
Abstract
Background:
Conventional psychological and pharmacological substance abuse treatments are limited to moderate effect sizes and fail to magnify outcomes when combined. Analog psychedelic agents N, N-dimethyltryptamine (DMT) and 5-methoxy-N, N-dimethyltryptamine (5-MeO-DMT) show therapeutic potential for treatment-resistant psychiatric disorders including substance addictions.
Methods:
This systematic review and meta-analysis synthesized DMT intervention studies (1960–2024) across PubMed, PsycINFO, Web of Science, and EBSCO databases, calculating pooled effects for substance use reduction. Subgroup sensitivity analyses examined the impacts of psychotherapy, population type, and treatment design on outcomes.
Results:
DMT yielded a large overall effect size for substance abuse reduction (g = 0.94, 95% CI: 0.56–1.31, p < 0.0001), with superior efficacy for drug use (g = 1.35, 95% CI: 0.63–2.07, p < 0.0001) compared to alcohol use (g = 0.65, 95% CI: 0.31–0.99, p < 0.0001). Studies incorporating psychotherapy showed significantly greater effects (g = 1.38, 95% CI: 1.06–1.71, p < 0.0001) than those without (g = 0.60, 95% CI: 0.09–1.12, p < 0.0001), with significant subgroup difference (p = 0.0121). High risk of bias and high heterogeneity were observed (I2 = 96.9%), with effects varying by substance type and treatment context. No publication bias was detected.
Conclusion:
When combined, available studies demonstrate DMT’s potentially substantial post-treatment efficacy for substance misuse, particularly with psychotherapy. Effect magnitudes vary by abused substances. Included studies had substantial methodological limitations and high risk of bias. Reported effects should therefore be interpreted as preliminary rather than indicative of established efficacy. Furthermore, the use of exploratory subgroup analyses in this review can only conclude that DMT efficacy for treating alcohol and substance abuse disorders is highly heterogeneous, depending on study and treatment design. If sustained positive results are clearly demonstrated in future research, it might position DMT-assisted psychotherapy as an effective, economical alternative to conventional treatments.
Keywords
Introduction
Substance use disorders (SUDs) are characterized by compulsive drug or alcohol use despite adverse consequences and constitute a major global health burden with significant challenges (Rhemtulla et al., 2016). Addiction involves a complex interplay of neurobiological, psychological, and environmental factors. Repeated substance exposure can contribute to neuroadaptations across multiple neural systems, including (but not limited to) dopaminergic reward pathways, which may alter motivation, behavior, and decision-making processes (Volkow et al., 2019). Diagnostic and Statistical Manual of Mental Disorders (DSM-V) criteria for SUDs require two or more symptoms (craving, tolerance, withdrawal, loss of control) plus distress or functional impairment (American Psychiatric Association (APA), 2022). As defined by the International Classification of Diseases (ICD-11), SUDs affect approximately 1.4% and 0.9% of the global population for alcohol and drugs, respectively (World Health Organization (WHO), 2018; Rehm et al., 2020), with impacts extending beyond diagnosed individuals to the 20.5% of households with subclinical misuse (Gruber and Taylor, 2006). Societal burdens include substantial healthcare costs ($226 billion annually in the USA), reduced productivity, family disruption, criminal damages, and 3.3 million premature deaths annually (Caulkins et al., 2014; Hoffman and Goldfrank, 1990; Rehm et al., 2020; Orford et al., 2013). Studies of families and parents with SUD report of Children experiencing developmental, emotional, and economic challenges, including disruption of attachment styles, roles, routines, communication, and social life. Parental SUD is characterized by an environment of fear, secrecy, unpredictability, violence, abuse, and emotional chaos (Lander et al., 2013).
Standard first-line evidence-based interventions for SUDs combine psychological and pharmacological approaches based on neurobiological, cognitive, and psychosocial addiction models (APA, 2006, 2018; National Institute for Health and Care Excellence (NICE), 2009). Psychological interventions include cognitive-behavioral therapy (CBT), dialectical behavior therapy (DBT), acceptance and commitment therapy (ACT), and psychodynamic therapies, while pharmacological treatments include medications such as naltrexone (National Institute of Drug Abuse, 2020). Both categories demonstrate only modest efficacy by way of meta-analysis. CBT shows an effect size of g = 0.44 (95% CI: 0.02–0.86, p = 0.039) compared to minimal intervention (Magill et al., 2019). Evidence for Naltrexone demonstrates modest and inconsistent efficacy in opioid use disorders. A recent meta-analysis found no statistically significant pooled effects for treatment retention (OR = 1.64, 95% CI: 0.78–3.44) or end-of-treatment abstinence (OR = 1.63, 95% CI: 0.57–4.72) across formulations (Zangiabadian et al., 2022). Injectable naltrexone was the only formulation showing a significant benefit for treatment retention (OR = 1.86, 95% CI: 1.17–2.98), suggesting formulation-specific and limited clinical effectiveness. For alcohol use disorder, a meta-analysis of 118 randomized controlled trials found that oral naltrexone (50 mg/day) was associated with statistically significant but modest reductions in return to heavy drinking compared with placebo (RR = 0.81, 95% CI: 0.72–0.90, p < 0.001), with a number needed to treat of 11, while injectable formulations demonstrated limited and inconsistent benefits (McPheeters et al., 2023). This suggests distinct neurobiological mechanisms across substance types. Psychological approaches like CBT yield a non-significant advantage over pharmacotherapy alone (Ray et al., 2020), undermining the evidence for psychotherapeutic modalities and suggesting their placebo or indirect influence on substance use reduction. Combined therapies yield only low-to-moderate effect sizes (g = 0.18–0.28) with minimal to no advantages over monotherapy (Dellazizzo et al., 2023; McHugh et al., 2010; Ray et al., 2020), underscoring the need for novel, targeted, and cost-efficient interventions across substance categories.
Psychedelic therapies
Since the 2000s, psychedelic-assisted therapy has reemerged in research as a promising intervention for treatment-resistant psychiatric conditions, including SUDs (Hall, 2022). Therapeutic mechanisms of psychedelics are likely at the neural, biochemical, and psychological level. Classic psychedelics act as serotonergic 5-hydroxytryptamine 2A (5-HT2A) receptor agonists, producing altered states and increased neuroplasticity that facilitate therapeutic change through enhanced meaning-making and psychological flexibility (Madsen et al., 2019; Preller et al., 2017; Vargas et al., 2023).
Under these conditions, therapeutic outcomes are influenced by the client’s mindset (“set”) and contextual elements (“setting”), with suggestibility contributing to cognitive restructuring through neuroplasticity-enhanced bottom-up information processing, which helps adjust maladaptive thought and behavioral patterns (Cavarra et al., 2022).
Psychedelic-assisted psychotherapy (PAP) represents a specialized form of medication-assisted psychotherapy that incorporates usually discrete psychedelic dosing sessions rather than sustained pharmaceutical administration. It incorporates preparatory sessions to establish set and setting, supported psychedelic experiences, and subsequent integration sessions (Greer and Tolbert, 1998; Pahnke et al., 1970). CBT with psychedelic therapy demonstrates potential for SUDs, though benefits correlated most strongly with mystical experience intensity rather than specific cognitive interventions (Bogenschutz et al., 2015; Dakwar et al., 2019; Garcia-Romeu et al., 2014; Rothberg et al., 2021). The relative contributions of pharmacological versus psychotherapeutic elements remain debated, with some researchers emphasizing contextual influence (Hartogsohn, 2017; Leary, 1961) and others highlighting enhanced emotional breakthroughs (Roseman et al., 2019) or deepened psychological insights over neurobiological mechanisms alone (Peill et al., 2022). No studies have isolated the effects of these components through controlled trials, nor established the method’s advantages over psychedelics alone.
N, N-dimethyltryptamine (DMT) and its structural analog 5-methoxy-N, N-dimethyltryptamine (5-MeO-DMT) are emerging psychedelic candidates for SUD treatment. Plant-derived DMT is the psychoactive component in traditional Amazonian ayahuasca preparations, while 5-MeO-DMT occurs naturally in Incilius alvarius toad secretions and certain plants (Sherwood et al., 2020). Despite long indigenous healing histories (Delgrasso, 2024; Miller et al., 2019), these tryptamine alkaloids show only preliminary evidence linking their induced mystical experiences to improved psychological health and reduced tobacco use (Ferreira and Reis-Pina, 2025; Timmermann et al., 2024). Even so, traditional ayahuasca ceremonies have gained popularity in contemporary addiction treatment, attracting international participants to specialized healing centers (Kavenská and Simonová, 2015; Politi et al., 2018).
Recent reviews indicate that while ketamine (a non-classic psychomimetic anesthetic), lysergic acid diethylamide (LSD), and psilocybin have accumulated substantial evidence for SUD treatment, with LSD demonstrating clinical efficacy, research on DMT/5-MeO-DMT remains limited and inconclusive (Richard and Garcia-Romeu, 2025; Piper et al., 2025). Sparse and inconclusive evidence consists primarily of qualitative reports, ethnographic studies, case reports, cross-sectional surveys, and observational studies, with no randomized controlled trials (RCTs) examining SUD outcomes (Apud et al., 2022; Jiménez-Garrido et al., 2020; Talin and Sanabria, 2017). Both DMT analog compounds also show potential beyond SUDs for treating eating disorders, mood disorders, anxiety, Post-Traumatic Stress Disorder (PTSD), Obsessive-Compulsive Disorder, personality disorders, and suicidality (Gómez-Sousa et al., 2021; Jiménez-Garrido et al., 2020; Shinozuka et al., 2024), with 5-MeO-DMT also studied for pain and postpartum depression (Kargbo, 2024). Initial findings suggest benefits for treating substance abuse, but methodological limitations preclude definitive conclusions regarding the magnitude of efficacy or its mechanisms. Evidence remains insufficient to support clinical implementation of DMT compounds for SUDs.
Current study aims
This systematic review with meta-analysis is the first to address critical research gaps regarding the therapeutic effects of DMT/5-MeO-DMT on drug and alcohol substance use severity.
By pooling available quantitative data, the statistical analysis refines previously calculated effect sizes while attempting to distinguish pharmacological from psychological modality contributions. Objectives include (1) determining efficacy in reducing substance misuse, (2) evaluating whether psychotherapy enhances outcomes beyond DMT’s pharmacological effects, (3) exploring how treatment design variations influence clinical outcomes, and (4) synthesizing evidence to develop a conceptual understanding of likely therapeutic mechanisms. By addressing existing evidential limitations, this study aims to advance understanding of the therapeutic potential of DMT/5-MeO-DMTand its assisted psychotherapy for substance abuse.
Methods
Study design
This systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) standards (Page et al., 2021) and the Cochrane Handbook guidelines (Higgins and Thomas, 2019). The protocol was preregistered with the Open Science Framework (OSF.io/75KD9) prior to data collection. A meta-analytic approach was justified to increase statistical power, resolve study inconsistencies, and quantify more precise magnitude of effects for DMT/5-MeO-DMT interventions, given the relatively small samples in available studies. This systematic pooling of data allows for more precise effect estimates than individual studies can provide alone.
The research questions were formulated using the Population, Intervention, Comparison, Outcome, and Study design (PICOS) framework (Hosseini et al., 2024). Adults over 18 years old with SUDs or problematic substance use served as the population of interest, with DMT or 5-MeO-DMT administered as the investigated intervention, with or without adjunct psychotherapy. Placebo, active control, treatment as usual, or pre-post intervention observations served as acceptable comparators. Study designs considered included RCTs, quasi-experimental designs, and pre-post observational studies.
Substance abuse severity served as the primary outcome and dependent variable responding to DMT interventions (independent variable) and was selected due to its prevalence across studies using psychometric instruments that quantify problematic consumption patterns (Higgins et al., 2024a). Tools like the Addiction Severity Index (ASI), Alcohol Use Disorder Identification Test (AUDIT), and Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST) show high but variable reliability and validity due to self-reporting and less relevant subscale criteria (Mäkelä, 2004; Reinert & Allen, 2002; Selin, 2003; WHO ASSIST Working Group, 2002). These limitations were mitigated by using only substance use pattern subscales and considering self-report reliability in interpretations.
Studies employing adjunctive psychotherapy were isolated as a subgroup to determine differential effect sizes. Additional subgroup analyses explored the potential influence of population type (community vs clinical samples), drug formulation, and intervention duration (single-session vs multi-session protocols). This design enables a comprehensive evaluation of both overall efficacy and specific moderating or confounding factors that influence treatment outcomes.
