
Abstract
Introduction:
Selective serotonin reuptake inhibitors (SSRIs) are commonly prescribed to older adults. In contrast to young subjects, it is unclear whether older adults may be vulnerable to cognitive side effects. Serotonin is involved in cognitive functions (e.g. memory). It is of great importance to examine the effects of SSRIs on memory functioning in older adults.
Objectives:
The objective of this systematic literature review is to summarize studies in which the effects of SSRI treatment on all aspects of memory functioning in older adults are investigated.
Methods:
PubMed, PsycINFO, CINAHL, and Embase were searched for all studies published until 18th of October 2021. Articles were included if they fulfilled the inclusion criteria as follows: (1) study design is (randomized) controlled trial, cross-sectional, or prospective cohort study; (2) study population consists of older adults (mean age ⩾65 years), or results for this age-group are reported separately; (3) intervention is use of an SSRI; and (4) effects on performance of any memory domain are measured and clearly described.
Results:
The search yielded 1888 articles, of which 136 were included for the full-text review. Eventually, 40 articles were included. Most studies reported no association between SSRI use and memory functioning. The studies that found a positive association mainly investigated older adults with mental or neurological disorders (e.g. depression or stroke). A few studies found a negative association in the following subgroups: non-responders (depression), patients with frontal brain disease, and women.
Conclusion:
Overall, no consistent negative effects of SSRIs on memory functioning in older adults were found after SSRI treatment. Most studies reported no change in memory functioning after SSRI use. Some studies even showed an improvement in memory performance. Positive effects of SSRIs on memory functioning were especially found in older adults with mental or neurological disorders, such as subjects with depression or stroke.
Keywords
Introduction
Over the last decade, the use of antidepressants seems to be rising (Brett et al., 2017). A longitudinal study observed that 6.6% of community-dwelling older adults used a selective serotonin reuptake inhibitor (SSRI) at 6 years follow-up (Marcum et al., 2016). In older adults, indications for antidepressant treatment are the same as they are for younger adults, for example, depression and anxiety disorders (Kok, 2013). It is well known that depression is often associated with memory impairment, both in adults and older adults (Marazziti et al., 2010). Remission of depression can lead to improvement of cognitive functioning (Story et al., 2008), suggesting a relation between depressive symptoms and cognitive functions. However, it has also been described that cognitive recovery can occur independent of depression treatment response (Jorge et al., 2010). This finding indicates that antidepressant treatment may have a dissociable effect on depressive symptoms and cognition.
Prevalence of cognitive impairment increases with age and is associated with lower quality of life (Bárrios et al., 2013). Therefore, it is relevant to investigate the effect of commonly prescribed medication, such as SSRIs, on cognitive functioning in older adults. It is plausible to assume that SSRIs affect cognitive functions, since serotonin (5-HT) is involved in attention and (working)memory (Štrac et al., 2016). Studies in older adults are lacking, but previous serotonergic challenge studies have suggested that SSRI administration is associated with acute improvement of long-term memory (Harmer et al., 2002) and positive information processing (Harmer et al., 2004; Norbury et al., 2009) in healthy adult volunteers. However, other studies have observed no acute effect on cognitive functioning (Rose et al., 2006; Siepmann et al., 2003) or even suggested impairment of vigilance after sub-chronic treatment (Riedel et al., 2005).
With aging, changes in 5-HT functioning occur; receptor expression and binding affinity of multiple 5-HT receptors have been shown to decrease in older adults (Fidalgo et al., 2013; Lu et al., 2004). Impaired 5-HT neurotransmission in aging has been associated with impaired cognitive processes (Rodriguez et al., 2012). Based on these changes, it could be hypothesized that SSRI treatment in older adults may have a different effect than in younger adults.
In conclusion, SSRIs are commonly prescribed to older adults, who already seem vulnerable to memory impairment due to age-related serotonergic changes and neurodegeneration. Therefore, it is important to know the possible effects of SSRIs on memory functioning in older adults. Given the limited amount of studies conducted in older adults, there is a need for a broad and general synthesis of the evidence. The aim of this systematic literature review is therefore to summarize all relevant findings on the effects of SSRIs on all aspects of memory function in older adults.
Methods
Protocol and registration
This systematic review was registered in the PROSPERO database under the ID CRD42021283326.
