
Abstract
Early intervention (EI) services—including but not limited to speech, physical, occupational, and mental health therapies—have been proven to significantly benefit young children’s development, shaping their readiness for school and offering pivotal support for caregivers. However, racial disparities persist in identification for and access to EI services. Little is known about the ways in which racism affects how caregivers experience and navigate the screening and EI referral process. Through in-depth qualitative interviews, we explored the experiences of nine minoritized caregivers with experience seeking EI services in the San Francisco Bay area of the United States. Using Critical Race Theory, we investigated how caregivers are racialized in the process. Our findings elucidate mechanisms of racialization, including but not limited to provider bias, managing stereotype threat, and dismissal of caregiver concerns. We also highlight ways in which such racialization contributes to disparities in who receives EI services. Understanding how this process racializes its users will elucidate pathways of change toward a more equitable system, in which minoritized children receive screening and early intervention services in a timely and appropriate manner.
Keywords
Early childhood offers a critical window to support children’s language, socioemotional, motor, and cognitive development (Shonkoff, 2003). Early identification of children’s developmental and behavioral needs—such as language delays or sensory challenges—and matching them to appropriate early intervention (EI) services—such as speech, occupational, physical, or behavioral therapy—has been shown to result in significant developmental gains from birth through the age of 5 years (Law et al., 2003). It also provides pivotal support for families, offering reassurance to caregivers that their child’s needs are being met (S. Jones et al., 2017). Eligible children have protected rights to EI services through the Individuals with Disabilities Education Act (H.R.1350—108th Congress, 2004), which secures federal funding for implementation of EI programs for children with developmental delays.
While there are many routes a family can take to reach EI services, the overall process generally consists of screening, referral, evaluation, and placement in EI services. We hereon refer to navigation of these steps as the “EI process.” EI services can be provided by an array of entities, including but not limited to, private providers, Regional Centers or other birth-to-3 systems, schools, and healthcare providers. Many families access services in partnership with their child’s pediatric provider. The pediatric primary care clinic plays a crucial role in screening for developmental-behavioral delays and referring for further evaluation or directly to services.
Racial Disparities in EI
Racial disparities exist within the field of EI and have been attributed to inequitable social structures (Boone Blanchard et al., 2021). For example, in studies that focused on autism spectrum disorder (ASD), Black and Latinx children have been historically less likely to be identified with ASD (Maenner et al., 2020). Current studies also show that when Black and Latinx children are identified, it is at a later age than White children (Barnard-Brak et al., 2021; Mandell et al., 2002, 2009; Romo et al., 2023). Some studies have shown that minoritized 1 children are less likely to be referred to EI services (Barfield et al., 2008; McManus et al., 2020). Once identified, minoritized children are underrepresented among participants enrolled in EI (Evans et al., 2016; Feinberg et al., 2011; Gallegos et al., 2021; Liptak et al., 2008; Magaña et al., 2016; D. M. Magnusson et al., 2017; Morgan et al., 2012; Romo et al., 2019; Rosenberg et al., 2008; Shenouda et al., 2022; Zuckerman et al., 2013, 2017), and are more likely to receive services in more restrictive settings (Meek et al., 2020). Given the racial achievement gap within the U.S. educational system (Gwartney, 1970), and the promise of EI in enabling both short and long term success in school, ensuring equitable access to EI is crucial.
Contributors to Racial Disparities in Diagnosis and Service Access
Researchers have identified structural barriers that contribute to disparities in EI identification and subsequent service reception. Several studies have highlighted disparities in the context of ASD in particular. Zuckerman et al. (2014) describe how lack of access to quality primary care among minoritized children may contribute to such disparities. This same pattern holds true when considering access to specialty care where developmental conditions are often further evaluated (Gillispie, 2021; Zuckerman et al., 2014). Language barriers throughout the screening, evaluation, and referral process have been cited as a contributing factor for some families (Cycyk et al., 2022; Stahmer et al., 2019; Williams et al., 2013; Zuckerman et al., 2017), as has the cultural relevance of screening and assessment tools and their application to children from minoritized backgrounds (Zuckerman et al., 2014).
Studies investigating minoritized family perspectives on the EI process highlight the ways in which their attitudes, beliefs, or behaviors differ from those of White families. For example, some have suggested that minoritized caregivers might have different beliefs around what is considered atypical development (Blacher et al., 2014; Cohen & Miguel, 2018; Norbury & Sparks, 2013). Other studies suggest that minoritized caregivers may prefer to wait for children to develop in their own time (Jimenez et al., 2012; D. M. Magnusson et al., 2017) or not believe that their child has a developmental diagnosis (Azad et al., 2022; Pearson et al., 2020). Research also highlights racial/ethnic differences in help-seeking for children outside of familial or social circles (D. M. Magnusson et al., 2017). For example, minoritized caregivers might be more likely to rely on social networks rather than physicians to inform whether or not to seek services (D. M. Magnusson et al., 2017; Zeleke et al., 2019). Several studies highlight mistrust of health systems (Dababnah et al., 2018; Zuckerman et al., 2017), and negative experiences with healthcare providers, where families’ concerns are dismissed (Dababnah et al., 2018; Pearson & Meadan, 2018; Stahmer et al., 2019). Other themes that have surfaced include stigma around disability 2 (Dababnah et al., 2018; Evans et al., 2016; Rivera-Figueroa et al., 2022; Stahmer et al., 2019), limited comprehension of EI policy and services (Evans et al., 2016; D. M. Magnusson et al., 2017), and confusion around EI systems of care (Stahmer et al., 2019).
These studies allow us to understand the ways in which different minoritized groups might have unique attitudes and experiences when it comes to EI. While racism operates in different ways, the aim of this study is to examine across minoritized groups—rather than comparing between groups—in order to understand how racialization 3 occurs more comprehensively. Instead of situating race as a predisposing factor to be analyzed, we aim to center the process of racialization. To our knowledge, research that examines the experience of racism in the EI process is limited. A few studies have documented how provider bias and racial microaggressions are experienced within the context of seeking EI (Dababnah et al., 2018; Gourdine et al., 2011; Lovelace et al., 2018). Our aim is to expand upon this foundation, and to understand whether and how minoritized caregivers perceive their process as racializing.
