
Abstract
Background:
Selective serotonin reuptake inhibitors (SSRIs) have a wide and increasing use for the treatment of depression and anxiety. Previous studies have indicated an increased risk of hyponatremia during the first months of treatment. We aimed to investigate the detailed time-course of SSRI-associated hyponatremia with a high temporal resolution, using registry data encompassing the total Swedish population.
Methods:
This was a population-based case control study using several national registers. Patients hospitalized with a principal diagnosis of hyponatremia (n = 11,213) were compared with matched controls (n = 44,801). Multivariable regression was applied to explore time-dependent associations between SSRIs and hospitalization due to hyponatremia.
Results:
Individuals initiating treatment with SSRIs were exposed to an immediately increased risk for hospitalization at week 1, reaching an adjusted odds ratio (aOR) (95% confidence interval) of 29 (19–46). The associations then gradually declined, reaching an aOR of 2.1 (1.0–4.2) by week 13. The aOR for individuals treated for longer than 13 weeks was 0.78 (0.71–0.85).
Conclusions:
This study revealed a dramatically increased risk of hyponatremia exclusively related to newly initiated treatment. Consequently, even subtle symptoms consistent with hyponatremia during the first weeks of SSRI treatment should prompt analysis of sodium levels. In patients treated with SSRIs for several months or years, other causes should primarily be sought in the event of hyponatremia.
Keywords
Introduction
Hyponatremia is the most common electrolyte imbalance, affecting up to 30% of hospitalized patients (Upadhyay et al., 2006). Its clinical spectrum ranges from mild non-specific symptoms such as nausea and fatigue to severe symptoms such as confusion, seizures and even death (Mannheimer et al., 2019). One of the most common causes of hyponatremia is drug treatment (Adrogue and Madias, 2000). Thiazides (Filippone et al., 2020; Friedman et al., 1989), antiepileptics (Falhammar et al., 2018), antipsychotics (Falhammar et al., 2019b) and several other drugs have been linked to an increased risk of severe hyponatremia (Falhammar et al., 2019a; 2020). Selective serotonin reuptake inhibitors (SSRIs) are important for the treatment of depression and anxiety, with a widespread and increasing use (De Picker et al., 2014). Evidence suggests an important time-dependent association that may be exclusively related to a more recently initiated treatment (Coupland et al., 2011; Farmand et al., 2018; Leth-Moller et al., 2016). If confirmed, this knowledge may be important to differentiate a causal relationship between SSRI treatment and severe hyponatremia from a spurious association. Furthermore, detailed knowledge on the time-course is a prerequisite for an optimal strategy and an adequate communication in order to detect SSRI-induced hyponatremia. The aim of the current study was to investigate the time-course of SSRI-associated hospitalization due to hyponatremia in the Swedish population, with a high temporal resolution.
Methods
This was a retrospective, population-based case-control study encompassing the adult Swedish population. Cases, defined as hospitalized subjects, aged 18 years or older, due to a first-ever primary diagnosis of hyponatremia (E87.1) or Syndrome of inappropriate antidiuretic hormone secretion (E22.2) between October 1, 2006 and December 31, 2014, were identified in the National Patient Register (NPR). A first ever diagnosis was defined as absence of a prior diagnosis (primary or secondary) of hyponatremia dating back to January 1, 1997. For each case, four controls without a previous diagnosis of hyponatremia were randomly identified using the Total Population Register. Controls were matched for age, sex and municipality. Each case was assigned an index date based on the date of hospital admission. For controls, the index date was defined as the index date of their matched cases. During the study period (January 1, 1997 to December 31, 2014), all diagnoses in the NPR were coded according to the International Classification of Diseases, 10th Revision (ICD-10). Concurrent and previous use of medications was identified using the Swedish Prescribed Drug Register (SPDR). The SPDR contains data on all prescribed and dispensed drugs in Sweden since July 1, 2005. Data on socioeconomic status was retrieved from the longitudinal integration database for health insurance and labor market studies register (LISA). The data collection process has been described in detail previously (Farmand et al., 2018). The study was approved by the Regional Ethical Review Board in Stockholm. Due to its retrospective epidemiological nature, no informed consent was required.
