
Abstract
Background:
Alcohol use disorder (AUD) is a major public health issue, posing harmful consequences for individuals and society. Recent advances in addiction research have highlighted the therapeutic potential of ketamine-assisted therapy for AUD. However, the exact mechanisms underlying its effectiveness remain unknown.
Aims:
This double-blind, pilot study aimed to investigate esketamine combined with mindfulness-based intervention (MBI) to examine whether esketamine enhances engagement in MBI for individuals with alcohol misuse problems and whether enhanced engagement has any impact on alcohol-related outcomes.
Methods:
In all, 28 individuals with alcohol problems were randomly assigned to receive sublingual esketamine hydrochloride (AWKN002: 115.1 mg) or vitamin C (placebo) in an oral thin film and took part in 2 weeks of daily MBI. Participants were assessed on various self-report measures, including mindfulness, engagement in MBI (physical and psychological), alcohol cravings and consumption.
Results:
Esketamine enhanced psychological engagement with a daily MBI, compared to placebo, and led to transient decreases in alcohol cravings. Esketamine also resulted in significantly greater mystical experiences and dissociative states compared to placebo.
Conclusions:
The findings suggest that esketamine may improve treatment outcomes when combined with mindfulness-based therapies through its ability to increase engagement with meditative practice.
Keywords
Introduction
Alcohol misuse is a major health problem worldwide and is the biggest risk factor for premature death, ill health, and disability among 15- to 49-year-olds (World Health Organisation, 2023), with only 18% of alcohol-dependent drinkers undergoing treatment in the UK (National Audit Office, 2023). Despite the current pharmacological and behavioural treatments available for alcohol use disorder (AUD), individuals who do receive treatment are 70%–80% likely to relapse within the first year (Bradizza et al., 2006), and many of these treatments are susceptible to delivering modest effects (Rothberg et al., 2021) and high attrition rates (Basu et al., 2017). This demonstrates the urgency and importance of developing more effective treatments for AUD.
Recent advances in addiction research have highlighted the therapeutic effects of ketamine in AUD. The N-methyl-D-aspartate antagonist ketamine, particularly esketamine (the S-enantiomer of ketamine), is showing increasing promise in clinical settings. Research has suggested that esketamine shares many similarities with racemic ketamine (Bahji et al., 2021); however, esketamine has greater analgesic effects due to its stronger antagonist action at the phencyclidine site on the NMDA receptor (Matveychuk et al., 2020). Ketamine has a good safety profile and does not produce cardiac or respiratory depression (Ivan Ezquerra-Romano et al., 2018), making it a favourable drug to administer in clinical contexts. In recent years, the administration of ketamine has been shown to decrease alcohol cravings (Yoon et al., 2019), aid in maintaining abstinence (Krupitsky and Grinenko, 1997) and reduce alcohol consumption (Dakwar et al., 2020) for individuals with alcohol dependence. Yoon et al. (2019) found that ketamine combined with naltrexone for individuals with major depressive disorder led to 80% of participants reporting fewer alcohol cravings at 4 weeks post-intervention. Krupitsky and Grinenko (1997) discovered that people who underwent existential psychotherapy combined with one dose of ketamine were 66% more likely to remain abstinent after a year, compared to 24% who received standard psychotherapy without ketamine. Dakwar et al. (2020) found that when compared to midazolam and motivational enhancement therapy (MET), ketamine plus MET resulted in a significant reduction in the number of heavy drinking days and lower attrition rates over 21 days post-drug. While the exact mechanisms underlying ketamine’s efficacy remain unclear, Dakwar et al. (2020) suggested that one mechanism by which ketamine may be beneficial is by allowing more meaningful engagement in therapy.
‘Mindfulness’ describes the awareness that arises when an individual consciously attends to the environment with interest and without judgement (Kabat-Zinn, 1994). Despite originating around five millennia ago in ancient Eastern and Buddhist philosophy, secular mindfulness has recently gained popularity in the Western world to enhance performance and well-being. The practice has become increasingly popular in mental health treatment in mindfulness-based interventions (MBIs), which combine key elements of mindfulness practice and psychological therapy (Gu et al., 2015). While both mindfulness and ketamine alone can generate therapeutic effects in mental health, it has been suggested that combining both approaches would yield better treatment outcomes. Both ketamine and mindfulness can produce intense ‘peak experiences’ (Dorjee, 2016; Nour and Carhart-Harris, 2017), altered states of consciousness, and mystical experiences (Millière et al., 2018). The beneficial impact of combining both approaches for AUD has now been demonstrated in clinical trials (Dakwar et al., 2020; Grabski et al., 2022).
The combination of both ketamine and mindfulness may be more beneficial for treatment outcomes in two ways (Payne et al., 2021). Firstly, ketamine may act as an experiential stepping stone to deeper, more meaningful mindfulness practise. The initiation of mindfulness practise can be difficult, especially for beginners, leading to increased confusion and decreased motivation to continue (Hunt et al., 2020). However, psychedelics, such as ketamine, produce states of consciousness that mirror deep meditative experiences, which may be a helpful illustration to motivate mindfulness practise (Payne et al., 2021). Ketamine may therefore, by producing an experience that resembles meditative states that would ordinarily take years of practise to achieve (Sedlmeier et al., 2018), promote motivation towards the practice.
Secondly, ketamine may aid in increasing engagement in therapy through the drug’s ability to decrease avoidance in meditation (Smigielski et al., 2019). While practising meditation can be rewarding, the process can generate distressing thoughts and emotions, which can induce psychological defence mechanisms (Lomas et al., 2015) and experiential avoidance (Hayes et al., 1996) that may restrict the effectiveness of the mindfulness practice. However, the addition of psychedelics with mindfulness may equip individuals with optimistic, less judgmental and anxiety-prone insights, which consequently buffer any negative experiences that may occur through deep meditative states (Payne et al., 2021). While the classification of ketamine as a psychedelic has been highly debated, many have included it in this class (e.g. Luke, 2012).
While most studies thus far with ketamine as a treatment for AUD have aimed for abstinence, it is increasingly acknowledged that controlled drinking, as opposed to complete abstinence, is a realistic goal for many AUD and is associated with numerous physical and mental health benefits (Witkiewitz et al., 2020). Given that ketamine is beneficial when combined with mindfulness-based approaches in alcohol and cocaine use disorder and that ketamine has been found to reduce attrition rates for people undertaking this practise, this study set out to investigate the impact of a single dose of esketamine on engagement with mindfulness practise in hazardous drinkers. We hypothesised that esketamine may enhance engagement in MBI and that this enhancement would be associated with better drinking-related outcomes for hazardous drinkers.