Anti-Racist Framework
Critical Race Theory (CRT) allows us to examine the ways in which racism is central in driving disparities (Ford & Airhihenbuwa, 2010). CRT is a framework and methodology originating from legal studies that is now more widely used in public health to better elucidate and challenge the root causes of health disparities (Ford & Airhihenbuwa, 2010). CRT emphasizes how race is socially constructed, and often erroneously used as a proxy for racism.
The purpose of this study is to use the CRT lens to explore how caregivers are racialized, and how such racialization leads to a delay in the EI process. We used a qualitative approach to understand and elevate the experiences of minoritized caregivers of children who participated in EI. Through qualitative interviews, we explored the following questions: (1) How does the process of accessing EI services racialize minoritized caregivers navigating it? (2) How do minoritized caregivers perceive racism as impacting their experience of the process?
Method
Setting, Recruitment, and Eligibility
All research procedures, including participant recruitment, were conducted in the San Francisco Bay Area, an urban setting with a diverse population and a large number of EI organizations. The University of California at Berkeley Institutional Review Board approved the protocol, with a Memorandum of Understanding with the University of California San Francisco. We used a purposive sampling strategy to recruit minoritized caregivers who had experienced—or were experiencing—the EI process (Kelly, 2010). We advertised through flyers posted in EI community organizations, primary care clinics, and on online social media platforms (i.e., caregiver support groups on Facebook). Flyers were posted in English and Spanish, in line with language capabilities of the research team. Participants contacted the research team if they were interested based on flyer information. Participants were eligible if they (1) were over the age of 18 years, (2) self-identified as racially minoritized, (3) had a child who received or was receiving EI services, and (4) spoke either English or Spanish. We did not set limits on how long ago the child participated in EI to allow for broader participation and given the limited literature on EI outcomes across time.
Data Collection Procedures
We chose in-depth interviews as our primary method of data collection in order to elicit participants’ narratives over the EI process, and surface the meanings connected with them. Researchers called interested participants to screen for eligibility, explain the study purpose and procedures in detail, and ensure participant understanding. After establishing informed consent, participants engaged in a one-on-one Zoom video interview with a researcher. Each participant was interviewed two separate times, each interview lasting approximately 1 hour, for a total contact time of 2 hours. The research team offered participants support with Zoom as needed. Participants received a $25 gift card for each interview to compensate for their time.
Interview topics were created in partnership with two community members—an EI Program Manager and an EI Resource Navigator—who self-identified as racially minoritized. Interviews were semi-structured, beginning with open-ended questions to allow participants to guide the conversation toward experiences that were important to them. Interviews covered the following topics: (1) experiences seeking EI services, (2) barriers and facilitators in the process, and (3) reflections of how racialized identity impacted the experience (see Appendix A).
As part of our methodology, we sought to center lived experience in a manner that included participants in the process of knowledge production, rather than treating subjects as objects of study. To achieve this, we used an approach called Black Feminist Epistemological Methodology, originally developed by James (2021), and grounded in the work of Black women scholars and the larger body of knowledge known as Black Feminist Thought. This entailed conducting a second interview with each participant, where the researcher read a written summary of the first interview to the participant, and gave the participant space to correct, validate, or contradict the researcher’s summary. This allowed the second interview to be a dialogue, in which participants had the opportunity to interact with their own data and have a sense of how they would be described in our writing. This collaborative approach not only ensured accuracy of findings—as a form of member checking—but ensured transparency of research findings with participants.
Participants
Nine participants were recruited, and eight participated in two interviews, with one person lost to follow up after the first interview. Eight interviews were conducted in English, and one in Spanish. Details about participants and their children are summarized in Table 1 (see Supplemental Table also). All children received some form of EI, with several still receiving services. Five participants had an initial concern about their child’s development and sought support through the EI process. Most started at the pediatric office, with one person self-referring to their local Regional Center, an agency contracted by California’s Department of Developmental Services to coordinate services. The remainder of participants did not have an initial concern but were told by a teacher to have their child assessed or had a positive screening in the pediatric office. For most families, EI services were accessed through the medical or Regional Center system, and once children turned three, they received services through their schools’ Individualized Education Program (IEP) system. Four children were patients of Kaiser Permanente, which offers therapeutic services within its own system. Two families reported paying for private services at some point within the EI process. The average time from initial concern to EI service reception varied greatly as each family had a unique path within the process, with some families receiving services within 1 month and others waiting years. Three participants had children currently between the ages of 15 and 20, and thus had experienced the EI process several years ago. These participants were included in the study because although EI services and resources have evolved over time, research has shown that racialized experiences of care have not meaningfully changed in that time (Boone Blanchard et al., 2021).
Demographics of Interview Participants (N = 9).
