
Abstract
Background:
The empathogen and psychostimulant 3,4-methylenedioxymethamphetamine (MDMA) is thought to boost both subjective well-being and social connection. Although MDMA is considered to enhance social connection to a greater extent than other stimulant drugs, few studies have compared MDMA to other stimulants. In addition, previous studies have focused on social positivity effects (e.g., increased trust) for specific in-lab interaction partners without considering more generalized social positivity effects (e.g., trust in one’s community).
Aims:
We tested the effects of MDMA on subjective ratings of well-being and global social connection, including feelings of trust toward one’s community and society. The effects of MDMA were compared to a prototypic stimulant, methamphetamine (MA).
Methods:
Across two studies, we examined differences in subjective well-being and global social well-being 90 minutes after a conversation on MDMA (study 1; N = 15; 100 mg) and after a conversation on MA (study 2; N = 20; 20 mg) compared to a placebo.
Results:
After MDMA, participants reported significantly higher global trust, t(14) = −2.583, p = 0.022, and marginally higher self-worth, t(14) = −2.000, p = 0.065, compared with after the placebo. Furthermore, MA did not alter scores of subjective well-being and social connection.
Conclusions:
Our findings extend previous research by demonstrating that MDMA increases feelings of trust in the social world beyond lab-specific interaction partners. These findings are consistent with user reports of generalized social well-being effects and support the idea that MDMA may have clinical value from a social psychological perspective.
Introduction
Psychedelic social psychology presents a new frontier of psychological inquiry. Psychedelic substances, or substances that markedly alter perception, mood, and consciousness (including hallucinogenic experiences), offer a unique opportunity to study ways to improve social connection and, consequently, subjective well-being (Carhart-Harris and Goodwin, 2017). Specifically, 3,4-methylenedioxymethamphetamine (MDMA; colloquially called “ecstasy”) is one psychoactive substance that has been forwarded as a strong candidate for use in building social connection through social psychological interventions (Lyubomirsky, 2022). Although MDMA also has receptor actions and behavioral effects that resemble those of psychedelics (Pentney, 2001), MDMA is chemically most similar to stimulant drugs. Accordingly, researchers have used the descriptors “empathogen” and “entactogen” (as opposed to “psychedelic”) to highlight MDMA’s distinctive effects on self-insight and social connection. In support of MDMA’s role in enhancing social connection, meta-analytic evidence reveals that MDMA has a moderately large effect on feelings of sociability (e.g., feeling loving and friendly; d = 0.86; Regan et al., 2021).
Notably, research establishing the effects of MDMA on social connection primarily tests acute social effects during experimental tasks (Bershad et al., 2019; Kirkpatrick and de Wit, 2015; Molla et al., 2023). However, theoretical perspectives suggest that the positive emotional and social experiences induced by MDMA may produce shifts in perspective that can carry forward to other social relationships and promote a global sense of connectedness (Lyubomirsky, 2022). Accordingly, further work is needed to determine whether MDMA’s social effects generalize to broader interpersonal relationships—especially if MDMA is to be considered a tool for boosting subjective and social well-being in the long term.
Importantly, much of the existing evidence on the generalizability of MDMA’s social effects remains anecdotal. While such accounts have fueled public interest through popular media coverage (e.g., ABC News, as reviewed by Lyubomirsky, 2022), rigorous empirical research is critically needed to test whether MDMA-induced social positivity extends beyond the immediate interaction partner(s) and beyond the context of the MDMA-facilitated social experience. Establishing the broader impact of MDMA on social positivity—spanning interpersonal relationships, social groups, and society at large—could provide a foundation from which to test its potential role in alleviating more enduring social challenges, such as loneliness and social anxiety.
MDMA may be uniquely suited to bolster social well-being, as it purportedly enhances social well-being to a greater extent than other psychoactive substances (for a review, see Bershad et al., 2016). However, little research to date has compared the social effects of MDMA to other psychoactive substances, and the research that does exist provides mixed results. A handful of studies speak to the unique social benefits of MDMA. For instance, in one study, MDMA, but not methylphenidate (a common treatment for attention-deficit/hyperactivity disorder), enhanced liking, closeness, openness, and trust in a facial recognition task (Schmid et al., 2014). In line with other research indicating that MDMA’s prosocial effects are mediated by the release of oxytocin (a hormone that enhances social bonding), MDMA increased oxytocin levels in this experiment, but methylphenidate did not (Schmid et al., 2014). In addition, another study reported that MDMA, but not methamphetamine (MA), increased attentional bias to positive social stimuli (images of faces with positive expressions) and self-related pleasantness of physical touch (soft brushing on the forearm; Bershad et al., 2019).