Variables
SSRI dispensations were identified by Anatomical Therapeutic Chemical (ATC) codes starting with “N06AB”, including fluoxetine, citalopram, paroxetine, sertraline, fluvoxamine and escitalopram. Drug exposure was defined as a drug dispensation <90 days prior to the index date. If the first SSRI dispensation in the 90 days period was preceded by a one-year period without SSRI dispensations, the exposure was considered new, otherwise as ongoing. New exposures were further subdivided according to how many weeks (1–13 weeks) prior to the index date they had commenced. Confounding factors accounted for in the statistical analysis included concurrent medications, socioeconomic factors and medical conditions identified using information from the NPR, the SPDR and LISA. Cardiovascular events were subdivided into those occurring within 90 days prior to the index date and older events. A complete list of exposure and confounding variables is provided in Table 1.
The definition of all factors included in the multiple logistic regression.

COPD: chronic obstructive pulmonary disease; NSAIDs: non-steroidal anti-inflammatory drugs; SSRIs: selective serotonin reuptake inhibitors.
During the 90 days before index date.
Statistical analysis
The association between SSRI exposure and hyponatremia requiring hospitalization was investigated using univariable and multivariable logistic regression. In the primary analysis, the duration of exposure to SSRIs was stratified by weeks of exposure (1–13 weeks, >13 weeks), as described above. In secondary analyses, odds ratios (ORs) were calculated for SSRI exposure regardless of duration and separated into new (0–90 days) versus ongoing.
To quantitate the disease burden and absolute risk of SSRI-associated hospitalization due to hyponatremia, adjusted ORs (aORs) were used to calculate attributable risk percentages. The attributable risk percentage is defined as the percentage of cases in a population that is attributable to the exposure of interest. This statistic indicates the percentage of cases that could theoretically be prevented by removing the exposure from the population. P-values < 0.05 were considered statistically significant. All calculations were performed using R version 3.6.1.24.
Results
During the study period, 11,213 individuals over 18 years of age were hospitalized with a principle diagnosis of hyponatremia (cases). In addition, 44,801 matched controls were included.
The majority were of female gender (72%) and the median age (range) was 76 (18–103) years. Table 2 shows a selection of medical characteristics and concurrent medications, including SSRIs, at index date among the study population. Overall, cases had more comorbidities and used more medications than controls. The most common accompanying medical conditions were previous malignant disease, ischemic heart disease and diabetes.
Medical characteristics in addition to SSRI use among cases (individuals hospitalized due to hyponatremia) and matched controls at index date.

COPD: chronic obstructive pulmonary disease; SSRI: selective serotonin reuptake inhibitor.
During the 90 days before index date.
The crude ORs (95% confidence interval (CI)) for hyponatremia among individuals exposed to SSRIs regardless of treatment duration was 2.23 (2.10–2.36). After adjustment for potential confounders, the OR was 1.22 (1.14–1.32). To further investigate the temporal association between initiation of SSRIs and hospitalization due to hyponatremia, we investigated the associations week by week (Figure 1). In general, crude ORs were higher than aORs. Individuals initiating treatment with SSRIs were exposed to an immediately increased risk for hospitalization at week 1, reaching an aOR (95% CI) of 29 (19–46). The associations then gradually declined, reaching an aOR of 2.1 (1.0–4.2) by week 13. The aOR for individuals treated for more than 13 weeks was 0.78 (0.71–0.85).