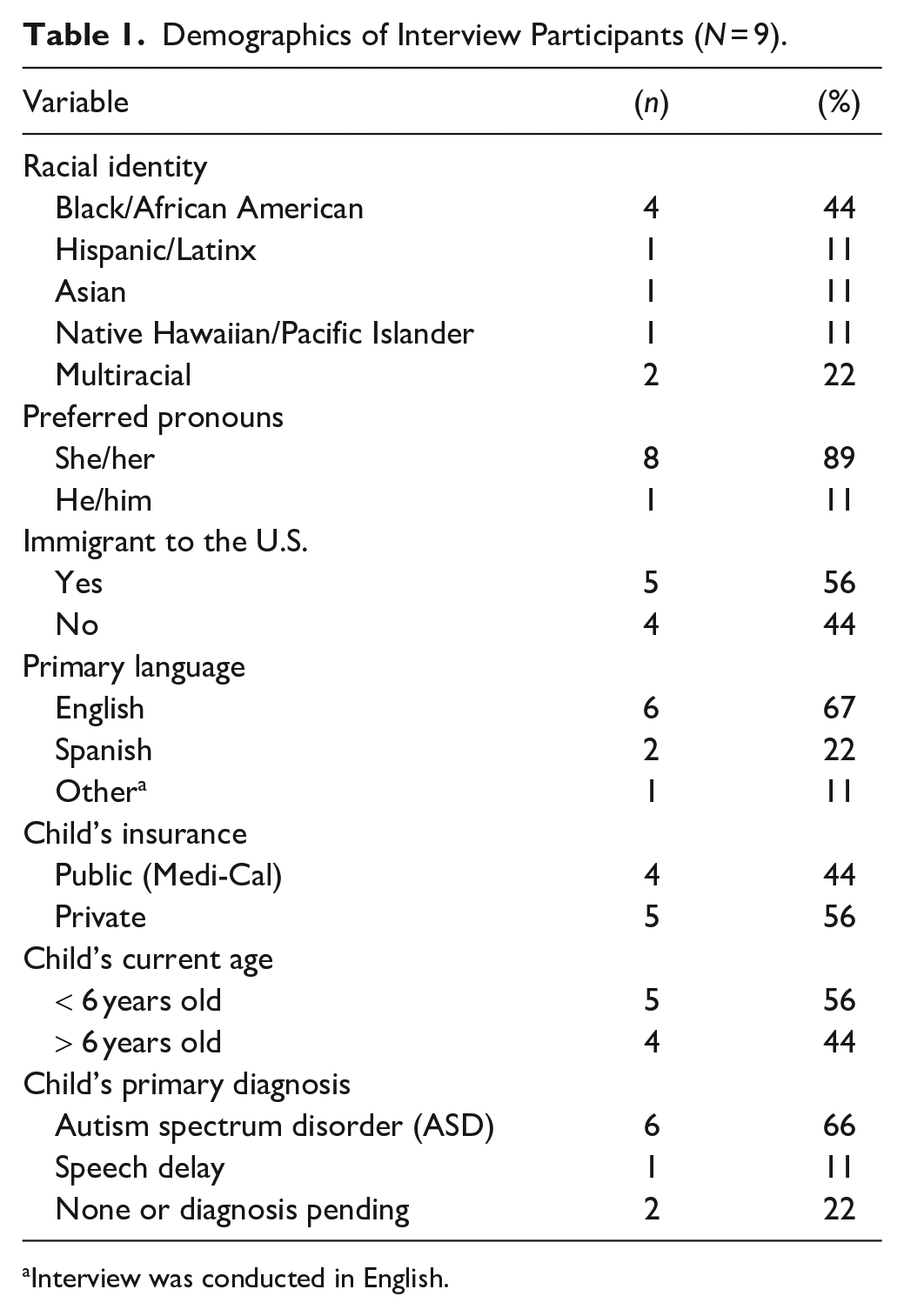
Interview was conducted in English.
Data Analysis
Audio recordings were transcribed through a professional transcription service. Spanish transcripts were translated to English by a member of the research team for whom Spanish is a native language. To ensure the accuracy of all transcripts, a research assistant compared each transcript to its corresponding interview and corrected any discrepancies. Transcripts were uploaded to the Dedoose qualitative data analysis program.
In order to ensure rich understanding of the data through conversation and consensus building, multiple coders were recruited. The coding team consisted of three researchers with training in qualitative analysis, two of whom had deep familiarity with the EI field. Through an inductive process (Pawluch & Neiterman, 2010), the lead researcher performed initial open coding of all transcripts, developing a preliminary codebook guided by the study’s research questions and supported by a thorough review of the literature. Initial open coding generated a list of 30 codes (e.g., “provider dismissal of concern,” “caregiver persistence”). After the other two coders reviewed the transcripts, the team further revised the codebook through group discussion and consensus. This process was repeated until a more finalized codebook was created, consisting of 22 codes. After this step, two members—a primary coder and a secondary coder—analyzed each transcript line by line. On a weekly basis, the team met to discuss the data, reconcile through consensus building, and adjust any discrepancies in coding. Code reports were generated, and corresponding data viewed in depth. Themes were generated using axial coding to group codes into larger categories. The final manuscript was reviewed by one participant and digitally shared with all participants.
With regards to our positionality to this work, two of us are Black (JJ, KM), three from other racially minoritized backgrounds (JA, AG, JM) one biracial (JC), and one White (SMH). While all of us have lived experiences that have shaped our relationships to racialization and ableism, only one team member has lived experience navigating the EI process. This brought to us an awareness of the inherent position of power we occupied in the research process as researchers or academics—lacking lived experience of the phenomena—seeking knowledge from participants, especially in consideration of the extractive dynamic that has historically existed between research institutions and marginalized groups. We used Black Feminist Epistemological Methodology, with the aim of centering the lived experience of participants and creating a collective dialogue, in order to bring participants into the analytic process as an attempt to intervene upon the power imbalance.
Findings
We sought to examine the nature of racialization among participants seeking EI services, based on stories shared. Specifically, we inquired: (1) How does the process of accessing EI services racialize minoritized caregivers navigating it? (2) How do minoritized caregivers perceive racism as impacting their experience of the process?
Though several participants reflected directly on ways in which racism impacted their experience, others did not identify racism as part of their experience. Understanding that racialization can be silent, unnoticed, we used the lens of CRT examine how even these experiences might be racializing. We explore our two research questions using five themes to capture mechanisms of racialization and examine how minoritized caregivers perceive racism as impacting their experience of the process: (1) Caregivers experienced dismissal of their concerns, (2) caregivers were made to feel like a burden on the system, (3) caregiver perceptions around provider bias, (4) racial bias led to dismissal and differential care, and (5) reactions of caregivers: stereotype threat and avoiding systems. We use “provider” broadly—unless otherwise specified—to capture any clinician, assessor, or direct service provider within the healthcare, Regional Center, or school systems.