Methods
A detailed method and analysis plan were pre-registered at the Open Science Framework. https://doi.org/10.17605/OSF.IO/5SY4C
Participants and design
In all, 28 participants were recruited from the community using social media advertisements; all participants produced a score between 8 and 40 on the AUD Identification Test (Saunders et al., 1993), either meeting the criteria for hazardous drinking (a score of 8–14) or moderate to severe AUD (a score of 15–40), were above the age of 18, were fluent English speakers and were seeking to reduce their alcohol consumption. Individuals were excluded if they had a history of psychosis or schizophrenia, were in treatment for a substance use disorder, had high blood pressure (>140/90) upon screening, had a body mass index (BMI) less than 16 or greater than 35, were on any medication contraindicated for use with ketamine or produced a positive urine screen for ketamine. Participants who displayed symptoms of alcohol withdrawal were also excluded based on an assessment made by the on-site psychiatrist.
This was a double-blind placebo-controlled mixed within- and between-measures study. Participants enrolled in a 2-week-long study where they were randomised in a 1:1 ratio to receive either esketamine hydrochloride in the form of two oral thin film strips (AWAKN002: total dose = 115.1 mg) or two strips of oral thin film vitamin C (placebo). Participants came into the study centre twice during the study: (1) for a screening visit (day 1) and (2) for drug administration (day 8) and provided online follow-up data on day 14. The study was approved by the institutional committee and all participants gave written informed consent.
Procedure
Participants visited the study centre for two sessions – an initial screening visit where their BMI, blood pressure and urine were assessed to determine eligibility with baseline measures completed immediately afterwards. They were given a daily mindfulness practise to complete each day for the next week. Participants then returned 7 days after the baseline visit for the drug administration visit. On this visit, participants completed several measures of psychological well-being, mindfulness and alcohol craving (see Figure 1) and were breathalysed to ensure they were alcohol-free. They were given the oral thin film of esketamine or placebo, and once the drug had been administered (see below), participants were given an eye mask to wear, and the option to listen to some soothing music through their headphones for 40 min. They then completed some post-drug follow-up measures. They were again given a daily mindfulness practise for the next 7 days (see Figure 1). Follow-up measures were completed online 14 days following the baseline visit.
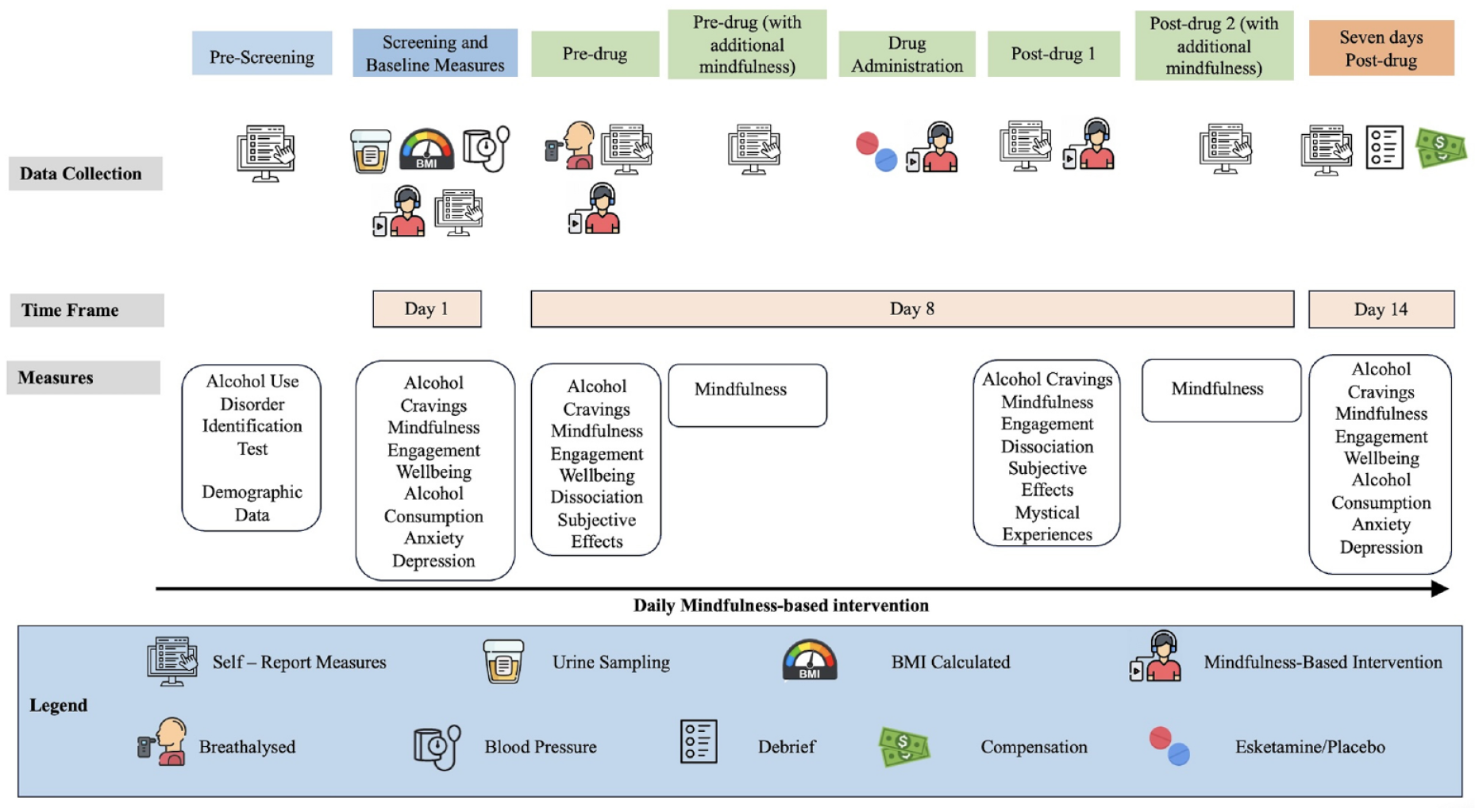
Overview of procedure and study timeline depicting measures taken at each study visit.