Procedures
Search, screening, and selection strategy
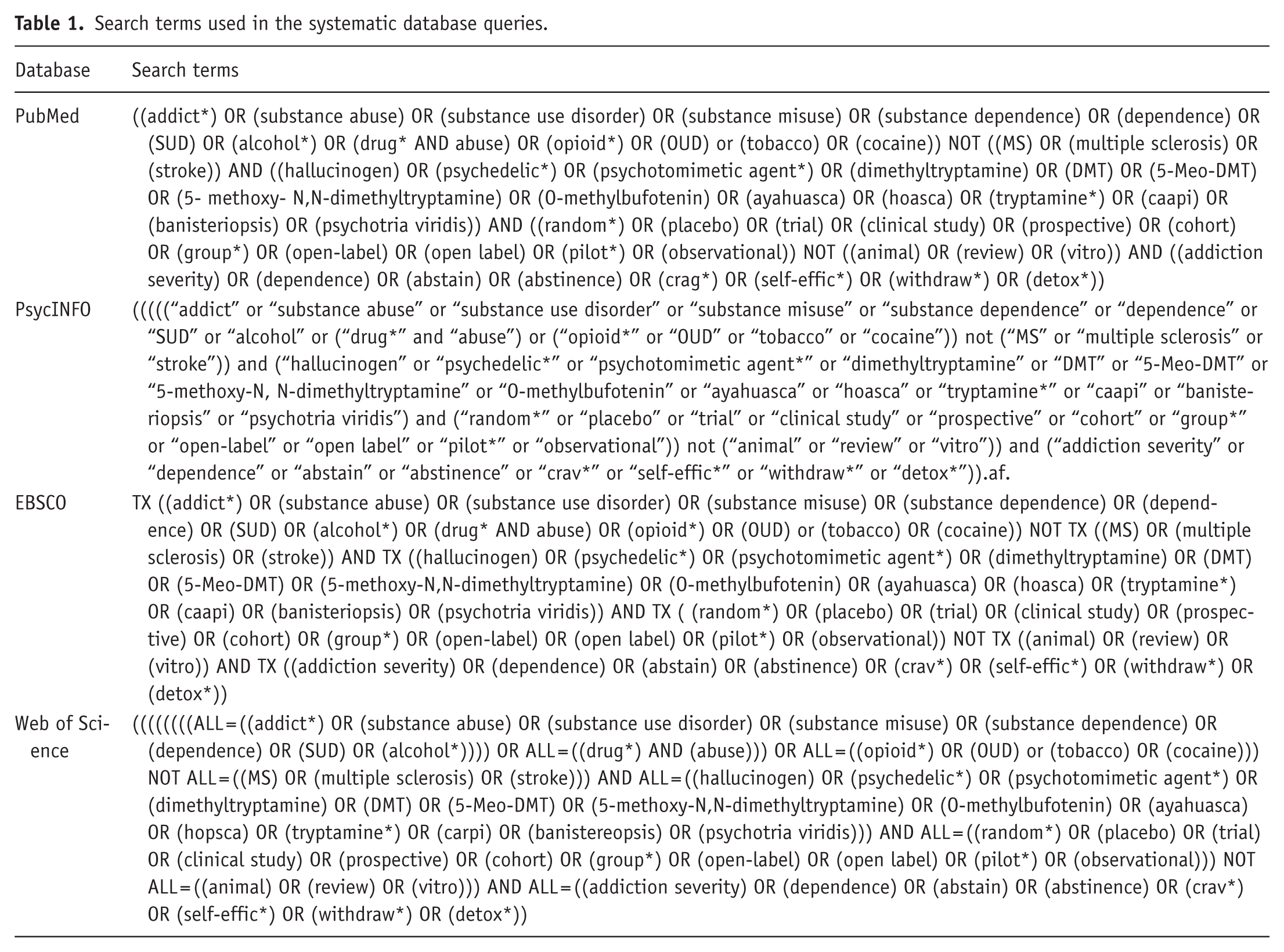
An extensive search in January 2025 across PubMed, PsycINFO, EBSCO, and Web of Science databases was supplemented by manual reference examination (Lefebvre et al., 2016; Page et al., 2021). Initial screening ended in January 2025, and newly published reviews were cross-referenced between February and March 2025 to ensure comprehensive study inclusion. Results were restricted to publications between January 1960 and December 2024, which was verified to span all DMT research. Additional sources were identified through forward and backward citation searching, expert consultation, and screening of relevant review articles. We also searched preprint servers (PsyArXiv, medRxiv) and clinical trial registries (ClinicalTrials.gov, EU Clinical Trials Register) to identify unpublished or ongoing studies. PICOS-directed search terms (Table 1) combined four conceptual blocks: (1) substance misuse (“addiction,” “SUD,” etc.), (2) DMT treatments (“dimethyltryptamine,” “ayahuasca,” etc.), (3) study designs (“clinical trial,” “observational study,” etc.), and (4) substance use outcomes (“addiction severity,” “abstinence,” etc.).
Search terms used in the systematic database queries.
Following result count verification, two investigators confirmed that the number of results and the first 20% of the publications matched to ensure replicability. Two people employed Rayyan software made by Rayyan Systems for manual deduplication and screening, first examining titles/abstracts before reviewing full texts of potential selections (Lefebvre et al., 2016). Inclusion and exclusion criteria were developed based on PICOS parameters underlying the research questions, informed also by previous reviews on psychedelic therapies and SUD treatments (McKenzie et al., 2024a). Selection criteria included: (1) adult participants with problematic substance use, (2) DMT or 5-MeO-DMT interventions, (3) substance use severity outcomes as continuous measures, and (4) clinical trials or prospective observational cohorts making within-group or between-group comparisons. Both monotherapy and the use of these psychedelic compounds as an add-on polytherapy treatment were considered. Due to blinding challenges with psychedelics, non-RCT studies were included. Exclusions included non-original research, retrospective studies, animal models, populations under the age of 18, cross-sectional surveys, case reports, and studies lacking baseline comparison measures or extractable data for calculating effect sizes. Finalist selections were subsequently evaluated by all investigators, with discrepancies resolved through consensus meetings.
The screening process was completed before the 2025 publication of reviews by Richard and Garcia-Romeu (2025). Later cross-referencing of these reviews identified 13 additional studies that were subsequently excluded due to methodological limitations. As illustrated in the PRISMA flow diagram (Figure 1), eight studies across seven reports met eligibility criteria for meta-analysis. These examined ayahuasca DMT or 5-MeO-DMT interventions on substance use outcomes through pre-post and longitudinal observational designs, with three including comparison groups. Settings varied from clinical programs to naturalistic ceremonial contexts.
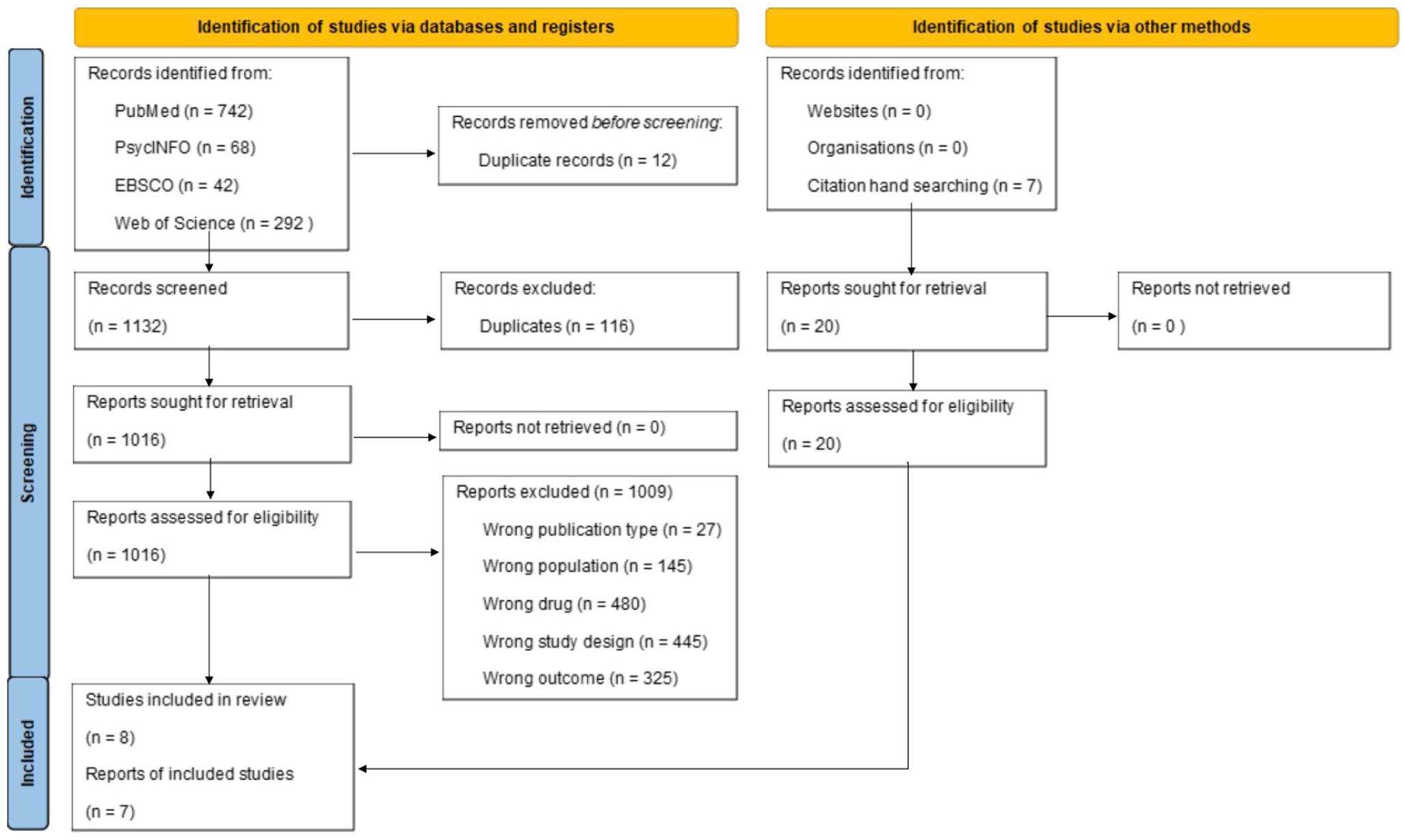
PRISMA 2020 flow diagram for systematic screening and review (adapted from Page et al., 2021). Licensed under CC BY 4.0.
Data extraction
Following Cochrane guidelines (Li et al., 2024), three investigators independently extracted data from the selected studies for synthesis and analysis. Data extracted from the selected studies included (1) study characteristics (design, location, outcome measuring instruments), (2) participant demographics (diagnostic criteria, mean age, gender proportions, substance use profiles, baseline, and post-intervention sample sizes), (3) intervention characteristics (compound formulation, dosage, additional drugs, treatment length, administration context, psychotherapy use), and (4) statistical data (baseline and post-treatment outcome mean, standard deviation, computed effect size with standard error).
Study characteristics were summarized to identify variables for sensitivity analysis and coded for use (McKenzie et al, 2024b). Missing data were requested from the original study authors, and imputation methods were applied after non-responsive attempts. Sample sizes required for an 80% powered finding were calculated for each study to be used in the quality assessment. One underpowered study was flagged during the quality assessment and still used in the data synthesis, with appropriate consideration and discussion of this single-study limitation. Finally, the effect sizes for alcohol and drug use reduction were calculated for each study as Hedge’s g with standard error (SE), based on pre- and post-intervention data only to maintain computational consistency.
Risk of bias and quality assessment
Two investigators evaluated study quality and risk of bias using two complementary tools. As the highest available standard, the Cochrane Risk of Bias 2.0 tool (Cochrane Methods, 2017; Higgins et al., 2024b; Sterne et al., 2019) evaluated bias across five domains: randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selective reporting (Higgins et al., 2024b). These domains assessed the risk of selection bias, performance bias, detection bias, attrition bias, and reporting bias, respectively. A low risk of bias designation required positive ratings across all domains. The Downs and Black Checklist for non-randomized and observational studies also assessed reporting, external validity, internal validity (involving confounding and selection bias), and statistical power (Downs and Black, 1998). The 27 checklist items receive scores of “yes” (1), “no” (0), or “unable to determine” (0), with domain scores summed to produce an overall quality index (QI), which demonstrates reliability and validity. Because all studies received high-risk and low-quality designations, ratings were not used to exclude studies; instead, they informed the interpretation of findings.
Analysis approach
A meta-analysis of pooled data was conducted to determine, with higher statistical power, the true effect size of DMT/5-MeO-DMT in reducing substance misuse. Sensitivity analyses examined potential therapeutic differences with adjunctive psychotherapy. A critical review and quality assessment, accompanied by exploratory subgroup analyses, were conducted to evaluate whether methodological variations contributed to outcome differences. The subgroups included: (1) interventions involving PAP, (2) community and clinical populations, (3) long-term therapy with more than one treatment session, and (4) polytherapy with concomitant use of a second psychedelic agent.