Data sources and search
The literature search was conducted in databases PubMed, PsycINFO, CINAHL, and Embase. The search consisted of predictor-related terms (e.g. SSRI), outcome-related terms (e.g. short-term memory and cognition), and specific limitations (e.g. humans and language restrictions). The complete search strategy is provided in Supplemental Appendix 1.
Study selection
All publications until the 18th of October 2021 were included if they fulfilled the following eligibility criteria: (1) study design is (randomized) controlled trial, cross-sectional, or prospective cohort study; (2) study population consists of older adults (mean age ⩾65 years), or results for this age-group are reported separately; (3) intervention is use of an SSRI; and (4) effects on performance of any memory domain, such as global memory (assessed by the Wechsler Memory Scale (WMS), mini-mental state examination (MMSE), etc.), semantic memory, visual/spatial memory, working memory, episodic memory, long-term memory, and/or short-term memory are measured and clearly described. Reference lists of publications and secondary literature (review articles, editorials, book chapters, etc.) were hand-searched for possible missing articles.
Data extraction and quality assessment
The selection process was in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009). Two authors (J.E.M.S. and S.S.) independently screened titles and abstracts for potential eligibility based on the abovementioned eligibility criteria. Next, full-text articles of potentially relevant citations were examined by these two authors (J.E.M.S. and S.S.). Disagreements were resolved by discussion until consensus was reached.
A standardized data collection form was used to extract information. Information was extracted from each included publication on: (1) study design; (2) characteristics of participants, including age, disease and use of co-medication; (3) type of intervention, including type of SSRI, dosage and duration of the intervention, and, if applicable, intervention for the control group; (4) tests used to assess memory performance; (5) observed effect of treatment on memory. One author (M.J.) extracted the data from included full-text articles and one author (J.E.M.S.) checked the extracted data. If full-text articles were not available, corresponding authors and/or affiliated institutes were contacted by e-mail.
The Cochrane Collaboration Tool for Risk of Bias (Higgins et al., 2011) was used for the quality assessment of randomized controlled trials. The adapted version for cross-over trials (Sterne et al., 2019) was used for randomized cross-over trials. Non-randomized clinical trials were assessed using the Risk of Bias In Non-randomized Studies of Interventions (ROBINS-I) (Sterne et al., 2016). Assessment of risks of bias and quality was done by author J.S.