Mindfulness-based intervention
During the screening visit, participants listened to three introductory mindfulness recordings, which described the benefits of mindfulness-based relapse prevention and helped provide the tools necessary to acknowledge alcohol cravings. For the duration of the study, participants were prompted to complete 14 daily MBI sessions via email, each lasting between 5 and 25 min.
The mindfulness sessions provided participants with a basic meditation practice suitable for beginners, letting subjects become relaxed and centred, embracing any thoughts or sensations during the experience. On days 7 and 14, subjects received an addiction and relapse prevention mindfulness practice. This session was tailored more specifically to problem drinking, helping participants recognise and acknowledge alcohol cravings while focusing on the ‘four ways’: breathing mindfully, recognising body signals, acknowledging thoughts and allowing the mind to wander.
Drug administration
During the second week of the study, on day 8, participants came to the research centre, where they received either esketamine hydrochloride in the form of two oral thin film strips (total dose = 115.1 mg; LTS Ohmann) or vitamin C (placebo, Bon Ayu) using a 1:1 ratio. Participants were required not to consume alcohol for 24 h, to fast for 4 h, and to only consume clear liquids 2 h prior to the administration to reduce the risk of vomiting. Participants were prepared for the esketamine experience they may encounter via a script read by the researcher. Once dosed, subjects listened to relaxation music for 40 min. The session duration of 40 mins was determined by following pilot work with esketamine (Rosenbaum et al., 2023), but the participants remained in the research centre until they had recovered from the effects of the drug and a medical doctor assessed participants’ ‘street readiness’ before they were discharged.
Measures
Engagement
Engagement in mindfulness was measured using an adapted scale created by Banerjee et al. (2018). To measure psychological engagement, a four-item questionnaire using a five-point scale, from 1 (extremely unlikely) to 5 (extremely likely) was used. The physical engagement was characterised by the frequency of practised mindfulness, measured by two self-report questions. Items included ‘On how many days (over the past week) did you practice mindfulness meditation at least once?’ and ‘How many times on average did you practice mindfulness meditation each day?’ Answers from both items were multiplied together to determine an overall physical engagement score.
Mindfulness
Mindfulness was measured using the Five Facets of Mindfulness Questionnaire (FFMQ-15; Baer et al., 2012), a 15-item questionnaire assessing five subscales of mindfulness: observing, describing, acting with awareness, non-judgement and non-reactivity. Additionally, the Mindfulness Attention Awareness Scale (MAAS; Brown and Ryan, 2003), a 15-item questionnaire, was also used to assess mindfulness.
Alcohol-related outcomes
Alcohol-related secondary outcomes, such as craving and alcohol consumption, were assessed using the Alcohol Craving Questionnaire Short-Form Revised (ACQ-SF-R; Singleton, 1995) and the Timeline Follow-Back Method (TLFB; Sobell and Sobell, 1992), respectively. The TLFB method was used to measure the number of alcohol units consumed, with 1 unit equating to 8 g of alcohol.
Subjective effects of ketamine
Dissociative states were measured using the Clinician-Administered Dissociative States Scale (CADSS; Bremner et al., 1998); subjective effects of esketamine, measured by the Bodily Symptoms Scale (BSS; Morgan et al., 2004); mystical experiences, measured by the Mystical Experience Questionnaire (MEQ-30; Pahnke, 1963).
Mood and well-being
Depressive symptoms were measured with the Eight-item Patient Health Questionnaire for Depression (PHQ-8; Kroenke et al., 2009); anxiety symptoms, by the Generalised Anxiety Disorder Assessment (GAD-7; Spitzer et al., 2006); and general well-being, measured by the Warwick-Edinburgh Mental Well-being Scale (WEMWBS; Tennant et al., 2007).
Statistical analysis
A detailed analysis plan was pre-registered at the Open Science Framework. https://doi.org/10.17605/OSF.IO/5SY4C
To analyse participant demographics between groups, independent sample t-tests were conducted, and chi-squared statistics were reported for categorical data. For continuous data, a Mann–Whitney U statistic was reported if the data was non-parametric. Main analyses of engagement, alcohol craving and mindfulness changes were analysed using multilevel modelling with time and group as the fixed effects variables and participants as the random effects variable. Secondary outcomes, such as mystical experiences, were analysed using an independent t-test. Jamovi Version 2.3 (https://www.jamovi.org) was used to conduct all analyses.
Mediation analysis was used to examine whether changes in engagement mediated changes in alcohol cravings. The jAMM model in Jamovi with bias-corrected 95% confidence intervals and the bootstrapping method with 5000 samples were used for the analyses.
Results
Participants
In all, 38 individuals were recruited, and after exclusions and drop-outs, 28 participants were enrolled in the study (Figure 2). In total, 15 participants met the criteria for hazardous drinking and 13 participants were indicative of AUD. See Table 1 for participant demographic data. Both groups were similar in their demographic characteristics, with no significant differences in any of the demographic variables following Mann–Whitney U or chi-squared tests.
