
Abstract
Background:
Medication adherence is a prerequisite to achieving beneficial treatment outcomes. In major depressive disorder, many patients fail to complete medication regimens, raising concern for poor treatment outcomes. It is usual to experience adverse drug reactions (ADRs) while taking antidepressants, and relative discomfort is reported by patients.
Aims:
The present review focuses on the presence of antidepressant-related side effects and the subsequent relationship with medication non-adherence.
Methods:
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed. Following the preliminary research, the research question and eligibility criteria were created based on the PICO framework. All articles retrieved from the selected databases were exported to Covidence, a Systematic Review managing software tool. Two reviewers assessed the papers to identify the risk of bias using the Joanna Briggs Institute critical appraisal tool for cross-sectional studies. Seven studies with a low–moderate risk of bias fulfilled the eligibility criteria and were conducted from 2013 to 2020 in Europe, Africa and Asia.
Results:
The results demonstrated high levels of suboptimal adherence ranging from 46% to 83% amongst the studied population. A variety of side effects were reported by a significant number of participants predominantly with moderate severity. A correlation between the presence of ADRs and suboptimal rates of adherence to antidepressants was found. Somnolence and headaches among other unspecified ADRs were found to increase the dropout rates for selective serotonin reuptake inhibitors.
Conclusions:
The present study elucidates the need for effective interventions to facilitate antidepressant adherence and enhance doctor–patient communication, benefiting both the individuals and the healthcare system and leading to better clinical outcomes and reduction of relapse-related costs.
Introduction
Adherence is a core component of medical treatment and can be defined as compliance with the guidelines provided by the physician regarding the taking of medicines (Keyloun et al., 2017). Medication adherence (MA) has been proven to be a prerequisite to achieving beneficial treatment outcomes, and failure to comply with medication regimes has been associated with negative consequences, not only on an individual level by jeopardising patients’ health but also on the wider community level, amplifying the healthcare costs caused by disease reoccurrence (Marrero et al., 2020).
Research has demonstrated suboptimal levels of adherence to medication in various chronic conditions such as hypertension (Tedla and Bautista, 2016) and HIV (Zhang et al., 2016) as well as in several mental health conditions such as schizophrenia (DiBonaventura et al., 2012) and depression (Ho et al., 2017). Specifically, in major depressive disorder (MDD), the dropout rates (rates of patients failing to complete their medication regimens) fluctuate from 10% to 60%, raising concern for poor treatment outcomes and subsequent increase in hospitalisation and emergency visits rates (Krivoy et al., 2016).
MDD as a disabling condition puts a significant burden on public health systems worldwide, affecting patients’ quality of life by aggravating morbidity and mortality levels, and increasing the need for healthcare services (Ho et al., 2017). Several studies suggest that MDD prevalence rates remain stable with societal and demographic factors influencing fluctuations in different geographical locations (Murphy et al., 2000; Rait et al., 2009; Richter et al., 2019; Schürmann and Margraf, 2018). Yet, others argue that it is expected to be one of the leading causes of illness by the end of the decade (Mathers and Loncar, 2006). MDD symptoms have been proven to decrease with the pharmacological treatment of antidepressant medication, resulting in better health outcomes and decreased mortality (Keyloun et al., 2017).
Antidepressants (ADs) are a core part of the treatment procedure for moderate or severe depression based on the NHS guidelines (NHS, 2021a), the National Institute for Health and Care Excellence (NICE, 2022) and are further corroborated by the literature (Cleare et al., 2015; Kennedy et al., 2016). The pharmacological treatment with antidepressants can be divided into two phases: the initiation/acute phase (6–12 weeks) and the continuation phase (4–9 months) (Keyloun et al., 2017). Several types of antidepressants can be clustered in groups: Selective serotonin reuptake inhibitors (SSRIs) such as fluoxetine, serotonin-noradrenaline reuptake inhibitors (SNRIs) such as venlafaxine, noradrenaline and specific serotonergic antidepressants such as mirtazapine, tricyclic antidepressants (TCAs) such as amitriptyline, serotonin antagonists and reuptake inhibitors such as trazodone and monoamine oxidase inhibitors such as phenelzine (NHS, 2021a).
Previous research has highlighted that adherence to antidepressant medication is often lower than in medication for other chronic conditions such as diabetes or hypertension (Keyloun et al., 2017). Therefore, it is vital to explore the factors that lead to optimal adherence to antidepressants. Factors influencing MA have been associated with characteristics related to the patient, the medication, the illness and the clinical setting (Hassan et al., 2016). In more detail, patient-related factors include beliefs and fears about medicines, gender, patients’ literacy, economic status, social support, etc. Medication-related factors include adverse side effects and desired efficacy, while illness-related factors include the severity of depression and existing comorbidities. Finally, clinical setting factors include follow-up rates and doctor–patient communication (Hassan et al., 2016; Hung, 2014).
During the first period of taking antidepressants, it is usual to experience various adverse drug reactions (ADRs) which differ based on the type of medication prescribed. It is advised to continue the pharmacological treatment despite the ADRs because the benefits outweigh the discomfort caused by the side effects several weeks after the medication initiation. Specifically, SSRIs and SNRIs are usually responsible for agitation or anxiety, digestion, sexual and sleeping disorders, dizziness and headaches. TCAs can cause among others dry mouth, constipation, drowsiness and weight gain (NHS, 2021b).
The literature demonstrates that antidepressant-related side effects persist for more than half of the patients even after taking antidepressants for 75–105 days; this is often underestimated by healthcare providers resulting in poor patient–doctor communication about the prescription (Kelly et al., 2008). Also, treatment dropout due to antidepressant-related side effects is estimated to occur after 6.5–7 weeks, while other reasons result in later discontinuation (Kelly et al., 2008).