Synthesis of result
Data will be presented in a narrative manner, because heterogeneous results inherent to the broad research question will make a meta-analytic analysis less appropriate. First, we will present the general results of SSRI treatment on memory functioning per memory domain. Second, we will present results for various populations of older adults (e.g. with depression and stroke).
Results
The search yielded 1888 articles, of which 136 were included for full-text review. Of these, 99 were excluded due to different reasons based on the exclusion criteria (Figure 1). Twenty-four potentially relevant articles were found from cross-references, of which three were included. We contacted 15 authors to obtain full-text articles that were not available to us. Of these, three authors responded. Eventually, a total of 40 articles were included, of which 23 randomized controlled trials, 3 controlled clinical trials, 6 non-controlled clinical trials, and 8 prospective cohort study. All 40 studies and their details and results are summarized in Table 1.
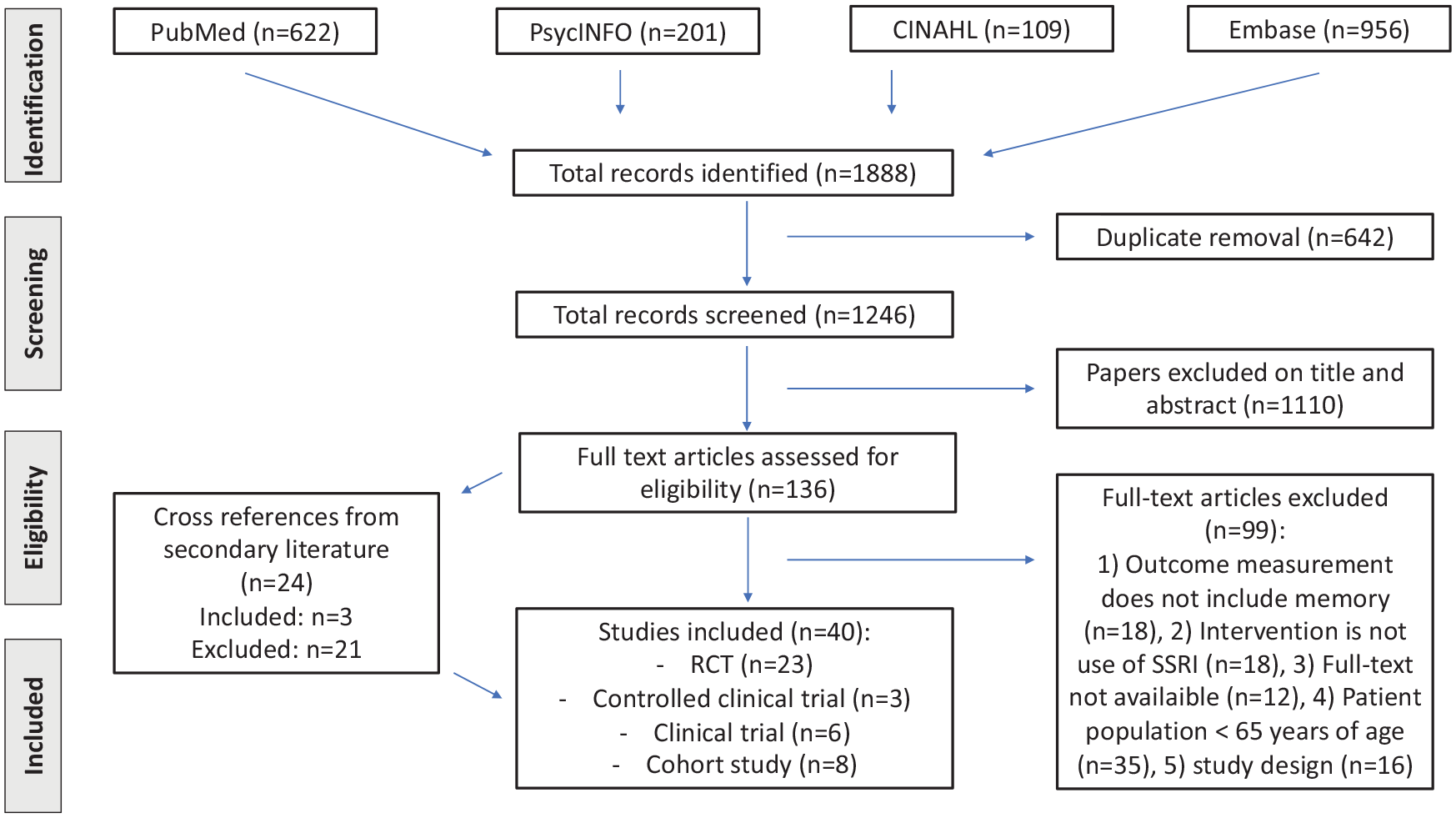
PRISMA flowchart search and screening process.
Characteristics of included studies.

SD: standard deviation; n: sample; MDD: major depressive disorder; DSM: Diagnostic and Statistical Manual of Mental Disorders; N/A: not available; mg: milligram; MMSE: mini-mental state examination; DSST: Digit Symbol Substitution Test; SLT: Shopping List Task; ICD: International Classification of Diseases; WRT: Word Recall Test; SSRI: selective serotonin reuptake inhibitor; WAIS: Wechsler Adult Intelligence Scale; FTD: frontotemporal dementia; DS: digit span; CANTAB: Cambridge Neuropsychological Test Automated Battery; AD: Alzheimer’s disease; NINCDS/ADRDA: National Institute for Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association; RBMT: Rivermead Behavioral Memory Test; ADAS: Alzheimer’s Disease Assessment Scale; WMS: Wechsler Memory Scale; PST: problem-solving therapy; RBANS: Repeatable Battery for the Assessment of Neuropsychological Status; HAM-D: Hamilton Rating Scale for Depression; rTMS: repetitive Transcranial Magnetic Stimulation; PD: personality disorder; HAM-A: Hamilton Rating Scale for Anxiety; FIM: Functional Independence Measure; CAMCOG: Cambridge Cognitive Examination; MADRS: Montgomery Asberg Depression Rating Scale; ROCFT: Rey–Osterrieth Complex Figure Test; BVRT: Benton Visual Retention Test; NOS: not otherwise specified; CNS: central nervous system; NIH: National Institutes of Health; GDS: Geriatic Depression Scale; GAD: generalized anxiety disorder; IDS: Inventory of Depressive Symptomatology; TCA: tricyclic antidepressants; SNRI: serotonin-norepinephrine reuptake inhibitor; NPI-Q: Neuropsychiatric Inventory Questionnaire.