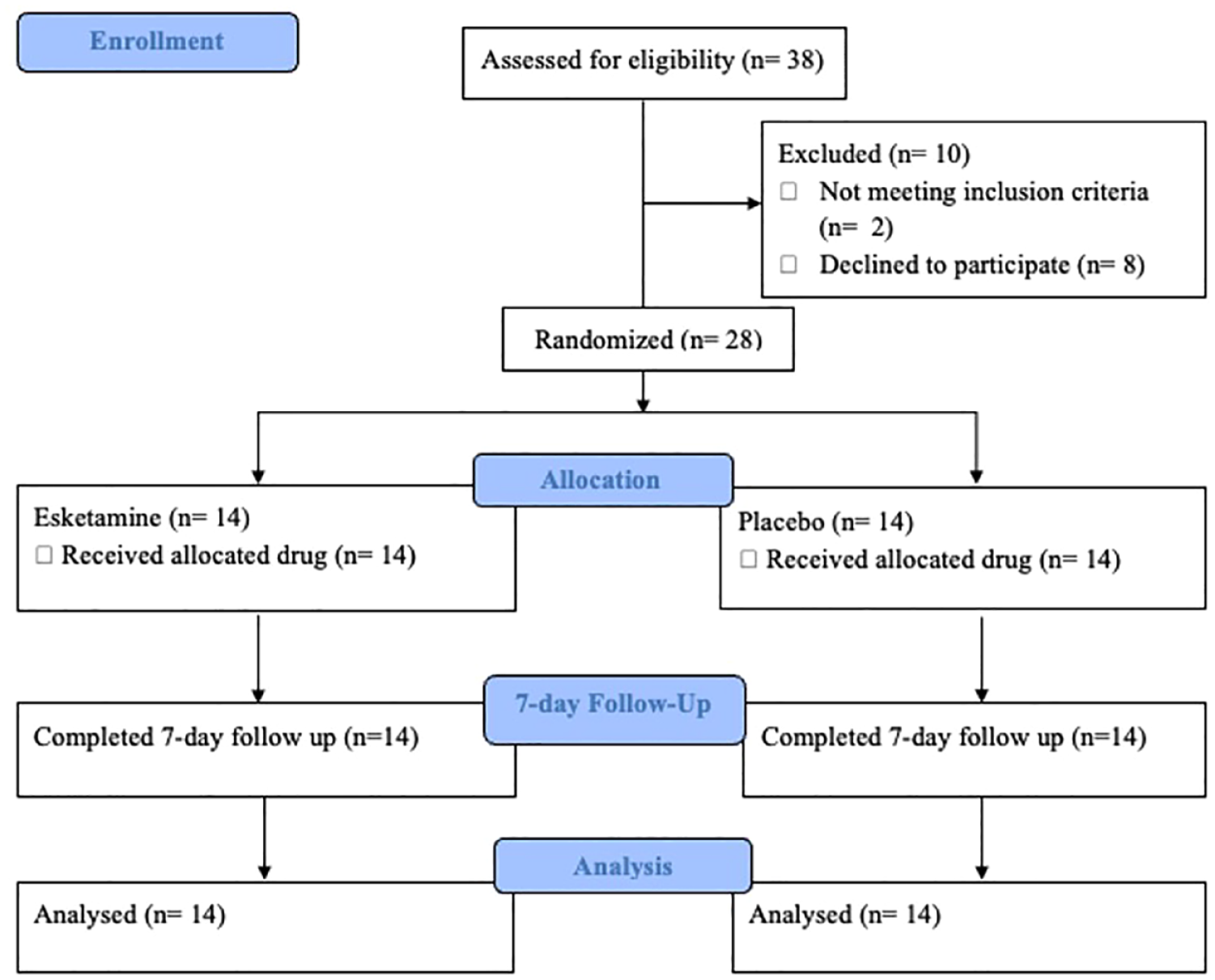
Study flow diagram portraying participants who were recruited, excluded and enrolled in the study.
Baseline participant’s characteristics of both esketamine and placebo conditions.
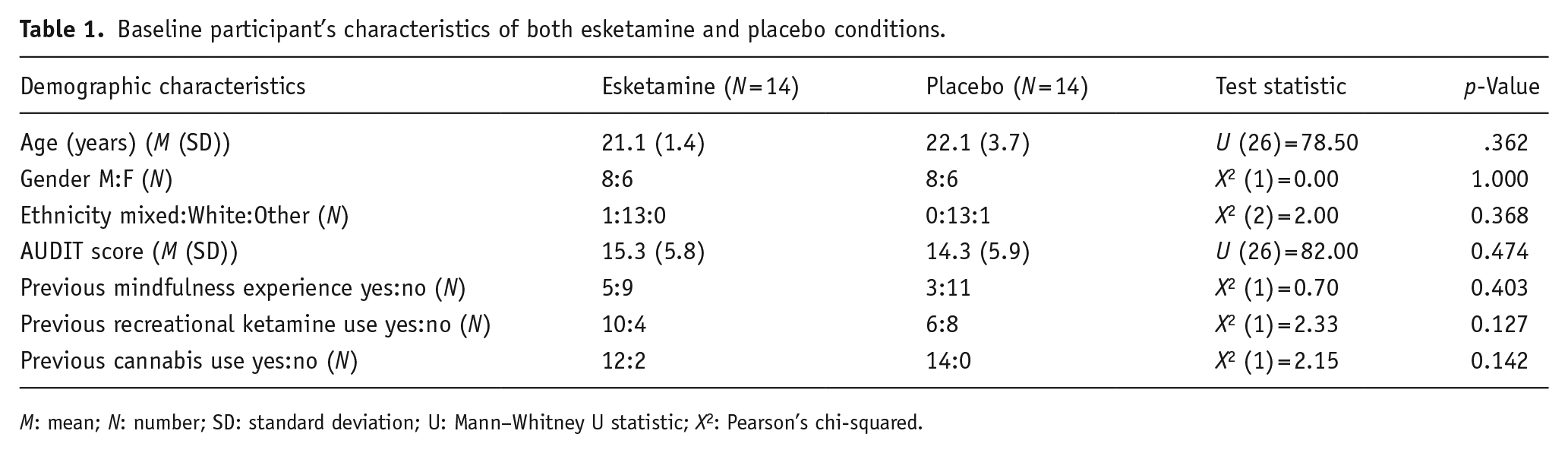
M: mean; N: number; SD: standard deviation; U: Mann–Whitney U statistic; X2: Pearson’s chi-squared.
Primary outcome: Engagement (psychological and physical) in MBI
In the mixed model analysis of psychological engagement, there was a significant main effect of group (F (1, 26) = 6.88, p = 0.014) and time (F (2, 56) = 5.47, p = 0.007), as well as time-by-group interaction (F (2, 52) = 6.45, p = 0.003). To further investigate these findings, a simple effects analysis revealed a significant difference between pre-drug and seven days post-drug for the esketamine condition (t (52) = −3.29, p = 0.002) but not for the placebo condition (t (52) = 1.71, p = 0.093) (see Figure 3). However, no significant main effect of time, group or time-by-group interaction was found for physical engagement (see Table 3 for data).
