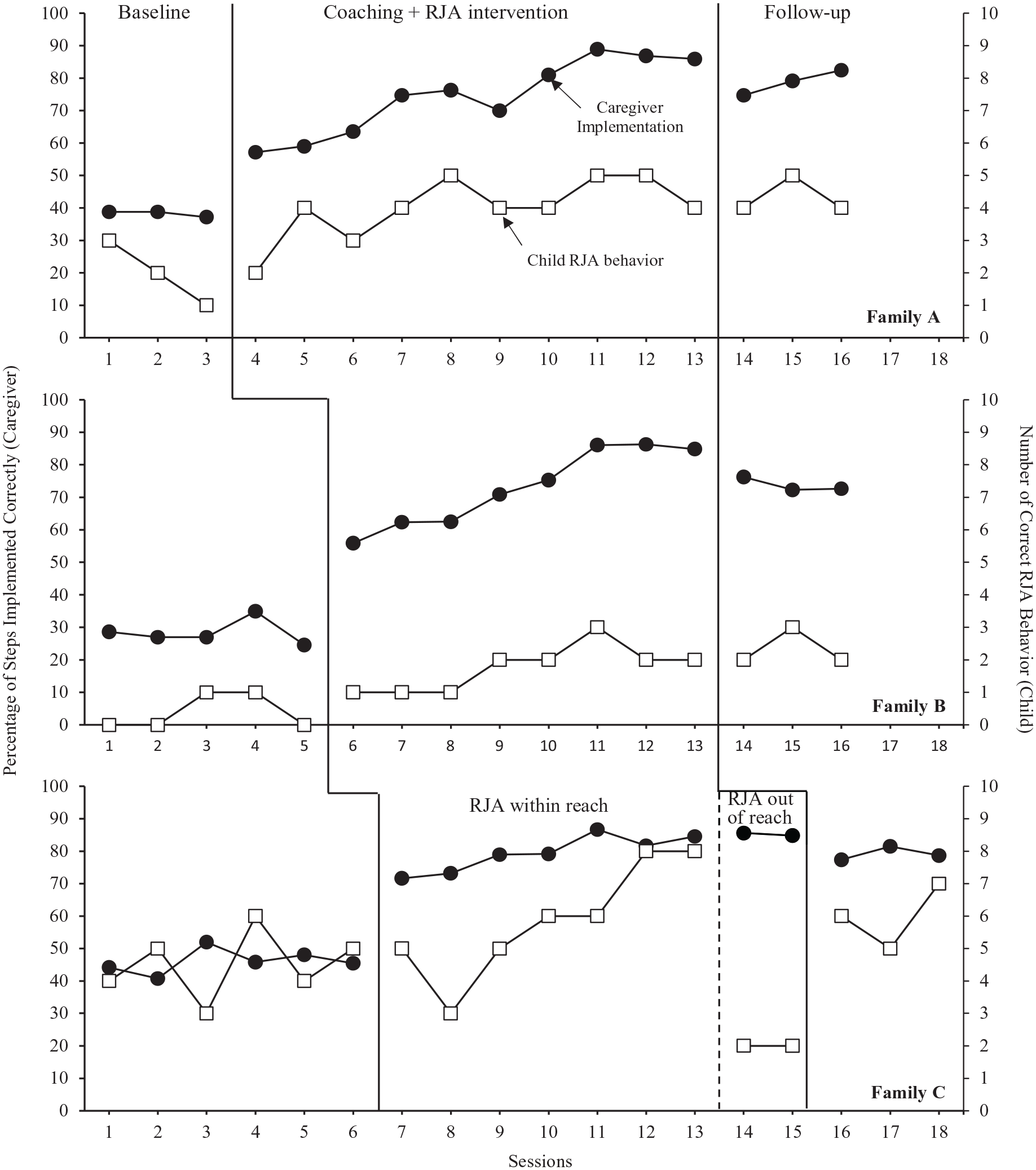
Percentage of steps implemented correctly by the caregivers and the number of correct RJA behavior by the children.