Data synthesis
Statistical analyses employed the “meta” package in R open source version 4.4.2 maintained by the R Core Team. Synthesized primary outcome effect sizes were calculated as standardized mean differences (SMDs) in Hedges’ g for drug and alcohol use with 95% confidence (CI) and prediction intervals (PIs) for substance use measures (Deeks et al., 2024). Because pre/post-intervention measurements are likely correlated but correlation coefficients are unpublished, analyses used a correlated effects model that assumed intra-study correlations of r = 0.2 (low), 0.5 (medium), and 0.8 (high) when estimating effect size (Pustejovsky and Tipton, 2021; Pustejovsky and Chen, 2023). Effect size values at each assumed correlation value were compared, and since no variations in SMD were noted, effect sizes at r = 0.5 were reported as results. Because all studies had high risk of bias, none were excluded as bias-defined outliers.
Because heterogeneity was anticipated, a random-effects model was employed with restricted maximum likelihood estimation for overall effects (Corbeil and Searle, 1976). Mixed-effects modeling was applied to subgroup analyses to retain a fixed effect for each specific subgroup factor while accounting for remaining random effects within subgroups (Brown, 2021). Heterogeneity at the 95% CI was quantified using I2 statistics with values of 25%, 50%, and 75%, indicating low, moderate, and high heterogeneity, respectively. τ2 designated between-study variance (Higgins, 2003). Heterogeneity parameters for subgroups were compared to identify likely moderators or confounders. Leave-one-out sensitivity analysis assessed the certainty of results. Publication bias was evaluated using Egger’s intercept test, along with visual inspection of funnel plots to detect asymmetry in published results. Critical review and quality assessment accompanied quantitative analyses to assess whether methodological variations contributed to outcome differences between substance categories and psychotherapy subgroups.
After requests for missing data went unanswered, Thomas et al. (2013) pre- and post-intervention substance use means were extrapolated from the report’s included chart, and absent standard deviations were imputed. Alternate standard deviation values from Rodrigues et al. (2024) were substituted, as that study had the most similar sample size (n = 11), with the caveat that it was underpowered and only reported alcohol use. For imputed drug use data, we used the standard deviation values from Rush et al. (2024) due to similar study characteristics, such as a clinical population, a larger sample size than other studies (Berlowitz et al., 2019), and long-term treatment. The results of subgroup analyses were similar when the imputed data from Thomas et al. (2013) were excluded, indicating that no accuracy issues resulted from these imputation methods.
Factor analyses
Subgroup analyses were conducted to explore possible factors that might moderate or confound DMT’s treatment effectiveness beyond adjunctive psychotherapy. Given the small number of included studies and high heterogeneity, these analyses should be considered preliminary indicators only. These exploratory subgroups included: (1) community vs clinical populations, (2) single-session short-term treatment versus long-term therapy with more than one treatment session, and (3) psychedelic drug formulation. Like the overall meta-analysis, all subgroup analyses include the imputed data from Thomas et al. (2013), and those results were verified by re-running the analysis without the imputed data, wherein results remained stable.
For the subgroup analysis examining whether session duration moderated the effects of DMT on substance use reduction, groups were defined by the number and frequency of doses. Four studies included more than 3 doses over weeks to months (Berlowitz et al., 2019; Fábregas et al., 2010; Rush et al., 2024; Thomas et al., 2013) and were coded as multi-session treatment paradigms. Three studies included three or fewer doses in a single day (Armstrong et al., 2023; Perkins et al., 2022; Rodrigues et al., 2024) and were coded as single-session therapies.
Because only one study delivered inhalant 5-MeO-DMT polydrug therapy with ibogaine, rather than orally administered ayahuasca (Armstrong et al., 2023), the differences resulting from this formulation difference were assessed using the leave-one-out approach, rather than sensitivity analysis by subgroups. Because all but one study (Thomas et al., 2013) employing psychotherapy included both individual and group delivery methods, the specific effects of these methods could not be differentiated.
Results
Study selection
The electronic and hand searches of the literature yielded 1132 results, 116 of which were eliminated as duplicates. A total of 1009 reports were removed from screening because they failed to meet the required inclusion criteria. The PRISMA flow diagram in Figure 1 illustrates the study selection and screening outcomes, in which eight studies across seven reports were ultimately eligible for inclusion in the meta-analysis. These studies, published between 2010 and 2024, examined the effects of ayahuasca DMT or 5-MeO-DMT interventions on substance use outcomes using a mix of pre-post and longitudinal observational designs. Three studies included comparison or control groups, while the others employed single-group designs. One between-group comparison study employed a single-blinded design using a psychoactive placebo (Rodrigues et al., 2024), while two others in a single report longitudinally examined the effects of ritual use in urban and jungle communities, comparing outcomes with those of urban and rural general population samples, respectively (Fábregas et al., 2010). Intervention settings ranged from structured clinical programs to naturalistic or ceremonial community contexts.
After thorough screening, the more recently published reviews by Richard and Garcia-Romeu (2025) and Piper et al. (2025) were cross-referenced, wherein 13 additional DMT and 5-MeO-DMT studies were considered but ultimately excluded due to methodological limitations. Five studies (in four reports) originally selected initially for the current meta-analysis were also included in one or both of the 2025 reviews: Armstrong et al. (2023), Berlowitz et al. (2019), Fábregas et al. (2010), and Thomas et al. (2013). Three other studies included in our meta-analysis—Perkins et al. (2022), Rodrigues et al. (2024), and Rush et al. (2024)—were not captured in either of the other recent reviews.
Characteristics of the included studies
Participant characteristics
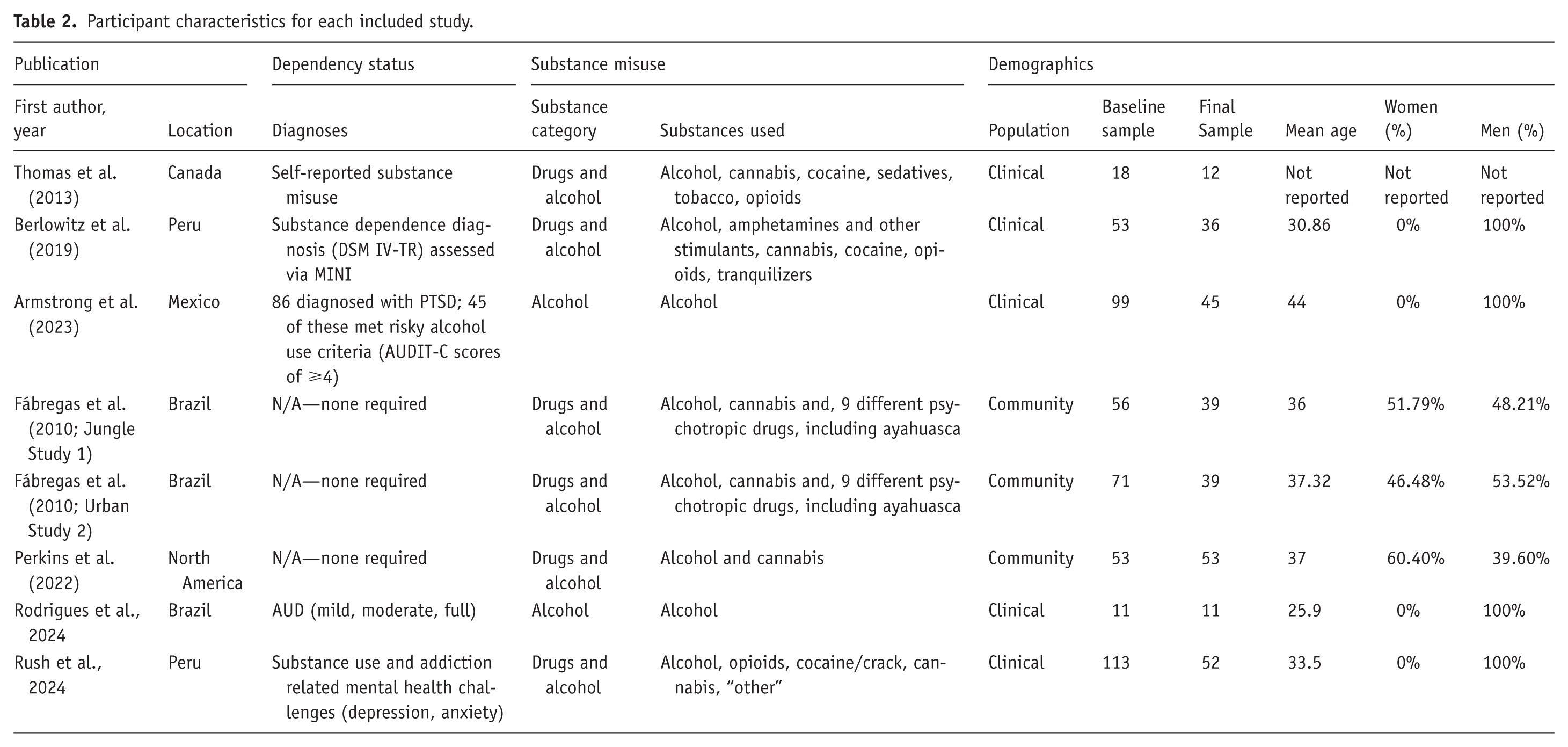
The pooled sample (Table 2) was comprised of 456 baseline participants (mean age 36.6 years, 79% male) with diagnosed or reported drug or alcohol misuse, with four of the eight studies being all-male. Substances of abuse included alcohol (exclusively examined in two studies) and various drugs across stimulant, sedative, cannabis, opioid, and psychotropic categories. Only one study by Armstrong et al. (2023) included individuals diagnosed with both PTSD and comorbid alcohol abuse, while other studies varied in their reporting of psychiatric comorbidities. Post-treatment assessments retained only 287 participants in total, representing a 37% attrition rate. While Hedge’s g effect size statistic was used here to compensate for small, changing samples, none of the studies employed intention-to-treat (ITT) methods to account for participant data losses in a conservative analysis that interprets dropouts as treatment failure (Gupta, 2011).
Participant characteristics for each included study.
Study characteristics
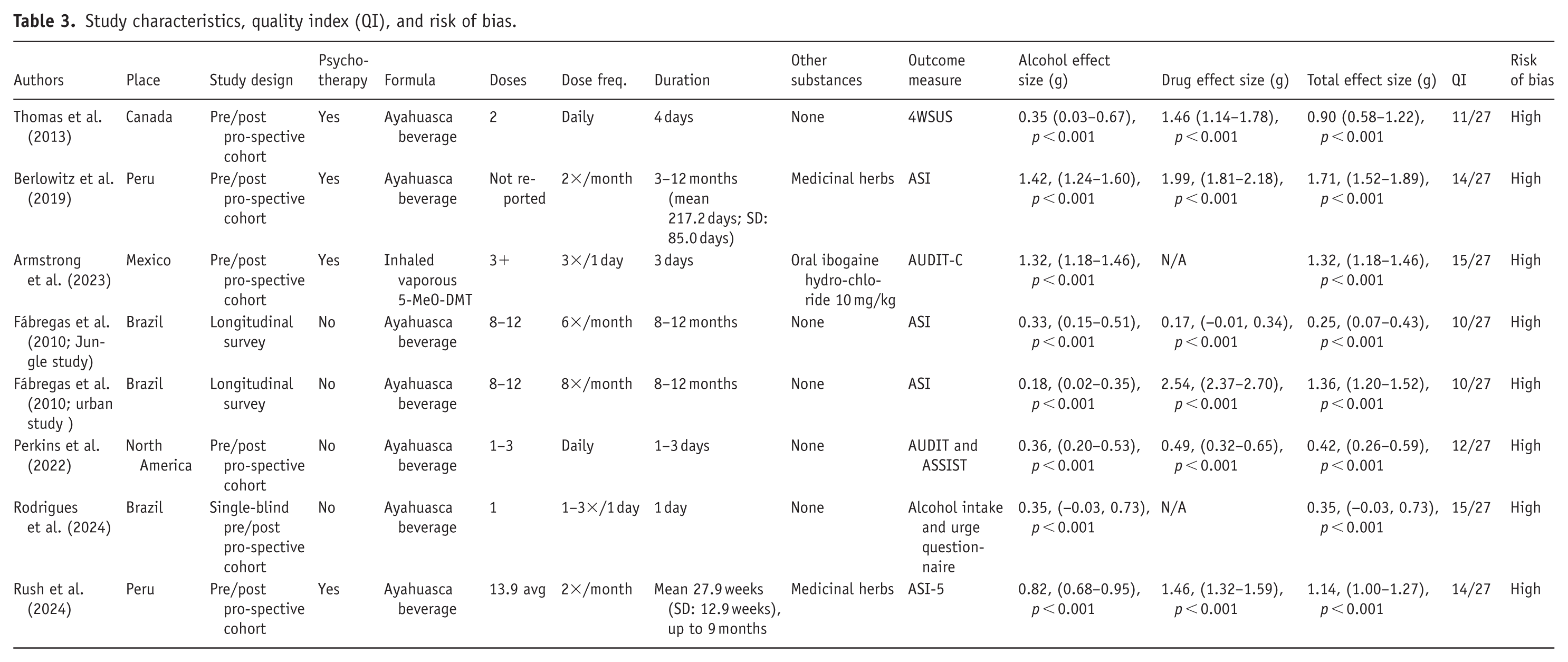
The included studies likewise exhibited heterogeneity in substances addressed and intervention design (Table 3).
