
Abstract
Many children with developmental delays need early intervention services but do not receive them. Developmental screening provides the impetus for identification of delays and service referrals but is not used consistently across all early childhood education settings. We used an implementation science framework to examine attitudes and engagement in a developmental screening program across three U.S. early childcare centers. Teachers demonstrated adequate knowledge of screening following training in the screener and were highly engaged in the screening process. Teachers’ positive attitudes toward screening increased yet perceived barriers to regular use of screening in their practice remained unchanged. Family participation in the screening process varied across centers and suggested a trend between family income and participation. Future research is needed to target pervasive barriers to teachers’ use of screening, such as perceived difficulties in engaging parents in the screening process.
Keywords
Approximately one in six U.S. children are diagnosed with a developmental disability (Boyle et al., 2011). Early identification of developmental delays and disorders is critical to ensure children and families have access to early intervention to address key social, emotional, and cognitive skills (Singh & Anekar, 2018). Developmental screening tools facilitate the identification of potential delays. Recent research has focused on the acceptability and competence of early care and education (ECE) providers in conducting screening (Branson & Bingham, 2017; Shahidullah et al., 2020) given their frequent contact with young children and their families and limitations to use of screening in primary care (Bright et al., 2019). Using an implementation lens, we examined changes in ECE teachers’ knowledge, attitudes, and perceived barriers to developmental screening following comprehensive training in screening practices using a research-tested screening tool.
Implementation of developmental screening is critical to lower the age of identification for developmental delays and connect children and their families to needed early intervention services (Guevara et al., 2013). Unfortunately, many children who need early intervention are missed until later in life. In 2019 less than 4% of children birth to age two received Part C intervention services under Individuals with Disabilities Education Improvement Act (Individuals with Disabilities Education Act [IDEA], 2004). For instance, many children with autism spectrum disorder (ASD) experience a 3- to 4-year delay in receiving a diagnosis after first exhibiting symptoms (Baio et al., 2018). Identification gaps are even larger for children living in poverty and for racial and ethnic minority children who tend to experience higher poverty rates than their non-Hispanic White peers (Durkin et al., 2010; Gradín, 2012). In their study of 131 infants at-risk for developmental delay, Fefferman et al. (2017) report the likelihood of connecting to early intervention services declined by 24% for every reduction of $10,000 in median household income (p < .05).
Front-line practitioners, such as (ECE) teachers and pediatricians, are ideally positioned to implement universal developmental screening. Examples of successful pediatric screening initiatives documented in the literature emphasize the potential for training in child development and screening practices to increase use of developmental screening (Berry et al., 2014; Bright et al., 2019). Unfortunately, barriers to sustained use of developmental screening are inherent in the complexities of pediatric practice including the need for buy-in and training among diverse staff (Berry et al., 2014; Pinto-Martin et al., 2005) and limited time to discuss results and recommendations following screening (Bright et al., 2019). In their recent survey research, Lipkin et al. (2020) found 30% of pediatricians reported they did not use developmental screening and over 40% indicated they did not refer at-risk children for services.
Teachers in ECE are well positioned to support regular screening for developmental concerns given their frequent contact and familiarity with children and their families, ample opportunities to observe child skills and growth, and training and experience in understanding typical child development. Universal screening in ECE can impact a large number of children as approximately 60% of all children 5 years old or younger receive some form of childcare outside of the home (Laughlin, 2013).
Developmental Screening in Early Care and Education Settings
Universal developmental screening is an essential component of ongoing child assessment in high-quality ECE programs (Halle et al., 2011). Within the child assessment standards of the Quality Rating and Improvement System (QRIS), a national rating system concerned with the assessment, improvement, and communication of quality levels in ECE settings (https://ecquality.acf.hhs.gov/), quality rankings are based on programs’ use of multiple indicators of children’s learning and development, including developmental screeners. Moreover, federally funded Head Start programs require regular use of developmental screeners (Improving Head Start for School Readiness Act, 2007). Thus, ECE teachers must be equipped with the skills to administer, score, interpret, and use information from screeners as part of high-quality practice. ECE teachers and administrators must also understand the conditions necessary to implement and sustain developmental screening programs amidst other demands and challenges of ECE settings. For instance, collaboration between teachers and other staff may facilitate efficiency in the screening process such as involving administrators in sharing results with families and recommendations for follow-up.
Despite ECE teachers’ training in child development and frequent access to children and their families, there are gaps in the availability of screening tools and their use in ECE settings. Many ECE teachers feel young children do not receive appropriate screening (Pizur-Barnekow et al., 2013) and report that they are unfamiliar with screening tools (Rispoli et al., 2021). The disconnect between availability of research-tested developmental screening measures and their use in ECE settings may reflect lack of effective professional development supporting their use (Forman & Barakat, 2011) as well as insufficient access to these tools.
When implemented, ECE teachers and parents find developmental screenings appropriate for use in ECE settings. Nelson et al. (2011) investigated parent perceptions of screening tools used in Head Start, the largest federally funded preschool program in the US and found that parents perceived the screening procedure important both for diagnostic and educational purposes. Benefits of the utilization of developmental screening tools in this program included closer parent-teacher relationships, improved parenting skills/strategies, and an increased understanding of developmental interventions (Nelson et al., 2011). Shahidullah et al. (2020) reported that the majority of ECE teachers supported the use of developmental screening tools in their organizations following training about developmental screening. These beliefs about the usefulness of screening were associated with ECE teachers’ current or anticipated use of developmental screenings.
The Ages and Stages Questionnaire, Third Edition (ASQ-3; Squires et al., 2009) is a developmental screening tool appropriate for early childcare settings. The ASQ-3 can detect a range of potential developmental concerns (Scarpa et al., 2013) and is recommended as part of high-quality ECE assessment (Halle et al., 2011). The ASQ-3 is a parent-report measure that screens for concerns based on the child’s age range (e.g., 2 mos., 18 mos.) across several domains such as communication, personal-social, motor, and problem-solving skills. In a review of the ASQ-3, Singh et al. (2017) report strong psychometric properties related to specificity (95.7%), sensitivity (87.4%), and test-retest reliability (92%). In another systematic review of 20 studies, the ASQ-3 was reported to demonstrate strong specificity (19/19 studies), sensitivity (13/18 studies), and reliability (11/18 studies) across multiple studies (Velikonja et al., 2017). Concurrent validity between other early childhood measures is also promising, such as the Bayley Scales of Infant Development II, demonstrating moderate correlations among multiple subscales for 2-year-olds (r = .45–.52; Gollenberg et al., 2010). The ASQ-3 technical manual reports an average convergent validity of 86% between the ASQ-3 and similar standardized measures (Squires et al., 2009).
