
Abstract
Background:
Over the last two decades, a number of studies have highlighted the potential of psychedelic therapy. However, questions remain to what extend these results translate to naturalistic samples, and how contextual factors and the acute psychedelic experience relate to improvements in affective symptoms following psychedelic experiences outside labs/clinics. The present study sought to address this knowledge gap.
Aim:
Here, we aimed to investigate changes in anxiety and depression scores before versus after psychedelic experiences in naturalistic contexts, and how various pharmacological, extrapharmacological and experience factors related to outcomes.
Method:
Individuals who planned to undergo a psychedelic experience were enrolled in this online survey study. Depressive symptoms were assessed at baseline and 2 and 4 weeks post-psychedelic experience, with self-rated Quick Inventory of Depressive Symptomatology (QIDS-SR-16) as the primary outcome. To facilitate clinical translation, only participants with depressive symptoms at baseline were included. Sample sizes for the four time points were N = 302, N = 182, N = 155 and N = 109, respectively.
Results:
Relative to baseline, reductions in depressive symptoms were observed at 2 and 4 weeks. A medicinal motive, previous psychedelic use, drug dose and the type of acute psychedelic experience (i.e. specifically, having an emotional breakthrough) were all significantly associated with changes in self-rated QIDS-SR-16.
Conclusion:
These results lend support to therapeutic potential of psychedelics and highlight the influence of pharmacological and non-pharmacological factors in determining response. Mindful of a potential sample and attrition bias, further controlled and observational longitudinal studies are needed to test the replicability of these findings.
Introduction
Since the approval of the first selective serotonin reuptake inhibitors (SSRIs) in the 1980s, major breakthroughs in the treatment of depression have been relatively sparse. A decades-long hiatus on clinical trial research with psychedelic ended in 2006 (Moreno et al., 2006). Since then, supportive evidence for psychedelic-assisted therapy has begun to accrue promising results, particularly in the treatment of depressive and anxiety symptoms and disorders (Barbosa et al., 2016; Carhart-Harris et al., 2017, 2021a, 2021b; Davis et al., 2021a; Gasser et al., 2014; Griffiths et al., 2016; Grob et al., 2011; Moreno et al., 2006; Osório et al., 2015; Palhano-Fontes et al., 2019; Ross et al., 2016; Sanches et al., 2016). Notably, improvements in symptom severity have been observed several months after just one or two isolated doses of the drug (Carhart-Harris et al., 2017, 2021a; Davis et al., 2021a; Gasser et al., 2014; Griffiths et al., 2016; Grob et al., 2011). A number of randomised controlled trials have now been performed, with one direct SSRI comparator trial finding psychedelic therapy to compare very favourably in multiple domains (Carhart-Harris et al., 2021a). Population studies, indirectly examining the effects of psychedelic-use, have found lower suicide and mental disorders rates in ‘recent’ psychedelic users versus a matched sample (Hendricks et al., 2015; Johansen and Krebs, 2015; Simonsson et al., 2021).
Psychedelic therapy is generally conceived of as a combination therapy, requiring both the pharmacological action of the drug and adjunctive psychological and environmental support (Carhart-Harris et al., 2018). Contextual (Carhart-Harris et al., 2018) or extrapharmacological (Hartogsohn, 2017) variables impinging on psychedelic experiences were referred to as ‘set’ and ‘setting’ in the early 1960s (Hyde, 1960; Leary et al., 1963), where ‘set’ refers to any prior psychological states and traits – plus expectations, and ‘setting’ refers to the external environmental context (Leary et al., 1963). Set and setting variables have been shown to influence both acute (Aday et al., 2021; Leary et al., 1963; Metzner et al., 1965; Sepeda et al., 2020; Studerus et al., 2012) and subsequent longer-term outcomes linked to psychedelic use (Agin-Liebes et al., 2021; Davis et al., 2021a; Garcia-Romeu et al., 2015; Griffiths et al., 2018; Haijen et al., 2018; MacLean et al., 2011; Palhano-Fontes et al., 2019; Roseman et al., 2018; Sepeda et al., 2020; Williams et al., 2021).
Specific predictive factors that can be regarded and qualifying as ‘set’ under a liberal definition of the construct – as an individual’s ‘prior psychology’ going into a psychedelic experience – include trait absorption (Aday et al., 2021; Haijen et al., 2018), psychopathology (Studerus et al., 2012), openness (Aday et al., 2021) and attachment style (Stauffer et al., 2021). Extending the definition even further to include demographic factors, age (Aday et al., 2021; Studerus et al., 2012), gender (Studerus et al., 2012) and previous psychedelic experience (Kettner et al., 2019; Studerus et al., 2012) could be included. Predictive ‘state’ factors include intention (Haijen et al., 2018), readiness for psychological surrender (Aday et al., 2021; Davis et al., 2021a; Haijen et al., 2018), pre-occupation (Aday et al., 2021; Davis et al., 2021a; Russ et al., 2019), anxiety (Haijen et al., 2018), a sense of trust (Haijen et al., 2018) and rapport with those present (Kettner et al., 2021; Murphy et al., 2022), as well as apprehensive and confused psychological states (Aday et al., 2021).
As expected, drug dosage is positively correlated with effects intensity (Griffiths et al., 2011; Hasler et al., 2004; Studerus et al., 2012), with some suggestions on an upper threshold or ‘ceiling’ in terms of ‘mystical-type experiences’ in healthy volunteers (Griffiths et al., 2011). Predictive ‘setting’ factors include the existence of music (Kaelen et al., 2015), other people (Kettner et al., 2021), non-defined ‘distractions’ (Haijen et al., 2018), whether the psychedelic is taken in a structured and supportive environment (Sepeda et al., 2020) and whether it is taken in a neuroimaging setting (Studerus et al., 2012). It is logical that the influence of setting factors depends much on how they are related to, creating overlap in this regard between set and setting, which may justify them being referred to more generally as ‘contextual’ (Carhart-Harris et al., 2018) or ‘relational’ variables (Hayes, 2019).
An important principle of a context-dependent or relational approach to psychedelics is that the psychedelic experience itself is an important mediator of subsequent therapeutic outcomes – and there is much evidence to support this (Carbonaro et al., 2016; Carhart-Harris et al., 2016b; Davis et al., 2019, 2020, 2021b; Garcia-Romeu et al., 2015; Gasser et al., 2015; Griffiths et al., 2016, 2018; MacLean et al., 2011; Passie, 1997; Roseman et al., 2018; Ross et al., 2016; Schmid and Liechti, 2017). Specifically, a number of studies have found that ‘peak’ or ‘mystical’ – type experiences, which feature feelings of unity, transcendence of time, space and self, and positive mood, are predictive of subsequent positive therapeutic outcomes (Bogenschutz et al., 2015; Davis et al., 2019; Garcia-Romeu et al., 2015; Griffiths et al., 2016; Murphy et al., 2022; Pahnke, 1963; Roseman et al., 2018; Ross et al., 2016). Another salient dimension of the psychedelic experiences is the challenging experience (CE), which includes feelings of paranoia, anxiety, insanity and grief (Johnson et al., 2008). High ratings for CE have been associated with both worsened (Barrett et al., 2016; Carbonaro et al., 2016; Haijen et al., 2018; Roseman et al., 2018) and improved long-term mental health outcomes (Carbonaro et al., 2016; Davis et al., 2021b). These contradictory findings are likely explainable by whether a period of psychological challenge results in a psychological insightful therapeutic breakthrough or not (Barrett et al., 2016; Carbonaro et al., 2016; Davis et al., 2020; Roseman et al., 2018; Watts et al., 2017).