Other studies, however, have reported mixed findings vis-à-vis the social benefits of MDMA or revealed other psychoactive substances to confer comparable social benefits. For example, one study found that MDMA significantly increased self-reported feelings of closeness to others, but did not significantly increase trust, empathy, and cooperation in computer-based behavioral tasks (Borissova et al., 2020). Another recent study (Molla et al., 2023) examined the effects of MDMA and MA in dyadic conversations between participants and found that both MDMA and MA increased feelings of social connection and oxytocin levels, but that oxytocin levels were only significantly correlated with increased self-ratings of social connection after MDMA and not MA. These results support the idea that MDMA’s positive effects on social outcomes are partially mediated by oxytocin (e.g., Schmid et al., 2014), but also raise questions about the pharmacological specificity of the social effect of MDMA.
The present research
In the present research, we adopt a social psychological perspective when interpreting the prospective social and well-being benefits of MDMA. To this end, we aim to address the following question: Do either MDMA or MA increase subjective well-being and global social well-being (i.e., greater social positivity toward broad interpersonal relationships) following a lab-based conversation task? The current research elaborates on previously published findings focused on positive social effects (e.g., feeling trusting, connected, and friendly) toward one’s conversation partner measured during and immediately after these social interactions (Molla et al., 2023). Specifically, the current paper presents pre-registered analyses (https://aspredicted.org/h2xs-wr62.pdf; see hypotheses and analyses related to “thriving”) examining broad aspects of subjective well-being (e.g., sense of self-worth, meaning, and life satisfaction), as well as more global social well-being outcomes (e.g., feelings of trust and belonging among others, the community, and society).
To address these questions, we conducted two studies, each using a two-session within-subjects design examining the effects of a drug on subjective well-being and global social well-being 1.5 hours following a 45-minute conversation. Study 1 compared MDMA (100 mg) with placebo, and Study 2 compared MA (20 mg) with placebo. Specifically, ratings on the following 9 subscales (of 18 total subscales) from the Comprehensive Inventory of Thriving (CIT; Su et al., 2014) were compared after conversations on drug and placebo (Study 1: MDMA; Study 2: MA): support, trust, respect, belonging, engagement, self-worth, meaning, optimism, and life satisfaction. The CIT was administered at orientation and 1.5 hours after each conversation session. We hypothesized the following:
Participants will report higher subjective and global social well-being (as indexed by support, trust, respect, belonging, engagement, self-worth, meaning, optimism, and life satisfaction) after a conversation under the influence of MDMA, compared with placebo.
Participants will report higher subjective and global social well-being (as indexed by support, trust, respect, belonging, engagement, self-worth, meaning, optimism, and life satisfaction) after a conversation under the influence of MA, compared with placebo.
Materials and methods
Study design
Participants in both studies completed three laboratory visits and a follow-up. They attended an orientation session to explain the study (T1), two in-lab conversation sessions separated by at least 4 days (T2 and T3), and a 1-week online follow-up (T4). They received a drug or a placebo in the two in-lab sessions (T2 and T3) under double-blind conditions. After the drug reached its peak effect, participants engaged in a 45-minute conversation (Aron et al., 1997) with a same-sex confederate who was not under the influence of a substance. Survey measures on subjective well-being and social connection, indicated by nine subscales on the CIT, were obtained at orientation and immediately after each study session.