Implementation Science to Address Gaps in Developmental Screening
There is a need to understand how best to prepare ECE teachers to implement and sustain regular screening with the families they serve, given the availability of well-developed developmental screening tools and importance of screening as part of high-quality ECE practice. Researchers need to better identify variables that affect uptake and sustainability of developmental screening in ECE to promote broader use of this practice, yet this gap is seldom addressed in the literature. Implementation science has been defined as “the scientific study of methods to promote the systematic uptake of research findings and other evidence-based practices into routine practice” (Eccles & Mittman, 2006, p. 1), and is critical in understanding how to best translate the research regarding evidence-based interventions into practice in a feasible manner (Cook & Odom, 2013). Unfortunately, implementation of evidence-based practices in educational settings is variable and lacks sustainability (e.g., Atkins et al., 2003), highlighting the need for understanding conditions that facilitate or complicate intervention implementation, and possible adaptations, necessary for translation of highly controlled research to real-word practice (Forman et al., 2013).
Lack of focus on implementation variables likely underlies the gap in availability of high-quality screening tools and their use in ECE settings. Forman and Barakat (2011) identified five factors often implicated in implementation success in education settings: organizational structures in the setting, characteristics of the setting, fit with the setting’s goals and policies, training and technical assistance, and support from administration. We used an implementation science framework to examine several of these critical implementation factors following ECE teacher training in use of the ASQ-3, including program characteristics, outcomes following training support, and perceived support from administration as potential barriers to screening use. We also studied other relevant implementation process variables including changes in teacher attitudes and knowledge about screening and results of the screening process across centers.
Current Study
We addressed the following research questions:
Method
Participants
We recruited participants from a list of state-licensed daycare and preschool centers in the surrounding geographical areas. Program directors were contacted by the research team and provided permission to contact teachers and invite their participation in the study. Twelve lead ECE teachers (n = 4 per center) from three early childhood education centers participated in developmental screening training and distributed ASQ-3 screeners to parents of children enrolled in their classrooms, scored completed screeners, and shared results with parents. Two of the centers were parochial daycares, one in an urban setting and the other in a suburban setting (i.e., Center 1 and 3 respectively). Center 2 was a child development center in a suburban setting. Teachers all identified as female (M age = 32.28 years old), and the majority noted their racial identity to be Caucasian with one teacher identifying as African American. All teachers had either their Associate’s (n = 6) or bachelor’s degree (n = 6). Teaching experience ranged from 2 to 31 years. Across all three centers, 128 parents participated in screening (Center 1, n = 22; Center 2, n = 25; Center 3, n = 81). The majority of parents (96%) at Center 1 self-reported their race/ethnicity as White (n = 21). In Center 2, 71% (n = 16) of parents self-reported as White and 13% (n = 3) self-reported as Asian American. In Center 3, 95% (n = 76) of parents self-reported as White. The majority of parents reported that they were married (94%; n = 119), while 4% reported being divorced (n = 5), 2% reported living with a domestic partner (n = 2), and 1% reported being single (n = 1). The average age of parents at the time of the screening was 36.57 years old. Sixty percent of children (n = 76) were female and 40% were male (n = 51). Children’s average age at the time of screening was 5.27 years old.
Following the training, teachers, administrators, and parents (n = 15) participated in follow up interviews using focus groups, each held separately at two of the centers (n = 6 and 9 at Center 1 and 3, respectively). Follow up interviews were completed 1 to 2 months after the last training. Interviews were moderated by a trained graduate student and ranged from 15 to 20 minutes in length. Interviews were audio recorded and transcribed verbatim following the meetings. Brief notes were also taken by the moderator. A follow up interview was not conducted at Center 2 due to changes in ownership and administrative leadership that occurred during the study period.
Constructs and Measures
Teacher screening knowledge
We used two measures of teacher screening knowledge as proxy measures of implementation fidelity. The Knowledge and Attitudes about Developmental Screening (KADS) is a five-item measure (range = 1–5, higher ratings indicate greater agreement with items) of familiarity with and views of developmental screening tools. Teachers completed the KADS before and after the screening process. Items asked about teachers’ (1) knowledge of the ASQ, (2) familiarity with conducting developmental screening using tools such as the ASQ or Modified Checklist for Autism in Toddler, Revised (M-CHAT-R; Robins et al., 2009), (3) comfort level in asking parents of children in their classroom to complete the ASQ-3, given materials and support from her/his supervisor, (4) comfort sharing results of a screener suggesting a child had a developmental delay, and (5) level of agreement with a statement indicating that ECE teachers should be responsible for screening children for developmental concerns. The KADS was developed by the research team as part of a previous survey of ECEP attitudes toward developmental screening (Rispoli et al., 2021). Because the KADS demonstrated low internal consistency (ɑ = .63) in the survey study, item-level differences were examined in the current study before and after teachers were trained and conducted screening.
In addition to the KADS, teachers completed a five-item evaluation after each training module to assess their knowledge of major concepts presented in the module. We designed the evaluations to reflect major points of emphasis in each module, and included multiple-choice, short answer, and true/false questions.
Teacher satisfaction with screening training
Teachers also completed a 13-item questionnaire developed for the study regarding their perceptions of each training module. We included items related to presentation content and delivery, utility and interest regarding presentation activities, and knowledge and engagement facilitated by the presenters. We also included two final items regarding the overall quality of the presentation and teachers’ perceived ability to incorporate the information into their work with families.
Barriers to screening for autism spectrum disorder
The Barriers to Screening for Autism Spectrum Disorder (Rispoli et al., 2021) is a 14-item measure (range = 1–6, higher ratings indicate greater perceived severity of barrier) of elements that may impede the use of screeners (e.g., lack of time, lack of administrative support), developed from a measure of teacher-perceived barriers to implementation of behavioral interventions (McGoey et al., 2014). In recent research (Rispoli et al., 2021), support was reported for the measure’s alignment with the Theory of Planned Behavior (Ajzen, 1991) in measuring ECE teachers’ perceived control, attitudes, and subjective norms regarding the use of developmental screening. Good internal consistency (ɑ = .94) was reported in this study of 132 ECE teachers (Rispoli et al., 2021).