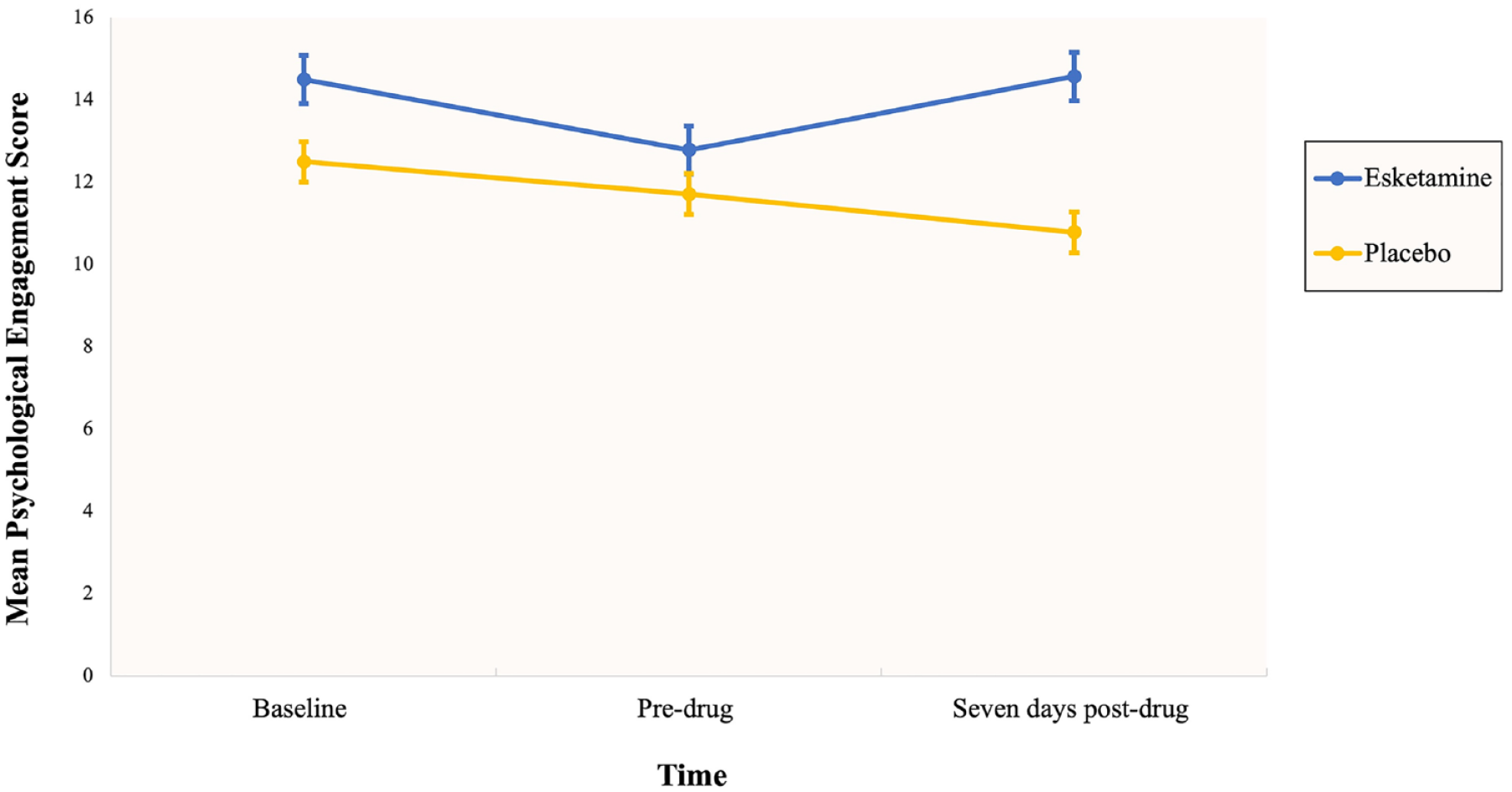
Changes in psychological engagement in mindfulness-based interventions across time.
Mindfulness
For scores of mindfulness measured using the FFMQ-15, the mixed model analysis revealed no significant main effect of group or time and no significant time-by-group interaction, while using the MAAS, there was a significant main effect of time (F (1, 26) = 6.21, p = 0.019) where mindfulness increased over the study period but no main effect of group or interaction (displayed in Table 2).
Table showing means and standard deviation for trait mindfulness (FFMQ-15 and MAAS scores).
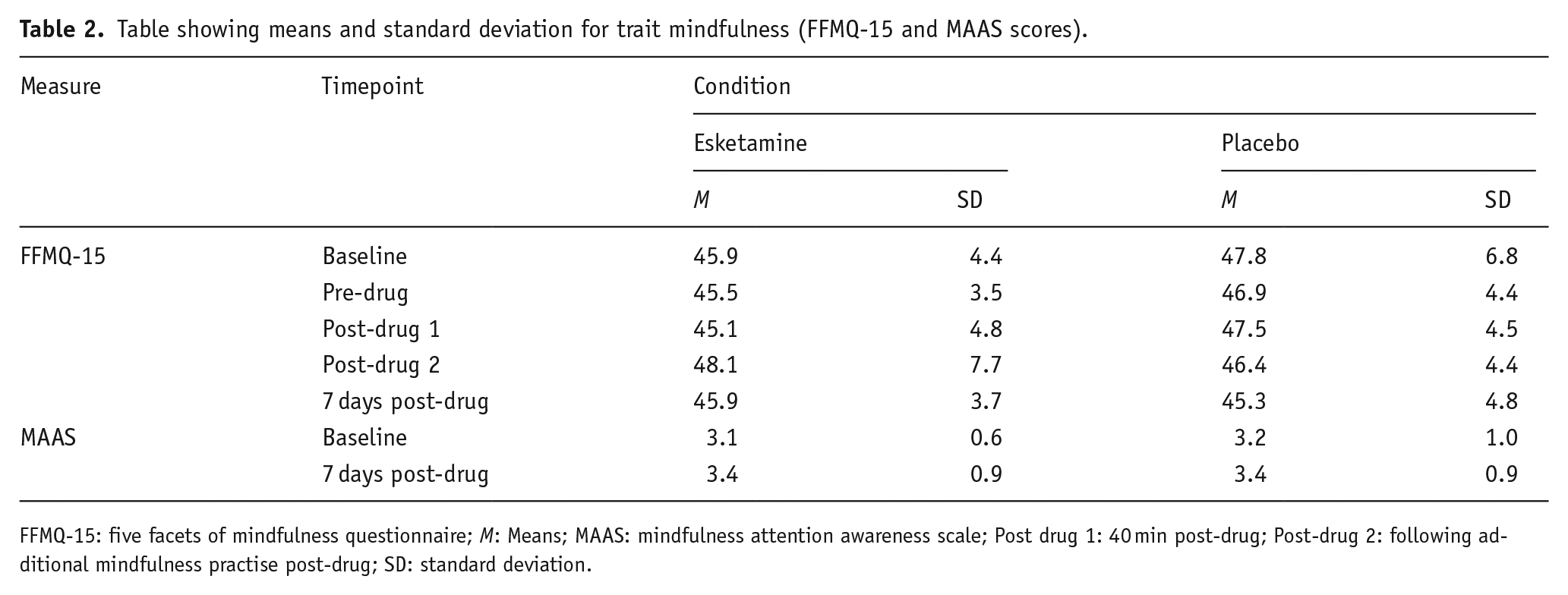
FFMQ-15: five facets of mindfulness questionnaire; M: Means; MAAS: mindfulness attention awareness scale; Post drug 1: 40 min post-drug; Post-drug 2: following additional mindfulness practise post-drug; SD: standard deviation.