The emotional breakthrough inventory (EBI) was devised to address this important qualification, and it has been found to add an important third component to predictive models that assess acute mediators of long-term outcomes linked to psychedelic use (Roseman et al., 2019). Having an emotional breakthrough is often accompanied by personal and interpersonal psychological insights (Roseman et al., 2019). Psychological insight is a well-known facet of the psychedelic experience and a common goal of the therapeutic process towards healing (Williams et al., 2021). Recently, studies show how personal insights during a psychedelic experience are associated with positive therapeutic outcomes in relation to depression and anxiety (Davis et al., 2020), racial trauma (Williams et al., 2021) and alcohol abuse (Garcia-Romeu et al., 2019) and that psychological flexibility seem to mediate effects (Davis et al., 2020; Williams et al., 2021). More recent work has found that psychological insight assessed soon after a psychedelic experience (using the brief ‘psychological insight scale (PIS)’) mediates the relationship between emotional breakthrough and improved mental health (Peill et al., 2022).
Some of the present authors recently published on the merits of pragmatic trials, real-world evidence and novel (e.g. digital and naturalistic) approaches to data collection on psychedelic use (Carhart-Harris et al., 2021b). The obvious advantage of well-controlled research is the strength of inferences that can be drawn from high-quality data, but the strength of more explorative research study designs is the superior depth, richness and ecological validity of the data they can yield.
Few naturalistic studies have investigated changes in major psychiatric symptom domains such as depression and anxiety before versus after a psychedelic experience in a prospective fashion. The primary aim of this study was to examine changes in anxiety and depression 2 and 4 weeks after a self-initiated psychedelic experience, and to investigate whether dosage, motive for use, prior psychedelic experience and the quality of the acute psychedelic experience would be predictive of therapeutic outcomes. Specifically, we hypothesised that having an emotional breakthrough and a ‘mystical type’ experience would be positively related to subsequent therapeutic improvements. We use prospective (i.e. before vs after) digital data collection via an online website ‘psychedelicsurvey.com’. Depressive symptoms served as the primary outcome and were assessed with the self-rated Quick Inventory of Depressive Symptomatology (QIDS-SR-16).
Methods
Study procedure
The present naturalistic observational study used online data collection in a prospective fashion via the website Psychedelic Survey (https://www.psychedelicsurvey.com). Inclusion criteria for participants were: (1) at least 18 years old, (2) good comprehension of the English language and (3) planning to take a psychedelic drug (psilocybin/magic mushrooms/truffles, LSD/1P-LSD, ayahuasca, DMT/5-MeO-DMT, salvia divinorum, mescaline or iboga/ibogaine) in the near future. Based on the a priori research questions of most interest, the present analyses used data from four of the five surveys conducted. The following time points were included: (1) 1 week prior to the planned psychedelic experience (baseline), (2) 1 day post-experience, (3) 2 weeks post-experience and (4) 4 weeks post-experience. For a full overview of the study design, see Haijen et al. (2018).
Dissemination of the survey and participant recruitment
Participants were recruited to the survey through online advertisement posted on Facebook groups, Twitter pages, email newsletters and online drug forums. At the recruitment website, participants were informed about the study and reassured about the anonymity of their responses and that they could withdraw from the study at any time. Participants gave informed consent via button press at the end of an information page and were invited to sign up on the website. Individuals were asked to provide their email address and the date on which they expected to have their psychedelic experience. An emailing system was programmed to send out emails with links to the online survey at the different time points according to the date of the psychedelic experience. All participants were given a unique identification number (ID) that made it possible to identify and link multiple survey responses of one individual, while protecting anonymity.
Measures
Outcome measures
The primary outcome was change in severity of depressive symptoms measured by the QIDS-SR-16 henceforth abridged to just the ‘Quick Inventory of Depressive Symptomatology (QIDS)’ (Rush et al., 2003) from baseline to 2 and 4 weeks after a self-initiated psychedelic experience – ‘post-experience’. The QIDS measures depressive symptoms by 16 items assessed on a 4-point Likert-scale with a maximum score of 27 points. The inventory is widely used and has shown acceptable psychometric properties and high validity (Rush et al., 2003). Using established cut-off values (Reilly et al., 2015), QIDS scores were used to divide participants into separate four groups with regard to presence/severity of depression: 0–5 (none), 6–10 (mild), 11–15 (moderate) and 16–27 (severe/very severe). In the present study, we excluded participants with no depressive symptoms (QIDS < 6) at baseline, thereby generating a study sample of participants with mild-to-severe symptoms at baseline (N = 302). This was done to aid translation to populations of individuals with depressive symptoms.
Internal consistency reliability was excellent (‘baseline’ measure: Cronbach’s alpha = 0.982; ‘2-week follow-up’ measure: Cronbach’s alpha = 0.994; ‘4-week follow-up’ measure: Cronbach’s alpha = 0.995). The main secondary outcome was Trait Anxiety measured using a short form of the Spielberger State-Trait Anxiety Inventory (STAI-T), which includes six items asking how one feels ‘in general’ (Marteau and Bekker, 1992). The measurement is derived from the widely used 20-item Spielberger State-Trait Anxiety Inventory (STAI) and has shown to possess satisfactory concurrent validity (Marteau and Bekker, 1992). The possible range of scores on the STAI-T is 20–80. A score of 40+ is used as a cut-off for clinical anxiety in the state version of the STAI. Internal consistency reliability was excellent (‘baseline’ measure: Cronbach’s alpha = 0.921; ‘2-week follow-up’ measure: Cronbach’s alpha = 0.971; ‘4-week follow-up’ measure: Cronbach’s alpha = 0.973).
Covariates
At baseline, participants were asked to provide demographic information regarding their: age, gender, education, nationality and psychiatric history. Participants were also asked about their previous psychedelic drug use with the following options: ‘Never’, ‘Only once’, ‘2–5 times’, ‘6–10 times’, ‘11–20 times’, ‘21–50 times’, ‘51–100 times’ and ‘More than 100 times’, and what their motives or intentions were for the experience with the options: fun/recreational/party, therapeutic/personal growth, medicinal, spiritual experience, religious experience, curiosity, social, connection with nature, to escape from difficult emotions and to confront difficult emotions. Participants rated each motive on a 4-point scale from ‘not at all’, ‘somewhat’, ‘moderately’ to ‘very much’. We chose only to investigate Medicinal Motive as a predictor of therapeutic outcome as this was most relevant in the present study for investigating clinical outcomes of a psychedelic experience.
One day after the experience, participants were asked what type of psychedelic they took. Options included: LSD/1P-LSD, psilocybin, ayahuasca, DMT/5-MeO-DMT, mescaline (Peyote, San Pedro), iboga/ibogaine or other. Drug doses were reported in LSD equivalents and defined as: low dose = no more than 0.5 tab/50 μg of LSD, a moderate dose = no more than 1 tab/100 μg of LSD, a high dose = no more than 2 tabs/200 μg of LSD, a very high dose = no more than 3 tabs/300 μg of LSD and an extremely high dose = more than 3 tabs/300 μg of LSD. Furthermore, participants completed measures of the acute psychedelic experience: Mystical Experience Questionnaire (MEQ), Challenging Experience Questionnaire (CEQ) and Emotional Breakthrough Inventory (EBI). The MEQ was used to measure mystical type experiences and consists of 30 items covering four subscales (mystical, positive mood, transcendence of time and space, and ineffability), rated on a 6-point Likert-scale from 0 = ‘not at all’ to 5 = ‘extreme (more than any other time in my life and stronger than 4)’ (Barrett et al., 2015). For this study, we used a total scale mean score and internal consistency reliability was good (Cronbach’s alpha = 0.846). The CEQ consists of 26 items measuring seven subscales (fear, grief, physical distress, insanity, isolation, death and paranoia) relating to CEs during the acute psychedelic experience, rated on a 6-point Likert-scale from 0 = ‘not at all’ to 5 = ‘extreme’ (more than any other time in my life and stronger than 4) (Barrett et al., 2016). For this study, we used a total scale mean score and internal consistency reliability was good (Cronbach’s alpha = 0.835). The EBI consists of six items rated on a visual analogue scale (0–100) with zero defined as ‘no, not more than usually’ and 100 defined as ‘Yes, entirely or completely’, measuring the overcoming of challenging emotions and experience of an emotional breakthrough (Roseman et al., 2019). Internal consistency reliability for the EBI was good (Cronbach’s alpha = 0.875).