Study characteristics, quality index (QI), and risk of bias.
Alcohol and drug abuse treatment
Six studies examined changes in both alcohol and drug misuse outcomes (Berlowitz et al., 2019; Fábregas et al., 2010; Perkins et al., 2022; Rush et al., 2024; Thomas et al., 2013), while two studies focused exclusively on alcohol-related measures (Armstrong et al., 2023; Rodrigues et al., 2024). Because psychedelic treatment may interact differently with substance-specific psychological patterns and addiction narratives, these differences were accounted for by calculating separate pooled effect sizes for abuse of drugs and alcohol.
Intervention design
Psychedelic formulations varied across studies, with six studies employing DMT administered orally as ayahuasca and one using inhaled 5-MeO-DMT 2 days after oral ibogaine. While two ayahuasca studies from Peru’s Takiwasi Center employed identical protocols that integrated traditional Amazonian plant medicine and Western addiction rehabilitation approaches (Berlowitz et al., 2019; Mabit et al., 1996; Rush et al., 2021, 2024), the remaining studies applied diverse methodologies and therapeutic frameworks. Four studies provided post-session psychotherapy in individual and group settings (Armstrong et al., 2023; Berlowitz et al., 2019; Rush et al., 2024; Thomas et al., 2013), while four provided no psychotherapeutic support (Fábregas et al., 2010; Perkins et al., 2022; Rodrigues et al., 2024). No details were provided about the specific therapeutic frameworks used.
Outcome measures
Substance use severity was assessed with several validated instruments, including ASI, AUDIT-C, ASSIST, and alcohol intake questionnaires such as the 4-week substance use scale (4WSUS). Overall, these scales have been ruled adequately valid and reliable for clinical and research use, contributing to study homogeneity (Mäkelä, 2004; Reinert and Allen, 2002; Selin, 2003; WHO ASSIST Working Group, 2002).
Treatment length and follow-up
All eight studies included in this study indicated at least one follow-up assessment after the intervention. For the meta-analysis, only the first post-intervention outcome was used to guarantee consistency and avoid confusing effects from long-term or repeated measures. Treatment duration varied substantially (1 day to 12 months), reflecting diverse dosing schedules ranging from single psychedelic administration sessions (k = 3) versus multiple sessions over extended weeks or months (k = 4). Changing the intensity and duration of treatment is an indication of the variance of therapeutic philosophies and resource availability.
Risk of bias
Cochrane’s systematic assessment of bias revealed that all studies demonstrated high overall risk, wherein as little as one high-risk domain automatically results in a high overall rating (Cochrane Methods, 2017). Studies uniformly demonstrated high risk in domains one (randomization), two (intended interventions), and four (outcome measurement) due to non-randomized designs and unblinding (Figure 2). These pervasive limitations indicate consequential risk of selection, performance, and attrition bias across all included studies. Detection bias (domain three) varied based on the randomness of missing data, with high-risk designation for unaddressed data absences. Within-study reporting bias (domain five) was frequently problematic due to inadequate reported protocol adherence. These deficiencies warrant a conservative interpretation, as directional bias, unblinded expectancy effects, and selective reporting may inflate effect sizes and compromise confidence intervals—considerations that are integrated into our results interpretation.
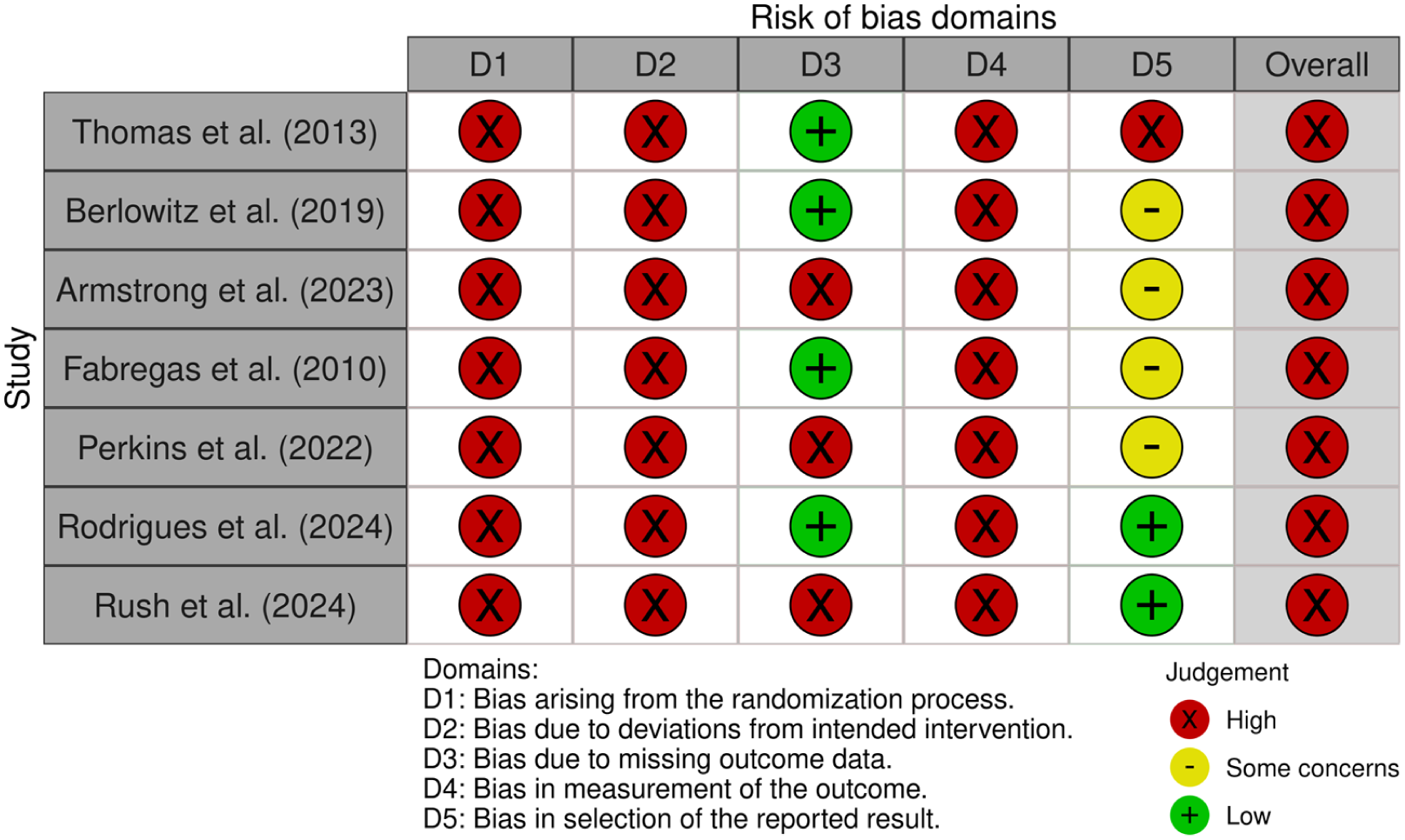
Risk of bias for each of the included studies (McGuinness and Higgins, 2020). Licensed under CC-BY-NC-ND 4.0.
Quality index assessment
The Downs and Black Checklist (Supplemental Appendix A) revealed variable methodological quality across studies, as indicated by quality index (QI) scores in Table 3. Reporting clarity and design descriptions were generally adequate. However, studies predominantly used uncontrolled, single-arm, unblinded designs and neglected ITT analytic methods that address participant attrition (Gupta, 2011). External validity was limited but similar across studies, which did not report on the representativeness of the sample compared to the populations from which they recruited. Internal validity weaknesses included predominantly unblinded designs (except Rodrigues et al., 2024) and single-arm interventions. Internal validity was similarly limited across studies due to the non-randomized design and the inclusion of only one intervention group without controls. Participant loss to follow-up was generally accounted for across studies unless unspecified or undeterminable (Fábregas et al., 2010; Perkins et al. 2022). All studies except Rodrigues et al. (2024) achieved >80% statistical power with an adequate sample size. The single-study deficit and generally small studies are compensated for by combining study data and using Hedge’s g effect size equation for small samples.
Meta-analysis
Treatment effects
The eight selected studies measured effect sizes by comparing post-treatment substance use severity to pre-treatment baseline measures (Supplemental Appendix B). Figure 3 presents forest plots of individual studies and pooled effect sizes with 95% confidence intervals for combined substance use, drug, and alcohol use. As seen in Figure 3(a), the total overall pre- to post-treatment effect size for reducing substance use severity was large at g = 0.94 (95% CI: 0.56–1.31, p < 0.0001; Durlak, 2009). When isolated to drug use alone, as seen in Figure 3(b), the effect size was even greater at g = 1.35 (95% CI: 0.63–2.07, p < 0.0001), compared to a moderately high alcohol use effect size of g = 0.65, as seen in Figure 3(c) (9%% CI: 0.31–0.99, p < 0.0001). Synthesized results were verified through a sensitivity analysis, systematically removing each study one at a time from calculations to identify changes in overall effect sizes. This revealed no significant alterations to the overall effects, confirming the accuracy of the findings. Egger’s test of the intercept revealed no significant publication bias (β0, p = 0.51), indicating a symmetrical distribution of results, which was confirmed by inspection of the funnel plot (Figure 4).
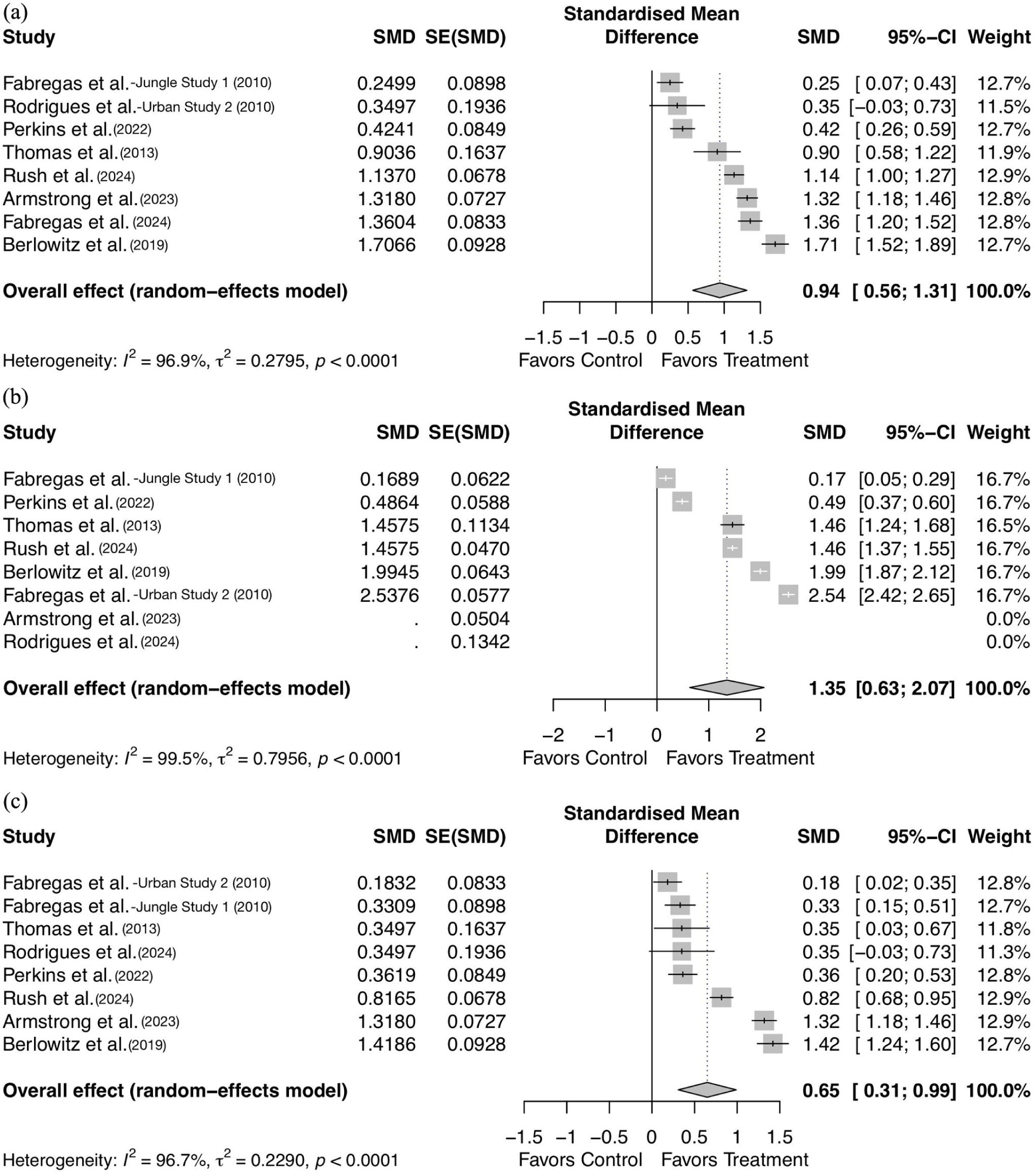
Forest plots of effect sizes. (a) Forest plot of total combined substance use effect sizes (r = 0.5), (b) Forest plot of drug use effect sizes (r = 0.5), and (c) Forest plot of alcohol use effect sizes (r = 0.5).