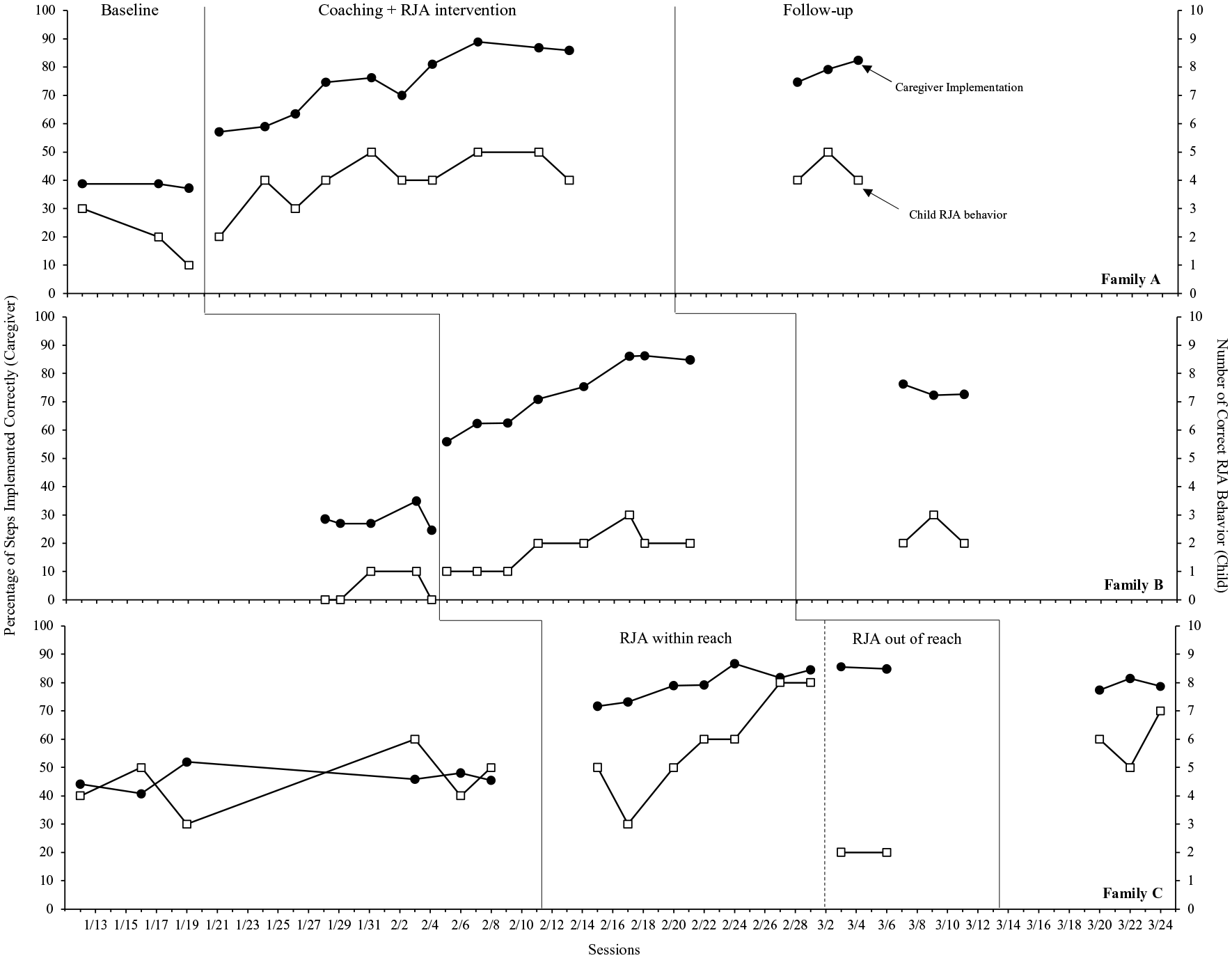
Percentage of steps implemented correctly by the caregivers and the number of correct RJA behavior by the children.