Caregivers Experienced Dismissal of Their Concerns
Several families shared instances in which their concerns were dismissed by providers. Caregivers described medical visits in which they were told that the child would “grow out of it” or that the caregiver should “wait.” For example, when Angela—a Filipina preschool teacher passionate about early childhood education—went to her pediatric provider concerned about her son’s lack of speech at the age of two, she was told to wait and denied her request for a speech therapy referral: “then nothing, 12 months came still nothing. So that’s when I told the doctor, ‘He’s not saying anything clear. He is kind of verbalizing, but there’s no clear words, and that concerns me’ and the doctor said, ‘no, you know what, it’s going to come.’ But that’s not what I wanted to hear. . .” This experience aligns with those of several other families who came to their pediatric provider with speech concerns and felt that their concerns went unheard.
Deborah similarly experienced dismissal in seeking services for her son, whom she suspected had ASD. Deborah identifies as Black, has a PhD in psychology, and works with clients with a wide range of developmental disabilities. Reflecting on her experiences speaking with various providers and evaluators within the Regional Center system, Deborah shared: “each time when I requested autism testing, I was told that he didn’t look like he had autism and so they didn’t see it as being necessary.” Deborah further lamented the lack of dialogue that occurred in those visits: “Why would you talk to someone who specializes in the field and say to them just rather flippantly, ‘he doesn’t look autistic.’ Why wouldn’t there even be a curiosity, like, ‘tell me what you’re thinking, tell me why do you think that, or what’s going on, or what’s been your journey, or have you had it looked at,’ just anything. Dialogue. Make it a two-way conversation.” This quote touches on a desire shared by many caregivers to be in partnership with their provider and have a conversation about their concerns.
Indeed, in instances where caregivers spoke positively about providers, it almost always centered around feeling like the provider acknowledged their concern and trusted their perspective. For example, Angela described interactions with a new pediatric provider that she continued seeing for years: “[the doctor] will sit down and ask, ‘how’s it going? How’s it really going?’ And so I just share with her how it’s really going. And then she’ll say, ‘okay, great’ or ‘let me know if that doesn’t work and we’ll figure something out’. It’s just, there’s follow up with her.” For Angela, she appreciated being able to share her experiences caring for her son and the challenges she encounters. She continued to describe how she felt supported by her pediatric provider and trusted that the provider would follow up on any next steps that they decided on together when it came to her son’s EI supports.
Caregivers Were Made to Feel Like a Burden on the System
Participants reported instances of being told that they were asking for too much, or where they felt their motivations behind seeking support from the EI system were questioned. Almost all caregivers touched on the need to be persistent in advocating for themselves when it came to accessing referrals, evaluations, or services. This would often take the form of multiple phone calls to push a referral along, or seeking support from multiple providers.
Seeking Referrals
After her son had “red flag concerns for ASD” following a screening interview, Leticia had a difficult time scheduling a subsequent evaluation appointment. She described her experiences calling and asking the medical clinic to make the referral: “And then every time you ask for the referral, they don’t like it. They keep saying, ‘you keep asking for a referral, you ask for a lot of referrals compared to our other patients.’. . . I mean, I am not asking just because I’m playing or just because I want to see the doctor and have fun. I’m asking because I’m trying to help my child get treatment.” Leticia further described how the pediatric office made an error in sending the referral. When she called, she felt like the office was ignoring her: “‘Please, can you do it?’ No, she just ignored me. To this day I didn’t get it.” This exemplifies how caregivers describe feeling ignored or deprioritized when following up with referrals.
Other caregivers shared this perception that providers were hesitant to make referrals. For Angela, she recalled: “I asked him, ‘can I get a referral?’ They said, ‘I could, but then it would take a long time.’ It didn’t seem like they wanted to go through the trouble.” Though the referral process often does take a long time, in this case the timeline might have been extended because—as perceived by Angela—the provider didn’t want to initiate the referral.
Seeking other providers
When it came to seeking opinions from other providers, some caregivers felt that this was negatively perceived by others as unnecessary. Sarah, a Black mother of a 4-year-old son with ASD, reflected on this: “If I go from pediatrician to pediatrician, looking for a different answer, well they can all see the same notes. And after a while it’s gonna look like, ‘oh, you’re just fishing for answers until you get what you want.’ Not, ‘you’re a concerned caregiver who’s looking for a doctor who’s willing to listen and help.’ It’s like, ‘oh, she’s just fishing for what she wants to hear.’”
Participants had a perception that staff didn’t like how they were “pushing” for referrals, or just “fishing” for what they wanted to hear. This aligns with racial stereotyping of minoritized people as trying to take unfair advantage of systems. Deborah shared a similar experience: “And it, and it felt like I was being accused of doctor shopping to be able to hear what I wanted to hear as opposed to try[ing] to find a professional who would just listen, period.” Deborah further recalled overhearing Regional Center staff accusing her of trying to “game the system”: “and those were the kind of things that I heard like, ‘she’s back again, trying to get a service. . . It’s a Black family. She must be trying to get an extra foster care bump or something.’”
Caregiver Perceptions Around Provider Bias
Throughout the process, caregivers perceived that bias led providers to make assumptions about a caregiver’s socioeconomic, education, language, literacy, or immigration status. In a few instances, caregivers felt like their concerns weren’t taken seriously because providers assumed the caregiver needed to change a behavior or practice at home first.
Isabel is a bilingual, multiracial mom who self-referred to the Regional Center when her son’s speech stopped progressing around the age of 2. There, she described the bias she perceived: “When they see that [I speak Spanish], I think they don’t see beyond because I felt sometimes that they only saw an immigrant coming here, and for some people it’s like, ‘oh, they came illegally’ or things like that.”