Behavior intervention rating scale
The Behavior Intervention Rating Scale (BIRS; Elliott & Treuting, 1991) is a 24-item scale assessing the acceptability and perceived effectiveness of the screening process using a six-point scale ranging from strongly disagree to strongly agree. The BIRS was completed by teachers and parents after the screening process. Item ratings were averaged across the three BIRS domains: Acceptability (α = .97), Effectiveness (α = .92), and Time of Effectiveness (α = .87; Elliott & Treuting, 1991).
Parent satisfaction with screening questionnaire
Parents also completed a 5-item measure of satisfaction with the screening process (e.g., ease of understanding screening questions, type, and method of delivering feedback on child’s results). Item ratings ranged from one “very dissatisfied” to five “very satisfied.” We created this measure for the study.
Follow-up interview questions
We developed five questions for this study from similar studies of program feasibility and acceptability (Hodgson et al., 2018; Pickard et al., 2016; Stadnick et al., 2013). Questions addressed teacher, parent, and administrator experience of the developmental screening training and implementation, use of the ASQ-3 (teachers and parents), and possible adaptations to the training, implementation, and feedback processes. We also asked participants about how the training and implementation processes compared to other screening initiatives.
Procedure
The developmental screening training consisted of five modules covering the topics of typical and atypical child development; administration, scoring, and interpretation of screening; and communicating results to families. Detailed information about each module is displayed in Table 1 and an overview of the procedures and measures can be found in Figure 1. The first author completed train-the-trainer preparation with the ASQ-3 developers prior to conducting the study and received permission to implement the training as part of the research study. The training prepared teachers to seek parental input on their children’s development by completing screeners, consistent with the intended use of the ASQ-3. Throughout the training, we emphasized the importance of parental involvement in the screening process for the quality of information provided and the opportunity to educate parents about typical development through discussion of results. We adapted training modules to meet the need of the study and included a broader focus on typical and atypical development than traditional ASQ-3 training, including the use of an ASD-specific follow-up measure if children displayed risk factors for this disorder. We included training on identifying risk factors for ASD and the use of a brief, user-friendly follow-up measure, the Checklist for Early Signs of Developmental Disorders (CESDD; Dereu et al., 2010), given the growing prevalence of this developmental disorder and known issues with its early identification (Baio et al., 2018; Durkin et al., 2010). The CESDD complemented the ASQ-3 since the latter was not developed to screen for ASD. We trained teachers to ask the parent of any child who exhibited risk for social and/or communication delays per ASQ-3 results to complete the CSEDD. We advised teachers to consider referring the family to a developmental evaluation with early childhood special education if children scored above the cutoff score of 2 on the CSEDD. Follow-up screening with the CSEDD occurred for one child.
Developmental Screening Training Module Content.
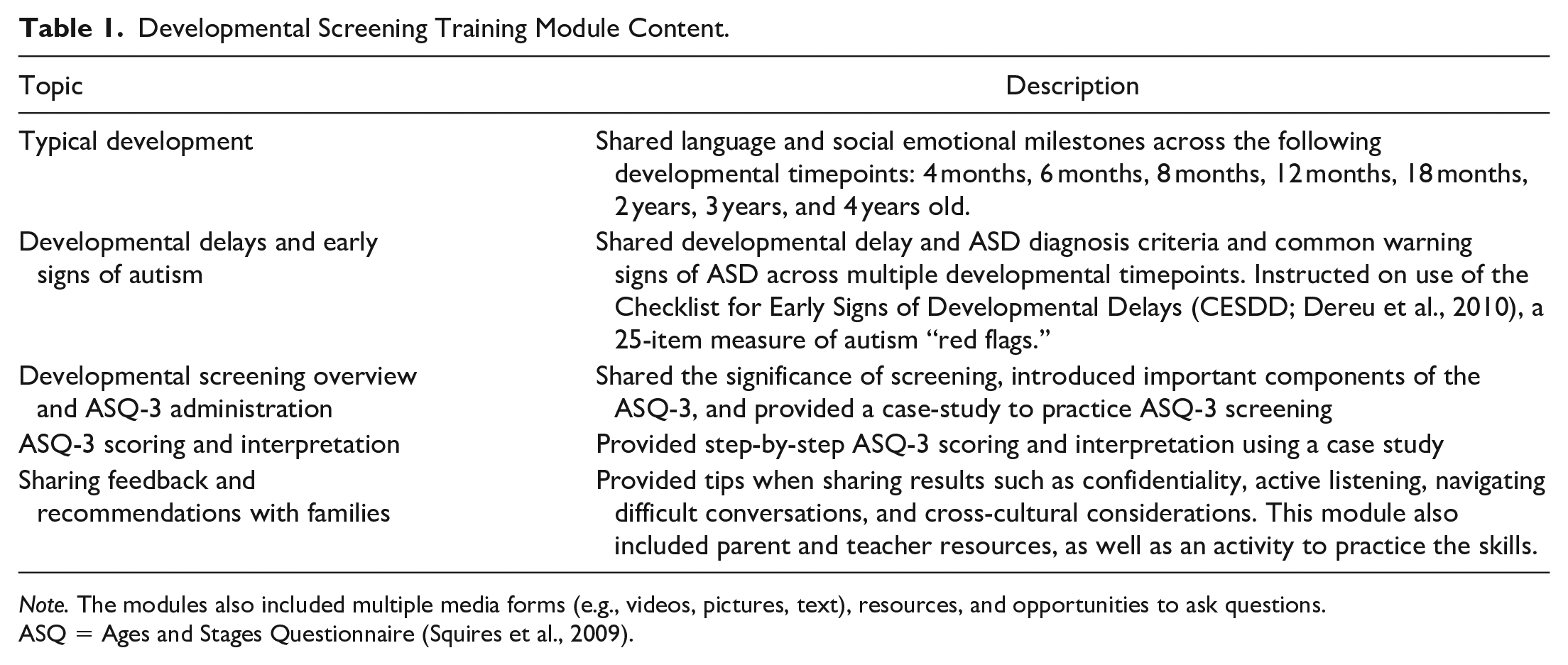
Note. The modules also included multiple media forms (e.g., videos, pictures, text), resources, and opportunities to ask questions.
ASQ = Ages and Stages Questionnaire (Squires et al., 2009).