Caregiver RJA Intervention Implementation Accuracy
The primary aim of this study was to determine whether caregivers can accurately implement RJA intervention procedures with their toddler-age child with autism in home settings. As shown in Figure 1, there was an immediate increasing trend and subsequent increase in level with no overlap with baseline conditions upon introduction of the caregiver coaching across all three caregivers. During baseline, the percentage of steps implemented correctly was less variable, with low levels ranging from 30% to 50%. Despite behavior therapists participating in online training sessions during caregivers’ baseline data collection, caregivers’ implementation of the intervention remained stable. For all caregivers, an increasing trend with a high level of correct implementation was observed immediately after caregiver coaching was provided, and the data were stable. The percentage of correct implementation reached over 85% (mastery), with Caregiver A performing 89% of steps correctly starting in the eighth coaching session, Caregiver B performing 86% of steps correctly in the sixth coaching session, and Caregiver C performing 85% of steps correctly starting in the fifth coaching session. Caregiver implementation of RJA to items out of reach depended on the child’s RJA behavior. Caregivers A and B did not have the opportunity to move to the next phase of the RJA intervention as their toddlers did not meet the criteria. Caregiver C was asked to implement RJA to items out of reach intervention for sessions 14 and 15; implementation accuracy remained at a high level, ranging from 82% to 79%. Coaching sessions were terminated when caregivers reached 85% accuracy in three consecutive sessions. A functional relation between caregiver coaching and caregiver correct implementation of RJA intervention was established with consistent increases in correct RJA intervention implementation when and only when coaching was implemented across all three coach–caregiver–child dyads.
During follow-up conditions across all three caregivers, the percentage of RJA intervention procedural steps implemented correctly was consistently lower than the final mastery criterion but consistently higher than baseline levels. All three caregivers’ implementation accuracy in follow-up conditions ranged from 73% to 82%.
Child RJA Behavior
The secondary aim of this study was to determine whether caregivers’ implementation of RJA intervention would result in changes in the RJA behavior of the toddler-age child with autism measured by the number of correct responses to caregivers’ 10 consecutive trials of RJA intervention. The items used in the RJA intervention were selected based on the caregivers’ report of the child’s preferred toys or items, and an informal preference assessment was conducted every 2 weeks for each family. As shown in Figure 1, children with autism had dissimilar levels of RJA behavior during baseline conditions. Child A displayed a decreasing trend in the number of correct responses to JA bids from 1 to 3. Child B remained at a low level in the number of correct responses to JA bids, ranging from 0 to 1. Child C’s data were variable in the number of correct responses to JA bids ranging from 3 to 6. During caregiver coaching and RJA intervention conditions, all three toddlers’ RJA behavior improved and showed an increasing trend with some variability in Child A and Child C data. All three had a few overlapping data points between the RJA intervention condition and baseline; the level was higher than the baseline and showed an increasing trend. Only Child C reached the criteria to move to RJA to items out of reach phase of the intervention procedure from RJA to items within-reach intervention (i.e., 80% correct responses in two consecutive trials). Following the implementation of RJA to items out of reach intervention, Child C’s number of correct RJA behaviors decreased immediately from 8 to 2.
During follow-up conditions, levels were more variable and similar to those in the caregiver coaching and RJA intervention conditions but higher than baseline conditions across three toddlers. Child A and B’s follow-up condition data did not overlap with baseline, with less variability ranging from 4 to 5 for Child A and 2 to 3 for Child B. Child C’s follow-up condition data overlapped with the baseline condition and was more variable, ranging from 5 to 7.
Social Validity
All three behavior therapists found online training highly beneficial and expressed confidence in coaching caregivers on RJA intervention procedures. While usage of caregiver coaching varied before and after the study, all therapists expressed intent to continue using BST caregiver coaching in their practices. Likewise, all three caregivers reported consistent satisfaction with caregiver coaching and expressed they would like to continue implementing RJA intervention at home and recommend this practice to other families (see Appendix C).