Aspects of the setting of the psychedelic experience were assessed in the third survey, using the following items: ‘Did your experience take place within a psychedelic drug retreat?’, ‘Was the setting designed and/or prepared with a therapeutic objective in mind?’ and ‘Was the setting more designed and/or suited for a recreational and/or social occasion, such as a party?’, which were all answered with either yes or no. Furthermore, the question was asked – how many people were present during the majority of the experience? Options included: ‘1 (only myself)’, ‘between 2 and 5’, ‘between 6 and 15’, ‘between 16 and 30’, ‘between 31 and 100’ and ‘more than 100’. In addition, it was asked whether individuals were present who took responsibility for the welfare of the participant during the psychedelic experience, which was answered with either ‘yes’ or ‘no’.
Statistical analysis
Statistical analyses were performed using the ‘Stata 15’ statistical package. Initially, descriptive and explorative analyses were conducted to examine marginal changes over time in QIDS and STAI-T and to investigate the correlation between QIDS and STAI-T scores at baseline and change scores. Explorative analysis using spearman correlations was done to assess the bivariate associations between predictor variables and QIDS and STAI-T, respectively. In the first analysis, we examined changes in QIDS and STAI-T 2 and 4 weeks after the psychedelic experience.
Linear mixed modelling (LMM) was used for its ability to handle missing data. LMM can include multiple covariates and analyse repeated measurements with unequal observations at the follow-ups using all existing data. LMM analyses were performed with either QIDS or STAI-T included as the dependent variable. Based on previous work, age (Hübner et al., 2020), gender (Kettner et al., 2021) and education (Hübner et al., 2020) were included as covariates to control for potential confounding effects on depression and anxiety scores.
Each of the models additionally contained time as a repeated effect, with an unstructured covariance design, and a random intercept to explain within-subject variance. As a function of the coefficient (B) from the LMM, predictive margins were calculated using the ‘margins’ command in Stata, which calculates average adjusted changes in QIDS and STAI-T from baseline to follow-ups and the average estimated changes on QIDS within severity of depressive symptoms at baseline as a covariate. Estimated mean QIDS and STAI-T scores are reported as ‘M’ and estimated changes in QIDS and STAI-T scores between timepoints are reported as ‘M-change’.
Since QIDS and STAI-T were significantly correlated, we used the QIDS as primary therapeutic outcome for further analysis. To investigate how QIDS changes within severity of baseline depressive symptoms, we first analysed changes in QIDS stratified on baseline QIDS scores. This model included time as a repeated effect and a fixed part: baseline QIDS score as main effect, the interaction effect with time, the above-mentioned confounder variables and a random intercept.
A weighted effect size (Cohen’s d) was calculated using the estimated changes in QIDS and STAI-T (M-change) divided by baseline standard deviation.
In the second part of the analysis, we investigated predictors of changes in QIDS scores. Based on the previous work, drug dose (Griffiths et al., 2011; Hasler et al., 2004; Studerus et al., 2012), motive (Haijen et al., 2018) and previous psychedelic experience (Kettner et al., 2019; Studerus et al., 2012) were included as potential predictor variables.
The LMM included QIDS as the dependent variable, time as a repeated effect and a fixed part: predictor variables of interest as main effects; drug dose, having a medicinal motive and number of previous psychedelic experiences, their interaction effects with time and a random intercept. The model was controlled for potential confounders; age, gender, education and baseline QIDS scores. To investigate the effects of the acute psychedelic experience on changes in QIDS, another LMM was fitted that included QIDS as the dependent variable, time as a repeated effect and a fixed part: MEQ, CEQ and EBI as main effects, their interaction effects with time and a random intercept. The model was controlled for potential confounders: gender, age and education. Due to a collinearity between the MEQ and EBI (r > 0.50, p < 0.001), two secondary models were run: one in which the MEQ was excluded and one in which the EBI was excluded from the analysis.
To show the effect of predictor variables, a standardised regression coefficient was calculated by multiplying the coefficient (B) by the ratio of the standard deviation of the independent variable and the dependant variable.
Results
Sample characteristics
Sample sizes for the four time points were N1 = 302, N2 = 182, N3 = 155 and N4 = 109, respectively.
Table 1 shows demographic information collected at baseline including age, gender, education, nationality, psychiatric history, previous use of psychedelics, medicinal motive and baseline symptoms of depression and anxiety, respectively. Mean age was 27.4 ± 10.1 years. Most participants were from the United States or the United Kingdom. The sample was majority male (70.9%), and most participants had completed an undergraduate university degree or higher (74.2%).
Characteristics of participants with mild-to-severe depressive symptoms at baseline (n = 302).
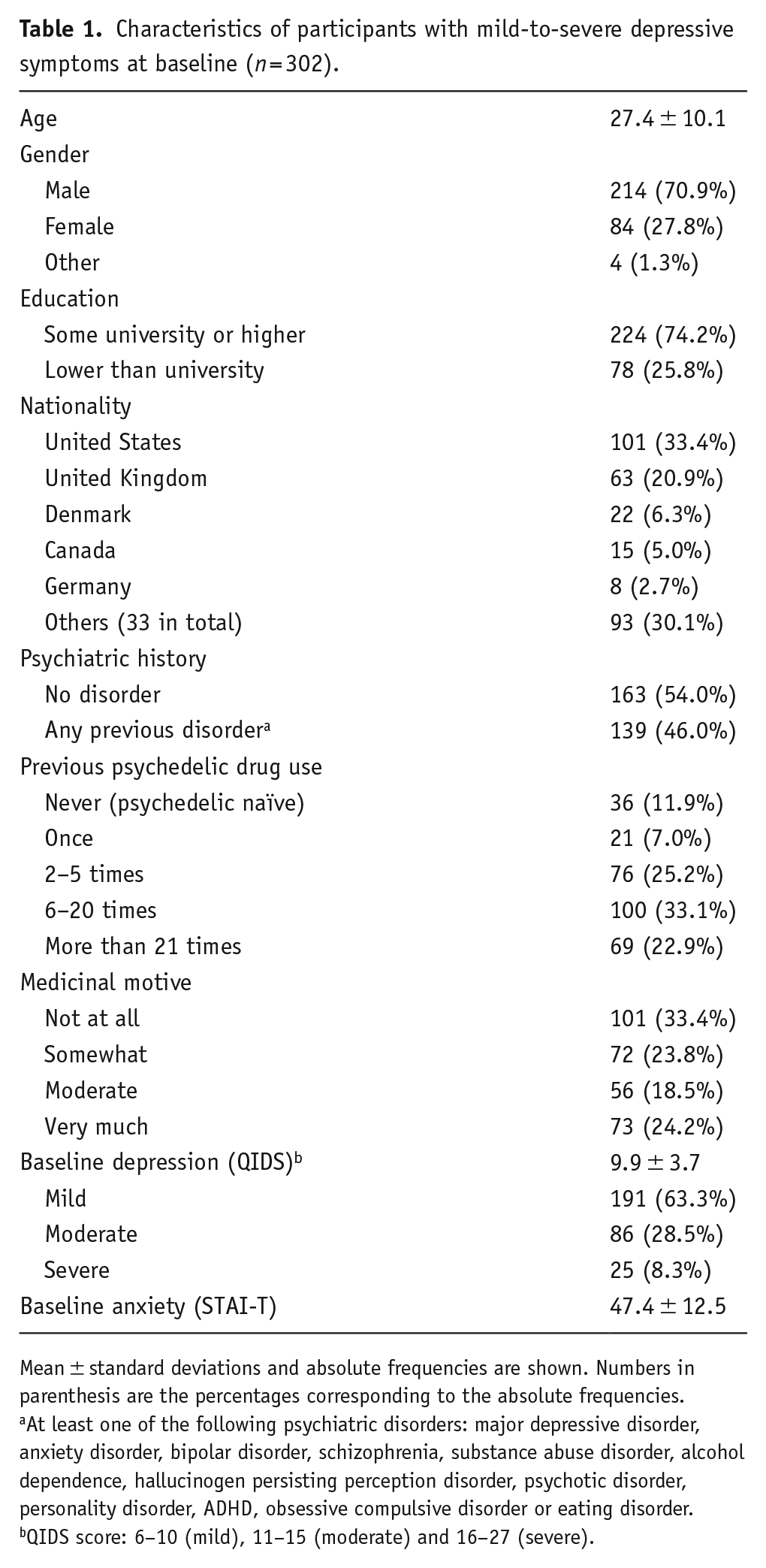
Mean ± standard deviations and absolute frequencies are shown. Numbers in parenthesis are the percentages corresponding to the absolute frequencies.