Aim and objectives
This review will focus on the presence of antidepressant-related side effects and the subsequent medication non-adherence as there is no systematic review exploring the effect of the antidepressants’ side effects on adherence. The first objective is to explore the prevalence of ADRs and MA among patients with depression over the last 10 years (2012–2022). Secondly, the authors aim to explore whether the presence of ADRs is associated with lower MA among patients with depression.
Methods
Protocol
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021) were followed and a study protocol was developed including the search strategy, the eligibility criteria, the data extraction items and the risk of bias assessment.
Search strategy
Preliminary research was conducted to explore the validity of the research idea. The EBSCO Discovery was used, and more broad search terms were selected. Google Scholar database was also used to investigate the systematic reviews that had already been conducted on this research area. Following the preliminary research, a more comprehensive list of search terms including three search clusters was developed (see Table 1) and the final research question was formulated based on the population, intervention, comparison, outcomes (PICO) framework (Methley et al., 2014) (see Appendix 1, Table A1). A systematic review search was performed on ‘APA PsycArticles’, ‘APA PsycInfo’, ‘MEDLINE’ and ‘Academic Search Complete’. Only research articles that were published in the English language in the last 10 years (2012–2022) in peer-reviewed journals were included by the filters selected in the search procedure. This time period was chosen as the purpose of the study was to explore contemporary data and because trends of antidepressant prescriptions by class are shifting through the decades as shown by Bogowicz et al. (2021).
Search strategy and keywords.
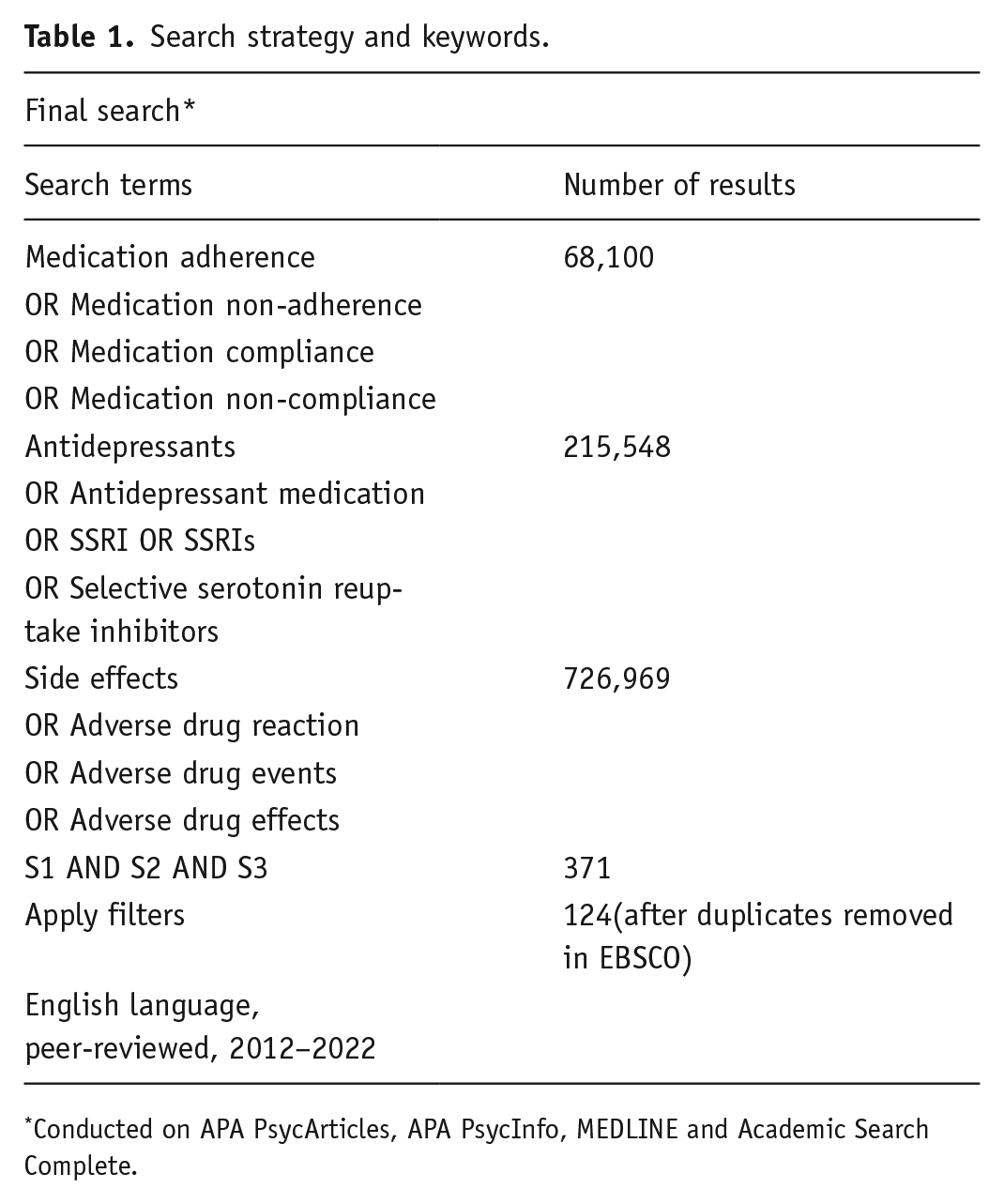
Conducted on APA PsycArticles, APA PsycInfo, MEDLINE and Academic Search Complete.