Discussion
The purpose of this study was to examine the effects of caregiver coaching using the BST model on the caregivers’ RJA intervention implementation. Secondarily, we assessed whether caregivers’ intervention implementation changed the RJA behavior exhibited by their toddlers with autism. Prior to behavior therapists coaching caregivers on RJA intervention implementation, they received online training from the first author. The coaching practices behavior therapists used for caregivers included pre-coaching (i.e., didactic teaching and modeling on the specific procedural steps and intervention techniques), coaching (i.e., rehearsal and feedback), and follow-up sessions. Similar to Schertz et al. (2013) and Prelock et al. (2011), caregivers learned to implement RJA intervention with their toddler-age child with autism at home accurately and independently after they received coaching from their behavior therapists. Only after 5–8 coaching sessions, which took less than 3 weeks across all participants, did caregivers implement with high fidelity. Less frequent and shorter coaching sessions needed for caregivers to accurately implement the intervention could be attributed to the strong relationship built between the caregiver, child, and the behavior therapist before the study (Amsbary et al., 2021). In addition, by doing preference assessment, caregiver coaching, and caregiver-implemented intervention within the families’ most familiar environments, it likely made it “easier for caregivers to apply newly learned teaching skills to their children across daily home routines and activities” (Brown & Woods, 2015). Consistent with previous findings on JA interventions (Meindl & Cannella-Malone, 2011; Paparella & Freeman, 2015), toddlers with autism demonstrated positive changes in their RJA behavior contingent upon caregivers’ implementation of the intervention. A functional relation between caregiver coaching incorporating the BST model and caregiver correct implementation of RJA intervention was established, with consistent increases in correct RJA intervention implementation contingent upon the delivery of coaching across all three coach–caregiver–child dyads.
The results of this study provide preliminary evidence caregivers can learn to implement RJA intervention at home using different items available in a typical environment for their toddler-age child with autism. Caregivers received individualized coaching from behavior therapists for five to eight sessions, 25–42 minute per session, to reach mastery criteria. Effective coaching strategies, including instructions, modeling, rehearsal, and feedback (i.e., BST model), were used to teach caregivers about the RJA intervention procedures during their typical home visit sessions. The RJA intervention implementation skills were added to preexisting parent training goals, suggesting caregivers were able to focus on multiple strategies during a relatively short period of time. It is possible that the use of the BST model as an evidence-based caregiver coaching strategy (Schaefer & Andzik, 2021) was responsible for caregivers’ immediate intervention implementation behavior change. Additional research is needed to determine the appropriate amount of caregiver coaching dosage that is feasible and effective for behavior therapists and caregivers, which leads to positive caregiver and child outcomes.
Although the overall outcomes for toddlers with autism RJA behavior were positive and replicated across tiers, change in child behaviors was minimal and less immediate than caregiver implementation behavior change. While we expected a delay in child behavior change compared to adults’ behavior change (Ledford et al., 2017; Windsor et al., 2019), the frequency of RJA behavior for all three children approximately doubled or tripled in frequency compared to the baseline condition. However, only Child C met the RJA intervention phase change criteria (i.e., 80% correct response) and was taught RJA to items out of reach. When RJA to items out of reach intervention was implemented by the caregiver, the child’s RJA behavior decreased immediately. In a previous study on teaching RJA using items within and out of reach to toddlers with autism, 65%–95% of correct child response was reported as a result of 70 to 95 sessions of intervention delivery. In the current study, however, the condition change decision depended on caregiver implementation behavior, and thus, only five to eight intervention sessions were conducted, which may not have been sufficient to expect a greater increase in the frequency of children engaging in RJA behavior. Further studies determining whether caregivers’ continuous implementation of the RJA intervention across daily activities will lead to the mastery of RJA behavior for toddler-age children with autism are warranted.
Four online training sessions on RJA intervention techniques and caregiver coaching strategies were sufficient for each behavior therapist to coach caregivers on RJA intervention implementation with high fidelity. Verbal and written instructions and video modeling strategies used to train behavior therapists via online format may have contributed to behavior therapists’ effective and efficient learning on RJA intervention and coaching practices. However, research outcomes on professional development and training are mixed. For example, some researchers suggested short-term professional development was ineffective for educator behavior change (Dunst et al., 2015), while others argue that despite the short coaching duration, a sufficient number of opportunities for practice and feedback may lead to immediate behavior change of professionals (e.g., Ledford et al., 2017; Sarokoff & Sturmey, 2004). Additional research is needed to explore which coaching strategies are feasible and effective across different training formats for professionals who are diverse in their expertise and prior experiences.