Isabel went on to describe an experience she had with a Regional Center case manager: “Well, he was a little condescending, as if he was doing me a favor. It was unprofessional. For example, he said, ‘Oh, don’t worry. You’re going to receive a bill, but it’s not for you to pay. We’re taking care of that.’ But it was the tone of voice, or it was as if we couldn’t afford that quantity of money or whatever, but was just the way that he presented himself. I didn’t like it.” In this example, the provider assumed Isabel was from a lower socioeconomic class than she actually was, in part because she spoke Spanish. There was also an underlying implication that she sought to benefit from the system without paying for services.
Isabel continued to describe how bias around her language status delayed her EI process: “they see you and think ‘she doesn’t speak English’. . . I can fully understand what you’re saying, but that, that was a struggle with [the Regional Center], pushing for some [interpretation] service that we did not request . . . . .” The consequence of this, she perceived, was that it took longer to schedule her appointment because they had to wait for an interpreter to be available, which delayed their timeline. Now, she knows to explicitly ask not to have an interpreter “because I know that delays the process.”
Assumptions that caregiver behavior or practice contributed to developmental need
Some caregivers reported experiences in which providers responded to their concerns by recommending that the caregiver change certain behaviors or practices. This phenomenon specifically applied to bilingual or non-English speakers, who were encouraged to alter their language practices at home. Leticia—a multiracial mother who arrived at the pediatric clinic with concerns about her son’s speech—recalled being told: “for five months, you need to talk only in English. Don’t talk other language with your child. Just talk in English. Even if someone comes to your home: father, mother, sisters, grandmother. . . everybody needs to talk in English.” For Leticia, her son’s speech regression was later found to be a symptom of ASD, and not due to multiple language exposure. Despite evidence that dual language exposure does not lead to language delay, Leticia was given advice to only speak English at home. This raises the question of the extent to which speech delays are not caught in a timely manner due to provider perceptions around multiple languages spoken at home and impacts on speech development.
Sarah shared her perception of how providers were more likely to assume that the caregiver wasn’t doing something right. While seeking out occupational therapy for her son from the school district, Sarah recalled a conversation with the assessor: “If I say, ‘my son doesn’t wanna eat that.’ ‘Well, you need to teach him to eat healthy foods.’ It’s always bounced back on the caregiver to redirect their behavior.” Sarah’s perception reflected her concern that her son’s behavioral challenge was assumed to be due to something she was doing wrong at home rather than something requiring additional support and intervention.
Racial Bias Led to Dismissal and Differential Care
Dismissal of concerns
In reflecting on reasons for provider dismissal previously discussed, several caregivers perceived that racism played an important role. Angela explained: “if we were White, we would receive the services. [Providers] would be willing to listen to us more. They’d be willing to negotiate with us rather than telling us, this is what you need to do.” Angela went on to say: “I always had [racism] in the back of my mind.” For her, this showed up in the way in which she felt spoken down to during conversations around child development: “And then [the pediatric provider] talked to me using the big words for ‘early childhood education’ and not even like realizing maybe I work with kids too. Maybe I have an understanding. . .I think there’s the assumption, like you don’t really know [about child development], so I’m not going to explain it to you.” This highlights the way in which these caregivers felt they were perceived by providers in a way that decreased their credibility when it comes to their child’s development. To Angela, this bias explained the dismissal of her concerns.
Mary, a Black woman with a disability, whose son was diagnosed with ASD at age 16, also suspected that minoritized caregivers’ concerns might be more readily disregarded because of racial bias of providers. She summarized this phenomenon: “When a caregiver goes to the clinician for, if they suspect something, developmentally. . . usually the clinician will write off what the caregiver is saying and say ‘everything is fine’ and send the caregiver on their way.” Mary went on to connect this phenomenon with why minoritized caregivers receive diagnoses late: “Especially for Black caregivers, most of us are like, ‘why does it take so long for us to get that diagnosis?’ Cause it’s not taking as long for our White counterparts, but it takes almost a staggering amount of time, like years, to get the diagnosis that we believe our children have, especially if we suspect something specific.” As Mary views it, minoritized caregivers are not hesitant to seek help but rather the EI systems are less responsive to their help-seeking attempts.
Sarah, a Black mother of a 4-year-old son with ASD, also shared this sentiment: “If I were not a person of color, most doctors would value what I have to say, even if it’s a totally crazy theory. If I was a White mom and I said, ‘Hey, I think my child has ABC’ they would say, ‘okay, well, let’s get a referral, let’s get a specialist. Let’s do this.’ It’s like automatic action. But as a Black mom, I could tell them my kid has the same thing. You’re disregarded like, ‘mm, no, I don’t think so.’ And then, for a lot of time for our children, it comes too late.”
Differential care
A few caregivers felt that the bias of providers resulted in their children being held to different developmental standards within the diagnostic process compared to White children. For example, Deborah felt like her son did not meet diagnostic criteria due to providers’ assumptions that it was “normal” for Black children to not meet certain developmental expectations: Expectations for skills were lower. And so, he wasn’t perceived to have any problems. So, let’s say that if he was a kid from an environment where they felt like that there were more resources available, then there would be a lack of understanding as to why he hadn’t met certain benchmarks. But because he was in a Black family, then they were like ‘he’s doing good enough to be in a Black family. Like the expectations for his developmental trajectory was much lower. And since he met those lower expectations, then they were like ‘he’s fine. What’s your problem?’
Other caregivers similarly questioned how providers might consider “normal” differently for their children. For some, they felt that providers perceived certain behaviors to be due to “normal bad behavior” that is “expected” of minoritized children, rather than a product of developmental needs. Mary described her experience: It’s a clinician. . . who is like. . . ‘well I’m seeing this Black child. . .this is the way that Black children historically act’. So that’s their own bias, their own prejudice.” She further added: “It’s still being seen as ‘something is wrong with this child that is separate from their diagnosis.’ Why is it when there’s a White kid who has a diagnosis of autism, you have no problem with seeing like this behavior might be a result of their autism, but with a Black kid. . . it can’t possibly be a result of them having a disability?