Eligibility criteria
The eligibility criteria were created based on the PICO framework. A primary diagnosis of depression and pharmacological treatment with antidepressants were the inclusion criteria. Animal studies, review articles, conference abstracts and editorials as well as studies with a qualitative design were excluded. Also, studies that focused on specific antidepressant medications or specific antidepressant side effects (e.g. sexual dysfunction) were excluded. This is because the present review aims to focus on multiple and not singular antidepressants and side effects. The focus on specific side effects among the studies would also affect the comparability of the findings. Longitudinal studies were also excluded as the measurements from different timepoints could be impacted by changes in the dose or type of medication. Similarly, studies with significant comorbidities and subsequent polypharmacy were excluded (e.g. HIV or cancer patients). Additionally, studies that focused on a specific population group (children, elderly, patients with another medical diagnosis, apart from depression, etc.) were excluded because of the complexity the management of their medication regimens might present (family members and caregivers could be involved).
Data extraction
All the articles retrieved from the selected databases after the three search clusters were combined with ‘AND’ and the filters were applied, were exported to Covidence, a Systematic Review managing software (Veritas Health Innovation, Melbourne, Australia). The data extraction was conducted by two reviewers. After the duplicates were removed, the reviewers did an initial screening of the title and abstract of the articles and subsequently reviewed the full text of the studies that were not excluded as irrelevant in the first stage. Conflicts were resolved through discussion meetings amongst the two reviewers until a consensus was reached. There were no instances where consensus was not reached. The screening and selection processes are described in Figure 1.
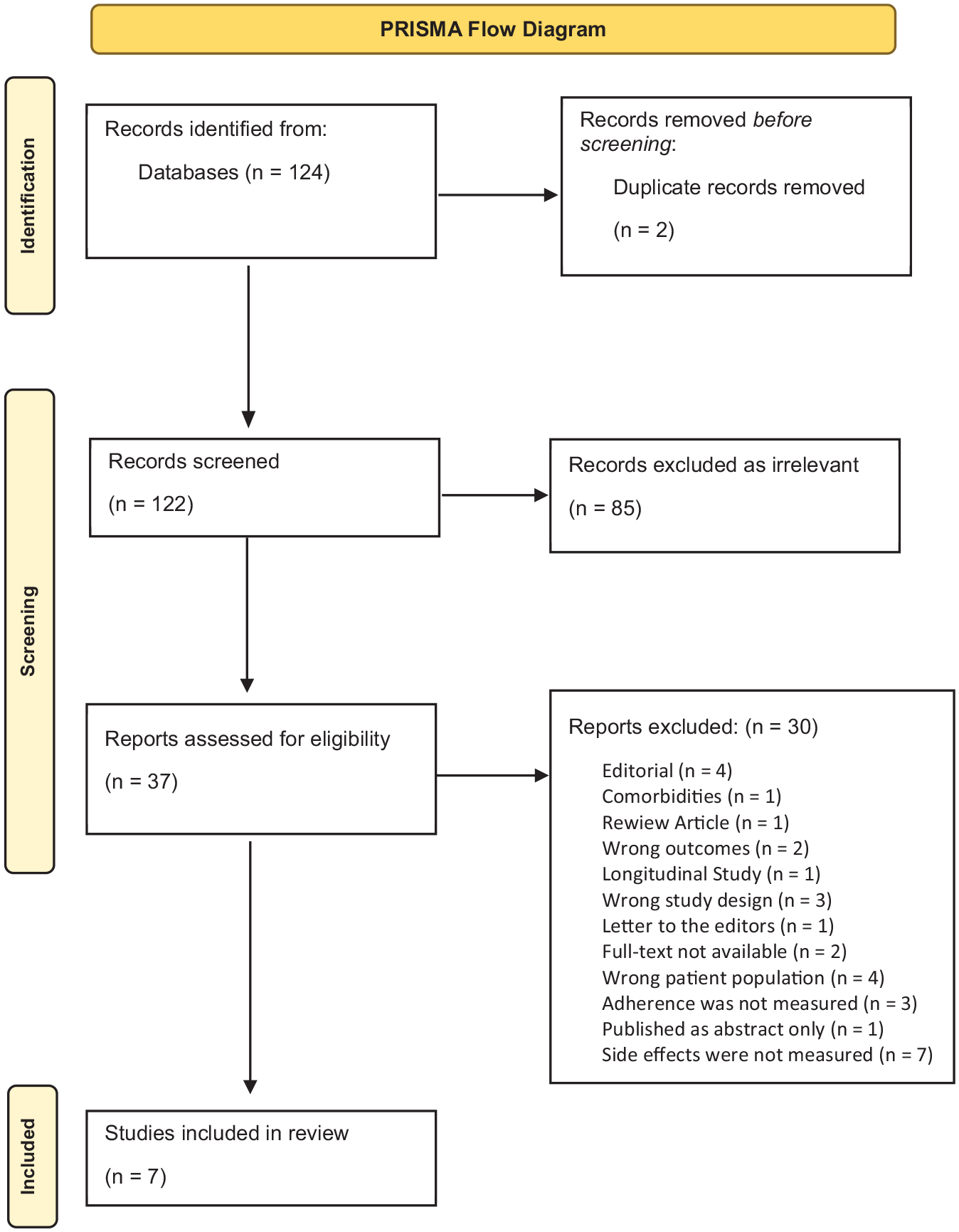
PRISMA flow diagram.
Data items
The data extracted were as follows: authors’ name, year of publication, number of participants and their primary diagnosis, country and setting where the study took place, study design, types of antidepressant medication, presence and severity of ADRs, MA levels and clinical outcomes. The limitations of the studies were also examined.