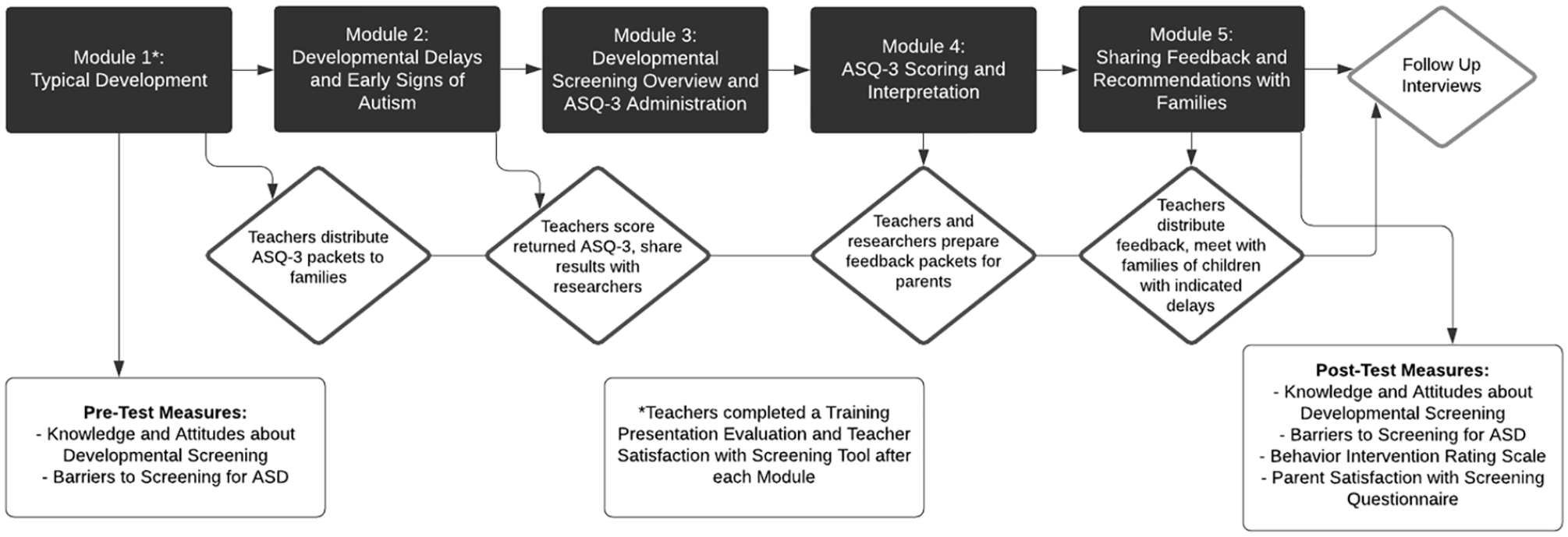
Diagram of study trainings, procedure, and pre- and post-test measures.
We implemented training over the course of 3 to 5 months in each center, with time scheduled in between each training session to allow for teacher administration, receipt, and scoring of ASQs. Training sessions ranged in length from 1 to 2 hours. Number of teachers attending the training sessions varied as teaching assistants were also invited to attend the trainings; lead teachers participating in the study attended all sessions at each center except for one teacher who missed the first session due to a family emergency. We provided teachers with screening packets to distribute to families of each child enrolled in their classrooms following the training on screening administration. We included a cover letter from the research team, consent form, and ASQ-3 screener appropriate for the age of each child in these packets. Teachers returned the consent forms to our team, and we documented completion and tracked which families from class returned the ASQ-3.
Teachers completed scoring and parent feedback, though we assisted the teachers with preparing results for families. Specifically, teachers scored completed ASQ-3 screeners; they were trained to score the ASQ-3 in Module 4 of the trainings through a presentation and practice case. Before results letters were prepared, members of our team reviewed each completed ASQ and corrected any scoring errors. Teachers discussed results with our team, and we then prepared parent feedback letters for the teachers to distribute. Teachers used letters as a tool to facilitate teacher communication about results, highlight areas in which the child was meeting developmental expectations, as well as describe any areas of concern. The letters contained links to developmental information available from the Centers for Disease Control (https://www.cdc.gov/ncbddd/actearly/milestones/milestones-in-action.html) and Zero to Three (https://www.zerotothree.org/early-development). Teachers distributed the letters along with a BIRS form for parents to complete. Teachers discussed results with the family and provided appropriate suggestions as indicated by results (e.g., follow-up with local school district early intervention services) for each child who scored in the at-risk or developmental delay category on any ASQ-3 domain.
We used a single-group, pre-post design to evaluate change in teacher attitudes and knowledge as measured by the Barriers and KADS following training in ASQ-3 and using the tool in their classrooms. We also measured parent and teacher perceptions of screening with the ASQ-3 at post-test using the BIRS. We elicited additional feedback from administrators, teachers, and parents via follow up interviews following screening. Pre-test data collection occurred before the first training session, and post-test data collection was conducted after teachers provided screening feedback to parents. Given issues with nonnormality in the quantitative data, we used nonparametric analyses to compare pre–post ratings on the KADS and Barriers Questionnaires. We also explored trends in teacher acceptability across demographic characteristics of each center. We also descriptively evaluated parent response rates across centers and compared those findings to demographic data to explore trends in parent engagement in the screening process.
The second and third authors, who are graduate students in a school psychology doctoral program, conducted thematic analysis (Braun & Clarke, 2006) to systematically derive themes from the follow up interview data. After completing training in thematic analysis, these members of the research team individually reviewed the interview transcripts to identify stakeholders’ experience while participating in the study, their thoughts about the ASQ-3 screener, recommendations for study improvements, and their interest in continuing the use of the ASQ-3. The researchers then met and identified common themes.
Results
Preliminary Results: Student Developmental Risk
Results from the ASQ-3 showed one student scored in the delayed range in communication and one in personal social. Seven at-risk concerns (i.e., parents are instructed to monitor and are provided learning activities) were found in communication, eight in fine motor, five in problem solving, five in gross motor, and three in personal social domains.
Research Question 1: Changes in Teacher Screening Knowledge
We used the Wilcoxon Signed Rank Test to compare the median of differences on the KADS at pre- and post-test. Following the training and implementation of screening, teachers reported greater familiarity with the ASQ (Mpre = 3.92, SD = 1.08; Mpost = 4.87, SD = 0.44; p < .01) and screening tools overall (Mpre = 3.33, SD = 1.37; Mpost = 4.33, SD = 0.50; p < .05). There were no significant changes reported in comfort asking parents to complete the ASQ-3, sharing results of screeners that indicated risk for developmental delay with parents, and belief that early childhood education teachers should be responsible for screening children for developmental concerns. Average scores on knowledge quizzes administered after each training module were high, ranging from 92.5% to 100% across modules.