Participants
Participants were recruited through posters and internet advertisements on social media. Healthy male and female volunteers aged 18–35 years were eligible for participation. Extensive screening procedures included a physical exam, psychiatric interview, medical history review, electrocardiogram, and assessment of drug use history. Exclusion criteria included having a medical condition requiring regularly prescribed medication; a current diagnosis of substance dependence, mood, anxiety, or psychotic disorders (per the DSM-5); a history of treatment for alcohol or drug use; abnormal electrocardiogram readings; high blood pressure; or current pregnancy. Participants also completed the Symptom Check List-90-Revised (Derogatis and Savitz, 1999). Additional screening ensured self-reported fluency in English, a body mass index (BMI) between 19 and 30 (considered normal BMI), high school completion, and the consumption of fewer than four alcoholic or caffeinated beverages daily. In Study 1, participants needed to have consumed MDMA between 1 and 40 times with no adverse effects (e.g., very high blood pressure or “bad trips”) to ensure participant safety and familiarity with the substance, but no habitual use. Participants provided written informed consent prior to the beginning of each study. The consent form was approved by the Institutional Review Board of the Biological Sciences Division at the University of Chicago. Methods were performed in accordance with the Declaration of Helsinki.
Drugs
Participants in Study 1 received 100 mg of MDMA in powdered form (Organix Inc., Woburn, MA, USA), placed in opaque size 00 capsules with lactose filler. Participants in Study 2 received 20 mg of MA (Desoxyn; Lundbeck Inc., Deerfield, IL, USA) in an opaque size 00 capsule with dextrose filler. Placebo capsules contained only lactose or dextrose. The doses were selected based on prior research that produced reliable subjective effects without adverse side effects (Hysek et al., 2014; Mayo et al., 2013; Wardle and de Wit, 2014).
Subjective and social well-being
Subjective well-being and social well-being outcomes were assessed using the CIT, which consists of 18 subscales related to various aspects of psychological well-being. For the current project, we selected and administered nine subscales thought most relevant to social and subjective well-being: support (e.g., “There are people I can depend on to help me”), trust (e.g., “I can trust people in my society”), respect (e.g., “I am treated with the same amount of respect as others”), belonging (e.g., “I feel a sense of belonging in my community”), engagement (e.g., “I get fully absorbed in the activities I do”), self-worth (e.g., “What I do in life is valuable and worthwhile”), meaning (e.g., “My life has a clear sense of purpose”), optimism (e.g., “I have a positive outlook on life”), and life satisfaction (e.g., “In most ways my life is close to ideal”). Each subscale comprised three items, with scores ranging from 1 (“Strongly disagree”) to 5 (“Strongly agree”). A mean value was computed for each subscale for each participant, and these mean values were used in subsequent analyses. Cronbach’s alpha coefficients, as indicators of internal consistency reliability, are provided for each subscale at each time point (orientation, session 1, session 2) in Table 1.
Cronbach’s alpha coefficients (internal consistency reliability).
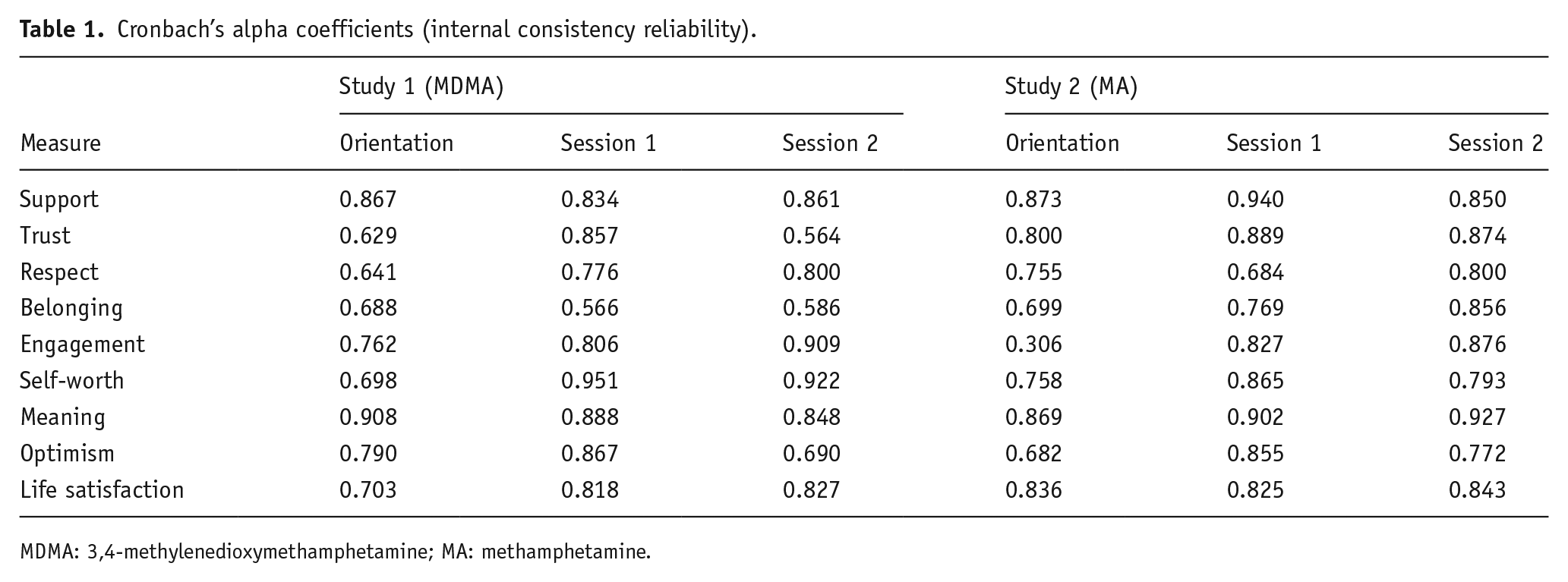
MDMA: 3,4-methylenedioxymethamphetamine; MA: methamphetamine.