Mary continued to express concerns that provider racial bias could result in a mislabeling of “emotional disturbance” in the education setting: “Why is it always Black children are seen as emotionally disturbed when. . . they have behaviors that are related to possibly having a developmental delay.” She continued to explain the implications of this labeling, or of having a developmental diagnosis that opens up opportunities for mislabeling as emotionally disturbed by the school system later on: “To have that label, then it means that a student could be possibly written off. . . That’s why a lot of caregivers don’t want the special education designation specifically, because historically it meant that most likely you were gonna end up in prison. Because that’s what happened, because those students became ‘unteachable’. So let’s just place them in a special education segregated classroom. . .”
While this parent expressed concern that racial bias might lead to a mislabeling, others were worried that provider bias could mean that the child would receive no diagnosis. For example, Isabel shared: “. . .And I would just sit there and wonder, how come it took us such a severe degree of autism for him to get services?” As this quotation suggests, minoritized children might have to present with more severe symptoms to meet the criteria for a diagnosis or services, because of the way they are perceived.
Reactions of Caregivers: Stereotype Threat and Avoiding Systems
Managing stereotype threat
In reflecting on the advocacy process, several caregivers revealed an awareness of how they had to adjust their behavior so as to not fulfill racial stereotypes, which is also known as managing stereotype threat (Spencer et al., 2016). Sarah summarized what this looked like for her: “I have a pediatrician, who’s a person of color, and I think if it had not been for him, listening to me, and not devaluing my opinions, cause as a woman and a woman of color, our opinions are always devalued. And if we kind of push for what we believe in, then we’re angry or we’re rude or, ‘she’s just another angry Black woman.’ So people don’t listen to you. And at first it kind of intimidated me, cause I was afraid to speak up or say what I didn’t like because I didn’t wanna be the angry Black woman, you know?”
Sarah further described how she was unsure about her son’s Individualized Education Program (IEP), but felt unable to advocate for changes during the IEP meeting: “So don’t give them a reason to think you’re an angry Black woman. Which sometimes just means having an opinion that people don’t like and so you tone it down simply because it has more consequences.” This exemplifies how minoritized caregivers might need to be more selective of how they advocate for themselves, if they disagree with the provider’s decision or have an opinion to share, for example. They might have to consider the risks of persistent advocacy, namely, fulfilling the stereotype threat and being treated accordingly.
Avoiding EI systems
Experiences of racial bias and dismissal made some caregivers not want to seek out the EI process. Deborah summed up this feeling: “What I experience firsthand are these constant, inappropriate behaviors that makes a caregiver take pause about whether or not they wanna approach the system again. . . I then didn’t seek out anything for several years because I was like, I don’t wanna deal with this again.” As a result of her perceived racialized treatment, Deborah opted to seek private evaluations outside of the healthcare system. Eventually she decided to pay for private EI services for her son, instead of going through the healthcare or Regional Center processes. She shared: “I think that the biases related to us being Black really interfered with them being able to see us for who we were and provide the services that we deserve to have. Everyone I know that’s White got the services I paid for, but for free. And that’s really not fair.”
In a discussion around why she hesitates to engage with the healthcare system when it comes to EI, Mary shared the following: “Think about all the caregivers who have come to the doctor, suspecting something and we’re written off. So we don’t trust the physicians to actually tell us the correct thing, cuz we’re suspecting something and it’s being written off.”
Discussion
Racial disparities in EI outcomes have been well documented (Evans et al., 2016; Feinberg et al., 2011; Gallegos et al., 2021; Liptak et al., 2008; Magaña et al., 2016; D. Magnusson et al., 2016; D. M. Magnusson et al., 2017; Morgan et al., 2012; Rosenberg et al., 2008; Zuckerman et al., 2013, 2017). In explaining such outcomes, prior qualitative studies have explored attitudes, behaviors, and experiences within minoritized groups to explain differences in outcomes (Azad et al., 2022; Evans et al., 2016; D. M. Magnusson et al., 2017; Pearson et al., 2020; Reyes et al., 2018; Sakai et al., 2019). Using CRT, we aimed to expand upon existing studies and examine the role of racism, via the process of racialization, in driving these disparities. While racialization does not operate in the same way for all groups, examining across minoritized groups rather than comparing between groups enabled an understanding of racialization more comprehensively.
Existing studies discuss how minoritized groups are more likely to mistrust systems—or hesitate in help-seeking (Burkett et al., 2015; D. M. Magnusson et al., 2017; Sakai et al., 2019). Our study complicates this picture. The majority of participants in this study had a concern about their child’s development and initially sought support—without hesitation—through the EI process. Our study suggests that it was rather the response of providers to caregiver concerns that limited the process. That minoritized caregivers experience dismissal from providers is a phenomenon well-documented in the literature (Dababnah et al., 2018; Pearson & Meadan, 2018; Stahmer et al., 2019). We examine such dismissal within the larger lens of racialization.
Even though most participants in this study initiated the help-seeking process, our findings still elucidate the complex reasons why caregivers might hesitate to engage with EI systems. For example, negative interactions with providers—whether due to perceived racial bias, provider dismissal, or managing stereotype threat—made it such that several caregivers did not want to re-engage with the system. Caregivers also might feel hesitant to seek EI support from a process that often adds labels that could further disadvantage a minoritized child. For example, one caregiver shared her concern that bias would lead to her son receiving a label (i.e., emotionally disturbed) that she felt would have significant implications for his educational opportunities and safety. Indeed, studies have shown that minoritized children are too often placed into certain disability categories—such as emotionally disturbed or intellectually disabled—compared with White children who receive less stigmatized labels (i.e., Attention-Deficit/Hyperactivity Disorder), as a result of racial bias (Skrtic et al., 2021; Meek et al., 2020). Importantly, children with such labels are more likely to be removed from general education classrooms and placed in exclusionary education settings (Meek et al., 2020), thus forming a mechanism by which minoritized children are disproportionately placed in separated special education settings (Blanchett et al., 2009; Ferri & Connor, 2005). That caregivers might be hesitant to approach EI systems in this context is justifiable. It is critical that providers in the EI process are aware of this phenomenon, and pay attention to how the interaction of racism and ableism may lead to certain labels impacting a child’s educational experience.