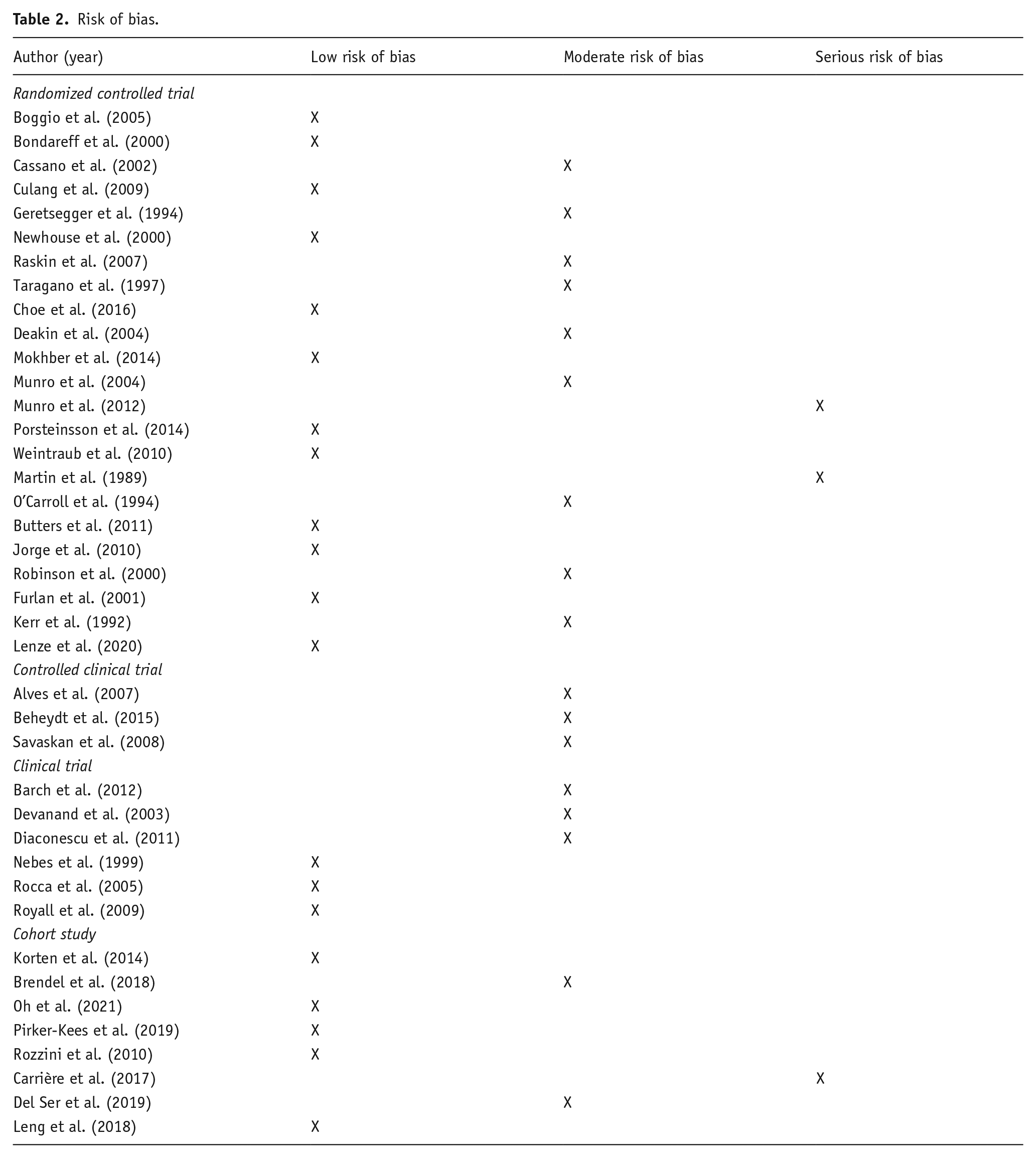
The risk of bias for the included studies varied from low risk of bias (n = 20) to serious risk of bias (n = 3). Especially in the non-randomized studies, there was moderate to serious bias due to confounding, but also in the randomized controlled trials the randomization process was sometimes not described clearly (e.g. method of randomization not specified) (Table 2).
Risk of bias.