At least one of the following psychiatric disorders: major depressive disorder, anxiety disorder, bipolar disorder, schizophrenia, substance abuse disorder, alcohol dependence, hallucinogen persisting perception disorder, psychotic disorder, personality disorder, ADHD, obsessive compulsive disorder or eating disorder.
QIDS score: 6–10 (mild), 11–15 (moderate) and 16–27 (severe).
Forty-six percent reported being previously diagnosed with a mental illness. At baseline, mean QIDS scores were 9.9 (6–10 = mild depression, 11–15 = moderate) ± 3.7, and mean STAI-T scores were 47.4 ± 12.5. The samples were relatively experienced with psychedelics, with 80% reporting having tried psychedelics more than once. Around 42.7% rated that they had a moderate or strong medicinal motive for the psychedelic experience. Table 2 shows data from time point 2 (1 day after the experience) including information on psychedelic drug type and drug dose and setting. LSD and psilocybin were the main drugs used with a majority of participants taking a moderate-to-high dose. More than half of the participants reported taking psychedelics in a therapeutic setting, with the remainder taking the psychedelic in a recreational/social setting or in another setting. The majority took psychedelics with others and guidance (39%), one-third took the psychedelic with others but without guidance and one-third were entirely alone for their experience.
Information about drug type, drug dose and setting collected 1 day after the experience (n = 182).
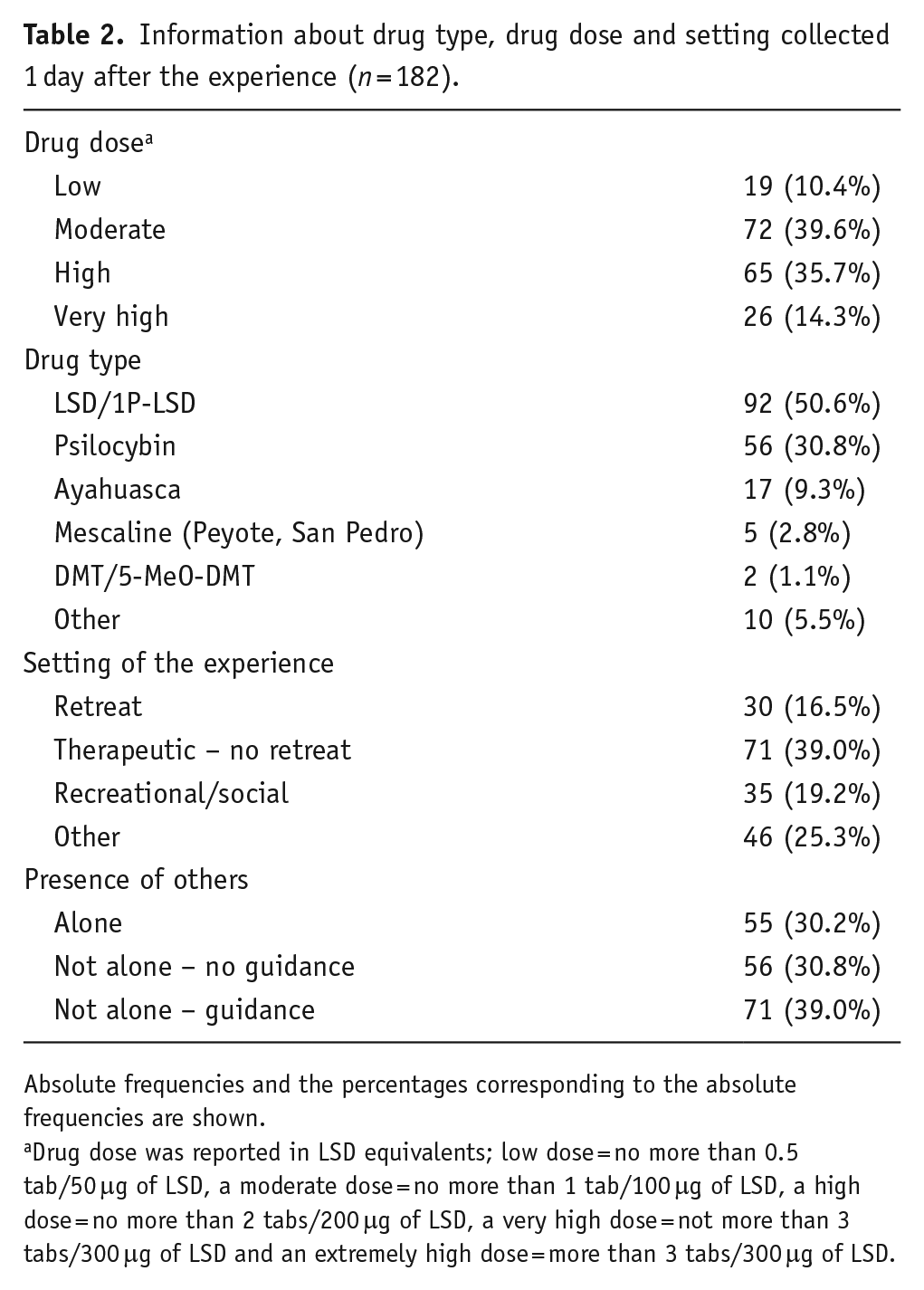
Absolute frequencies and the percentages corresponding to the absolute frequencies are shown.
Drug dose was reported in LSD equivalents; low dose = no more than 0.5 tab/50 μg of LSD, a moderate dose = no more than 1 tab/100 μg of LSD, a high dose = no more than 2 tabs/200 μg of LSD, a very high dose = not more than 3 tabs/300 μg of LSD and an extremely high dose = more than 3 tabs/300 μg of LSD.
Predictors of attrition in the full study sample were found among demographic variables, including age and educational level, as well as personality traits. Specifically, low conscientiousness and high extraversion were the strongest predictors of drop-out (β = −0.079, p = 0.024) and (β = 0.082, p = 0.012), respectively. Neither the quality of the acute experience nor psychedelic-induced long-term psychological changes predicted study attrition, see Hübner et al. (2020), for a thorough coverage of this matter.
Mean changes in self-reported clinical symptoms
Table 3 and Figure 1 shows predicted margins of changes in self-reported clinical symptoms (QIDS and STAI-T) at 2 and 4 weeks post-experience (see Table 7 in Supplemental Appendix for main effects of time and covariates). QIDS scores were significantly reduced from baseline to 2 weeks post-experience (M-change = −4.37, SE = 0.32, p < 0.001, Cohen’s d = 1.18, Table 3), with no further change from 2 to 4 weeks post-experience (M-change = 0.19, SE = 0.34, p = 0.567, Cohen’s d = 0.06, Table 3). From baseline to 4 weeks post-experience QIDS scores reduced significantly (M-change = −4.17, SE = 0.37, p < 0.001, Cohen’s d = 1.13, Table 3). Likewise, STAI-T scores were significantly reduced from baseline to 2 weeks post-experience (M-change = −6.17, SE = 0.90, p < 0.001, Cohen’s d = 0.49, Table 3), with no further significant changes from 2 to 4 weeks post-experience (M-change = 0.84, SE = 0.92, p = 0.364, Cohen’s d = 0.08, Table 3). From baseline to 4 weeks post-experience, STAI-T scores decreased significantly (M-change = −5.33, SE = 1.05, p < 0.001, Cohen’s d = 0.43, Table 3).