In our study, caregivers felt there was an assumption from providers that certain behaviors were expected of minoritized children. Caregivers perceived that this created a different threshold for “abnormal” based on racial stereotypes and resulted in minoritized children needing to have more severe symptoms to receive services. Furthermore, caregivers reported experiences in which they felt that providers assumed that the caregiver did not understand their child’s development, or that the caregiver needed to first alter a parenting practice at home. The question this raises is, to what extent does bias lead providers to be more inclined to wait or not refer minoritized children because there is an assumption that something within the family practices should be “fixed” first before proceeding with further assessment?
Having to advocate within the EI process is well-documented in the literature (Cohen & Miguel, 2018; Pearson et al., 2020; Pearson & Meadan, 2018; Stahmer et al., 2019). Findings from this study surfaced how minoritized caregivers feel their advocacy efforts might be perceived by others. For example, a few caregivers experienced how other people interpreted their persistence in a racialized manner, or consistent with racialized notions that paint minoritized people as “welfare queens” (Nadasen, 2007), or trying to unfairly take advantage of a system. Our results also elucidate the unique burden that comes with persistence as a minoritized caregiver: having to manage stereotype threat, which is defined as the fear of fulfilling a racial stereotype (Spencer et al., 2016). A White person’s behavior when advocating for their child might be perceived differently than a minoritized person’s, where the latter may come off as more aggressive even if it is the same behavior. Caregivers reported an awareness of this dynamic as they navigated the EI process. The question this raises is whether there are outcomes caregivers might have pushed for—or referrals they might have asked for—but didn’t because of not wanting to fulfill this stereotype threat.
The Levels of Racism framework put forward by C. P. Jones (2000) analyzes the various levels in which racism operates to impact health disparities: systemic, interpersonal, and individual. Our study illuminates racialization within the process of accessing EI services, and specifically highlights ways in which racialization shows up at the interpersonal level. This is summarized in Figure 1. We emphasize how racialized experiences can shape caregiver and provider behaviors in ways that could delay the EI timeline, leading to disparate outcomes. We highlight how provider bias and dismissal could exacerbate these disparate outcomes as well.
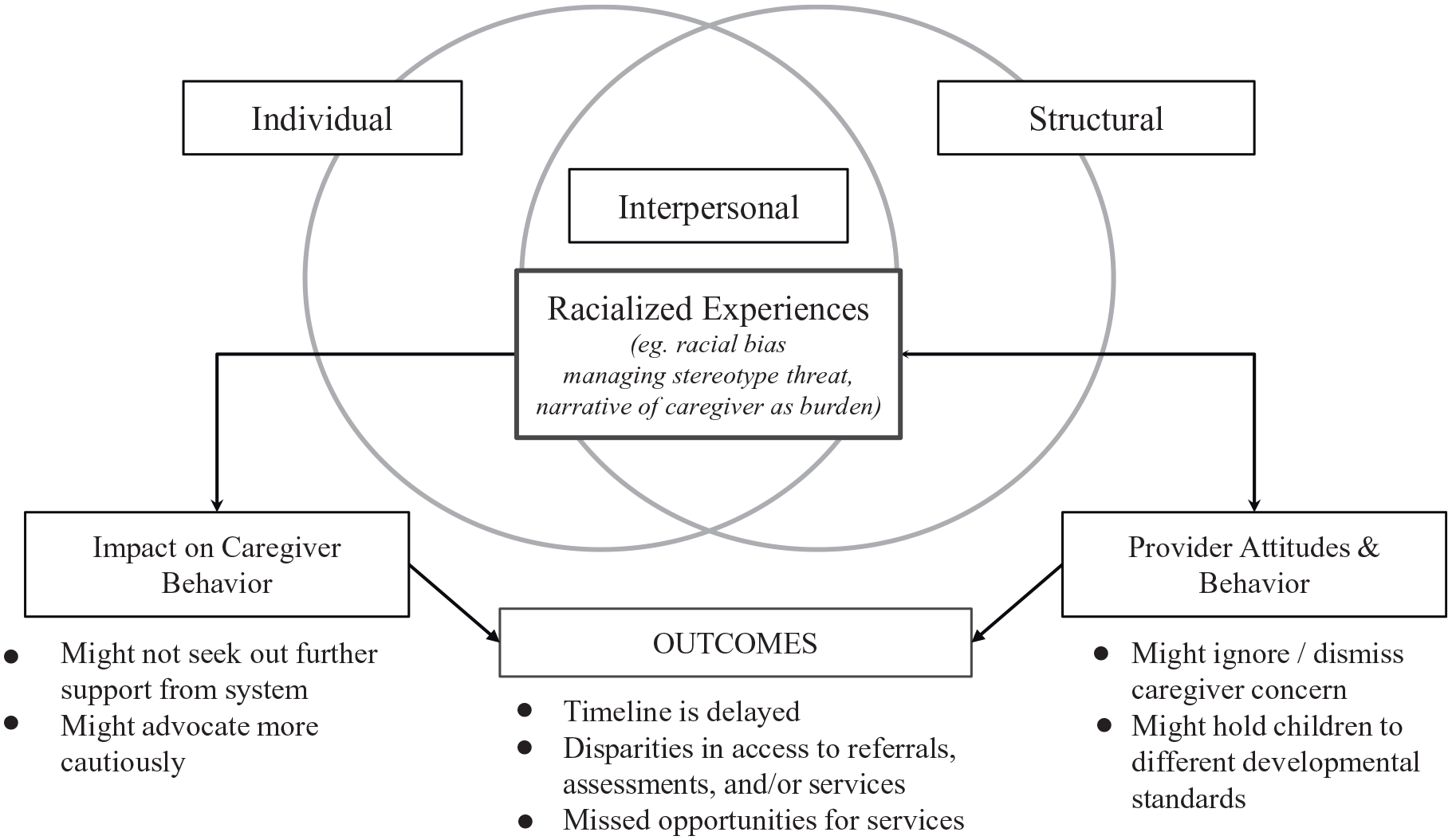
Caregiver experiences of interpersonal racism and potential impact on outcomes.