Effects on global memory
In total, 29 studies assessed global memory, using MMSE, WMS, Blessed Information and Memory Test (BIMT), the Clifton Assessment Schedule (CLAS), Alzheimer’s Assessment Scale (ADAS), the Rivermead Behavioral Memory Test (RBMT), the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS), the Cambridge Cognitive Examination (CAMCOG), the Dementia Rating Scale (DRS) or the National Institutes of Health (NIH) Toolbox Cognition Battery, and Alzheimer’s Disease Assessment Scale. Of these, 11 studies reported an association between SSRI use and improvement of global memory functioning, 16 studies reported no effect, and 2 studies reported an impairment in global memory functioning associated with SSRI use. The results are shown in Table 3, specified per type of memory.
Results of studies, divides into different types of memory.
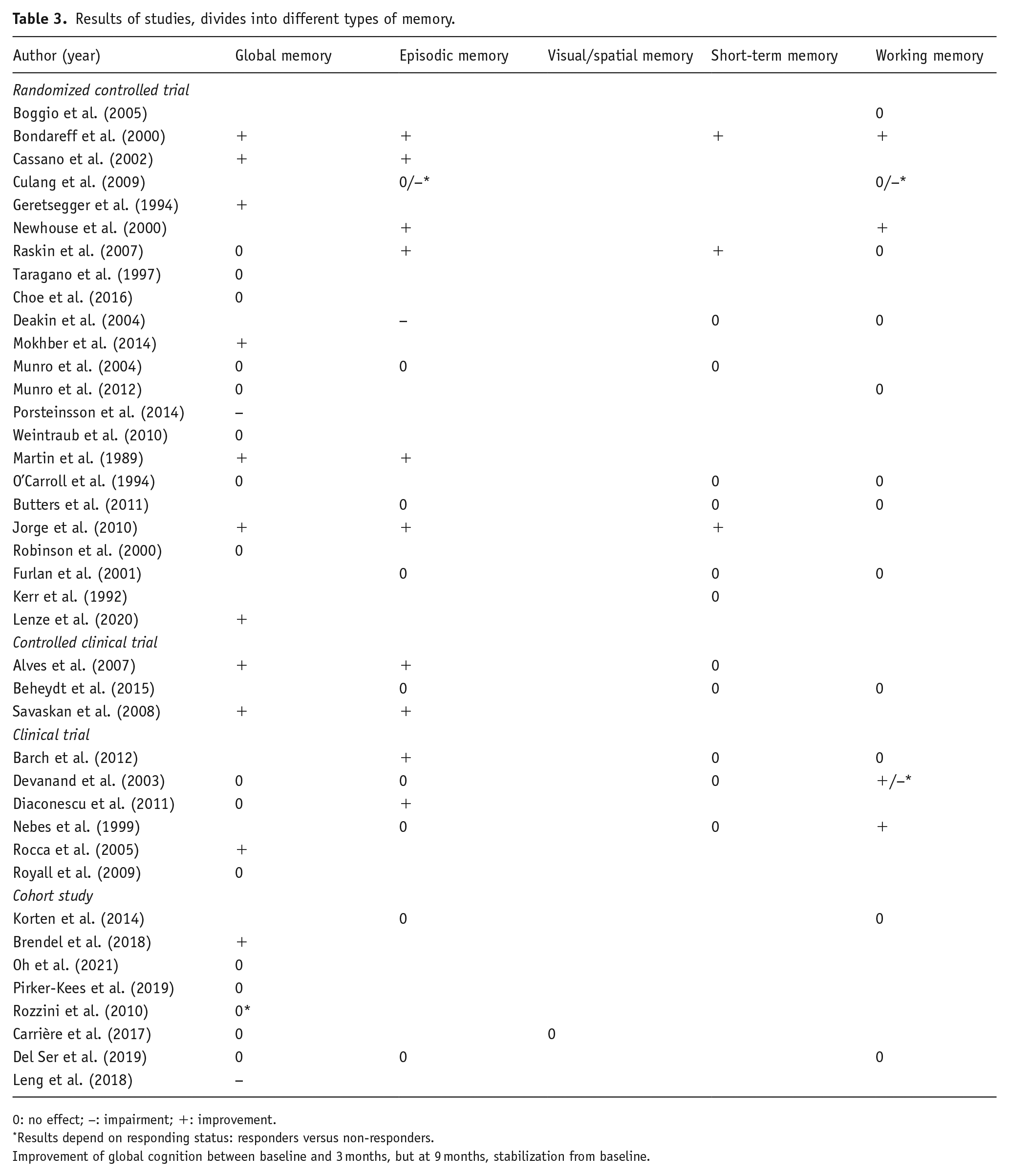
0: no effect; −: impairment; +: improvement.