Predictive marginal mean changes in QIDS and STAI-T from baseline to 2 and 4 weeks, respectively.
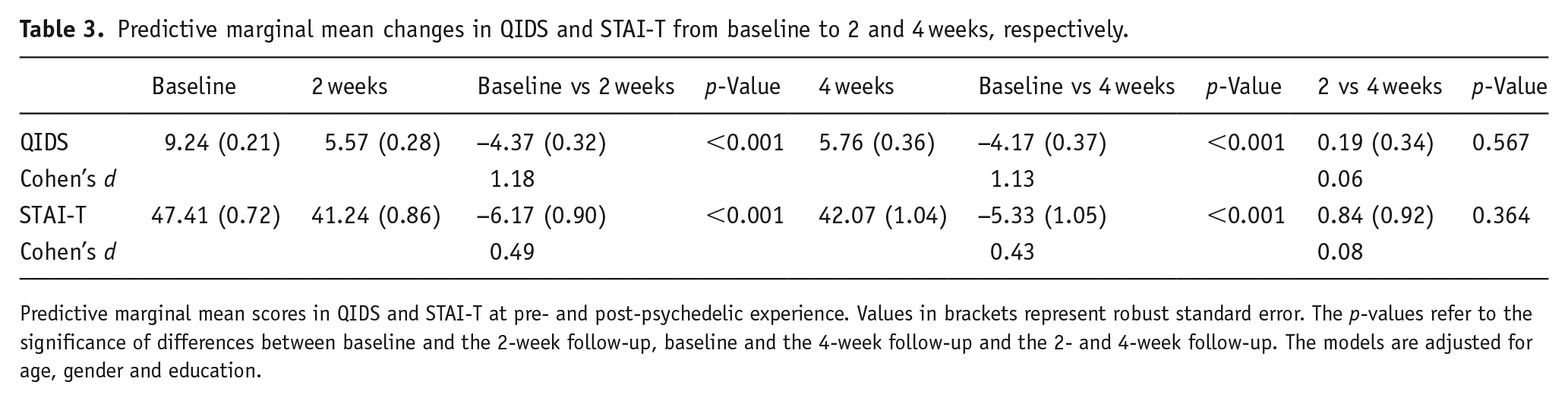
Predictive marginal mean scores in QIDS and STAI-T at pre- and post-psychedelic experience. Values in brackets represent robust standard error. The p-values refer to the significance of differences between baseline and the 2-week follow-up, baseline and the 4-week follow-up and the 2- and 4-week follow-up. The models are adjusted for age, gender and education.
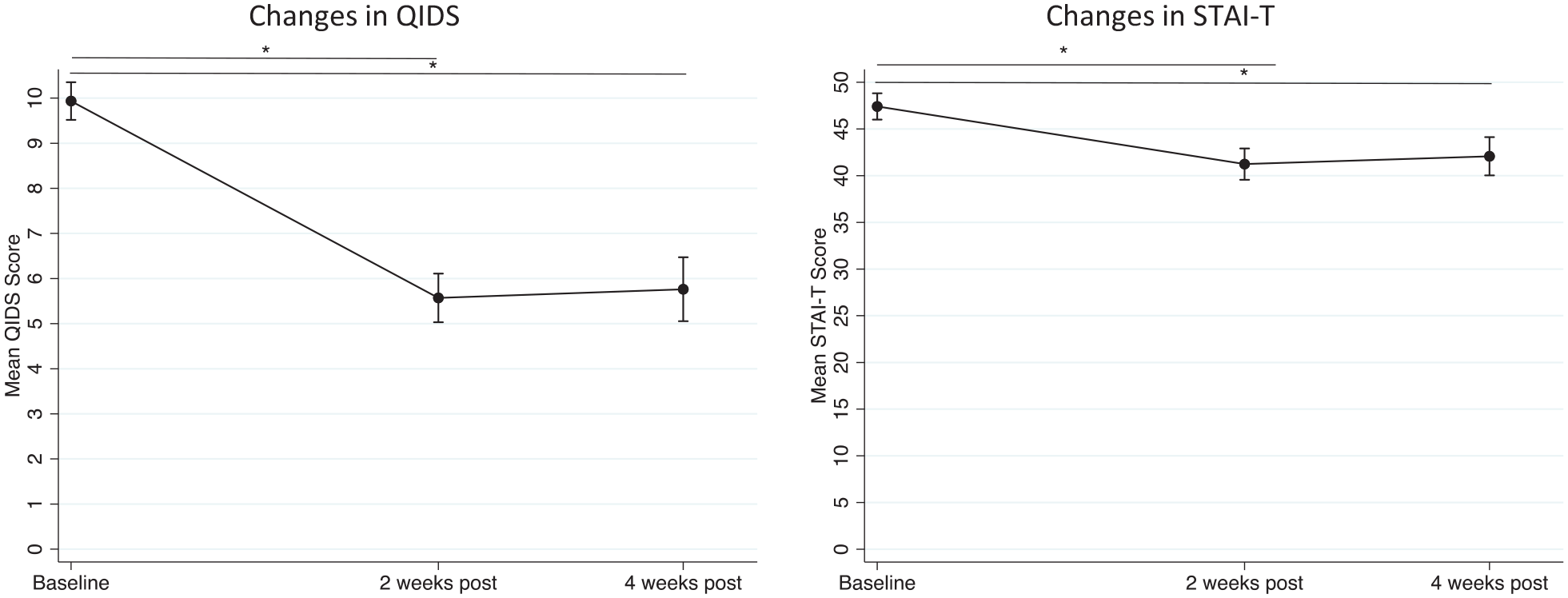
Changes in depressive symptoms (QIDS) and anxiety (STAI-T). Scores at baseline, that is, 1 week before the psychedelic experience, and at 2 and 4 weeks after the experience. Error bars represent mean ± 95% CI. The models are adjusted for age, gender and education. *p ⩽ 0.05.
Table 4 shows changes in QIDS stratified by baseline QIDS scores grouped according to severity of depressive symptoms (see Table 8 in Supplemental Appendix for main effects of time and effect estimate of the interaction between baseline QIDS score and time (2 and 4 weeks post-psychedelic experience)). All groups exhibited significant reductions in QIDS scores from baseline to 2 weeks post-experience with little or no significant changes from 2 to 4 weeks post-experience. Most significantly, participants with moderate and severe depressive symptoms at baseline decreased to a level of mild depressive symptoms at 2 weeks (i.e. a decrease to M = 6.97 (0.62), p < 0.001 from moderate symptoms at baseline (Cohen’s d = 1.52) and a decrease to M = 6.34 (1.00), p < 0.001 from severe symptoms at baseline (Cohen’s d = 3.28), Table 4). Although not significant, there was an increase in QIDS scores from 2- to 4-week follow-up in the participants with severe depressive symptoms at baseline (M-change = 2.19 (1.32), p = 0.096, Cohen’s d = 0.73, Table 4), indicating a tendency for recurrence of symptoms at the 1-month timepoint. Cohen’s d analysis of QIDS changes and associated effect sizes was conducted in a sub-sample of participants with moderate-to-severe depressive symptoms at baseline: N = 111 at baseline, N = 81 at 2 weeks and N = 56 at 4 weeks. Effect sizes were especially large at 2 weeks (Cohen’s d = 2.4) and 4 weeks (Cohen’s d = 2.1).