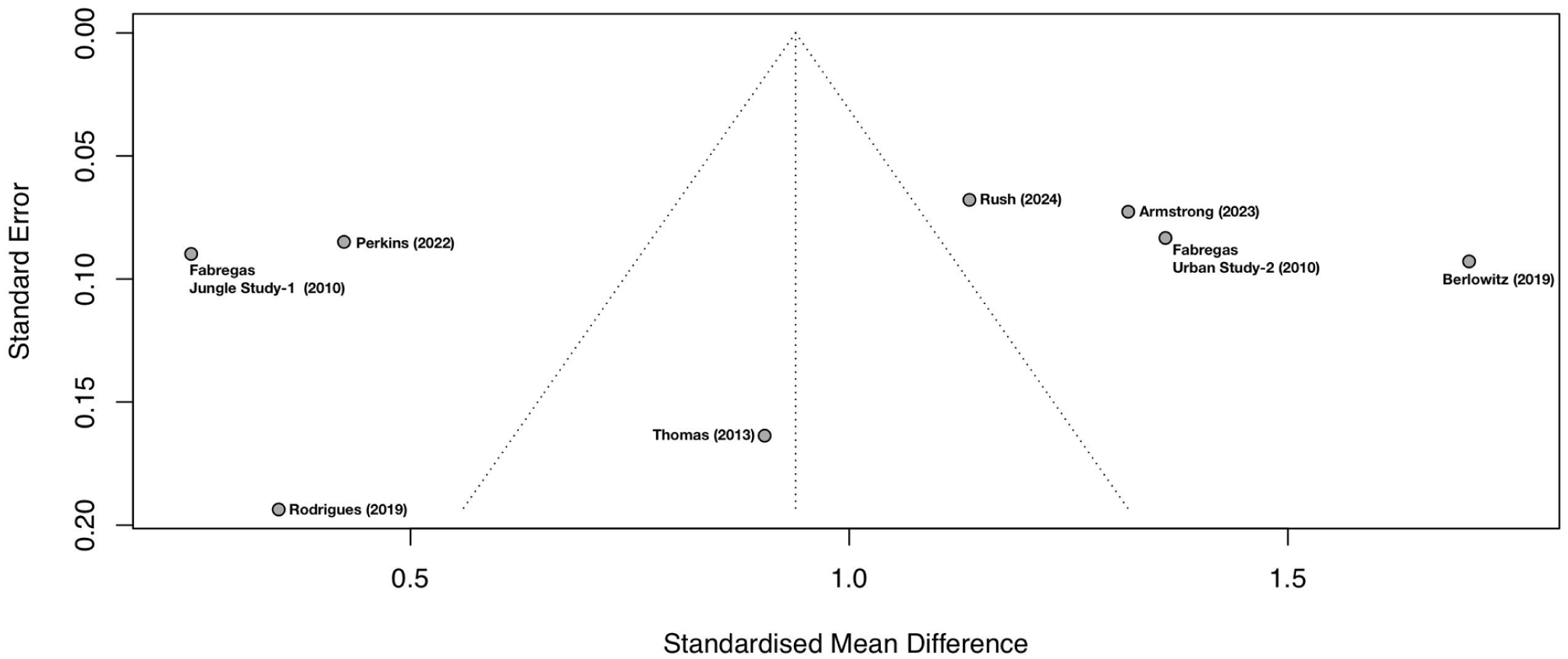
Funnel plot of all study results illustrating the symmetrical distribution of effect sizes (in Hedge’s g at r = 0.5).
Overall heterogeneity before analysis by subsets indicated moderate between-study variance of τ2 = 0.28 (95% CI: 0.12–1.19, p < 0.0001), and a high proportion of variance due to heterogeneity at I2 = 96.9% (95% CI: 95.5%–97.9%, p < 0.0001. The use of psychotherapy as an adjunct treatment is a primary source of heterogeneity, as are other aspects of intervention and study design.
Psychotherapy’s moderating effects
When stratified by the presence of psychotherapy as seen in Figure 5(a), studies that incorporated adjunct psychotherapy (k = 4) demonstrated a very large and statistically significant pooled effect size (g = 1.28, 95% CI: 0.96–1.60, p < 0.0001) and substantial heterogeneity (I2 = 90.3%, τ2 = 0.096, p < 0.0001). In contrast, studies without psychotherapy (k = 3) yielded a medium but still statistically significant effect size (g = 0.60, 95% CI: 0.09–1.12, p < 0.0001) with substantial heterogeneity (I2 = 97%, τ2 = 0.26, p < 0.0001). The test for subgroup differences was statistically significant (p = 0.0287), indicating that psychotherapy may have significantly moderated the effect of DMT treatments on substance use severity.
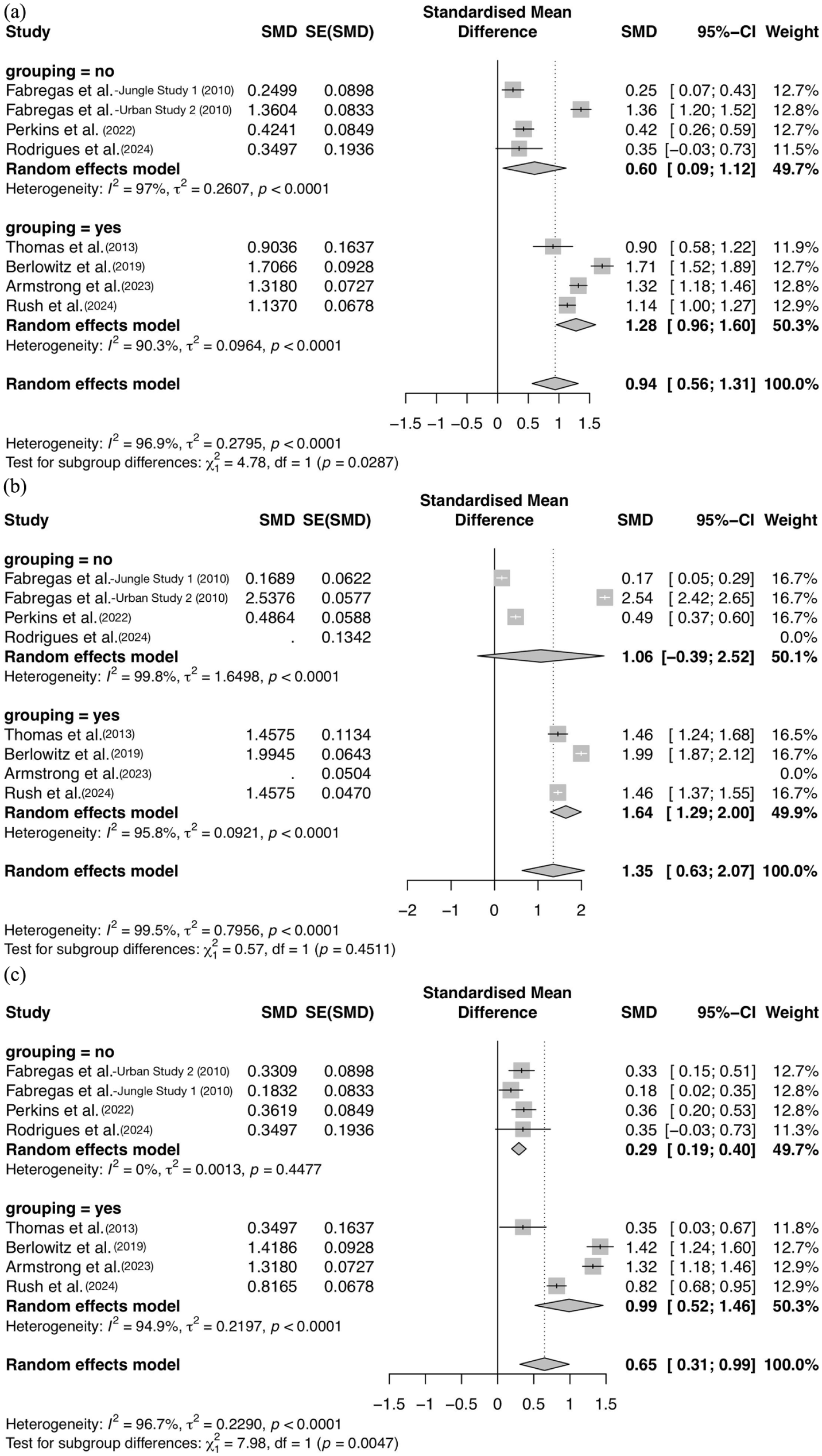
Forest plots of the effect sizes for substance misuse severity reduction in groups of studies with and without adjunct psychotherapy use. (a) Forest plot of total substance use (alcohol and drug) effect sizes (r = 0.5), (b) Forest plot of the drug misuse reduction effect sizes in groups of studies with and without adjunct psychotherapy use, and (c) Forest plot of the alcohol misuse reduction effect sizes in groups of studies with and without adjunct psychotherapy use.
As seen in Figure 5(b), drug use severity was reduced with the largest substance-specific effect size when psychotherapy was employed (k = 4, g = 1.64, 95% CI: 1.28–2.00, p < 0.0001), demonstrating substantial heterogeneity as usual (I2 = 91.3%, τ2 = 0.088, p < 0.0001). In contrast, studies without psychotherapy (k = 3) yielded a smaller but still large effect size (g = 1.06, 95% CI: −0.39, 2.52, p < 0.0001), also with substantial heterogeneity (I2 = 99.6%, τ2 = 1.65, p < 0.0001). However, the chi-squared (χ2) test for subgroup differences was not statistically significant (p = 0.45), implying that substance-specific inferences cannot be made about psychotherapy’s mediating role in addressing drug misuse with DMT specifically.
As seen in Figure 5(c) for alcohol use, studies that incorporated adjunct psychotherapy (k = 4) demonstrated a large and statistically significant pooled effect size (g = 0.99, 95% CI: 0.52–1.46, p < 0.0001) with substantial heterogeneity (I2 = 94.9%, τ2 = 0.22, p < 0.0001). Studies without psychotherapy (k = 3) yielded a far smaller effect size (g = 0.29, 95% CI: 0.19–0.40, p < 0.0001) with no statistically significant determinable heterogeneity (I2 = 0%, τ2 = 0.0013, p = 0.45). The χ2 test for subgroup differences, however, was statistically significant (p = 0.0047), indicating the significance of psychotherapy’s role in moderating the effects of DMT-based therapy for reducing alcohol use severity.
Clinical and community populations
A subgroup analysis examining whether having a community (k = 3) or clinical (k = 5) sample may have influenced substance use outcomes found that the total effect size for clinical samples was very large (g = 1.10, 95% CI: 0.68–1.53, p < 0.0001) and moderately high for community samples (g = 0.68, 95% CI: 0.00–1.35, p < 0.0001), as seen in Figure 6(a). The analysis revealed substantial heterogeneity of results across both community (I2 = 92.6%, τ2 = 0.22, p < 0.0001) and clinical groups (I2 = 98%, τ2 = 0.35, p < 0.0001), while the test for subgroup differences was not significant (p = 0.30).