Results depend on responding status: responders versus non-responders.
Improvement of global cognition between baseline and 3 months, but at 9 months, stabilization from baseline.
Effects on episodic memory
Episodic memory functioning was assessed using Word Recall Test (WRT), Shopping List Task (SLT), facial picture recognition test, delayed pattern recognition, paired-associate learning (PAL), and subtests of the RBANS and CAMCOG. Half of these studies (10 out of 20) found an improvement in episodic memory functioning, while 8 studies reported no effect. One study found the effect to be depended on responding status. Patients who improved on depression after use of SSRI did not experience an effect on episodic memory, but patients who did not improve on depression did experience an impairment in episodic memory functioning. One other study reported a post-SSRI impairment in episodic memory functioning, measured with delayed pattern recognition task (see Table 3).
Effects in visual or spatial memory
One study has assessed visual or spatial memory, using the Benton Visual Retention Test. This prospective cohort study did not find an effect of SSRIs on visual memory (see Table 3).
Effects on short-term memory
Fourteen studies assessed the effect of SSRIs on short-term memory, using forward digit span, consonant trigrams, Wechsler logical memory, immediate recall of WRT, SLT, PAL, and pattern recognition and subtests of RBANS, WMS, and CAMCOG. Three reported an improvement, while 11 studies reported no effect. No studies reported an impairment of short-term memory after use of SSRI (see Table 3).
Effects on working memory
Working memory was assessed in 16 studies, using the Digit Symbol Substitution Test (DSST), backwards digit span, letter–number sequencies, and the Wechsler figural memory. In 3 studies, an improvement in working memory functioning was found, while in 11 studies, no effect was reported. In 2 studies, the effect of SSRIs on working memory depended on responding status; responders showed no effect in one study and an improvement in the other study. In both studies, non-responders showed impairment of working memory after use of SSRI (see Table 3).
Effects on memory in depressed subjects
In 17 studies, the effects of SSRIs on memory functioning in older depressed subjects were reported. The results are shown in Supplemental Appendix, Table 4. Global memory was assessed in 10 studies, of which 6 showed improvement while the others reported no effect after SSRI treatment. Episodic memory improved after use of SSRI in 8 of 13 studies, 4 studies found no effect, and 1 study found the effect to be depended on responding status (no effect in responders and impairment in non-responders). Short-term memory was assessed in seven studies, two showing improvement and five did not report any effect. The effects of SSRIs on working memory was depended on responding status according to two studies: one found that responders did not have any effect while non-responders experienced impairment and the other study reported an improvement in responders and an impairment in non-responders. Three studies showed an improvement in working memory functioning after SSRI use and the remaining five studies found no effect. The quality of the studies in depressed subjects was good to moderate (Table 2).
Effects on memory in subjects with dementia
Thirteen studies included subjects with dementia of various etiologies (Supplemental Appendix, Table 5). Global memory was assessed in 12 of them; 3 reported improvement, 1 reported impairment, and the remaining 8 studies reported no effect on memory functioning. Episodic memory was measured in three studies, one reporting improvement, one reporting impairment, and one reporting no effect. Three studies reported on the association between short-term memory and working memory and SSRI use in patients with dementia, but none found an association. Most studies in dementia patients were of good quality, except two studies had serious risk of bias (Martin et al., 1989; Munro et al., 2012) (Table 2).
Effects on memory in general population
Five studies of good to moderate quality included healthy subjects from the general population. The results are shown in Supplemental Appendix, Table 6. Two studies reported outcomes on global memory functioning, of which one study found a positive effect and the other found no effect. Episodic memory, short-term memory, and working memory were reported in two studies, none of them reported an effect.
Effects on memory in miscellaneous study populations
We grouped five studies as “miscellaneous.” Post-stroke cognitive functioning related to use of SSRI was reported in three studies (Jorge et al., 2010; Robinson et al., 2000; Royall et al., 2009), one study investigated older adults with generalized anxiety disorder (GAD) (Butters et al., 2011), and one study a population of community-dwelling older adults who used antidepressants (Carrière et al., 2017). The results are shown in Supplemental Appendix, Table 7. In post-stroke patients, improvement of global memory, episodic memory, and short-term memory was reported in one study, while the other two studies reported no effect on global memory functioning. In older adults with GAD, no effects were reported on episodic memory, short-term memory, or working memory. In community-dwelling older adults who used antidepressants, no effects were found on global memory or visual memory, but this study had serious risk of bias (Carrière et al., 2017).