Changes in QIDS score by severity of baseline depressive symptoms (baseline QIDS score a ).
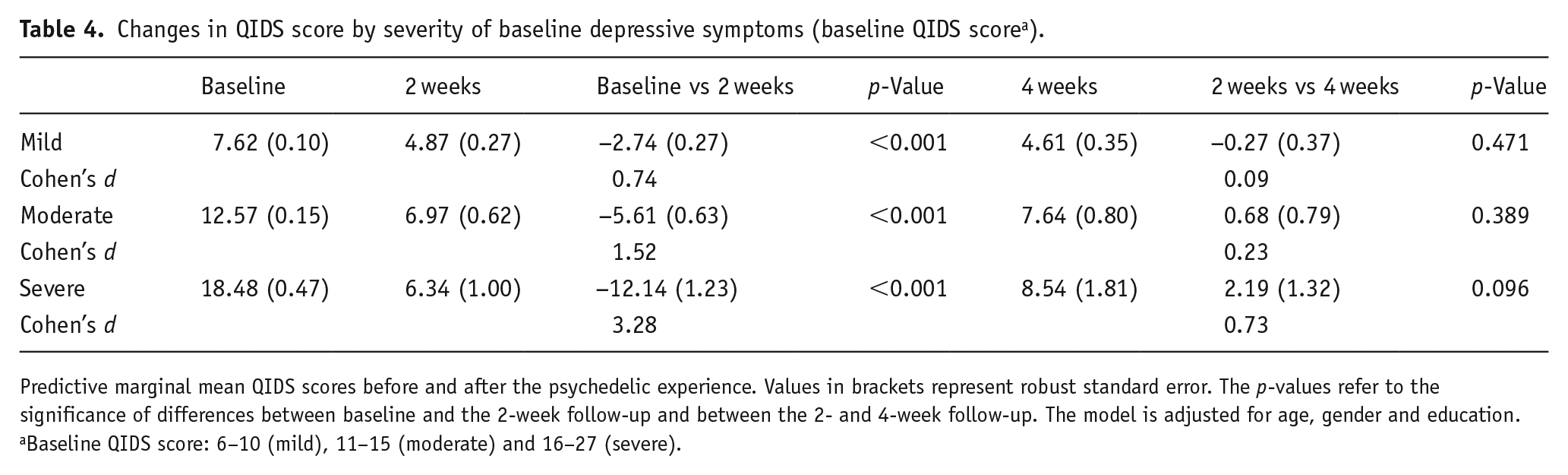
Predictive marginal mean QIDS scores before and after the psychedelic experience. Values in brackets represent robust standard error. The p-values refer to the significance of differences between baseline and the 2-week follow-up and between the 2- and 4-week follow-up. The model is adjusted for age, gender and education.
Baseline QIDS score: 6–10 (mild), 11–15 (moderate) and 16–27 (severe).
Clinical predictors of changes in depressive symptoms
In the second analysis, we investigated predictors of changes in QIDS scores from baseline to 2 weeks post-experience. The 4-week follow-up was not assessed given that no significant changes in QIDS were observed between 2 and 4 weeks in these groups (see Table 4). Results from the LMM analysis of clinically relevant predictor variables, that is, previous psychedelic use, medicinal motive and drug dose are shown in Table 5. Across the sample, having a medicinal motive had the strongest effect on changes in depressive symptoms reflected by a significant interaction between time and ratings of medicinal motive (B = −0.991, β = 0.316, p = 0.002), meaning that being more medicinally motivated was associated with larger decreases in depressive symptoms. In addition, higher drug doses were found to be associated with larger decreases in depressive symptoms (B = −0.824, β = 0.196, p = 0.029). Previous psychedelic use was associated with changes in symptoms in the opposite direction (B = 0.508, β = 0.213, p = 0.033), meaning that more lifetime experience with psychedelics was associated with smaller decreases in depressive symptoms. These predictive models were corrected for age, gender, education and baseline QIDS scores.
Previous psychedelic use, medicinal motive and drug dose predicting changes in QIDS.
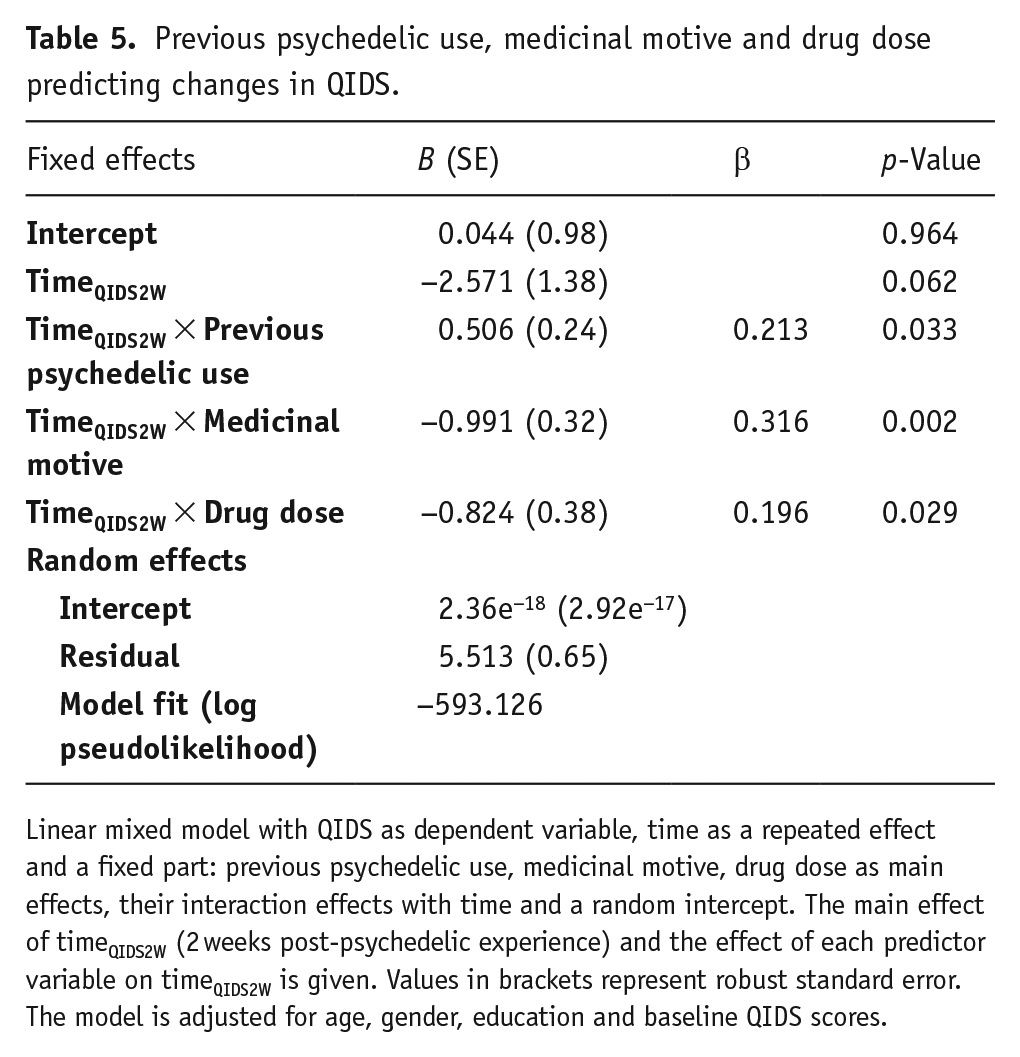
Linear mixed model with QIDS as dependent variable, time as a repeated effect and a fixed part: previous psychedelic use, medicinal motive, drug dose as main effects, their interaction effects with time and a random intercept. The main effect of timeQIDS2W (2 weeks post-psychedelic experience) and the effect of each predictor variable on timeQIDS2W is given. Values in brackets represent robust standard error. The model is adjusted for age, gender, education and baseline QIDS scores.