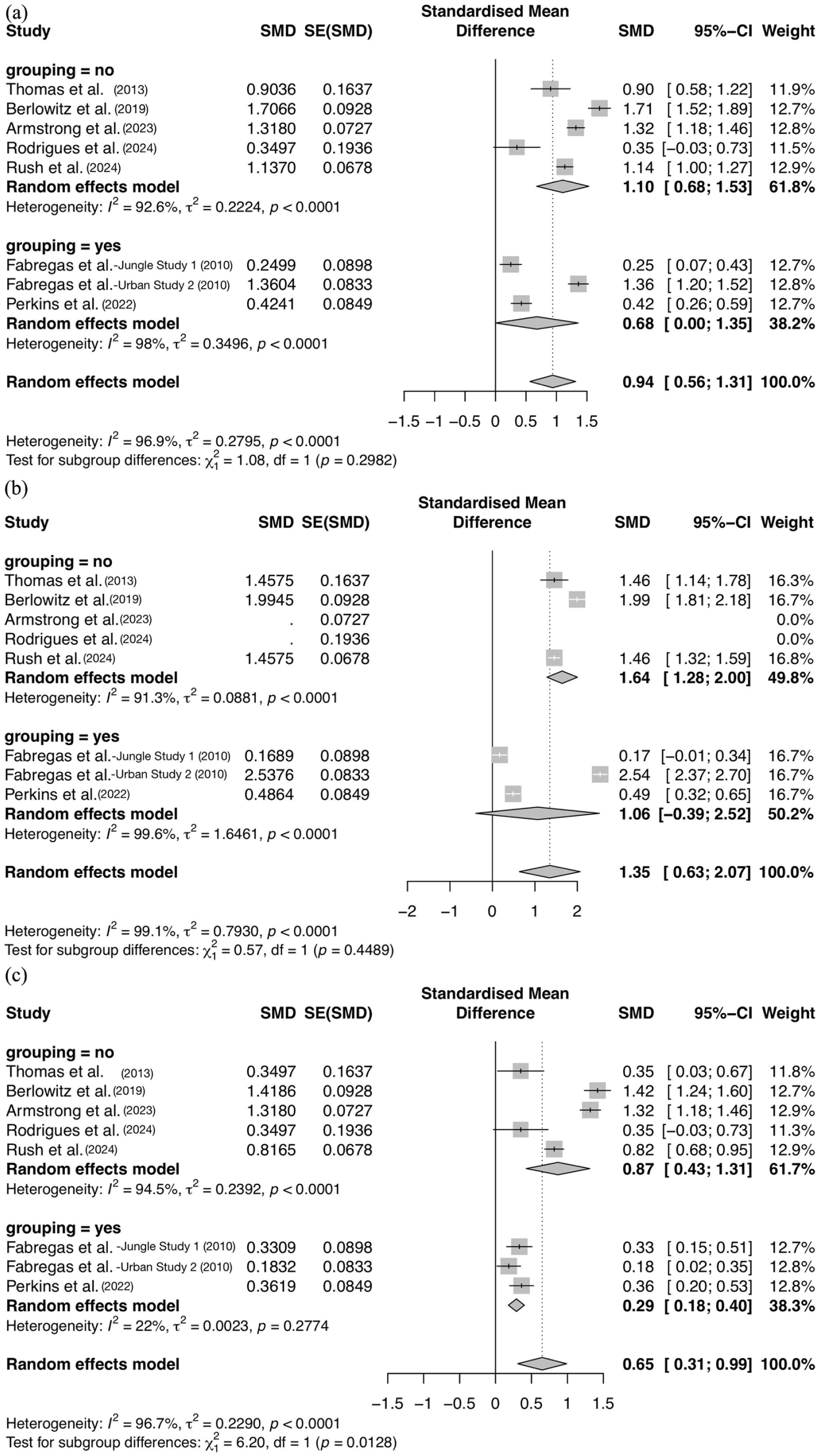
Forest plots of effect sizes segmented by groups of studies with community and clinical populations. (a) Forest plot of total substance misuse severity reduction effect sizes by population type, (b) Forest plot of drug use reduction effect sizes by population type, and (c) Forest plot of alcohol use reduction effect sizes by population type.
As seen in Figure 6(b), when isolated to drug use, the effect size was greater for both clinical samples (g = 1.64, 95% CI: 1.28–2.00, p < 0.0001) and community samples (g = 1.06, 95% CI: −0.39, 2.52, p < 0.0001), which reflects overall substance-specific effect size patterns. Substantial heterogeneity persisted across studies in both clinical (I2 = 91.3%, τ2 = 0.088, p < 0.0001) and community groups (I2 = 99.6%, τ2 = 1.65, p < 0.0001), and the test for subgroup differences was again not significant (p = 0.45).
The only statistically significant differences resulting from population type were for alcohol use reduction effect sizes (p = 0.013 for the Chi-squared test), where the clinical group had a moderately large effect size of g = 0.87 (95% CI: 0.43–1.31, p < 0.0001) and substantial heterogeneity across studies (I2 = 94.5%, τ2 = 0.24, p < 0.0001), as seen in Figure 6(c). Community samples had a medium-low effect size of g = 0.29 (95% CI: 0.18–0.40, p = 0.28) and far lower outcome heterogeneity (I2 = 22%, τ2 = 0.0023, p = 0.28).
Treatment length
As seen in Figure 7(a), the large total effect size for reducing all substance use when receiving short-term DMT treatment with up to three doses in one single session was g = 0.71 (95% CI: 0.09–1.33, p < 0.0001) with sustained high heterogeneity across these studies (I2 = 97.2%, τ2 = 0.28, p < 0.0001). The even larger total effect size for long-term multi-session therapy was g = 1.07 (95% CI: 0.59–1.56, p < 0.0001), also with substantial heterogeneity across the group’s studies (I2 = 97.2%, τ2 = 0.29, p < 0.0001). Despite the gap between effect sizes, the test for subgroup differences was not significant (p = 0.36), as seen in Figure 7(a).
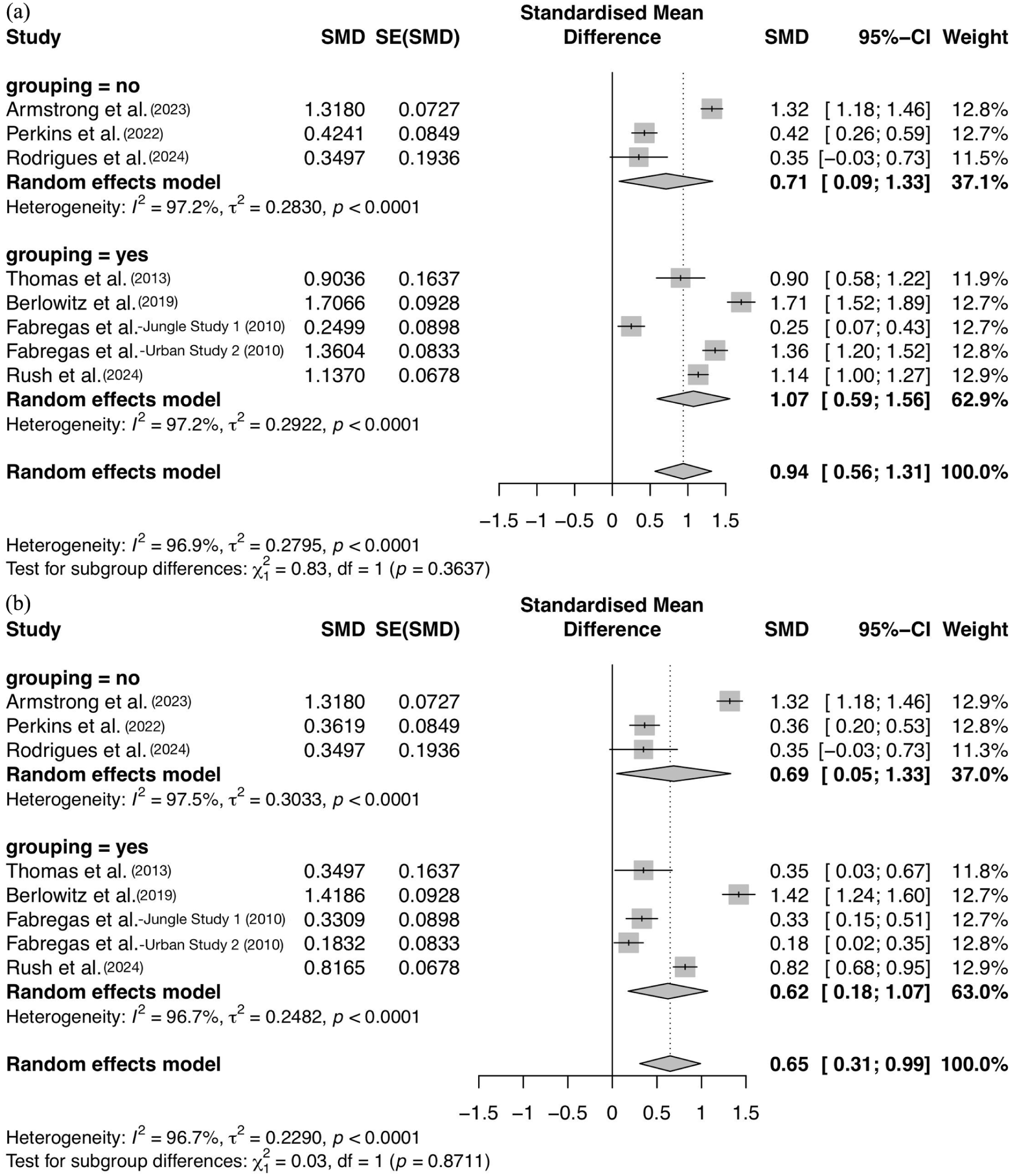
Forest plots of effect sizes segmented by groups of studies with short- and long-term treatment duration. (a) Forest plot of total substance misuse severity reduction effect sizes by treatment duration, (b) Forest plot of alcohol use reduction effect sizes by treatment duration.
As seen in Figure 7(b) for alcohol use, the effect size was larger for single-session therapy with an effect size of g = 0.69 (95% CI: 0.05–1.33, p < 0.0001), while that of multisession therapy was g = 0.62 (95% CI: 0.18–1.07, p < 0.0001). The analysis continued to reveal substantial heterogeneity across studies in both groups: short-term therapy (I2 = 97.5%, τ2 = 0.30, p < 0.0001) and long-term therapy (I2 = 96.7%, τ2 = 0.25, p < 0.0001). Again, the test for subgroup differences here showed that the difference in alcohol use outcomes due to treatment duration was not significant (p = 0.87).
Subgroup analysis for treatment length could not be conducted for drug use reduction, as there was only one single-session study addressing drug use (Perkins et al., 2022). However, a leave-one-out analysis omitting only Perkins et al. (2022) suggests that the study does slightly reduce the overall drug use effect size (Δg = −0.17, Δp = −0.0001), as represented by line 6 of Figure 8.
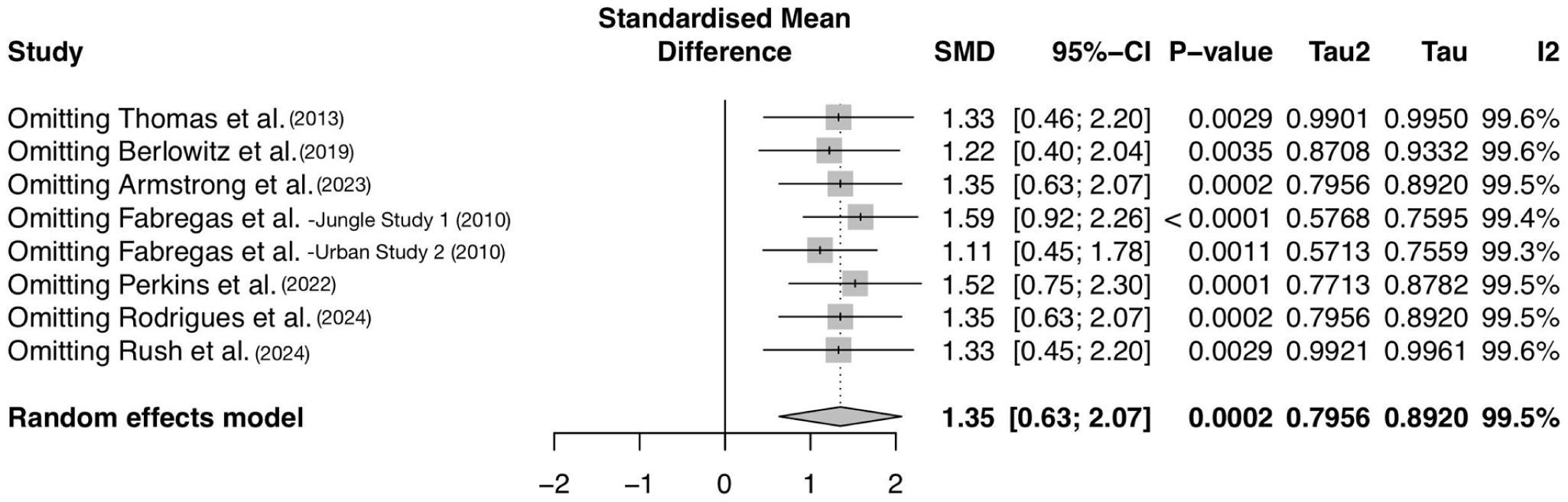
Forest plot of drug use reduction pooled effect sizes resulting from the omission of each study. Omitting Perkins et al. (2022) in line 6 represents changes in the pooled drug use reduction effect size due to the removal of a short-term single-session treatment study.