Research Question 2: Teacher-Perceived Barriers to Implementation
Four of the top five barriers rated by teachers remained the same from pre- to post-test (1 = not serious, 6 = extremely serious). These barriers were difficulty communicating with families about children’s needs (pre: M = 4.18 [0.75]; post: M = 4.09 [1.92]), lack of training on how to refer families for more evaluation/services (pre: M = 4.36 [1.28]; post: M = 4.00 [1.41]), lack of time to score screeners and prepare feedback for families (pre: M = 4.36 [1.50]; post: M = 4.00 [1.73]), and lack of training on discussing screening results (pre: M = 4.73 [1.01]; post: M = 4.00 [1.41]). The average rating across all Barriers items decreased slightly from pre-test (M = 4.01, SD = 0.82) to post-test (M = 3.63, SD = 1.36) but comparison of median difference ratings using the Wilcoxon Signed Rank Test was nonsignificant. Exploration of trends in the data suggested relatively greater improvement in perceived barriers for more experienced teachers (1.04 decrease in barrier ratings for teachers with 10+ years of experience) compared to teachers with fewer years of experience (0.13 increase in barrier ratings for <10 years of experience).
Research Question 3: Teacher Screening Acceptability
Teachers rated the training as highly acceptable (training evaluation M = 3.87, SD = 0.34; range = 1–4). On the BIRS (1 = strongly disagree, 6 = strongly agree) teachers (M = 5.27, SD = 0.79) and parents (M = 4.54, SD = 1.12) provided ratings suggesting that they found screening implementation acceptable and useful.
Research Question 4: Implementation Factors Across Programs
We stratified teacher ratings and screening return rates to explore potential differences in implementation variables across centers by family income levels. Teacher attitudes and knowledge about screening were similar across centers, though Center 2 reported lower overall beliefs that screening should be part of their job (see Table 2). The largest percentage of screeners (83%) were returned by families in Center 3, which also served families with the highest median family income and largest portion of parents with graduate degrees. ASQ return rates were 41 and 63% in Centers 1 and 2, respectively. See Figure 2. The lowest return rate occurred at the center with the smallest portion of parents who earned their college degree, though there was no clear trend between return rates and parental education (see Figure 3).
Teacher Knowledge and Attitudes Regarding Screening Across Centers.
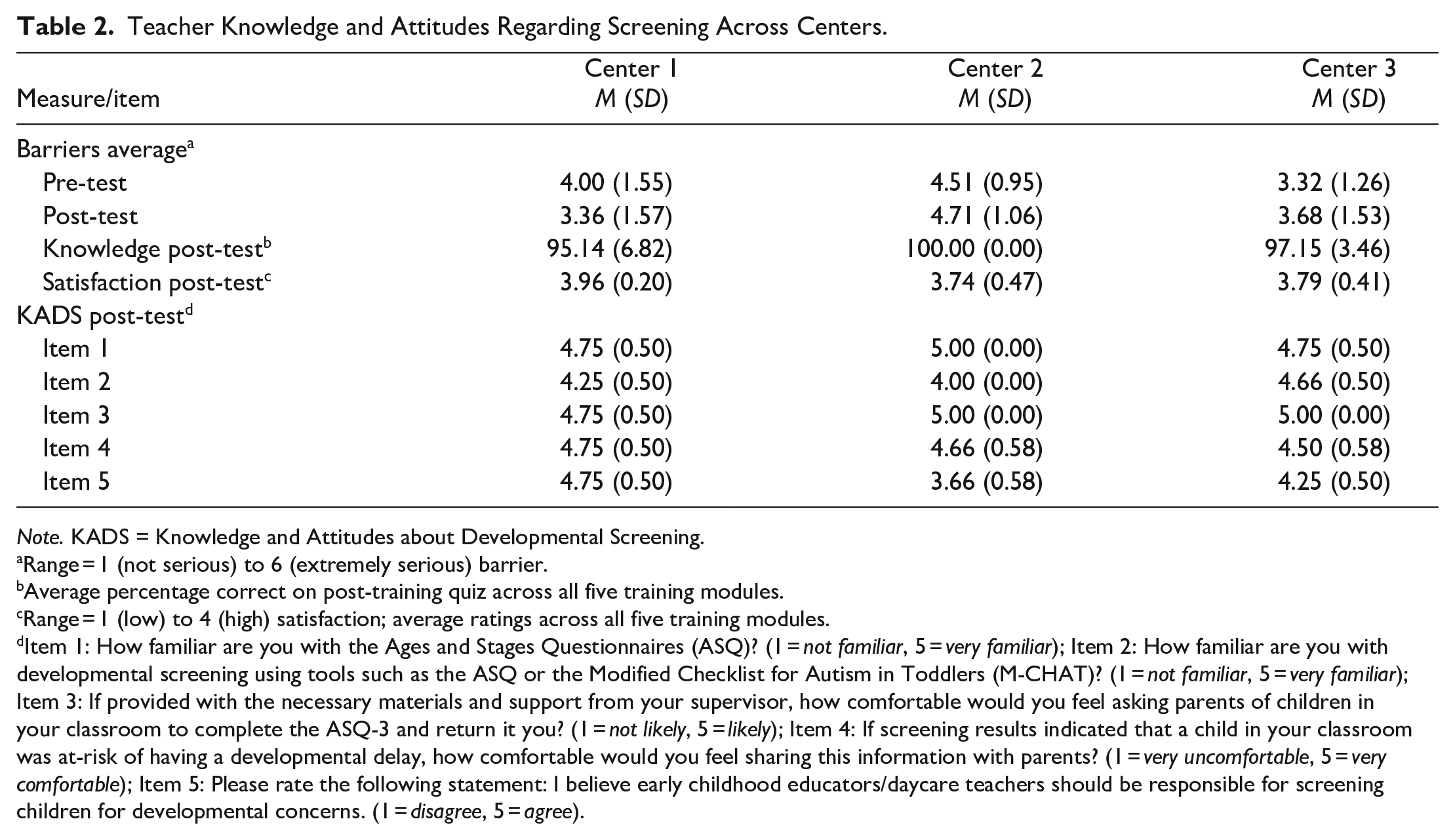
Note. KADS = Knowledge and Attitudes about Developmental Screening.
Range = 1 (not serious) to 6 (extremely serious) barrier.
Average percentage correct on post-training quiz across all five training modules.
Range = 1 (low) to 4 (high) satisfaction; average ratings across all five training modules.