Implications
At the interpersonal level, this research suggests that efforts to address racial bias in clinic settings are necessary. We recommend couching anti-bias training within a larger framework of anti-racism training, such that providers are encouraged to not only have an awareness of their biases but also to actively question the structures that create and perpetuate such biases. Building an anti-racist lens will ideally ensure that providers remain attentive toward minoritized caregivers’ questions and concerns about their children’s development, and see caregivers as agents existing within oppressive systems rather than focusing on behaviors that confirm racial stereotypes. Additionally, providers should strive to understand the caregiver’s relationship to developmental diagnoses, with the background knowledge that minoritized children have been and continue to be disparately marginalized by such labels. Within healthcare spaces, efforts to recruit a more racially and linguistically diverse workforce is key to providing more culturally sensitive and accessible care.
At the community level, efforts to support caregivers in navigating these complex systems are needed. Indeed, the question of who has access to what information and resources when it comes to EI—and why—is worth further examination. Efforts are underway to address this issue of equitable information sharing. One example is FACES, a 6-week parent advocacy intervention that offers information and training for Black parents of children with ASD (Pearson & Meadan, 2021). While such interventions are important, we must underscore that solutions at this level are not enough to address disparities at large. Structural change is needed to more radically shift outcomes and ensure equity of access. This includes expanding access to primary and specialty healthcare services for minoritized groups. At the state level, efforts should be made to monitor how IDEA funds are distributed to assess equity of EI service distribution. Research to better understand the ways in which structural racism impacts EI outcomes should be prioritized. This includes improvements to the reporting of participation in EI by race and ethnicity, as this data is often under collected and reported (Steinbrenner et al., 2022).
Limitations
Due to the nature of recruitment—in which participants contacted researchers if they were interested in participating—it is likely that the sample self-selected for families who had experiences aligned to this study’s focus, and were more engaged in the EI process. Additionally, as part of the consent process, researchers reminded participants that questions would be asked about race and racism, possibly priming participants to retell their experiences through that lens.
This study sought to explore how racism might contribute to disparities in EI service access. Within this larger goal, we focused on stories of participants who experienced the process, to more deeply understand how this process racializes its users. However, this inherently excluded families who would have benefited from access to diagnostics, evaluations, or EI services but did not receive them, as well as families who had not yet started the process. Because a significant part of recruitment took place in medical clinics, our sample consisted heavily of people with access to the healthcare system.
Within the study sample, three participants had children currently between the ages of 15 and 20, and thus had experienced the EI process several years ago. It is possible that their stories highlight features in the pathway that are no longer practiced. Finally, our sample included a few participants who simultaneously worked within the EI field, including a preschool teacher and two family resource navigators. These individuals may have offered insights on the EI system from both the parental and a professional lens, having access to institutional knowledge.
Conclusion
We sought to understand barriers to accessing EI services by using a CRT lens to explore the mechanisms by which caregivers are racialized within the process. Surfacing the experiences of families who navigate these systems, we highlighted ways in which the process can be racializing. Additionally, we outlined mechanisms by which racialization contributes to a delayed EI process altogether. Efforts to understand and address racial bias, and center perspectives of minoritized caregivers within the EI process are greatly needed. Only then can we begin to address the deep racial disparities in EI participation and enable all children to access supports in a timely manner.
Supplemental Material
sj-docx-1-tec-10.1177_02711214241249110 – Supplemental material for Caregiver Experiences of Racialization While Accessing Early Intervention (EI) Services for their Children
Supplemental material, sj-docx-1-tec-10.1177_02711214241249110 for Caregiver Experiences of Racialization While Accessing Early Intervention (EI) Services for their Children by Jessa N. Culver, Susanne P. Martin Herz, Adriana Guzman, Javier Aguayo, Jyothi Marbin, Kenya Martinez and Jennifer James in Topics in Early Childhood Special Education
Supplemental Material
sj-docx-2-tec-10.1177_02711214241249110 – Supplemental material for Caregiver Experiences of Racialization While Accessing Early Intervention (EI) Services for their Children
Supplemental material, sj-docx-2-tec-10.1177_02711214241249110 for Caregiver Experiences of Racialization While Accessing Early Intervention (EI) Services for their Children by Jessa N. Culver, Susanne P. Martin Herz, Adriana Guzman, Javier Aguayo, Jyothi Marbin, Kenya Martinez and Jennifer James in Topics in Early Childhood Special Education
Footnotes
Acknowledgements
We thank Dr. Katharine Zuckerman (Oregon Health and Science University) for insightful comments on the manuscript.
Author Contributions
JC, SMH, and JJ contributed to the study conception and design.
Material preparation and data collection was performed by JC, AG, and JA. Analysis was performed by JC, AG, JA, JJ, SMH, and JM. The first draft of the manuscript was written by JC and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Author JC has received a $700 grant from the Center for Race and Gender at the University of California, Berkeley for research-related expenses. Author JC has also received $1,800 from the UC Berkeley—UCSF Joint Medical Program for research-related expenses.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Review Board (IRB) of the University of California at Berkeley on July 13, 2021, protocol # 2021-05-14349. University of California San Francisco (UCSF) relied on UC Berkeley IRB for review of the human subjects activities.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.