Alcohol craving
There was a significant main effect of time (F (3, 77.2) = 15.23, p ⩽ 0.001) and a significant group-by-time interaction (F (3, 77.2) = 5.64, p = 0.002) on alcohol craving. To further investigate these findings, a simple effects analysis was conducted, revealing a significant decrease in alcohol cravings from pre- to post-drug administration for the esketamine condition (t (77.52) = 2.76, p = 0.007) but not for the placebo condition (t (77.01) = −1.66, p = 0.101). See Figure 4 for data.
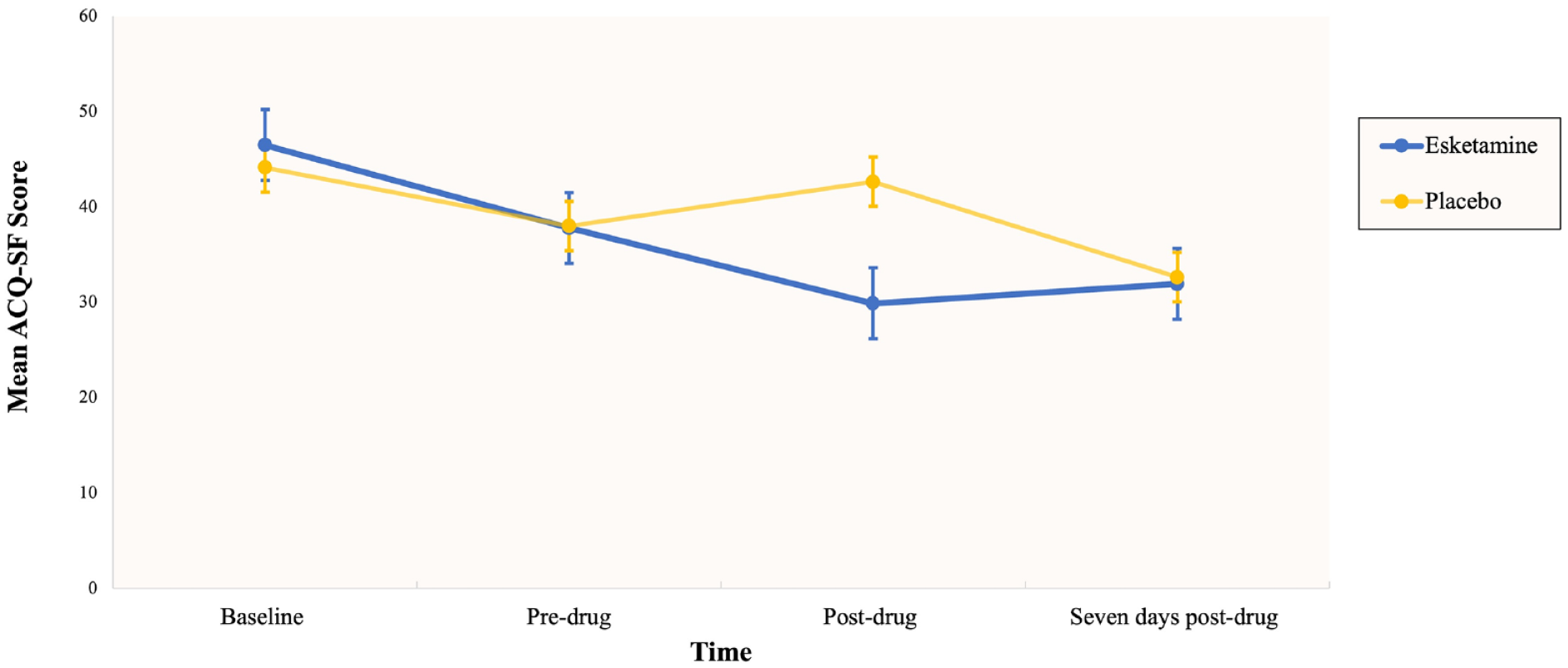
The impact of esketamine on mean alcohol craving score across four time points, baseline (day 1), pre and post-esketamine administration on day 7, and day 14 of the mindfulness practice.
Alcohol consumption
For alcohol consumption on the TLFB, the mixed model analysis revealed a significant main effect of time (F (1, 26) = 9.48, p = 0.005) with lower alcohol consumption at the study end, but no significant main effect of the group nor an interactional effect (See Table 3 for data).
Table showing means and standard deviation for measures at baseline, pre-drug and 7 days post-drug.