Procedure
Orientation
During the orientation session, participants completed personality and baseline questionnaires (including the CIT), were instructed on procedures, and provided informed consent. To reduce expectancy effects, participants were told they might receive a stimulant, a sedative, a placebo, or a hallucinogenic drug. Participants were instructed to fast for at least 8 hours before each session, abstain from use of any drug for at least 2 days before each session (except for cannabis, which required a 7-day abstinence period), and abstain from alcohol for 24 hours before each session. To ensure compliance, participants were informed that drug and alcohol testing would occur at each study session and that noncompliance would disqualify them from completing the study.
Study sessions
The two sessions lasting 4.5 hours were scheduled from 9 a.m. to 1:30 p.m., separated by a minimum of 4 days (for study 1) or 3 days (for Study 2). Each session began with testing adherence to drug and alcohol abstinence via urinalysis (CLIAwaived Instant Drug Test Cup) and a breathalyzer (Alco-Sensor III; Intoximeters, St. Louis, MO, USA), respectively, as well as pregnancy testing for women. At 9:30 a.m., participants ingested a capsule of either a drug (Study 1: MDMA; Study 2: MA) or a placebo. Participants then relaxed in a room for 1 hour to allow for drug absorption. At 10:40 a.m., they were led to a separate room in which they engaged in a 45-minute conversation with a same-sex stranger (confederate). Confederates were trained in the conversational procedure (Aron et al., 1997) but were unaware of which drug was administered to participants. At 1:30 p.m., after the conversation’s conclusion, participants completed measures relating to their conversational experience and the CIT. For procedures and measures not reported in this paper, see Molla et al. (2023).
Conversation task during study sessions
For the structured small-talk conversation (Aron et al., 1997), a different set of eight questions was provided every 15 minutes for the dyad to use as prompts (e.g., “What is your favorite holiday? Why?”). Different questions were presented for the two separate study sessions to minimize order effects. Participants could choose to skip any questions they did not wish to discuss. The conversations were audiotaped (data not reported here).
Analytic strategy
Our analyses involved two sets of two-tailed dependent means t-tests at the 0.05 alpha level (p < 0.05). First, we tested significant mean differences in subjective well-being and social connection outcomes between post-drug and post-placebo session ratings. That is, we compared within-subject post-drug scores on MDMA with post-placebo scores for Study 1, and compared within-subject post-drug scores on MA with post-placebo scores for Study 2. Our second set of t-test analyses involved testing significant differences in gain scores from orientation to post-placebo session and from orientation to post-drug session (MDMA for Study 1; MA for Study 2).
As specified in our pre-registration, we also intended to assess growth trajectories with multilevel models or residualized change models. However, given the limited sample size (Maas and Hox, 2005) and our counter-balanced design of drug administration, multilevel models could not be estimated. Specifically, the counter-balanced design of our study entailed that a variable representing time could not be modeled, as some participants received a placebo for their first conversation session, and some received a drug. Accordingly, this also means that the time difference between the orientation session and the post-drug session for some participants was about 1 week, and for other participants (those who received the placebo for their first session), the time difference was about 1.5–2 weeks. Thus, the time difference between orientation and the post-drug session is a confound that is not represented in our dependent means t-tests, but could be addressed in future studies without a counter-balanced design. Despite the limitation counter-balancing places on testing change over time, we opted to use counter-balancing in the present studies to minimize participant expectancies about drug effects at each study session.