Item 1: How familiar are you with the Ages and Stages Questionnaires (ASQ)? (1 = not familiar, 5 = very familiar); Item 2: How familiar are you with developmental screening using tools such as the ASQ or the Modified Checklist for Autism in Toddlers (M-CHAT)? (1 = not familiar, 5 = very familiar); Item 3: If provided with the necessary materials and support from your supervisor, how comfortable would you feel asking parents of children in your classroom to complete the ASQ-3 and return it you? (1 = not likely, 5 = likely); Item 4: If screening results indicated that a child in your classroom was at-risk of having a developmental delay, how comfortable would you feel sharing this information with parents? (1 = very uncomfortable, 5 = very comfortable); Item 5: Please rate the following statement: I believe early childhood educators/daycare teachers should be responsible for screening children for developmental concerns. (1 = disagree, 5 = agree).
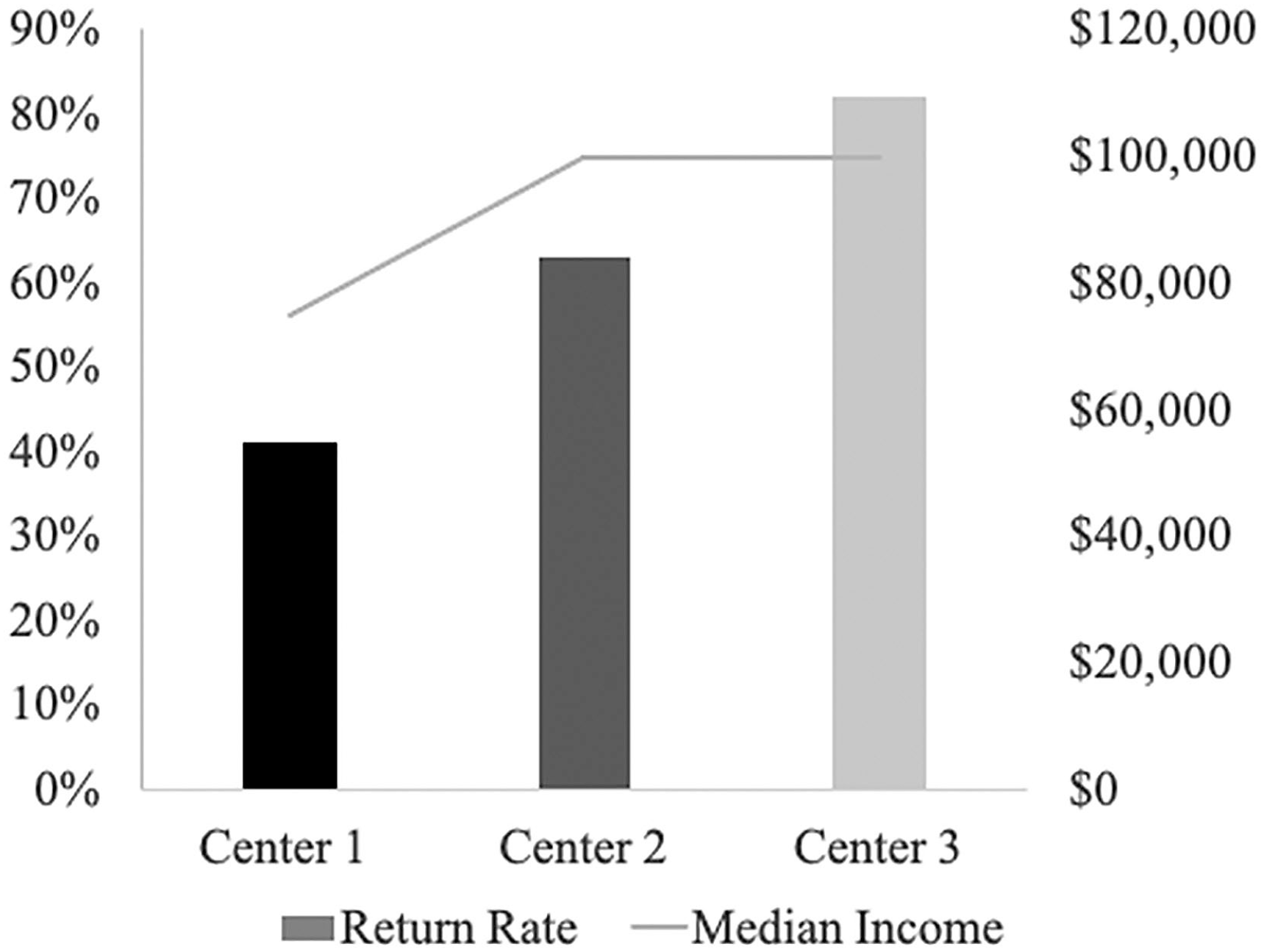
Exploration of trend in ASQ-3 return rates and family income across participating centers.