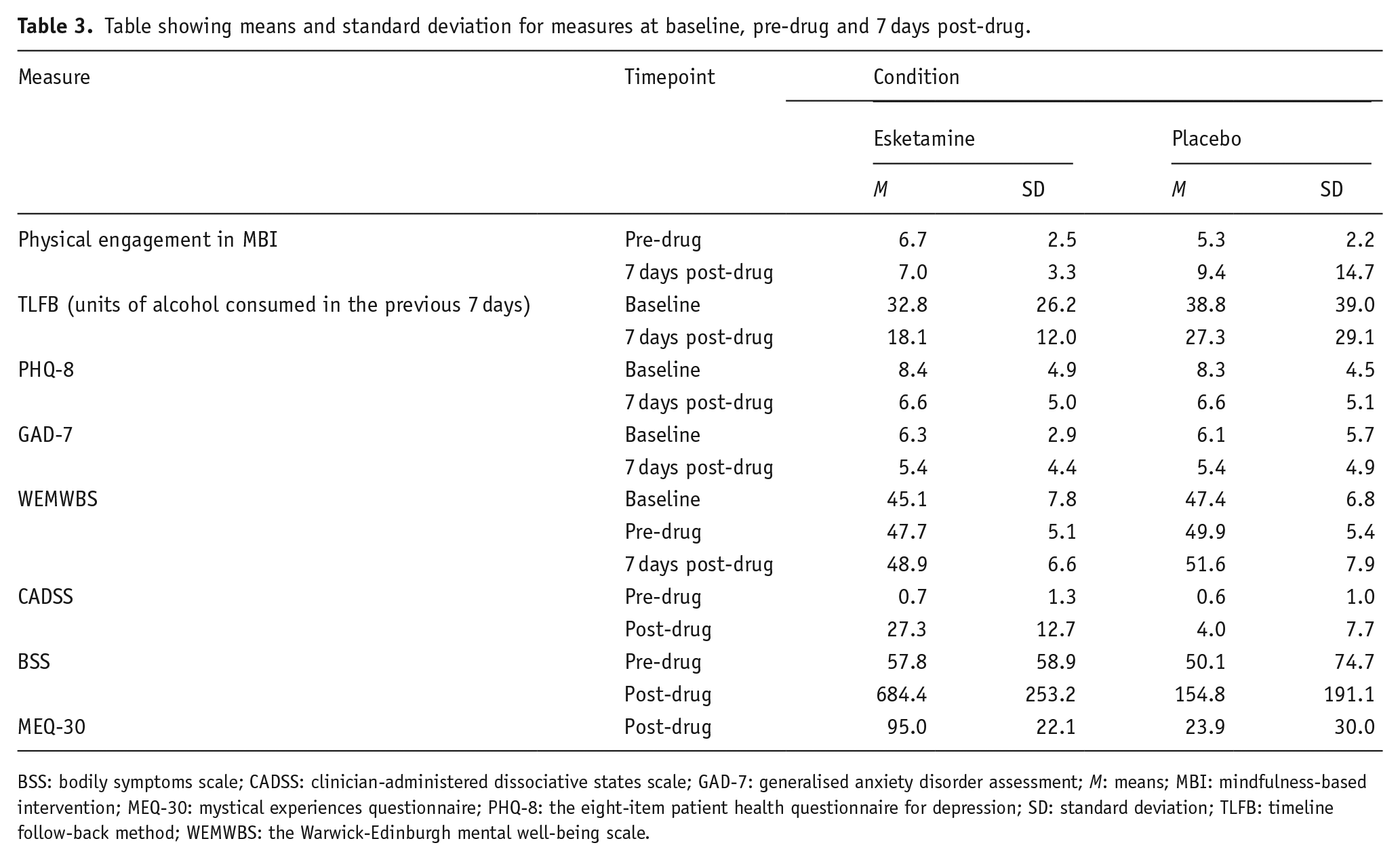
BSS: bodily symptoms scale; CADSS: clinician-administered dissociative states scale; GAD-7: generalised anxiety disorder assessment; M: means; MBI: mindfulness-based intervention; MEQ-30: mystical experiences questionnaire; PHQ-8: the eight-item patient health questionnaire for depression; SD: standard deviation; TLFB: timeline follow-back method; WEMWBS: the Warwick-Edinburgh mental well-being scale.
Mood and well-being
For secondary outcomes such as anxiety, depression and general well-being the time-by-group interaction was not significant for any of the models. However, there was a significant main effect of time for depression (F (1, 26) = 2.41, p = 0.046) reflecting an overall reduction in scores from the start of the study to the end in both the placebo and esketamine groups. Additionally, there was a significant main effect of time for general well-being (F (2, 52) = 3.46, p = 0.039), with well-being increasing for both groups across the three time points (data displayed in Table 3).
Subjective effects of esketamine
There was a significant time-by-group interaction effect for dissociative states (F (1, 26.22) = 35.37, p ⩽ 0.001) and bodily symptoms (F (1, 26) = 42.37, p ⩽ 0.001), and it was found that the administration of esketamine in comparison to placebo led to significantly greater mystical-type experiences (see Table 3).
Mediation
Alcohol cravings. A regression analysis was performed with alcohol craving as the outcome variable, and esketamine as the predicting variable. The overall model was not significant (F (1, 109) = 1.44, p = 0.233, R2 = 0.013). In the mediation model, esketamine was significantly associated with psychological engagement (path a); however, psychological engagement was not significantly associated with alcohol craving (path b). The direct path from esketamine to alcohol craving was also not significant (path c′). Lastly, the indirect effect of esketamine to alcohol craving via psychological engagement was not significant (β = 0.03, p = 0.565).
Discussion
To our knowledge, this is the first study to explore whether esketamine works therapeutically by enhancing engagement in MBI and whether this influences treatment outcomes. It was found that, in comparison to the placebo, esketamine enhanced psychological engagement in meditative practice and produced transient decreases in alcohol cravings. This occurred in the absence of group differences in subjectively rated mindfulness. Both groups increased in ratings of mindfulness across the 2-week period and decreased alcohol consumption. Research has demonstrated that ketamine is beneficial as an adjunct to psychological therapies (Grabski et al., 2022) and while many theoretical explanations have been proposed to explain the mechanisms that underlie ketamine’s efficacy, such as its antidepressant effects (Serafini et al., 2014), the disruption of the reconsolidation of drug-related memories (Das et al., 2019) and its effect on neural plasticity (Ivan Ezquerra-Romano et al., 2018), the precise mechanisms remain ambiguous. However, the finding that esketamine led to significantly greater psychological engagement with mindfulness practice provides supporting evidence for the hypothesis that ketamine may increase engagement in treatment (Dakwar et al., 2019). The addition of ketamine to MBI can help overcome meditation-associated difficulties such as decreased motivation (Hunt et al., 2020), increased attrition rates and experiential avoidance (Hayes et al., 1996), which are achieved through ketamine’s facilitation of profound meditative states of consciousness (Soler et al., 2016) and the generation of optimistic, non-judgemental and anxiety-free emotional states (Payne et al., 2021). In contrast to self-rated psychological engagement, no significant differences were observed for physical engagement which reflected the number of sessions of meditative practise.
The finding that esketamine increases psychological engagement within meditative practice also has important clinical implications. It suggests that ketamine may advantageously reduce the likelihood of individuals dropping out of MBIs and, therefore, decrease the likelihood of relapse. While MBIs are highly efficacious (Sancho et al., 2018), they suffer high attrition rates (Lam et al., 2022), which demonstrates the potential utility of incorporating ketamine into these types of therapies. It would be interesting to examine whether these effects generalise to other types of psychological therapy beyond mindfulness and suggest a nonspecific, yet important role for ketamine in augmenting therapy.