Exclusions
Two participants from Study 1 were excluded from analyses. One participant was excluded because both confederates rated them very negatively and felt the participant did not adhere to the intended structure of the conversation. The second participant was excluded for socializing with one of the conversation partners outside of the study sessions (before the follow-up), raising concerns about potential confounding factors such as a heightened sense of closeness to their study partner. No participants from Study 2 were excluded.
Results
Demographics
Participants in Study 1 had a mean age of 26.7 years (range: 20–31 years ), with 53% identifying as male and 87% having graduated from college or completed master’s level education. Participants in Study 2 had a mean age of 22.8 years (range: 19–30 years old), with 45% identifying as male and 45% having graduated from college or completed a master’s. In addition, the majority reported low-to-moderate drug use, with participants in Study 1 reporting higher lifetime drug use compared with participants in Study 2 (see Supplemental Table S1).
Comprehensive inventory of thriving
Study 1: MDMA versus placebo
According to a dependent means t-test, participants reported significantly higher trust immediately after the MDMA session relative to after the placebo session, t(14) = −2.583, p = 0.022. Furthermore, we observed a significant increase in trust ratings from orientation to post-MDMA conversation compared with from orientation to post-placebo conversation, t(14) = −2.582, p = 0.022. That is, trust, on average, increased from before to after the MDMA session (Mpost-MDMA = +0.18, standard deviation (SD) = 0.45), but decreased from before to after the placebo session (Mpost-placebo = −0.07, SD = 0.41).