Study risk and bias assessment
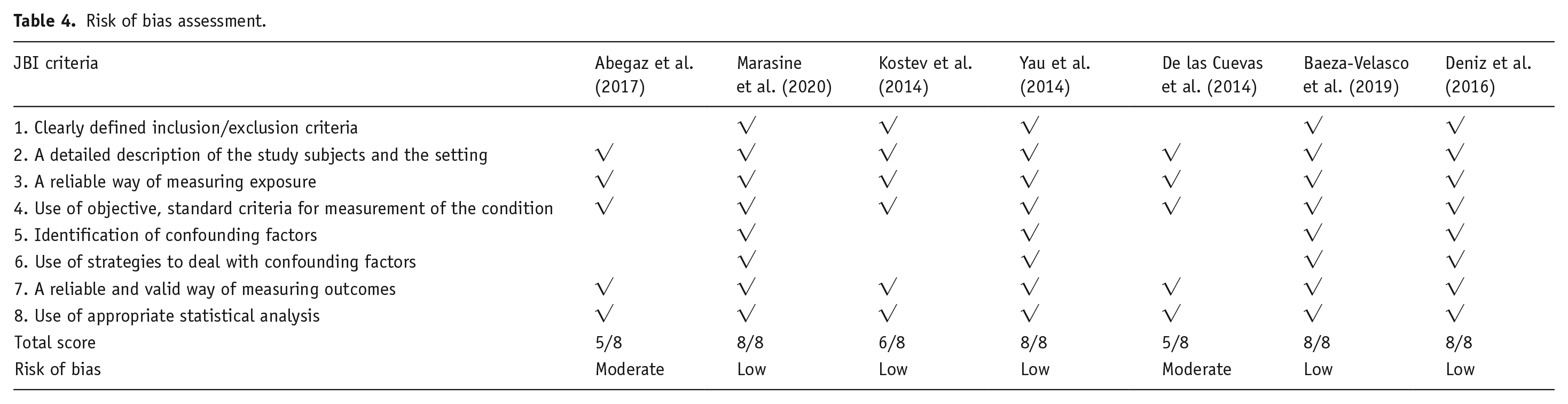
Two reviewers assessed the papers to identify the risk of bias using the Joanna Briggs Institute (JBI) critical appraisal tool for cross-sectional studies (Moola et al., 2020). A high risk of bias is identified for the studies that had a positive answer in less than half (<4) of the criteria, while a low risk of bias is present when the studies scored positive answers in more than 70% (>5.6) of the criteria. The rest of the studies presented a moderate risk of bias according to Moola et al. (2020) as low, medium and high risk of bias classification.
Results
Study selection
The study selection process is presented in Figure 1. The final search resulted in 124 studies of which 2 were duplicates and were removed before the screening. In all, 122 papers were included in the first screening stage and 85 of them were clearly irrelevant to the research question and were excluded based on the title and abstract. In all, 37 studies were included in the full-text screening stage. Finally, seven studies fulfilled the eligibility criteria. Three of the selected studies explored the factors associated with antidepressant medication non-adherence, finding ADRs to be one of them, while the other four specifically explored antidepressant side effects and MA.
Study characteristics
The selected studies were conducted from 2013 to 2020 in Europe (Spain, Germany and France), Africa (Ethiopia) and Asia (Turkey, Nepal and Hong Kong). The timeframe of the studies was from 3 months to 3 years and data were collected at a single point in time for each participant (no longitudinal studies were included). The participants of the final papers were adults over 18 years of age who had a primary psychiatric diagnosis of depression, with the female gender being overrepresented. The number of participants fluctuated from 53 to 50,824 (see Table 2).
Summary of included studies’ characteristics.
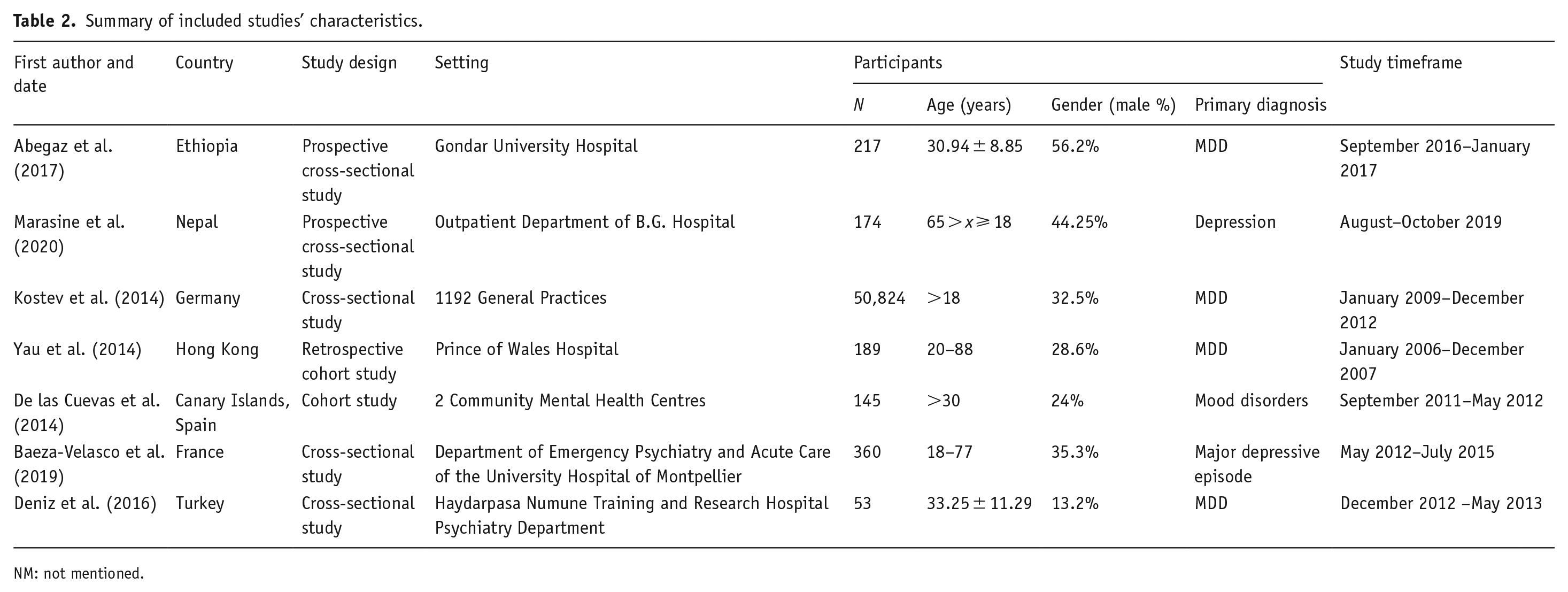
NM: not mentioned.