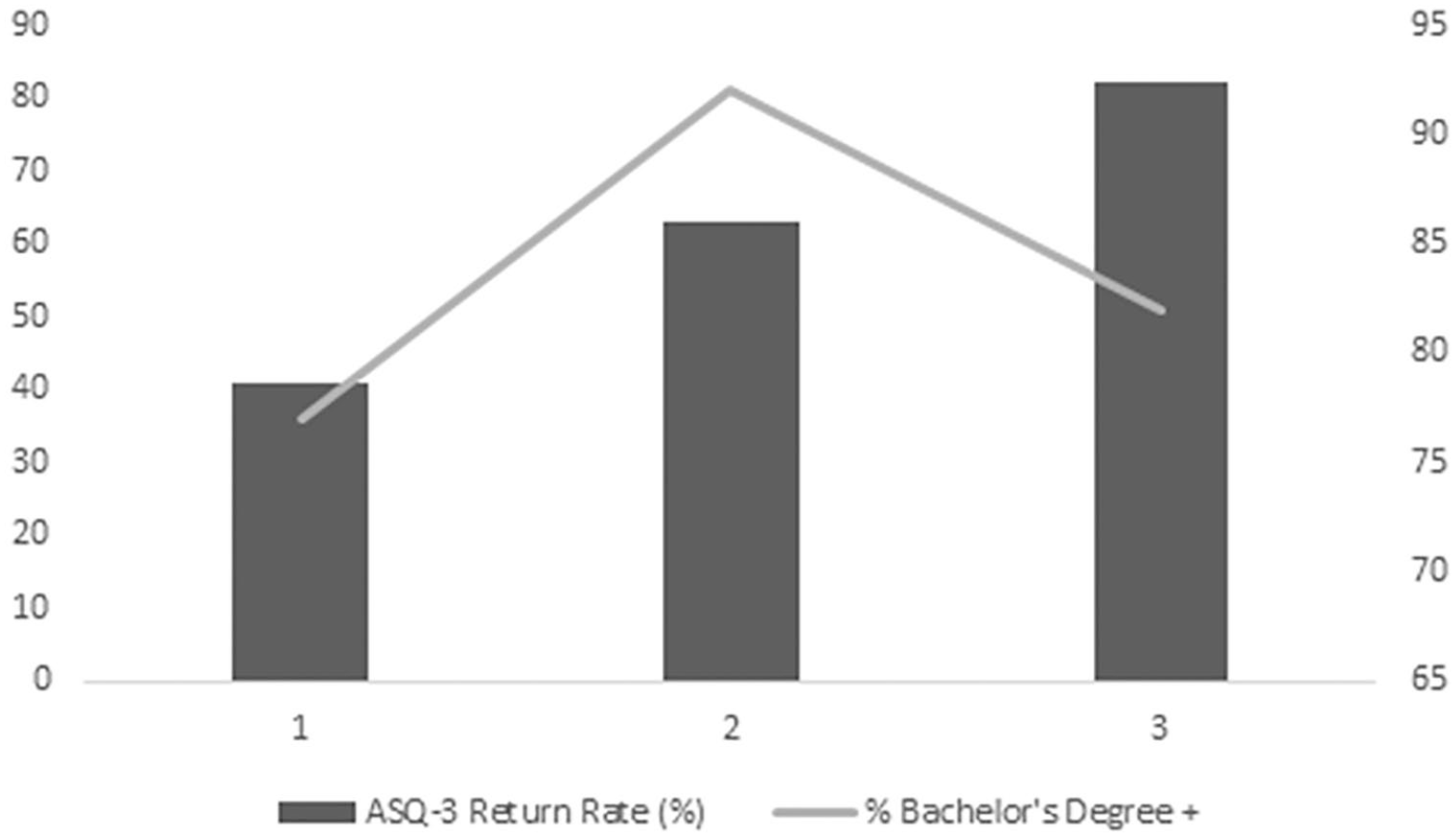
ASQ-3 return rates and parental education.
We analyzed follow up interview data for common themes and differences in attitudes and feasibility across centers. Overall, teachers and parents reported positive attitudes toward the screening process and teachers were interested in continuing use of the ASQ-3 in their centers. One teacher from Center 3 commented, “I’ve already kind of implemented that” indicating she was continuing to use the screener even after the end of the study. Teachers’ capacity for distributing and collecting screeners was one factor that appeared to contribute to feasibility of implementation. Response rate was lower for Center 1 and teachers at this center noted that they would have benefitted from having one teacher in charge of the process of collecting all screeners. Teachers also noted that they believed with continued implementation of this screening process they could get parents more involved. One teacher from Center 1 noted, “I think the next time we do it, if we’re more prepared for it, I think we could definitely get the parents more into it as well.” Parents in both follow up interview groups reported that the ASQ-3 was like other screeners they had encountered before and therefore was not cumbersome. However, parents noted that they would have liked to receive the scored ASQ screener accompanied with more information either verbally or in writing. For instance, one parent shared they would have liked information on “how to help with the development of a certain skill if they are scoring low on it. Like what we do at home as parents to help with that.” Participants in both follow up interview groups noted little implementation of other screeners and thus no clear theme emerged for how the screening process compared to other, similar initiatives.
Discussion
Despite widespread availability of developmental screening tools, factors related to their use in early childhood and education centers are not well understood. In this study, we evaluated changes in teacher attitudes and knowledge about screening as well as factors related to implementation of an established developmental screening tool, the ASQ-3. Parents’ participation in screening and perceived acceptability of the screening program was also studied, as well as program characteristics that may have been related to participation in screening. There was some positive change in ECE teachers’ attitudes toward screening and increased knowledge of the screening process. Parents indicated satisfaction with the screening process, though data were limited by a low response rate to the acceptability questionnaire. Screener return rates varied across centers, and differences suggest sociodemographic factors may have been related to families’ decision to participate in screening.
User understanding is a key element in fostering implementation of new practices in educational settings (Briesch et al., 2013). Previous research suggests many ECE teachers report low levels of familiarity with screening tools (Author et al., 2018) and that screening may occur infrequently in these settings (e.g., Pizur-Barnekow et al., 2013). In this study we examined teachers’ knowledge of module-specific information following each training session and attitudes toward screening. Teachers indicated a high level of knowledge on post-test quizzes created for the study following all modules, suggesting that they understood information about the use of ASQ-3, typical and atypical development in young children, and how to share information about developmental screening results with families. Teachers also reported significantly higher levels of familiarity with the ASQ-3 and screening tools in general following the training and use of the ASQ-3 with their families.
Despite positive findings regarding teacher understanding, results were somewhat mixed for teachers’ attitudes toward the screening process. Overall teacher acceptability as measured by the BIRS was positive. However, teachers did not report significantly higher levels of comfort in requesting that families complete the ASQ-3, sharing results of the screening with families, or belief that screening should be part of their role following their participation in the training and screening process. It is notable that average ratings increased for teachers’ attitudes about asking families to complete screeners and sharing results with families. It is possible that the small sample size precluded detection of significant differences in pre-post ratings. Nevertheless, concerns about sharing negative results with families and worries about lack of available providers for referrals are also identified by physicians as barriers to implementation of developmental screening (Pinto-Martin et al., 2005) and other research with ECE teachers suggests that teachers have low expectations for parent participation in screening and follow-through with screening recommendations (Shahidullah et al., 2020).
Teachers’ beliefs about whether screening should be an expectation of their role were slightly lower at post-test, suggesting that despite training and use of screeners with families, teachers may not perceive their use of developmental screening as a critical part of their practice. This lack of change may be due to several factors, including competing demands for teachers’ time, belief that screening should be conducted by administrators rather than teachers, or belief that developmental concerns are detectable without the use of screening tools. These concerns may be addressed by considering Forman and Barakat’s (2011) framework for implementation science; namely, that support from administration is a key factor for sustained educational initiatives. In future studies, researchers should explore teacher attitudes toward the use of screening tools in their practice relative to other responsibilities as well as how perceptions of support from administrators may impact teacher attitudes toward this practice.