Acute psychedelic measures mediating changes in depressive symptoms
Another model was run to investigate measures of the acute experience as predictors of change in QIDS from baseline to 2 weeks post-experience in a subsample of participants with mild-to-severe depressive symptoms. Result from the LMM including acute experience measures of emotional breakthrough (EBI), challenging (CEQ) and mystical-type (MEQ) experiences are reported in Table 6. Across the sample, only the EBI significantly predicted changes in QIDS from baseline to 2 weeks after the experience, reflected by a significant interaction between EBI scores and time (B = −0.024 (0.01), β = −0.201, p = 0.039). This interaction was not significant in the model including MEQ, which can be explained by the multicollinearity between the EBI and the MEQ (r = 0.52, p < 0.001). A third model excluding the EBI found the MEQ to have an insignificant effect on changes in QIDS (B = −0.026, β = −0.155, p = 0.095).
Measures of the acute psychedelic experience predicting change in QIDS.
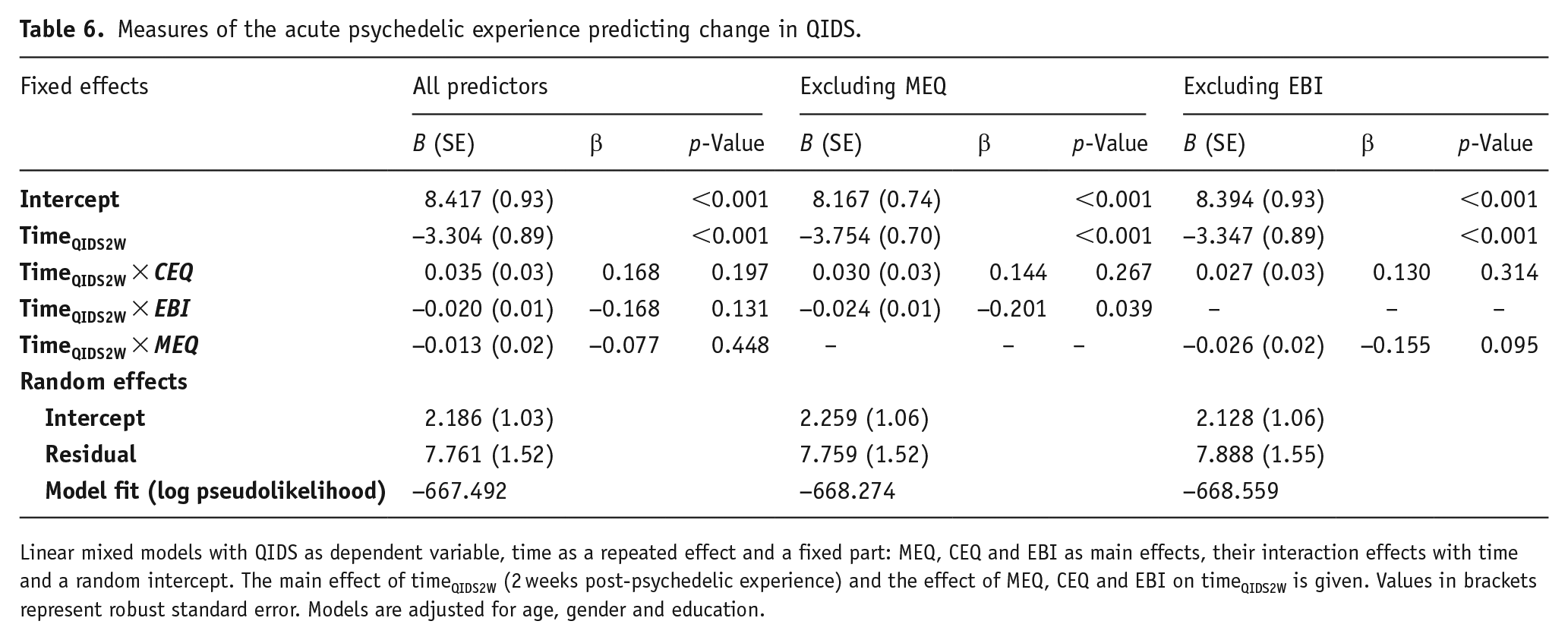
Linear mixed models with QIDS as dependent variable, time as a repeated effect and a fixed part: MEQ, CEQ and EBI as main effects, their interaction effects with time and a random intercept. The main effect of timeQIDS2W (2 weeks post-psychedelic experience) and the effect of MEQ, CEQ and EBI on timeQIDS2W is given. Values in brackets represent robust standard error. Models are adjusted for age, gender and education.
Discussion
This study is among the largest naturalistic study to prospectively assess changes in symptoms of depression and anxiety in a sample of participants with symptoms of depression following a psychedelic experience. Significant reductions in both depression and anxiety scores following a self-initiated psychedelic experience were detected at both 2 and 4 weeks after the psychedelic experience. These results are in line with both early and more recent psychedelic studies that have highlighted promising therapeutic effects of psychedelics – particularly in relation to psychedelic-assisted psychotherapy.
A systematic review of the first era (1950s–1960s) of psychedelic trials in mood disorder symptoms recently concluded, among 423 individuals in 19 studies, 335 (79.2%) showed ‘clinician-judged improvement’ after treatment with psychedelics (Rucker et al., 2016). These trials were of a period prior to the establishment of validated measures and quantitative response criteria, but more recent experimental and cross-sectional studies have lent support to the merits of psychedelic therapy for depression, with two notable recent controlled trials finding response rates exceeding 70% (Carhart-Harris et al., 2021a; Davis et al., 2021a). These trials supplement a number of lab-based experimental studies conducted in the last 10 years that have found consistent positive results in favour of the therapeutic potential of psychedelic therapy for treating symptoms of depression and anxiety (Carhart-Harris et al., 2016a, 2017; Davis, Barrett and May, 2021; Gasser et al., 2014; Grob et al., 2011; Griffiths et al., 2016; Osório et al., 2015; Ross et al., 2016; Sanches et al., 2016; Watts et al., 2017). Specifically, controlled trials involving both inert and active comparators, such as first-line standard of care (an SSRI course) plus psychological support in one recent trial (Carhart-Harris et al., 2021a), serve to highlight the robust and reliable antidepressant and anxiolytic effects of psychedelic therapy.
In the current study, reductions in depressive symptoms from baseline to 2-week follow-up were found to be large by convention (Cohen’s d = 1.2) and were comparable to those seen in controlled studies (e.g. Carhart-Harris et al., 2016a, 2017) when assessing a comparably severe subsample, that is, Cohen’s d of 2.1–2.4 in those with moderate-to-severe depressive symptoms at baseline. Provocatively, these results imply that it is possible to achieve comparable efficacy via ‘naturalistic’ use of psychedelics to what has been observed in controlled trials. It remains possible that the present study’s sample sought to emulate some of the methods of the controlled research, such as having a ‘sitter’ or ‘guide’, listening to music and having individual and community support before and after their experience.