Methodological evaluation
Five of the selected studies had a cross-sectional design while the other two had a retrospective approach to collecting the data. Only one study was conducted in general practices and one in community-based mental health centres. Participants for the rest of the studies were hospital psychiatric patients. The clinical diagnosis of depression was one of the inclusion criteria and was determined by the psychiatrists based on the International Classification of Diseases (ICD-10) and the Diagnostic and Statistical Manual of Mental Disorders 4th Edition (DSM-IV). Regarding the ADRs and the MA, the studies that adopted a cross-sectional design utilised self-reported questionnaires to collect the data. The retrospective design studies used clinical information reported by physicians from computerised databases. Table 3 describes in detail the questionnaires used for each outcome variable. It can be noted that the majority of the studies utilised similar psychometric tools for data collection.
Summary of data collection process.
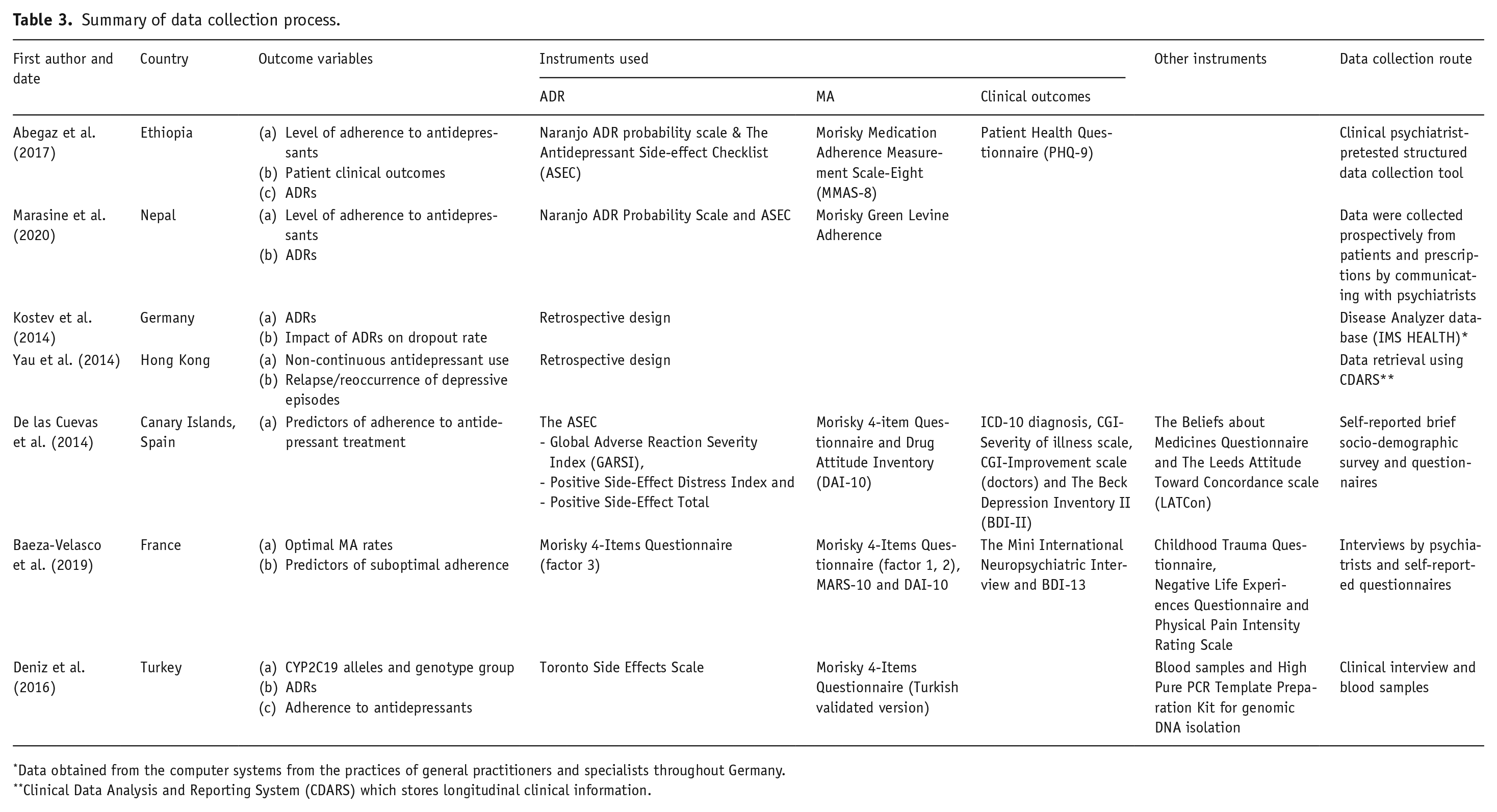
Data obtained from the computer systems from the practices of general practitioners and specialists throughout Germany.