Self-worth scores were marginally higher after MDMA compared with placebo, t(14) = −2.000, p = 0.065. We also observed a marginally significant difference between gain scores from orientation to post-MDMA conversation and orientation to post-placebo conversation, t(14) = −2.00, p = 0.065, such that participants reported gains in self-worth, on average, from orientation to the post-MDMA session (Mpost-MDMA = +0.20, SD = 0.57), but they reported slight declines in self-worth, on average, from orientation to the post-placebo session (Mpost-placebo = −0.02, SD = 0.54).
When comparing post-MDMA conversation scores and post-placebo conversation scores, as well as gain scores from orientation to post-MDMA conversation and from orientation to post-placebo conversation, no significant differences emerged for life satisfaction, optimism, meaning, belonging, support, or engagement. See Table 2 for means and standard deviations.
Study 1 subjective and social well-being gain scores.
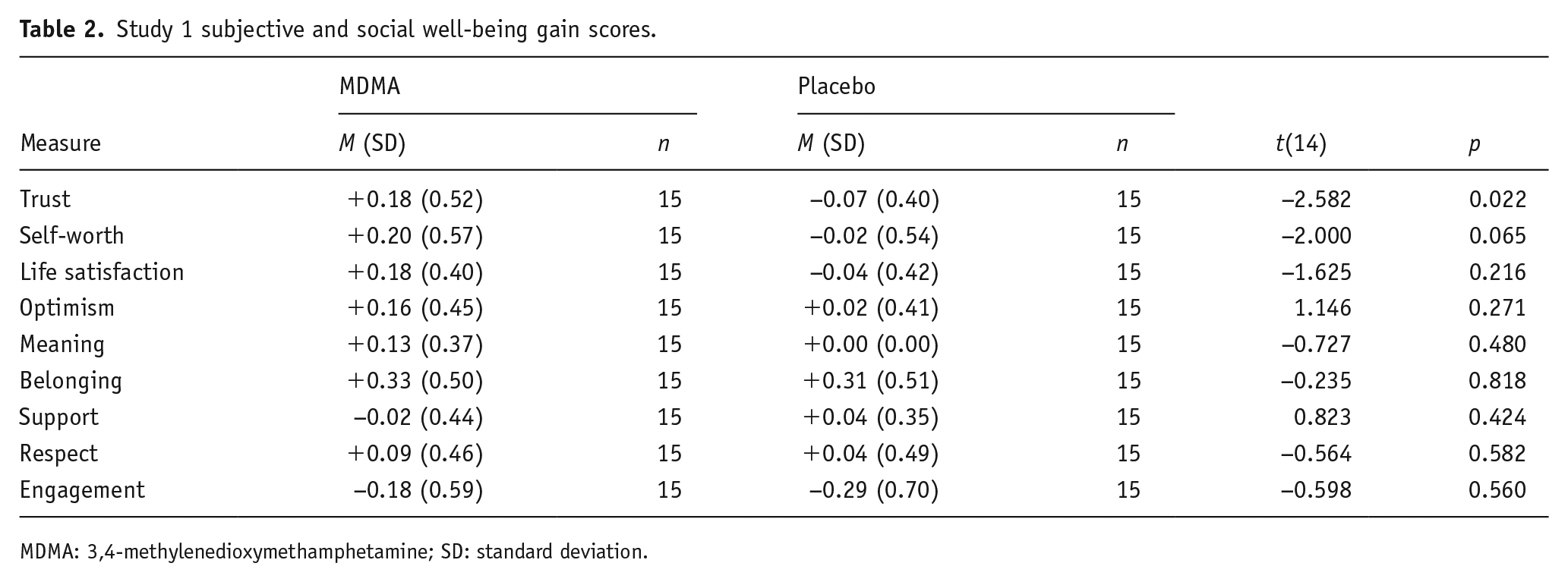
MDMA: 3,4-methylenedioxymethamphetamine; SD: standard deviation.
Study 2: MA versus placebo
Participants did not report higher subjective or social well-being post-MA conversation relative to post-placebo conversation, nor did they report significant increases in these measures from orientation to post-MA conversation. These measures included trust, worth, life satisfaction, optimism, meaning, belonging, support, respect, and engagement. See Table 3 for means and standard deviations.
Study 2 subjective and social well-being gain scores.
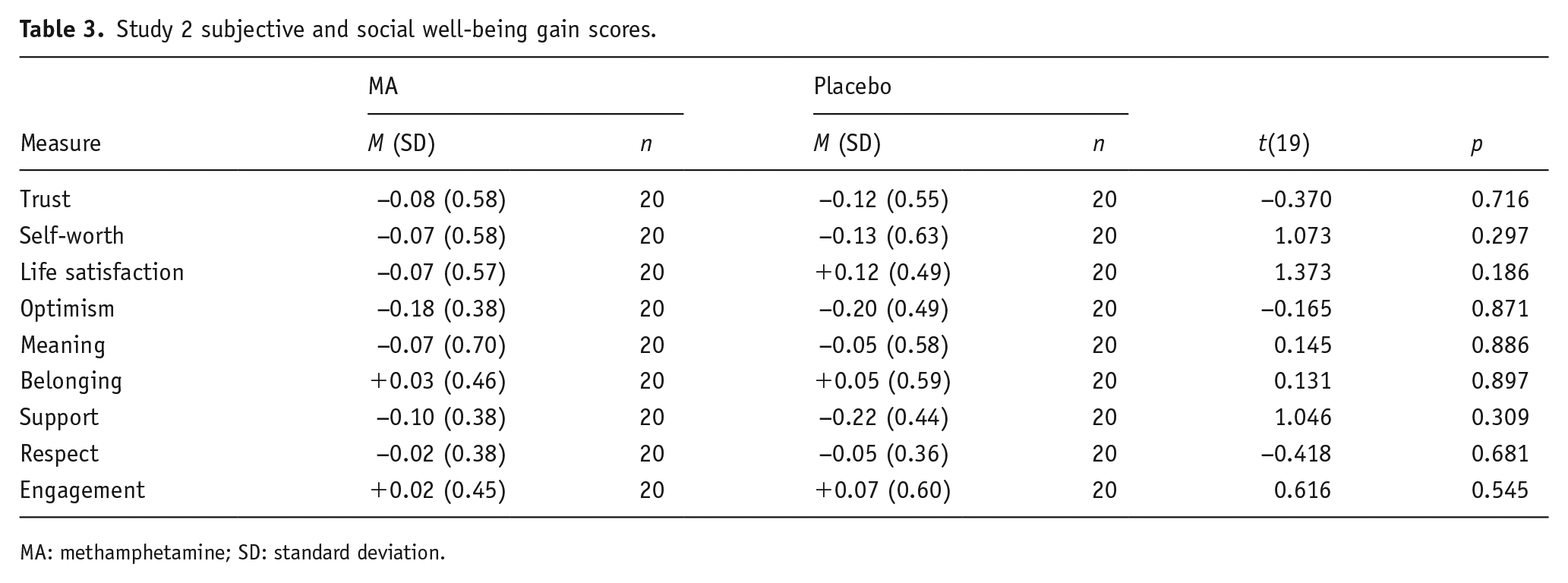
MA: methamphetamine; SD: standard deviation.