Individual differences in social communication development might explain the variability in RJA behavior outcomes across toddlers with autism. Caregiver coaching and the RJA intervention were personalized and individualized based on their preferences and/or needs. For example, the prompting procedure used in the intervention procedure was selected by the caregivers’ report on what they prefer and what has been effective for them during their interaction with the child during their typical routines and activities at home. Both coaching and intervention occurred in home settings utilizing items that are typically available and preferred by the child. It may be possible that although these individualized approaches are facilitators of successful EI outcomes, each child’s developmental differences and characteristics are the main factors that may determine the frequency and duration of the intervention needed for the child to master the RJA skills. Future research may focus on investigating whether the variable outcomes could be addressed with a more systematic individualized approach or whether some toddlers require continuous opportunities to practice newly acquired skills across daily routines/activities at home.
Data collection on both behavior therapists’ coaching fidelity and caregivers’ RJA intervention implementation fidelity increased confidence in considering child characteristics as variables that may have contributed to the toddlers’ RJA behavior change. The purpose of caregiver-implemented intervention is to enhance caregivers’ capacity to teach their child and in turn, result in the child’s improved development and learning (Powell & Dunlap, 2010). Given that high-fidelity implementation of effective caregiver coaching practices and high fidelity of effective intervention are required to have positive child outcomes (Barton & Fettig, 2013), all future studies should measure and report coaching fidelity and intervention fidelity in caregiver-implemented intervention research.
Limitations
The results of the current study should be considered in light of several limitations. First, the duration of intervention was relatively short across caregiver–child dyads. While five to eight sessions were sufficient for all three caregivers to acquire and maintain RJA intervention implementation skills for three consecutive sessions, additional opportunities and longer duration of interventions might have resulted in the mastery of RJA behavior for toddlers with autism. Second, data to suggest a generalization of caregiver and child outcomes across multiple routines and activities in a typical setting are limited. Although caregivers selected the intervention setting within the home environment based on their preferences and needs every session, settings such as the kitchen or bathroom were not included. However, it may be important to assess the generalizability of caregivers’ implementation of RJA intervention and toddlers’ engagement in RJA behavior in such settings, given the necessity of children’s RJA skills during mealtime and care routines. Third, although follow-up session data were promising, data were collected after a short period of time upon intervention termination (i.e., after 2 weeks). Data collection after a longer delay may allow stronger evidence of the long-term effect of caregiver coaching and caregiver-implemented RJA intervention.
Conclusion
The results of this study indicate that caregiver coaching to improve caregivers’ capacity to implement RJA intervention in home settings for their toddlers with autism is an effective approach for caregivers to independently implement the intervention with high fidelity and for children to engage in more frequent RJA behavior. Caregivers were able to master the RJA intervention implementation skills after five to eight coaching sessions spanning approximately 3 weeks for each caregiver. Although children’s engagement in RJA behavior varied across three toddlers with autism, all three doubled or tripled in the frequency of the correct RJA behavior. Results suggest that caregiver coaching using the BST model may be an efficient approach that can improve endogenous individuals who may be spending the most time in the child’s routine interacting and providing support. Given the importance of supporting families of young children with autism and adequately supporting those children within the context of a typical environment to promote their early social-communication skills (e.g., JA behavior), the caregiver coaching using the BST model examined in this study holds promise as a method to improve the capacity of families and development of children.
Supplemental Material
sj-docx-1-tec-10.1177_02711214241255045 – Supplemental material for Coaching Caregivers to Teach Responding to Joint Attention for Toddlers with Autism
Supplemental material, sj-docx-1-tec-10.1177_02711214241255045 for Coaching Caregivers to Teach Responding to Joint Attention for Toddlers with Autism by Gospel Y. Kim, Kathleen N. Tuck, Elisabeth J. Malone and Kathryn M. Bigelow in Topics in Early Childhood Special Education
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.