Discussion
The aim of the present systematic review was to summarize all relevant findings on the effects of SSRIs on all aspects of memory function in older adults.
Overall, no consistent negative effects of SSRIs on memory functioning in older adults were found after 4 weeks to 10 years of SSRI treatment. The majority of studies reported no change in memory functioning after SSRI use. Interestingly, also positive effects of SSRIs on memory functioning were found. This seemed to be most pronounced in older adults with mental or neurological disorders, such as subjects with depression or stroke.
Depression
Global memory and episodic memory functioning in patients with depression seemed to be most sensitive to positive influence of SSRI use (see Table 4). The relationship between improved memory functioning and improved depression symptoms (treatment effect) is difficult to determine on basis of the current review. However, two studies reported that improvement of memory functioning was associated with responder status (Culang et al., 2009; Devanand et al., 2003). Non-responders were more likely to experience impairment in memory functioning, while responders showed no effect (Culang et al., 2009) or even improvement (Devanand et al., 2005). In total, three studies found correlations between (remission of) depression and cognitive outcome (Culang et al., 2009; Devanand et al., 2003; Diaconescu et al., 2011). In contrast, other studies have reported that the effect was independent of depression symptoms (Jorge et al., 2010; Raskin et al., 2007). Also, a greater reduction in depression scores did not predict a greater effect on memory functioning (Barch et al., 2012). Baseline severity of depression did not seem to influence results. The majority of studies were conducted in patients with severe depression, but also in mild-to-moderate depressions, some studies reported improvement of memory functioning (Rocca et al., 2005; Savaskan et al., 2008) and others no effect (Devanand et al., 2003; Korten et al., 2014). Taken together, the association between improved memory performance and depression conditions cannot be ascertained on basis of the current review.
Also, in some of the studies in depressed patients, two treatments or SSRIs were compared to each other (Alves et al., 2007; Bondareff et al., 2000; Cassano et al., 2002; Furlan et al., 2001; Geretsegger et al., 1994; Mokhber et al., 2014; Newhouse et al., 2000; Robinson et al., 2000; Rocca et al., 2005; Taragano et al., 1997). Inherent to this study design is the possible bias of practice effects, meaning that the improvement reported is not due to treatment, but to the fact that patients learn to perform better on the cognitive tasks. Even though practice effect is an important factor to take into account, in this review also placebo-controlled studies and studies with a healthy comparison group showed positive effects of SSRIs on memory functioning (Alves et al., 2007; Jorge et al., 2010; Lenze et al., 2020; Raskin et al., 2007; Savaskan et al., 2008), making it unlikely that practice effect accounts for all reported improved memory functioning.
Dementia and other brain diseases
Results in patients with dementia were mostly pointing toward no effect of SSRI use on memory performance, but three studies indicated possible improvement of memory functioning (Brendel et al., 2018; Martin et al., 1989; Mokhber et al., 2014) (see Table 5 in Supplemental Appendix). Interestingly, two studies reported impairment of memory functioning associated with SSRI use (Deakin et al., 2004; Porsteinsson et al., 2014). Both studies were performed in dementia with frontal dysfunction. This underlying subtype could potentially be more prone to SSRI-associated memory impairment.
In post-stroke patients, Jorge et al. (2010) reported improvement of global memory, episodic memory, and short-term memory. Two other studies failed to replicate this finding in global memory functioning (Robinson et al., 2000; Royall et al., 2009).
Healthy controls
Five studies assessed the association between SSRI use and memory functioning in healthy older adults (Carrière et al., 2017; Del Ser et al., 2019; Furlan et al., 2001; Kerr et al., 1992; Lenze et al., 2020; Leng et al., 2018) (see Table 6 in Supplemental Appendix). The majority reported no association. Lenze et al. (2020), however, reported an improvement in global memory functioning in older adults who did not have objective cognitive deficits, but did experience subjective cognitive decline. This could represent an early cognitive vulnerability. One study did report an impairment in global memory functioning (Leng et al., 2018). Interestingly, this study did only include women which could indicate a gender effect.