Discussion
MDMA, but not MA, significantly increased feelings of global trust after a conversation with a stranger, and marginally increased feelings of self-worth (or feeling valuable and worthwhile). These results extend our knowledge of the social effects of MDMA and support previous research indicating that MDMA increases trust (Bershad et al., 2016; Schmid et al., 2014; Stewart et al., 2014). Our results are also consistent with previous reports that MDMA reduces neural responses to social threat (angry faces; Bedi et al., 2009), decreases concerns about negative evaluations from others in instances of personal disclosure (Baggott et al., 2016), and enhances the patient–therapist alliance via increased trust in the context of psychotherapy (Heifets and Malenka, 2016). Taken together, the present findings suggest that MDMA may be especially helpful for building a sense of social safety.
On a more novel basis, our findings elaborate on the more well-documented acute effects of MDMA on trust and social positivity toward one’s immediate social interaction partner, including results from the present study published elsewhere (Molla et al., 2023). More precisely, Molla et al. (2023) reported on data from the current studies focused on connection and enjoyment during each conversation with complementary physiological data on oxytocin (a socially bonding hormone). The researchers found that both MDMA and MA significantly increased conversational enjoyment and sense of connection to their conversation partners. MDMA and MA also increased feelings of feeling stimulated, insightful, sociable, loving, friendly, and a sense of vigor relative to placebo. In addition, MDMA uniquely increased ratings of feeling trusting, appreciated, grateful, anxious, and confused, while MA uniquely increased ratings of feeling understood and decreased ratings of fatigue. Last, while both MDMA and MA increased oxytocin levels in these studies, oxytocin was only significantly correlated to feeling closer to one’s conversation partner after MDMA.
While other analyses from these studies highlight many shared positive benefits of MDMA and MA on social connection for specific interaction partners (Molla et al., 2023), the present analyses indicate only MDMA significantly increased a sense of global trust beyond one’s immediate interaction partner that extends to one’s “neighborhood,” “society,” and “most people” (per the language of the CIT) 1.5 hours after a conversation on MDMA. To a lesser extent, MDMA also uniquely improved sense of self-worth, or feeling valuable, worthwhile, and that one is important and contributes to society—feelings that are complementary to trust and a sense of social safety. The particular effects of MDMA on global trust also parallel previous findings from the current studies, indicating that oxytocin is only significantly related to perceived partner connection after MDMA, not MA (Molla et al., 2023). The unique relationship between oxytocin and perceived partner connection after MDMA implicates unique pathways driving increased social connection between MDMA- and MA-influenced interactions, and in the case of MDMA, these unique effects may more readily enable generalization of social positivity toward the broader social world. Importantly, however, additional research is needed to test these preliminary speculations about drug mechanisms. The present studies provide direct support for the idea that MDMA uniquely increases feelings of global trust compared with MA. The observed effects of MDMA on global trust in the present analyses also complement the previously published finding that only MDMA, and not MA, significantly increased trust for specific, in-lab interaction partners (Molla et al., 2023).
The fact that MDMA, but not MA, was found to be beneficial for global social well-being further highlights its intervention promise—especially in light of its better safety record compared with MA and other substances (Nutt et al., 2010). Notably, although MA appears to encourage feelings of social connection in conversation and boosts sociability in the short term (Homer et al., 2008; Molla et al., 2023), chronic MA use is associated with impaired social functioning, such as increased social isolation and aggressiveness (Homer et al., 2008). MA also ranks as the fourth most harmful drug among 20 commonly-used drugs and substances (including alcohol, heroin, cocaine, and cannabis) when considering factors such as mortality, costs to physical health, risk of dependency, and costs to relationships and family; MDMA, by contrast, ranks as the fourth least harmful (Nutt et al., 2010). Accordingly, when comparing the benefits of different substances, it is critical to weigh their short-lived benefits against the backdrop of their long-term prospects for adjustment (or maladjustment).