Clinical Data Analysis and Reporting System (CDARS) which stores longitudinal clinical information.
Risk of bias for included studies
JBI critical appraisal tool for cross-sectional studies (Moola et al., 2020) was used to assess the quality of the studies. All the selected papers scored very high on the items and the risk of bias was low (See Table 4).
Risk of bias assessment.
Results of individual studies
Adverse drug reactions
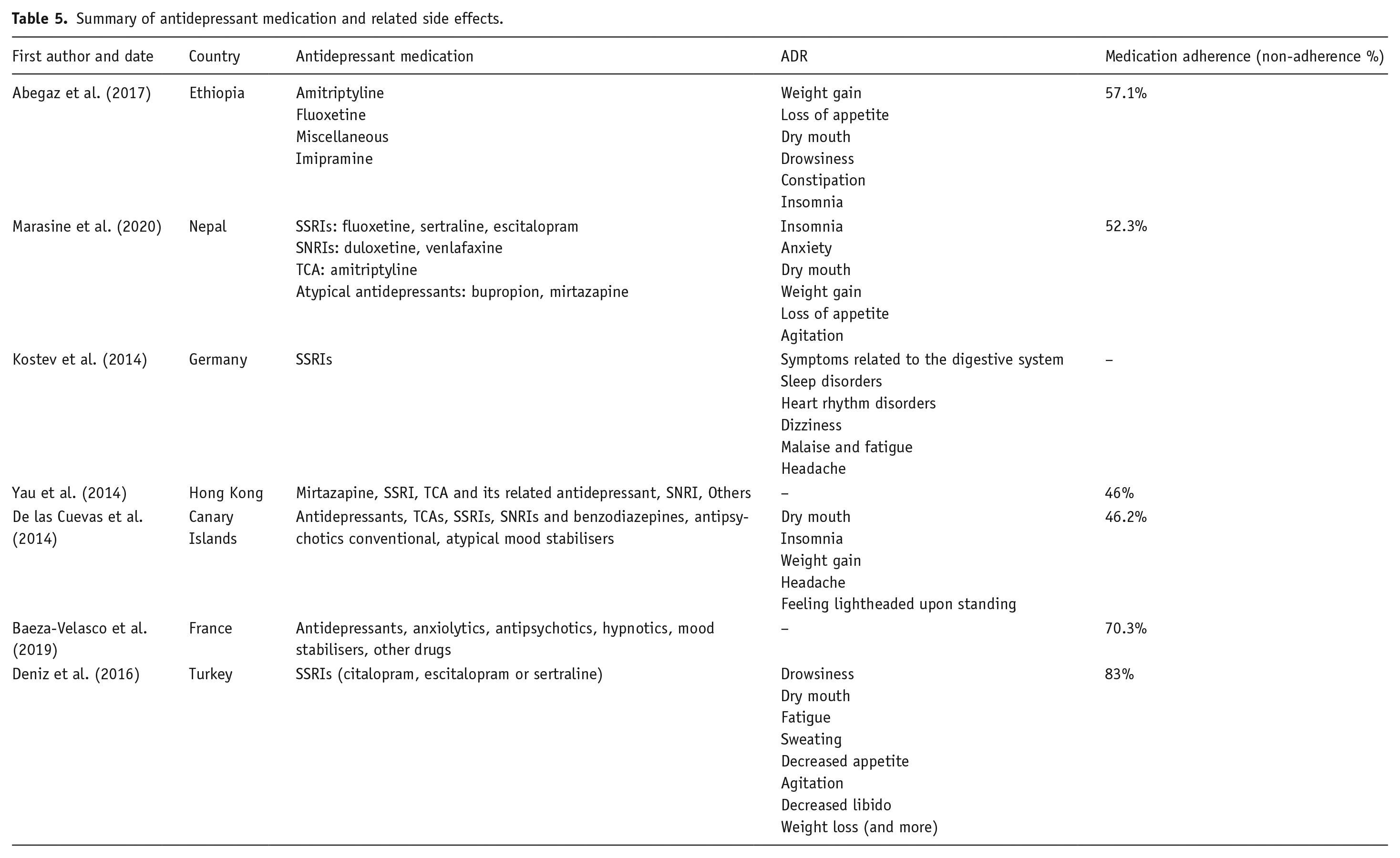
Five studies explored the different types of side effects in detail (Abegaz et al., 2017; De las Cuevas et al., 2014; Deniz et al., 2016; Kostev et al., 2014; Marasine et al., 2020). As Table 5 demonstrates, the most prevalent ADRs were similar to all the studies with slight differences in the hierarchy. Most of the studies had a variety of antidepressant medications being prescribed except for the studies of Kostev et al. in Germany and Deniz et al. in Turkey which explored solely SSRI prescriptions. It should also be noted that the German study did not report the total percentage of participants that encountered side effects. The other four studies reported the percentage of patients that experienced ADRs which was significantly high (over 50%). Additionally, the three studies that explored the severity of the ADRs reported a high prevalence of moderate severity side effects followed by severe ones (Abegaz et al., 2017; Marasine et al., 2020). Appetite dysregulation (weight gain, loss of appetite), sleep disorders (insomnia, drowsiness), dry mouth and headaches were some of the most common side effects. Drowsiness and dry mouth were found to be the ‘most troubling’ in the Turkish study by Deniz et al.
Summary of antidepressant medication and related side effects.