Drug formulation
An exploratory leave-one-out sensitivity analysis omitted the single inhalant 5-MeO-DMT polydrug therapy study (Armstrong et al., 2023) to assess its impact on the pooled effect sizes for alcohol use outcomes. The Armstrong et al. (2023) study only assessed differences in alcohol abuse patterns and did not address drug use, so substance-agnostic generalizations cannot result from this approach. Removing the Armstrong et al. (2023) study led to a modest shift in both SMD (Δg = −0.10) and p-value (Δp = +0.0008). Overall, the pooled alcohol use effect size remained largely consistent after removal of this study with an alternative drug formulation, as charted by the forest plot in line 3 of Figure 9.
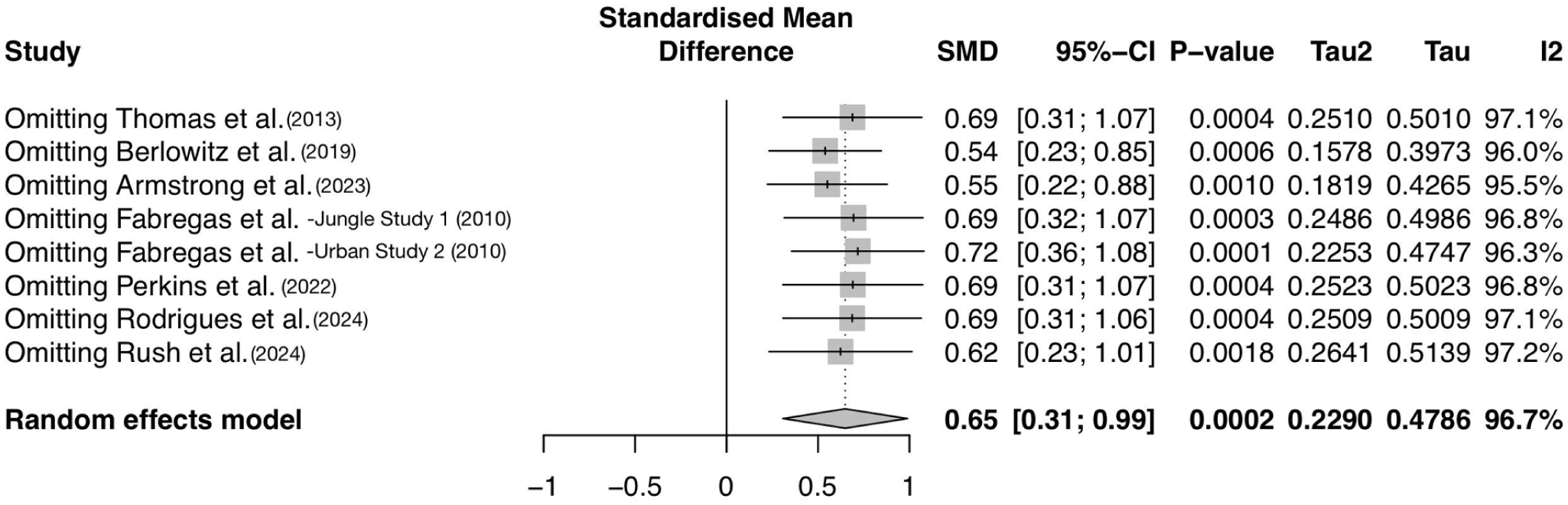
Forest plot of alcohol use reduction pooled effect sizes resulting from the omission of each study. Omitting Armstrong et al. (2023) in line 3 represents changes in the pooled alcohol use reduction effect size due to the removal of a study treating with inhalant 5-MeO-DMT after oral ibogaine.
Discussion
This meta-analysis represents the first systematic evaluation of DMT analog efficacy for substance abuse (Lovakov and Agadullina, 2021). It is also the first to preliminarily demonstrate that studies incorporating psychotherapy showed significantly larger effects than those without suggesting genuine additive or moderating effects. DMT and 5-MeO-DMT as similar analogs together demonstrated potential to significantly reduce substance abuse severity from baseline, aligning with the findings of other psychedelic meta-analysis targeting depression and anxiety (Yao et al., 2024) and with reviews supporting LSD’s efficacy for SUDs (Davis et al., 2019: 9; Richard and Garcia-Romeu, 2025). Substantially augmented effects with psychotherapy diverged from conventional pharmacological–psychological combinations, indicating unique synergism with psychedelics. Surprisingly, drug use changes showed superior outcomes to alcohol use, indicating distinct substance-specific therapeutic mechanisms for these categories. The absence of publication bias supports the internal consistency of the available evidence. However, given the low methodological quality and heterogeneity across studies, conclusions regarding the effectiveness of DMT interventions remain preliminary. While the intervention shows potential, higher quality and replicated outcomes are required.
Proposed mechanisms
The magnitude of observed effects may stem from DMT’s neurobiological mechanisms, therapeutic alliance, contextual factors, or a combination of these factors. Like LSD, DMT analogs might outperform conventional medications through 5-HT2A receptor agonism, enhancing neuroplasticity, and creating opportunities for psychological change (Cavarra et al., 2022; Vargas et al., 2023). Across modalities, trusting therapeutic relationships predict outcomes (Del Re et al., 2021), while set and setting generate non-pharmacological effects that correlate with improved well-being (Borkel et al., 2023; Hartogsohn, 2016). Psychedelics’ enhanced environmental suggestibility potentially amplifies therapeutic effects within ceremonial contexts, explaining why traditional Amazonian healing centers demonstrated particularly robust outcomes (k = 2, g = 1.99, 1.46), with cultural and ritual elements perhaps optimizing responses (Berlowitz et al., 2019; Rush et al., 2024). These contextual factors, while therapeutic, contributed to heterogeneity, consistent with the influence of set and setting on psychedelic effects (Hartogsohn, 2016). Existing evidence cannot differentiate pharmacological effects from contextual influences or distinguish specific from non-specific mechanisms. As such, interpretations remain preliminary.
Substance-specific effects
The larger effect sizes observed for drug use compared to alcohol use may reflect differences in underlying mechanisms, different measuring instrument sensitivities, and drug diversity among stimulant, sedative, opioid, and psychotropic substances. Notably, two studies reported minimal or non-significant reductions in cannabis use following ayahuasca exposure (Fábregas et al., 2010; Thomas et al., 2013), while Perkins et al. (2022), which assessed only alcohol and cannabis outcomes, reported smaller drug-related effect sizes than most other studies. This pattern suggests that cannabinoids may possess distinct properties affecting their responsiveness to DMT intervention. Still, definitive conclusions cannot be drawn due to potential confounding from persisting cultural, religious, or medicinal cannabis practices—especially in Indigenous settings (Balant et al., 2021). DMT’s effect size for drug use reduction is likely understated when including this cannabis data. Overall, differences between drug and alcohol outcomes may reflect substance-specific neurobiological interactions (Johansson et al., 2006). These differences may result from varying neurotransmitter system involvement, as all abused substances affect dopaminergic reward systems to different degrees, while alcohol affects a wider range of neurotransmitters (Tomkins and Sellers, 2001).
Moderating and confounding factors
Psychotherapy
Subgroup analysis revealed significantly larger effect sizes in studies that incorporated psychotherapy, suggesting that psychotherapy likely significantly moderates the effects of DMT treatment. This contrasts with conventional therapies, where CBT shows no adjunctive advantage to pharmacotherapy (Ray et al., 2020) and suggests an effect through distinctly different mechanisms made available by DMT’s action. A statistically significant difference between groups with and without psychotherapy for alcohol use reduction, but not drug use reduction, further implies differences in substance-specific mechanisms of action.
A subgroup analysis on the implemented mode of psychotherapy (group or individual) was unfortunately not feasible, as all studies that included psychotherapy used both group and individual psychotherapy together. The only exception was the Thomas et al. (2013) study, which used only group psychotherapy. Literature shows that group-delivered psychotherapy may influence treatment outcomes in terms of group verbal sharing and processing of the psychedelic experience to support the integration of the experience (Loizaga-Velder and Verres, 2014). Future studies should investigate how different kinds of psychotherapy mediate treatment effects.
Overall, enhanced efficacy may result from the additional psychotherapeutic integration of cognitive and transpersonal elements of psychedelic experiences. DMT potentially augments psychotherapy by increasing psychological flexibility, facilitating profound emotional breakthroughs (Roseman et al., 2019), and promoting deeper psychological insights (Peill et al., 2022). Induced mystical experiences, which correlate with improved psychological health markers, may partner with psychotherapy to facilitate substantial shifts in substance use through altered meaning-making and identity transformation that is less readily attained in conventional treatments (Ferreira and Reis-Pina, 2025; Kangaslampi, 2023). Psychotherapeutic benefits and their cognitive-behavioral effects might outweigh the neurobiological changes promoted by DMT in treating alcohol addiction, which involves multiple neurotransmitter systems, compared to the more targeted pharmacodynamic activity implicated in drug addiction.
Clinical and community populations
This review explores additional potentially mediating and confounding factors to identify other plausible explanations for outcome differences observed with the addition or omission of psychotherapy. Subgroup analyses comparing clinical and community samples revealed that population type produced statistically significant differences in effect sizes exclusively for alcohol use outcomes. Although alcohol use outcomes demonstrated lower effect sizes than drug use outcomes overall, clinical populations exhibited significantly larger effect sizes for alcohol misuse reduction compared to community populations, where their pooled effect size (g = 0.29) was radically lower than overall effect sizes across all substances (g = 0.94).
While differential response patterns between alcohol and drug use may reflect distinct mechanisms of action underlying DMT and psychotherapy interventions, substantial heterogeneity exists in substance-specific treatment effects. This heterogeneity is exemplified by persistent cannabis use documented in community populations (Fábregas et al., 2010; Thomas et al., 2013), and the attenuated DMT effects on alcohol use within these communities may reflect similar patterns not due to mechanisms alone. Observed differences likely reflect floor effects among DMT responders, wherein clinical sample participants presented with greater baseline substance use severity, thereby establishing lower thresholds for measurable improvement and yielding more pronounced treatment-related changes (Andrade, 2021). Conversely, community samples reporting substance misuse without formal SUD diagnoses may present with less severe baseline substance use patterns, positioning them closer to functional ceiling levels on primary outcome measures. This proximity to optimal functioning may constrain the magnitude of measurable improvement despite potential therapeutic benefit from DMT intervention. These measurement limitations may be further compounded by reduced reliability of ASI and other scales in subclinical populations, potentially underestimating or obscuring genuine treatment effects across different participant groups (Conway et al., 2010).
Treatment duration
It’s interesting to note that multi-session treatment over weeks or months did not appear to present any advantages over short-term single-session DMT therapy for substance misuse, as no significant subgroup effects were found for treatment duration. The statistical insignificance of outcome differences related to short-term (single-session) or long-term (multi-session) treatment durations may be explained by the fact that we were unable to reliably isolate this subgroup analysis by substance type. While the single short-term study with lower effects addressing drug use serves as an indication that longer-term treatment over multiple sessions might boost reductions in drug use, causal inferences cannot be made based on this mode of analysis. Although this meta-analysis cannot conclude that treatment duration mediates outcomes, other research finds that the number of DMT doses significantly moderates treatment effects for anxiety and depression (Leger and Unterwald, 2021). This has also been found to be true for other indirect outcomes when treating substance abuse with psilocybin or LSD, with multiple doses moderating the intensity of the acute psychedelic experience and provoked insight (Garcia-Romeu and Richards, 2018; Garcia-Romeu et al., 2019).
Psychedelic drug formulation
Omitting Armstrong et al. (2023) study from the meta-analysis suggests that this study, which used inhalant 5-MeO-DMT (rather than ayahuasca), does slightly augment the overall effect size, potentially due to the stronger potency of 5-MeO-DMT. However, this deviation from the overall pooled effect size was not substantially different from when other studies were also excluded one at a time. The two drug formulations cannot, therefore, be determined to influence substance use reduction outcomes significantly.
Study design implications
While gender-based differences in substance misuse prevalence (Substance Abuse and Mental Health Services Administration, 2018), instrument reliability (De Oliveira et al., 2014), and treatment response (Becker et al., 2016) may justify single-gender studies, the imbalanced demographic composition of the included studies and of the total pooled population limits generalizability. Primarily male participation is particularly problematic given that women are likely as vulnerable to misuse and may be more susceptible to the addiction cycle of abuse (Zakiniaeiz and Potenza, 2018). Inconsistency in including comorbid diagnoses introduces significant study heterogeneity, which complicates the interpretation of treatment effects and potentially obscures condition-specific treatment responses. A high participant attrition rate across all studies increases the risk of attrition bias and inflated treatment effect estimates.