Importantly, our results also represent a valuable advance within the MDMA experimental literature, given our use of naturalistic social contexts (conversations with strangers) to test its social effects. The call for social and positive psychologists to consider the value of developing and testing biointerventions invites additional psychedelic research from a social psychological perspective to supplement neural and pharmacological findings (Lyubomirsky, 2022). In this spirit, we encourage future MDMA researchers to continue using ecologically valid social stimuli and social situations, as well as to leverage social psychological theory and methods when designing and interpreting psychedelic intervention research. Additional research is also needed to replicate the present findings that feelings of social positivity experienced for immediate interaction partners can extend to other social relationships. Finally, ongoing research will be essential to establish whether these feelings of generalized social positivity endure beyond 1.5 hours following an MDMA-facilitated social interaction. If such findings hold, MDMA may be one pharmacological tool to mitigate enduring negative cognitions associated with loneliness and social anxiety.
The current project had notable limitations. First, our sample sizes were small (Nstudy 1 = 15; Nstudy 2 = 20). The procedural involvement, time-intensive effort, and ethical considerations render it difficult to administer a drug-assisted subjective and social well-being intervention at scale. Yet, larger sample sizes are needed in the future to increase confidence in these effects. Second, the differential recruitment criteria across our two studies (requiring experience with prior use of MDMA, but not for MA) may have produced different expectancies regarding the drug experience and self-selected different types of participants. Future comparative psychedelic research could maintain consistent inclusion criteria for the psychoactive substances assessed. Third, our study design entailed separately comparing the relative effects of MDMA versus placebo and MA versus placebo, but it would be useful in future studies to use designs that enable direct comparisons between the effects of MDMA and MA.
Fourth, our counterbalanced design prevented us from carrying out more sophisticated regression analyses that would enable us to model growth in our outcomes over time, rendering the time between the orientation session and the first drug session a confound that cannot be accounted for in our dependent means t-tests. Although we intentionally chose to counterbalance drug and placebo sessions in the current studies in favor of minimizing participant expectancies, future studies might prioritize study designs enabling more precise estimates of change over time.
The fifth limitation also concerns studying changes to outcomes over time. Additional research could examine the duration of subjective and global social well-being effects beyond 1.5 hours following a drug-facilitated interaction. Notably, the self-reported social positivity we observed 1.5 hours after peak drug effects may still reflect residual effects of the administered drug (albeit at decreased concentrations). Future research could test the duration of improvements to global social well-being after the acute influence of MDMA diminishes—for example, using additional follow-up periods, from immediate return to baseline (e.g., 4–6 hours after drug administration) to 1 day following drug administration, and so on (de la Torre et al., 2000). The present research offers novel, foundational evidence that MDMA bolsters trust for the broader social world (beyond specific interaction partners in the lab), including one’s neighborhood, society, and “most people.” Although demonstrating the generalizability of MDMA-induced social positivity to other social actors is a key first step in assessing the potential utility of MDMA in promoting social well-being in the long term, more research is needed to establish whether and how long these effects endure beyond the acute phase, and how these benefits might be integrated in everyday life.
In conclusion, we found that MDMA, but not MA, increased feelings of trust—and to a lesser extent, self-worth—in dyadic conversations. A sense of trust and safety is foundational for experiencing and actively engaging in caring and fulfilling social interactions, from physical intimacy to doctor–patient bonds (Gilbert, 2009). More broadly, positive emotions are functionally adaptive and signal safety and permission to play and explore, including in the context of interpersonal relationships (Fredrickson, 2005). Our studies provide preliminary support that the empathogen MDMA is uniquely consequential for positive social outcomes like a sense of trust and worth—potential building blocks of further psychological and interpersonal flourishing.
Supplemental Material
sj-docx-1-jop-10.1177_02698811251370999 – Supplemental material for The empathogen 3,4-methylenedioxymethamphetamine, but not methamphetamine, increases feelings of global trust
Supplemental material, sj-docx-1-jop-10.1177_02698811251370999 for The empathogen 3,4-methylenedioxymethamphetamine, but not methamphetamine, increases feelings of global trust by Ramona L. Martinez, Nina Radošić, Hanna Molla, Harriet de Wit and Sonja Lyubomirsky in Journal of Psychopharmacology
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.