Despite lack of change in teachers’ perceived role in screening, participation rates and satisfaction ratings were high. All ECE teachers who participated in the training distributed the ASQ-3 to families of children in their classrooms, except for one Center 2 teacher who left the center before the study was completed. Parents who returned acceptability questionnaires likewise reported a high level of satisfaction with screening, though the response rate for the BIRS acceptability questionnaire was low. It is possible that parents who were less satisfied with the screening process chose not to return acceptability questionnaires. Though more research is needed to understand parents’ attitudes toward developmental screening and their relation to involvement in the screening process, some work suggests most parents follow through with referrals provided as part of community-based screening (Marshall & Raffaele Mendez, 2014). Nevertheless, in another sample of ECE teachers (N = 134), researchers found that teachers anticipated low levels of participation of parents in screening, despite teachers’ widespread enthusiasm for the importance of screening and its role in their work. In this same study, low levels of parent participation in screening were cited as a primary potential barrier to the implementation of screening programs (Shahidullah et al., 2020). In other work, Dereu et al. (2012) examined the potential for ECE teachers to complete developmental screening on behalf of the children they serve and found similar utility to that of parent-completed screening. Efforts to use ECE teachers as screening respondents may underscore difficulties in engaging parents in the screening process in addition to concerns with parents’ accuracy in understanding and judging developmental skills.
Following the screening process, teacher-identified barriers to screening remained unchanged. Specifically, teachers continued to perceive difficulties with communication with families, awareness of referral sources for children needing additional support, time, and training on how to discuss results with families as significant barriers. In similar research by Shahidullah et al. (2020), ECE teachers identified time, parent issues, and limited teacher knowledge as barriers to screening. In the study, only half of the sample of early childcare teachers indicated they felt comfortable providing feedback from the ASQ-3 to families, and less than 30% felt that parents would complete screeners. Though more research is needed, trends in the data suggest that teachers with more experience perceived greater reduction in barriers to screening following training compared to their less experienced peers. Together, these findings underscore the importance of training and technical support in implementation (Forman & Barakat, 2011) and suggest a need for additional support beyond initial training, such as coaching, to alleviate the barriers to use of developmental screening programs in ECE settings. Support in addressing perceived barriers to use of screening may be particularly important for newer ECE providers. In the current study, parent feedback letters were prepared by the research team to increase feasibility and provide teachers with a tool to facilitate discussions about screening results. It is possible that teachers may have been more satisfied with greater levels of control over how results were shared, such as by creating these letters themselves or using other methods to facilitate conversations about results. Future research should evaluate optimal supports for teachers to communicate results of screening with parents.
In the current study, the greatest proportion of screeners were returned in the center serving families with relatively higher average income and education levels, highlighting how program characteristics can play a crucial role in successful implementation and barriers to implementation (Forman & Barakat, 2011). These families may have had greater resources (e.g., time due to flexible working hours) but additional research is needed to understand parents’ attitudes and perceived barriers to participating in screening. Other studies suggest fear of labeling and misperceptions about the purpose of developmental screening is a barrier that needs to be addressed for successful, large-scale, community-based screening programs (Shahidullah et al., 2020).
Study Limitations
This study was limited by the small sample size. Though the centers varied somewhat by geographic location, communities served, and family demographics, more research is needed to better define implementation factors for large-scale, community-based screening initiatives. Another limitation was the lack of psychometrically tested instruments for measuring teacher attitudes and barriers to screening. Fidelity of teacher administration, scoring and communicating of screening results was not measured and should be evaluated in future research. While appropriate for study data, the use of nonparametric analyses to evaluate group differences in screening knowledge and barriers increased the risk of measurement error and results should be interpreted with caution. Finally, follow up interviews were conducted with teachers from the same program, which may have influenced their responses to interview questions.
Implications for Future Research
We addressed a gap in the literature through investigating factors related to implementation of a developmental screening tool, the ASQ-3. Many implications emerged, particularly surrounding implementation factors. Future research should expand the work here to consider how to address barriers to screening noted by ECE teachers, using larger samples that allow for more robust analyses. In the current study, we found that while teacher understanding and knowledge after the training was high, teacher-identified barriers to screening remained unchanged. Researchers should thus consider these barriers to implementation and which variables may be most critical. For example, it may not be possible from a practical standpoint to immediately address all barriers including perceived difficulties with communication with families, awareness of referral sources for children, time, and training on how to discuss results with families. Instead, research should systematically address barriers perceived by ECE teachers in order of their perceived significance and measure effects of attempts to address these barriers on teacher and parent perceptions of screening, as well as child receipt of additional testing or services. The utility of extended support for screening implementation, such as through ongoing teacher coaching guided by fidelity checks, should be studied in future research.
Furthermore, research is needed to further explore differences in response rates across settings. In the current study, response rates varied across centers. In our study, the largest percentage of ASQ’s were returned by families in the center with the highest median family income, with a trend suggesting an association between return rates and income. In future studies, researchers should consider differences in response rates and evaluate what factors are associated with response rates for families in large, diverse samples that allow for statistical testing of correlates of screening participation.
Implications for Practice
There are multiple implications for practice. Broadly, teacher attitudes and parent satisfaction support the use of developmental screening in ECE settings. This practice provides an opportunity to enhance early detection of developmental delays among children and subsequently allows for a quicker connection to needed interventions and services. Accordingly, screening is considered an element of high-quality ECE (https://ecquality.acf.hhs.gov/). Training in developmental screening should be made widely available to ECE teachers and should include increased focus on complex aspects of using screening programs including communicating the screening procedures and results with families. Resources should be made available to ECE teachers to foster meaningful use of screening results. For instance, teachers’ comfort in communicating results and recommendations to families following the screening process may be enhanced by templated lists of resources and referral information that can be individualized by teachers with the support of administrators.
Ongoing support such as teacher coaching and assessment of teacher attitudes toward the use of screening will likely be increased with sustainability of professional development efforts. During implementation of screening programs, ECE administrators should make explicit efforts to elicit teacher buy-in as some teachers may not interpret this task as a part of their job responsibility. In practice, buy-in may be improved by addressing some teacher-perceived barriers to developmental screening such as concerns with relaying results that a child is exhibiting risk for developmental delays. Finally, administrators and teachers should invite feedback from parents regarding their decision to return or opt not to return screeners. This information can inform future efforts to engage more parents in the screening and follow-up process and increase effectiveness of service provision.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Support for this study was provided by a grant awarded to Kristin Rispoli by the Michigan State University Center for Autism, Intellectual, and other Neurodevelopmental Disabilities (C-RAIND).