Intervention design differences—particularly regarding psychedelic compounds, formulation, dosing, and psychological support—limit this review’s capacity to isolate specific therapeutic mechanisms and best practices. For example, the pharmacological heterogeneity presented using both DMT and 5-MeO-DMT analog variants, in both oral and inhaled formulations, as part of a monotherapy or poly-drug therapy regimen, represents several confounding variables. Although both substances are tryptamine-class psychedelics, they exhibit notable differences in their pharmacology, subjective effects, routes of administration, and contextual practices, limiting the extent to which we can interpret the outcome of their combined effect (Reckweg et al., 2022). Notably, our only study involving 5-MeO-DMT (Armstrong et al., 2023) administered it in combination with ibogaine. As a result, the independent contribution of 5-MeO-DMT cannot be isolated, and no generalizable claims can be supported based on the current evidence. Our exploratory leave-one-out analysis by drug formulation rendered it impossible to disentangle formulation effects from co-administration effects. Thus, these findings should be interpreted with caution until standardized designs for both DMT and 5-MeO-DMT are conducted to establish clearer comparative effects.
In addition to interventional heterogeneity posed by the introduction of psychotherapy, non-standardized therapist training and often unclear supervision protocols introduce potential therapist effects that may similarly confound treatment outcomes synthesized in this study. The lack of standardization extends to varied settings, ranging from traditional shamanic ceremonies to clinical environments. These widely varied treatment paradigm elements likely influence outcomes and remain insufficiently controlled or measured, making it impossible to isolate therapeutic mechanisms.
Treatment duration and dosing schedule variations likely capture different phases of therapeutic response, as psychedelic interventions typically exhibit both acute and sustained effect patterns (Nikolic et al., 2024; Preller et al., 2020). This temporal heterogeneity could theoretically illuminate dose–response relationships in well-designed trials; however, it instead introduces confounding variance within the meta-analytic framework.
While the substance use severity scales employed are valid and reliable overall, methodological limitations do exist (Reinert and Allen, 2002; Selin, 2003; WHO ASSIST Working Group, 2002). Variable gender-based reliability and ASI’s questionable capacity to differentiate between substance types (Humeniuk et al., 2008; Mäkelä, 2004; McLellan et al., 1985; Simon et al., 2023) potentially compromise measurement consistency across mixed-gender samples and substance categories in this review. Pride, shame, or other self-image concepts may introduce detection bias through self-reported measures. Temporal disparities between instruments (e.g., AUDIT’s 12-month timeframe versus more recent history surveys) may differentially affect the detection of treatment response, particularly for brief treatments. While timeframe-appropriate instrument selection mitigates this issue, Armstrong et al.’s (2023) application of AUDIT for a 3-day intervention represents a temporal mismatch, yielding underestimated treatment efficacy.
Study quality implications
Most studies’ lack of controlled conditions undermines causal inferences, and neglect of ITT analytic methods introduces systematic bias through the exclusion of dropped participants, which might represent treatment non-response. Inadequate sample representativeness limits external validity and likely reflects self-selection with positive treatment expectations rather than the general substance-using population. Consequently, effect estimates are most applicable to self-selected, treatment-seeking populations with positive expectations toward psychedelic interventions rather than the broader substance-using population. Observed changes lacking control conditions demonstrate low internal validity and are inadequate to support causal inferences attributed directly and entirely to interventions, leaving open questions of effects due to participant expectations, healing trends without treatment, or the influence of a supportive environment. Taken together, these limitations correspond to a low certainty of evidence as estimates are highly sensitive to bias, as informed by the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) framework (Goldkuhle et al., 2025). As such, the synthesized effects should be understood as preliminary indicators of possible rather than certain treatment efficacy.
It should be noted that the Rodrigues et al. (2024) study’s inability to detect subtle effects may have been due to its underpowered design. While this may skew the pooled results toward diminished outcomes, the sample size adequacy for 80% powered results or greater among all other studies largely overpowers this influence, increasing the credibility of meta-analysis findings.
Finally, we imputed missing data from Thomas et al. (2013) with standard deviation values from Rodrigues et al. (2024), acknowledging that the study was underpowered and only reported on alcohol outcomes. Although these substitutions followed established approaches for handling missing data, the method introduces assumptions that the variability in outcomes is comparable to what could have been observed in the Thomas et al. (2013) study and thus may bias the resulting effect estimates. Notably, exploratory subgroup analyses were similar when the imputed Thomas et al. (2013) data were excluded, indicating minimal impact of these imputation methods on overall results. However, these results involving imputed standard deviations should be interpreted with caution.
Study evaluation
This rigorous systematic synthesis of DMT intervention studies yielded reliable effect size estimates through high-powered data pooling. Predetermined screening criteria ensured objectivity, and a comprehensive search methodology promoted unbiased reporting and reproducible analysis. The number of studies was adequate for meta-analysis, but including more homogeneous RCTs would yield more reliable conclusions. All studies used similar, validated measures, contributing to homogeneity, but self-reports reduced measure reliability. Some study characteristics varied, limiting the validity and certainty of the findings. Although we critically evaluated their influence—for example, through our exploratory leave-one-out analysis of different drug formulations—it remained impossible to disentangle the effects of formulation from the co-administration of 5-MeO-DMT and DMT. Marked heterogeneity in DMT-assisted psychotherapy outcomes compromised the generalizability of psychotherapy’s associated findings, representing average rather than predictable treatment outcomes. Differences in setting (traditional shamanic vs clinical) also complicated interpretations of therapeutic mechanisms due to the environmental variables. This investigation’s limited scope excluded valuable subgroup analyses by formulation, dosing, treatment duration, and setting, which could evaluate each characteristic’s influence on outcomes. While effect sizes appeared substantial, the exclusion of control groups limited causal attribution, so natural recovery, regression to the mean, or placebo effects might also contribute to outcomes. Pervasive high risk of bias due to methods likewise undermines confidence in effect size estimates and psychotherapy’s moderating effects, necessitating caution in interpreting efficacy claims. The absence of extended follow-up data suggests that observed effects could represent transient responses and does not inform treatment durability. These early estimates should inform future hypotheses rather than confirm treatment efficacy and require controlled research validation rather than representing actionable clinical evidence.
Future research
Future research should address these limitations through RCT designs and follow-up meta-analyses, excluding studies with high risk of bias. Other meaningful outcomes, like relapse rates, should be measured while comparing treatment to active control groups and eliminating confounding factors. Comparing a manualized or semi-standardized psychotherapy approach will ideally isolate pharmacological from psychotherapeutic effects. Various therapeutic frameworks (CBT, DBT, ACT, psychodynamic) should also be evaluated with DMT to identify the most advantageous approach to reducing substance misuse, with findings evaluated across other psychedelic therapies. Mixed-methods studies can identify productive elements of psychedelic and complementary psychotherapy, and longitudinal studies should measure long-term outcomes. To differentiate pharmacological effects from contextual influences, studies should measure specific contributions of DMT formulations, dosing regimens, environments, and set/setting elements. Comparative analysis of traditional ceremonial versus clinical settings could determine how ritual elements influence outcomes, with beneficial components integrated into treatment paradigms. Differential outcomes between alcohol, drugs, and cannabis warrant substance-specific research into DMT interactions with neurobiological phenomena, exploring varied dosing regimens to optimize treatment by substance type. Neuroimaging studies may specifically illustrate neural correlates of SUD recovery mechanisms and inform new lines of inquiry. Finally, research might address common neuropsychiatric comorbidities with enhanced vigilance and rescue protocols for adverse events, particularly with psychosis risk. Overall, there is a substantial opportunity to progress our knowledge of how DMT-assisted therapy rehabilitates substance abuse.
Clinical implications
Identified ethical deficiencies—inadequate informed consent, insufficient safety monitoring, and unclear boundary protocols—rendered findings ethically problematic for clinical translation. Psychedelic-specific ethical standards must be refined to reduce human subject risk and increase the credibility of future studies for direct translation to safe clinical guidelines. Safety monitoring protocols, enhanced informed consent, and contingency plans would reduce risks while enabling research with more diverse clinical populations that include medical comorbidities. With such safety measures in place, extended studies can determine optimal dosing schedules for sustained benefits. Evidence-based best practices emerging from safe, ethical research should inform policy recommendations and therapist training requirements, providing a strong foundation for responsible clinical implementation.
Establishing long-term efficacy and safety profiles remains paramount for clinical adoption. Addiction treatment efficacy is defined by sustained abstinence over months to years, not acute improvements. The absence of extended follow-up data, therefore, undermines the current findings’ clinical relevance. Furthermore, the lack of long-term safety monitoring means delayed adverse effects remain unknown, creating ethical constraints on clinical use.
The observed efficacy gap between alcohol and drug use challenged DMT’s perceived status as a universal SUD intervention. Without mechanistic clarification, clinicians cannot reliably predict treatment responses for specific substances of abuse. This reduces DMT’s immediate clinical utility and would require that treatment decisions be based on incomplete understanding, risking wasteful rounds of ineffectual treatment.
Standardization is crucial for the translation of psychedelic research into pragmatic clinical practice. Heterogeneity in DMT-assisted psychotherapy means that clinicians attempting to replicate findings without standardized protocols faced some degree of outcome uncertainty. Guidelines and procedures should be substance-specific, considering alternatives for cannabis dependence, which demonstrated lesser DMT response. Given superior efficacy for alcohol and other abused drugs, standard DMT or 5-Meo-DMT protocols may someday complement treatments, especially for treatment-resistant populations. If durable effects are confirmed, optimized DMT formulations with brief, targeted integrative psychotherapy may prove more cost-effective than ongoing pharmacotherapy and long-term psychotherapy.
Conclusion
This study provides preliminary evidence that DMT/5-MeO-DMT interventions may yield large effects for substance use reduction, especially when combined with psychotherapy. While the emerging literature suggests potentially meaningful effects, the overall certainty of evidence is low due to high risk of bias and heterogeneous methodologies. Accordingly, the present findings should be viewed as informing future trial design and refining hypotheses. Considering addiction’s substantial global burden, findings suggest DMT-based interventions could offer promising alternatives for individuals responding inadequately to existing treatments. Further investigation is warranted to confirm DMT efficacy and psychotherapy’s adjunctive role. Advances in safe, effective, ethical DMT therapy could meaningfully reduce personal suffering and societal costs associated with substance abuse while expanding treatment options.
Supplemental Material
sj-docx-1-jop-10.1177_02698811261430518 – Supplemental material for Efficacy of N, N-dimethyltryptamine (DMT) psychedelic therapy for substance misuse: A systematic review and meta-analysis
Supplemental material, sj-docx-1-jop-10.1177_02698811261430518 for Efficacy of N, N-dimethyltryptamine (DMT) psychedelic therapy for substance misuse: A systematic review and meta-analysis by Lisa M. Wallace, Andrea Bujor, Gustavo Sudre, Mark Kennedy, Diana-Elena Bahnareanu and Khushi Mittal in Journal of Psychopharmacology
Supplemental Material
sj-docx-2-jop-10.1177_02698811261430518 – Supplemental material for Efficacy of N, N-dimethyltryptamine (DMT) psychedelic therapy for substance misuse: A systematic review and meta-analysis
Supplemental material, sj-docx-2-jop-10.1177_02698811261430518 for Efficacy of N, N-dimethyltryptamine (DMT) psychedelic therapy for substance misuse: A systematic review and meta-analysis by Lisa M. Wallace, Andrea Bujor, Gustavo Sudre, Mark Kennedy, Diana-Elena Bahnareanu and Khushi Mittal in Journal of Psychopharmacology
Footnotes
Acknowledgements
We would like to express our sincere gratitude to Prof. Maria Gudbrandsen for her constructive feedback and guidance throughout the development of this review. We are also thankful to Dr. Kulbir Birak for his consistent mentorship and support, and to Doctoral Candidate Shalini Bhattacharya for her valuable input on analytical strategy and interpretation.
ORCID iDs
Author contributions
All authors have contributed significantly to the development of this manuscript. Lisa M. Wallace led the conceptualization, methodology, investigation, systematic database searches, study screening, data extraction, analysis, interpretation of findings, supervision, and preparation of the original draft, along with revisions. Khushi Mittal contributed to conceptualization, investigation, formal analysis, validation, and writing during the review and editing phases. . Andrea Bujor contributed to the methodology, investigation, study screening, analysis, manuscript drafting and revisions. Diana-Elena Bahnareanu contributed to investigation, study screening, and manuscript drafting. Gustavo Sudre was instrumental in guiding the statistical methodology and data analysis and contributed substantially to supervision and manuscript revisions. He is supported by the Rosetrees Trust and the Pears Foundation through the Rosetrees Pears Chair of Bioinformatics. Mark Kennedy provided overarching conceptual guidance, supervision, and editorial review. All authors have read and approved the final version of the manuscript.
Funding
Gustavo Sudre is supported by the Rosetrees Trust and the Pears Foundation through the Rosetrees Pears Chair of Bioinformatics. However, these funds are not attributed to this project. Other authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
These data and meta-data are available upon request.
Systematic review registration
Supplemental material
Supplemental material for this article is available online.