While the main aim of this study was to understand the underlying therapeutic mechanisms of esketamine, it also set out to explore whether esketamine and MBI combined would lead to changes in alcohol-related outcomes. Although decreases in alcohol consumption were sustained, they were not significantly different between groups. This differs from previous research (Dakwar et al., 2020; Grabski et al., 2022) that has shown the effectiveness of ketamine in reducing alcohol consumption and demonstrates an absence of these effects for hazardous drinkers given a single dose of esketamine. However, esketamine was found to significantly decrease alcohol cravings post-drug administration, compared to the placebo condition. One explanation for these findings is that positive expectations of receiving the drug could have led to increased alcohol cravings in the placebo condition, especially if participants had a degree of investment in receiving the drug, thus leading to the nocebo effect. Moreover, individuals may be less inclined to seek alcohol during the immediate post-ketamine phase. The reductions in cravings were transient and failed to last for 7 days post-drug, which is inconsistent with previous research (Dakwar et al., 2019; Yoon et al., 2019). One explanation for this finding could be due to the sample of harmful drinkers rather than treatment-seeking patients with severe AUD, as has been used in previous studies (e.g. Grabski et al., 2022), which may have impacted results; cravings were likely higher pre-ketamine in the dependent group of alcohol users from these studies.
Increases in mindfulness were observed across both conditions and align with the research of Dakwar et al. (2019), who found no significant differences between the ketamine and placebo conditions, using the same scale. This may reflect a lack of sensitivity to the measure, which has in the past been criticised as individuals’ self-attributed mindfulness levels may differ from their actual ability to be mindful, and additionally a shift in the internal reference point may occur as individuals may assess themselves as being more (or less) mindful after an MBI.
While these findings have revealed that increased psychological engagement within meditative practise is a consequence of esketamine, they do not provide evidence that it is associated with better alcohol-related outcomes. The decision to investigate the psychological underpinnings of esketamine alongside MBI rather than alternative therapies was largely informed by previous studies (Dakwar et al., 2019). While ketamine has been shown to have increasing benefits in combination with other therapies for addiction, studies have highlighted that it may be best suited in conjunction with mindfulness, as the ketamine experience can act as a catalyst for greater mindfulness practice (Dakwar et al., 2019). Additionally, both ketamine and meditation practice can give rise to mystical experiences (Millière et al., 2018), which can lead to significant perspective shifts (Krupitsky et al., 2002, 2007; Morgan et al., 2017) that can help contribute to its therapeutic effects. Additionally, the psychedelic model (Greenway et al., 2020) proposes that ketamine experiences produce ‘breakthrough realisations’, generate enhanced awareness of the unconscious processes that underlie addiction, and improve feelings of internal and external connectedness, which can also be beneficial in addiction recovery (Garel et al., 2022: 11). Considering that the esketamine condition experienced significantly more mystical experiences and dissociative states, this could be an additional explanation for the observed transient reductions in alcohol cravings.
Limitations
There are several limitations to this study. First, a limitation inherent to studies of psychedelic-like compounds, such as ketamine, is the issue of blinding participants due to the unique subjective effects associated with the drug. The inclusion of individuals with prior experience with ketamine (57%) and other recreational drugs compounded this issue. Ketamine is the third most common recreational drug of use, and its popularity is increasing in the UK (Office for National Statistics, 2023). While it may be beneficial to exclude those with prior experience, consequently this would exclude a substantial proportion of the hazardous drinking population and, hence, become a non-representative sample. For more effective blinding, future research should use an active placebo such as midazolam, which has been shown to reduce this bias in previous studies (Dakwar et al., 2019).
Second, the mindfulness training programme was very brief and may not have been able to produce the degree of change observed in formal MBI for mental health. Future research should consider testing similar changes in engagement and mindfulness with a more in-depth training programme involving multiple in-person experiential sessions over a number of weeks. We used subjective reports to measure engagement with MBI. Future research ought to explore the utilisation of objective methods to verify meditation practice engagement and ensure consistency when administering esketamine to all participants, which could also improve the reliability of study outcomes.
The lack of assessment of participants’ motivation to reduce alcohol consumption is another limitation. Hazardous drinkers, who report high motivation to decrease their alcohol consumption, are more likely to attempt to decrease their alcohol intake at a 6-month follow-up (De Vocht et al., 2018). Although all individuals in this study were seeking to reduce their alcohol use, their level of motivation was not assessed. Due to the impact that different levels of motivation can have on behaviour change, future research should consider including an assessment of motivation to reduce alcohol consumption and assess this throughout the study.
The issue of the population should also be recognised. The population largely consisted of hazardous drinking students, which may have contributed to the absence of a durable impact on alcohol-related outcomes. A follow-up study using treatment-seeking individuals may yield more promising findings.
Conclusion
Despite the limitations and brief nature of this study, this is the first to provide evidence that psychological engagement may be a factor in mediating treatment outcomes for ketamine-assisted therapy. Understanding the psychological underpinnings is vital for the development and advancement of ketamine-assisted therapy for AUD in society.
Supplemental Material
sj-jpeg-2-jop-10.1177_02698811241254834 – Supplemental material for Esketamine combined with a mindfulness-based intervention for individuals with alcohol problems
Supplemental material, sj-jpeg-2-jop-10.1177_02698811241254834 for Esketamine combined with a mindfulness-based intervention for individuals with alcohol problems by Emily M Gent, Joshua W Bryan, Maisy A Cleary, Tegan I Clarke, Harry D Holmwood, Rania O Nassereddine, Chris Salway, Simon Depla, Sarah Statton, Joy Krecké and Celia JA Morgan in Journal of Psychopharmacology
Supplemental Material
sj-jpg-1-jop-10.1177_02698811241254834 – Supplemental material for Esketamine combined with a mindfulness-based intervention for individuals with alcohol problems
Supplemental material, sj-jpg-1-jop-10.1177_02698811241254834 for Esketamine combined with a mindfulness-based intervention for individuals with alcohol problems by Emily M Gent, Joshua W Bryan, Maisy A Cleary, Tegan I Clarke, Harry D Holmwood, Rania O Nassereddine, Chris Salway, Simon Depla, Sarah Statton, Joy Krecké and Celia JA Morgan in Journal of Psychopharmacology
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Celia JA Morgan has received contract research funds from Awakn Life Sciences and has been seconded to their organisation. The other authors declare no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by funding from Awakn Life Sciences with additional funds from University of Exeter.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.