Other factors that may have affected results
The studies that were included in which SSRI treatment lasted 12 weeks or longer (Barch et al., 2012; Beheydt et al., 2015; Bondareff et al., 2000; Brendel et al., 2018; Butters et al., 2000, 2011; Carrière et al., 2017; Cassano et al., 2002; Choe et al., 2016; Del Ser et al., 2019; Devanand et al., 2003; Jorge et al., 2010; Leng et al., 2018; Lenze et al., 2020; Mokhber et al., 2014; Munro et al., 2004, 2012; Newhouse et al., 2000; Oh et al., 2021; Pirker-Kees et al., 2019; Robinson et al., 2000; Rocca et al., 2005; Rozzini et al., 2010; Weintraub et al., 2010) were slightly more likely to find positive effects than studies reporting results of treatments of 4 weeks or shorter (Deakin et al., 2004; Furlan et al., 2001; Kerr et al., 1992; Martin et al., 1989; O’Carroll et al., 1994; Savaskan et al., 2008) and less likely to find negative results. This could indicate that long-term SSRI use does not have a deleterious effect on brain functions related to memory.
While our results did not show any convincing evidence of a negative effect of SSRI use on memory functioning in older adults, there are some contradictory findings in other studies with adult volunteers. It is suggested that SSRI use could lead to impaired memory functioning in adult volunteers; negative results on learning, episodic memory, and short-term memory have been reported (Chamberlain et al., 2006; Schmitt et al., 2001; Skandali et al., 2018; Wadsworth et al., 2005). It should be noted that these acute effects may be dose-dependent (Saletu et al., 1986). Together with the long-term studies reported in this review, this suggests that SSRI treatment can have an initial deleterious effect on memory but after reaching a steady state, these effects are no longer found. This difference can be explained on basis of the difference of acute- and long-term treatment of SSRIs on the brain (Sugrue, 1983).
Another observation was that underlying neuropsychiatric vulnerability appeared to play a role in the effect of SSRI use on memory functioning. This is also suggested by findings of a negative effect of acute tryptophan depletion on global memory (measured by MMSE) only in patients with Alzheimer’s disease and remitted depression, but not in healthy older control subjects (Porter et al., 2000, 2005) (although it should be noted that completing the MMSE is a fairly easy task for most healthy older adults, which could lead to failure to notice a more subtle impairment). A possible explanation for these findings is the hypothesis that memory performance relates to 5-HT in an inverted U-curve, implicating that memory performance is optimal at a certain level of 5-HT, but decreases when 5-HT levels increase or decrease from that optimum (Meeter et al., 2006; Riedel et al., 1999, 2002). Considering impaired 5-HT functioning as an important pathogenic factor in both depression (Jacobsen et al., 2012) and Alzheimer’s disease (Xu et al., 2012), it can be understood why patients with these neuropsychiatric disorders are more likely to experience cognitive improvement with SSRI treatment, compared to healthy subjects who are already on the 5-HT optimum.
Methodologic considerations
The strength of this systematic review is the inclusion of studies using study designs of sufficient quality with a broad range of study populations. Nevertheless, there are a number of limitations that needs to be mentioned. The present findings must be interpreted with caution, because there is always a risk of publication bias. Some studies included a small number of patients, which can lead to low statistical power and failure to identify an effect of SSRI treatment (Type II error). There did not seem to be a difference in reported results between studies with small populations versus large populations. Also, the studies used different outcome measures to test memory performance, making direct comparisons of findings difficult. Some tests may be more sensitive for change after treatment with an SSRI. There was heterogeneity in study population and intervention (type of SSRI). Therefore, we also reported the results both for the total study population and per subgroups.
In conclusion, the current systematic review showed that SSRIs do not impair memory performance in older adults and patients. Interestingly, some subgroups may even benefit from long-term SSRI treatment on memory performance. For refining these subgroups, further research is recommended. A randomized placebo-controlled cross-over design in older adults with and without neuropsychiatric vulnerability could be recommended. Long-term effects, possible confounding factors, such as depressive complaints, pre-existing cognitive impairment, gender, and variability in type and dose of SSRI, but also clinically relevant outcome measurements such as quality of life should be taken into account.
Supplemental Material
sj-docx-1-jop-10.1177_02698811221080462 – Supplemental material for The effects of selective serotonin reuptake inhibitors on memory functioning in older adults: A systematic literature review
Supplemental material, sj-docx-1-jop-10.1177_02698811221080462 for The effects of selective serotonin reuptake inhibitors on memory functioning in older adults: A systematic literature review by Julie EM Schulkens, Kay Deckers, Maud Jenniskens, Arjan Blokland, Frans RJ Verhey and Sjacko Sobczak in Journal of Psychopharmacology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.