MA and the impact of antidepressant side effects
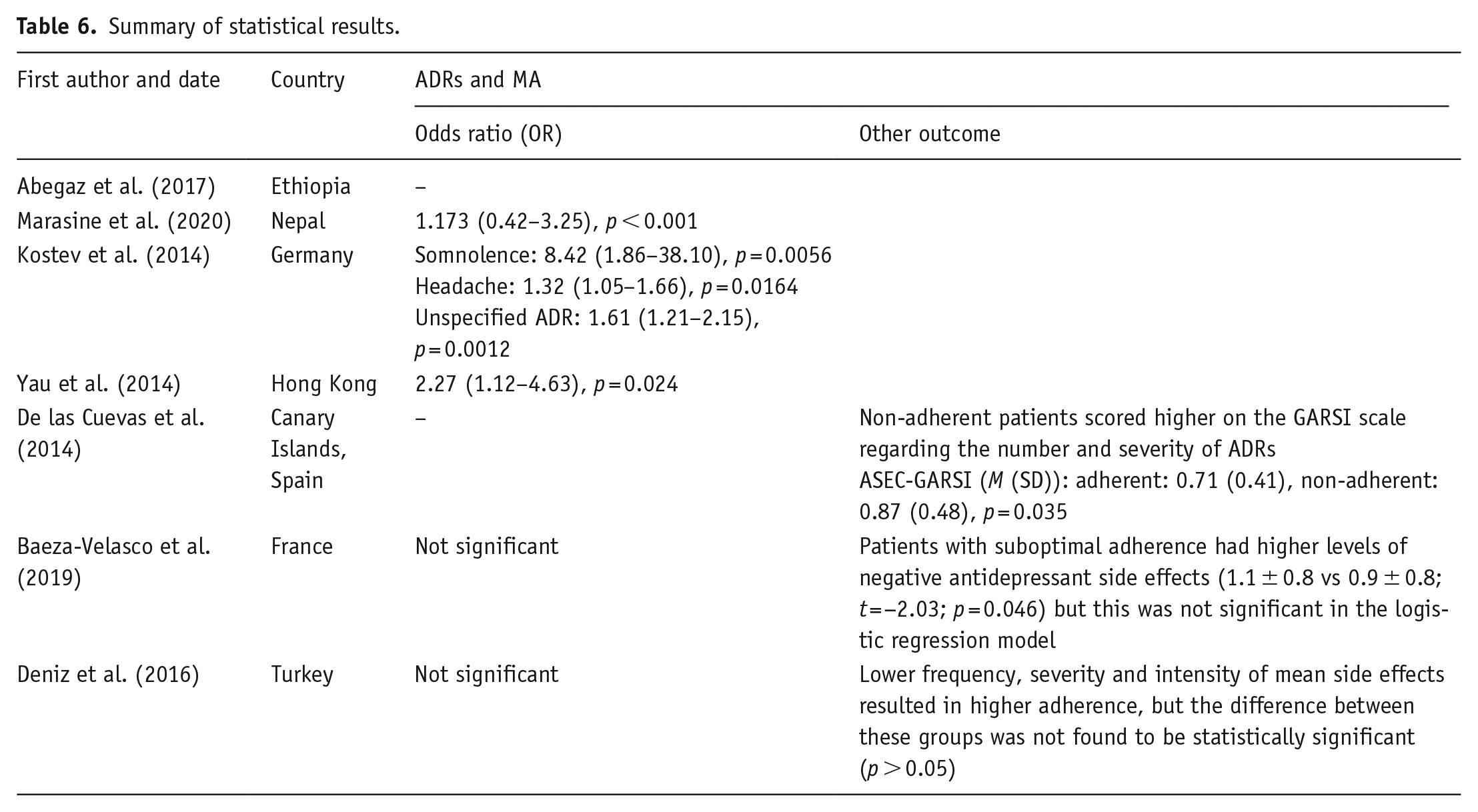
The results of the selected studies demonstrate that the levels of antidepressant non-adherence or low adherence among patients with depression are very high fluctuating from 46% to about 83% (see Table 5). Side effects while taking antidepressants appeared to be associated with the medication non-adherence levels in all studies, except for the study conducted in Ethiopia by Abegaz et al. (2017) where they explored these variables independently suggesting that future research should aim to establish their correlation. More specifically, three of the selected studies demonstrated that the presence of side effects increases the odds of the patients being less adherent to their antidepressant medication regimes (Kostev et al., 2014; Marasine et al., 2020; Yau et al., 2014). Kostev et al. (2014) also highlighted the impact that specific side effects have on the adherence level, with somnolence increasing the odds of the dropout rate 8.42 times. It should be noted that in this paper non-adherence was determined based on dropout rates and other indices of adherence (e.g. missed doses) were not reported. Moreover, in the study conducted in France in 2018 by Baeza-Velasco et al., patients with suboptimal levels of adherence had higher scores in the ‘Negative medication side effects’ questionnaire, yet the causal association was not found to be significant in the logistic regression model (Baeza-Velasco et al., 2019). Similarly, in the study conducted by Deniz et al., in 2016, more adherent participants were found to have lower scores in the frequency, severity and intensity of side effects; however, this was not found statistically significant. De las Cuevas et al. (2014) also found non-adherent patients to score higher in the ASEC-GARSI questionnaire measuring the number and severity level of the ADRs. However, a causal effect was not specifically explored (see Table 6).
Summary of statistical results.