A secondary aim of the present study was to explore potential predictors of response. Higher drug doses were found to be predictive of larger changes in depressive symptoms. This result accords with those from a previous study that found significantly larger increases in long-term well-being after a high dose of psilocybin compared with a low dose (Griffiths et al., 2011). Higher doses are more likely to produce the intensity and quality of acute experience (Griffiths et al., 2011; Haijen et al., 2018; Hasler et al., 2004; Madsen et al., 2019; Studerus et al., 2012) that seems to be important (if not necessary) for robust therapeutic outcomes (Carbonaro et al., 2016; Carhart-Harris et al., 2017; Griffiths et al., 2008; Haijen et al., 2018; Roseman et al., 2018). Consistent with previous findings and current and long-standing assumptions about the context-dependency of psychedelic outcomes (Carhart-Harris et al., 2018; Haijen et al., 2018; Hartogsohn, 2017; Leary et al., 1963; Metzner et al., 1965; Studerus et al., 2012), having medicinal motives for use was associated with larger improvements in depressive symptoms and trait anxiety. This was true even after adjustment for baseline depressive symptoms. Medicinal motives are likely to be related to positive prior expectancy, a major component of the action of all effective treatments, including placebo (Olson et al., 2020) and SSRIs (Hjorth et al., 2021). Positive expectancy has recently come under the spotlight in psychedelic research where for example, belief about receipt of a psychedelic appears to be major driver of outcomes (Kaertner et al., 2021; Olson et al., 2020; Szigeti et al., 2021; Van Elk et al., 2021). Whether expectancy is a (justifiably or experimentally) extricable component of any treatment, not just psychedelic therapy, is a question worthy of some thought (Carhart-Harris et al., 2021b).
The present results showed that having emotional breakthrough during the acute psychedelic experience was significantly associated with a larger decrease in depressive symptoms. Although the effect estimate was small, this finding supports recent work by our group that emotional breakthrough during the acute psychedelic experience is reliably predictive of subsequence improvements in mental health outcomes. Indeed, we have now seen this in both healthy participants (Roseman et al., 2019), individuals with eating disorders (Spriggs et al., 2020) and individuals with depression in a recent controlled trial. Thus, the present results indicate that measuring specific therapeutic facets of the acute experience such as emotional breakthrough is important in order to understand the therapeutic process and mediating factors.
Another salient facet of the subjective psychedelic experience is the gain of new insight during (Davis et al., 2021a) and after the psychedelic experience (Peill et al., 2022). Insight experiences have previously been found to correlate with positive outcomes after psychedelic use in a lab-based study of depressed patients (Roseman et al., 2018) and in a cross-sectional survey study of participants with anxiety and depression in which the psychological insight questionnaire (PIQ) was used (Davis et al., 2020). Moreover, in our recent double-blind randomised controlled trial, sub-acute psychological insight was found to mediate the relationship between emotional breakthrough and improvements in depression – using a new scale to measure insight that is, the psychological insight scale (PIS) (Peill et al., 2022).
The EBI (Roseman et al., 2019), PIQ (Davis et al., 2020) and PIS (Peill et al., 2022) have several similarities as they aim to measure knowledge gained through a psychedelic experience leading to mental health improvements. The EBI measures the acute emotional experience and processing of difficult emotions and memories (Roseman et al., 2019), whereas the PIQ measures the process of meaning-making within the psychedelic experience and emotional processing leading to new insights in a broader sense: awareness of life purpose, goals, coping techniques, etc. Thus, the PIQ seems to capture a more integrative aspect of the psychedelic experience (Davis et al., 2020). Similarly, the PIS is a measure intended to be used at least 1 day after an acute psychedelic experience – where it can have prognostic predictive power (Peill et al., 2022). The current study did not include the PIQ as it was not published when we collected the present data; thus, further research is needed to explore the relationship between these two measures (i.e. the PIQ and PIS), as well as to utilise the new psychological insight scale, the PIS (Peill et al., 2022).
Unlike in previous studies (Bogenschutz et al., 2015; Davis et al., 2019; Erritzoe et al., 2018; Griffiths et al., 2008, 2016; Haijen et al., 2018; MacLean et al., 2011; Nour et al., 2017; Schmid and Liechti, 2017), the MEQ was not significantly predictive of response in this study. However, it is possible that the mystical-type experience has a core dimension – for example, a sense of the interconnectedness of things, also known as ‘the unitive experience’ – that could perform well in predictive models, while being amenable to a mechanistic understanding. Given the consistent performance of the MEQ as mediator of therapeutic outcomes in a range of populations (Bogenschutz et al., 2015; Davis et al., 2019; Erritzoe et al., 2018; Griffiths et al., 2008, 2016; Haijen et al., 2018; MacLean et al., 2011; Nour et al., 2017; Schmid and Liechti, 2017), we do not advocate abandoning it, as it seems to be capturing something functionally important; however, we wonder whether there may be scope for revising how it is used or for supplementing it with measures of emotional breakthrough and psychological insight.
Limitations
Several limitations of the current study should be noted. Firstly, as the study was not controlled, only weak inferences that can be drawn on its data. Response bias and non-compliance with instructions, including the reliable completion of surveys on schedule, may have affected the data quality. Self-selection bias is consistent weakness of psychedelic studies and particularly naturalistic ones, where the sample is likely to be skewed towards psychedelic ‘advocates’, who may also be biased via past use (Haijen et al., 2018), for example, more than half of the participants had with a history of more than six prior uses of psychedelics. The majority of participants enrolled in the present study were young (mean age was 27), male (i.e. 71%) and well-educated. In addition, the survey design required participants to be planning a psychedelic experience in the near future, which might have excluded individuals using psychedelics in a more spontaneous manner, who may for example, through poor preparation, be more vulnerable to negative outcomes. The large attrition rate observed in the present study is another limitation that may have created a bias towards those who were more motivated with procedures and thus, likely to respond – and favourably in relation to psychedelics. Rare cases of iatrogenesis may be overlooked due to an attrition bias, that is, loss to follow-up. This possibility is entirely speculative, however.
Partially alleviating the concern of an attrition bias, another study from our lab investigated predictors of attrition (i.e. ‘drop out’) rate in the same sample being reported on here and found no relationship between attrition and depressive symptoms (QIDS) or ratings of CE (CEQ) (Hübner et al., 2020). Consistent with what is known about attrition in research studies more generally, younger age and lower educational levels were predictive of drop-out.
Conclusions
In summary, the present naturalistic study supports clinical trials and cross-sectional data favouring the therapeutic potential of the psychedelic experience. Robust reductions in both depressive symptoms and anxiety levels were found from baseline to 2 and 4 weeks following a naturalistic psychedelic experience. Higher psychedelic dose, being more medicinally motivated, having had fewer previous psychedelic experiences and having an emotional breakthrough during the drug experience were all predictive of larger mental health improvements. Despite the inherent limitations of a naturalistic and uncontrolled design, this study adds valuable evidence to the literature supporting the therapeutic potential of psychedelics, which bear specific relevance to current legalisation and decriminalisation initiatives. However, we caution that these data are vulnerable to bias. Indeed, it remains essential to use precautionary messaging regarding the context-dependency of the safety and efficacy profile of psychedelic drugs.
Supplemental Material
sj-docx-1-jop-10.1177_02698811221101061 – Supplemental material for Antidepressant effects of a psychedelic experience in a large prospective naturalistic sample
Supplemental material, sj-docx-1-jop-10.1177_02698811221101061 for Antidepressant effects of a psychedelic experience in a large prospective naturalistic sample by Victoria Amalie Nygart, Lis Marie Pommerencke, Eline Haijen, Hannes Kettner, Mendel Kaelen, Erik Lykke Mortensen, David John Nutt, Robin Lester Carhart-Harris and David Erritzoe in Journal of Psychopharmacology
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Centre for Psychedelic Research at Imperial College is supported by its philanthropic supporters listed here: ![]() . RCH acts as an advisor to Entheon Biomedical, Maya Health, Osmind, Beckley Psytech, TRYP Therapeutics, Synthesis Institute, Journey Collab, Journey Space and Usona Institute. DE has received funding from NIHR and is scientific advisor for Mydecine, Entheon Biomedical, Clerkenwell Health, Smallpharma Ltd and Field Trip Health Ltd.
. RCH acts as an advisor to Entheon Biomedical, Maya Health, Osmind, Beckley Psytech, TRYP Therapeutics, Synthesis Institute, Journey Collab, Journey Space and Usona Institute. DE has received funding from NIHR and is scientific advisor for Mydecine, Entheon Biomedical, Clerkenwell Health, Smallpharma Ltd and Field Trip Health Ltd.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.