Discussion
Medication adherence
One of the primary aims of this systematic review was to explore the levels of MA among patients diagnosed with depressive disorder. The results demonstrated high levels of non-adherence with most studies reporting that about one-half of the participants did not adhere to the medication regimes. This corroborates previous findings, suggesting that MA in antidepressants is a challenging situation that requires attention and effective interventions to reduce the risks embedded in the significant dropout rates (Ho et al., 2017; Marrero et al., 2020). It is well established that low levels of MA are linked with poor clinical outcomes and higher relapse in depressive disorder (Ho et al., 2017); therefore, this finding should not be overlooked. The selected studies’ samples suggest a diverse cultural and social background having been conducted in a variety of countries and continents, elucidating that despite the healthcare system differences, this is a shared challenge that needs to be faced effectively. However, some studies have illustrated cultural differences in the levels of compliance with antidepressants, showcasing that several population groups such as Latinos, African Americans and immigrants demonstrate lower adherence levels (Hung, 2014; Interian et al., 2013). The present study could not capture such differences and it is suggested that future systematic reviews should explore the influence of various racial backgrounds comprehensively to reinforce inclusive interventions that respect individual differences. Moreover, it is important to highlight that the selected studies were conducted in both outpatient and inpatient settings. Research has shown that the levels of adherence to outpatient treatment visits differ between patients that are hospitalised and patients in outpatient units. Specifically, it was found that hospitalised patients rarely attend such visits, even though they usually have a longer medical history of depression and higher severity of illness (Karpov et al., 2018). It would be interesting to explore if such differences apply to MA levels between these patient groups.
Adverse drug reactions
This study aimed to investigate the prevalence of antidepressant-related side effects. There was adequate homogeneity regarding the types of antidepressants that were prescribed in the selected studies, with most of the studies focusing on multiple pharmacological treatment options. The drawback of this broader methodological approach is that it is not possible to conclude about the different types of antidepressants and their specific side effects. However, the findings showed a variety of side effects. In the majority of the studies, a considerable number of participants reported experience of ADRs, usually of moderate severity. These findings are independently important because patients experiencing ADRs usually receive prescriptions for lower doses than the optimal titration dose, resulting in longer periods of treatment and prolonging of the disease. It is also understandable that even if the side effects do not result in dropping out of treatment, they jeopardise the patient’s quality of life (Kelly et al., 2008). Additionally, it is known that patients’ beliefs and fears about antidepressant medication influence the experience of side effects (Ho et al., 2017) but it can also be argued that the experience of ADRs can impact the perceptions about antidepressants, especially when side effects related to sexual dysfunction are experienced (Clayton et al., 2014). Therefore, it is important to acknowledge the subsequent negative psychological effects that several ADRs can have on patients who are already severely impacted by depression.
The effect of ADRs on MA
The findings among all selected studies confirmed the correlation between the presence of ADRs and suboptimal rates of adherence to antidepressant medication. Almost all studies that tested a potential causal effect using regression models found that ADRs increase the odds of patients presenting lower adherence levels. Only one study explored the relation of specific side effects with the levels of MA, highlighting that somnolence and headaches increase the dropout rates for SSRI treatment regimens (Kostev et al., 2014). This is supported by the findings of another study that explored the severity and intensity of the reported side effects, where somnolence was found to be amongst the most troubling (Deniz et al., 2016). These findings are of high importance because they highlight the need to develop interventions that target such side effects to mitigate the negative impact of non-adherence. Healthcare practitioners could provide educational information to patients before prescription in regard to the potential side effects that they might encounter and their characteristics (acute or persistent) (Kelly et al., 2008). In research conducted on the Chinese population about adherence to ART treatment for HIV, it was found that there is a mediating effect of self-efficacy in the impact that ADRs have on MA (Zhang et al., 2016). Patients with higher adherence self-efficacy were better at dealing with discomfort related to side effects and were more likely to follow the physician’s directions on taking the medication. It is demonstrated in Bandura’s Social Cognitive Theory (1998) that self-efficacy can enhance motivation and influence the effect and behaviour of individuals resulting in better health behaviours (Zhang et al., 2016). Future research should explore the potential mediation effect of self-efficacy on antidepressant medication adherence and the presence of ADRs. This could lead to the development of successful interventions that would facilitate the regulation of the discomfort caused by ADRs and reduce the dropout rates.
Limitations and modifications
This systematic review has several limitations. Firstly, grey literature (unpublished research articles) was not included in the search strategy resulting in a potential publication bias. Also, only English language articles were included limiting the breadth of the represented populations. However, studies from almost all continents were included. Secondly, the search strategy was limited to a selection of specific databases that the EBSCO database provided access to, although this did include Medline. Thirdly, the heterogeneity of the methodological approach and statistical analysis used in the selected studies should be taken into account in conjunction with the variety of instruments used to measure the outcome variables. Future systematic review studies could expand their searches in more databases and decide upon specific psychometric instruments in their review protocol. Furthermore, it is suggested that more efficient methods of monitoring side effects should be developed to account for polypharmacy and multimorbidity which is the reality of clinical practice.
Conclusion
The level of optimal MA is often overestimated by physicians, while the level of side effects experienced by the patients is underestimated (Kelly et al., 2008). Therefore, the present systematic review is of significant importance to the patients, elucidating the urgent need to develop effective interventions to facilitate adherence to antidepressants and enhance the communication between the patients and the doctors. This can benefit both the individuals and the healthcare system leading to better clinical outcomes and subsequent reduction of relapse-related costs.
Footnotes
Appendix 1
PICO framework.

| P | I | C | O |
|---|---|---|---|
| Patient, population or problem | Intervention or exposure | Comparison | Outcome(s) |
| Patients diagnosed with depressive disorder | Receiving antidepressant medication | Existence and severity of side effects | Levels of medication adherence |
Author’s note
The present review was not registered.
Dr L H Roberts is now affiliated to University West of England, Bristol, UK.
Bernard D. Naughton is now affiliated to Centre for Pharmaceutical Medicine Research, Kings College London.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.