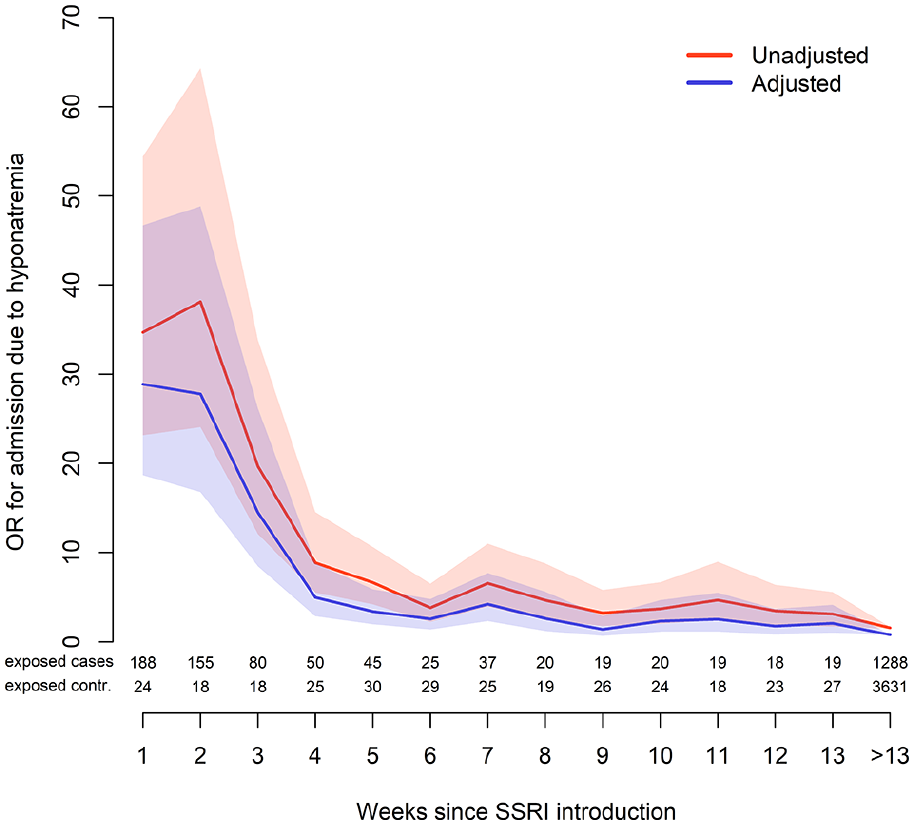
Unadjusted and adjusted ORs, accompanied with 95% CIs for hospitalization due to hyponatremia week by week.
To estimate the corresponding disease burden, we analyzed the percentage of cases that were hospitalized due to hyponatremia potentially attributed to SSRI treatment (attributable risk percentage). For individuals with any SSRI exposure the attributable risk (95% CI) was 3.2% (2.1–4.2%), indicating that 363 individuals may have been hospitalized due to a hyponatremia attributed to SSRIs over the nine-year study period.
Discussion
This is the first study specifically designed to investigate the time-course of SSRI-induced hyponatremia. It revealed an immediate dramatic increase in risk of hyponatremia sustained over the first four weeks that then gradually declined. By contrast, there was no evidence that ongoing treatment with serotonergic antidepressants increases the risk for hospitalization due to hyponatremia.
Although the association between SSRIs and hyponatremia has been known for many years, knowledge of the time-course has been insufficient (De Picker et al., 2014). Some studies have indicated a risk that is markedly higher (ORs ranging from 5 to 9) shortly after initiation as compared to ongoing treatment (Coupland et al., 2011; Gandhi et al., 2017; Leth-Moller et al., 2016). We have previously investigated the association between various antidepressants, including individual SSRIs and hospitalization due to hyponatremia. That study showed an effect that appeared to be exclusively related to newly initiated treatment (Farmand et al., 2018). For a more thorough investigation of the time-course of the risk, we have now analyzed week-by-week associations between the initiation of SSRIs and hyponatremia. Due to the greater resolution of the analysis focusing on individual weeks rather than a three-month period, as was the case in our previous paper, we now focused on SSRIs as a whole in order to reach sufficient power. Consequently, the present study was not able to inform on the risk associated with each individual substance. Although few studies have been able to compare the risk associated with individual substances, data indicate that the risk may be similar across different SSRIs (Coupland et al., 2011; Farmand et al., 2018; Gandhi et al., 2017). Also, for the reason of insufficient power, we chose not to investigate the effect of antidepressants that are less commonly prescribed in Sweden – for example, Monoamine oxidase inhibitors Tricyclic antidepressants, and Serotonin and norepinephrine reuptake inhibitors.
Results indicate an immediate and high increase in risk, sustained over the first four weeks, that then gradually declines (Figure 1). The mechanism for SSRI-induced hyponatremia has not been fully elucidated. However, animal studies point towards an underlying serotoninergic and α-adrenergic receptor mediated increase in antidiuretic hormone secretion (Brownfield et al., 1988; Leibowitz et al., 1990). We have previously presented time-dependent associations where the risk of severe hyponatremia is more pronounced in, or exclusively related to, newly initiated treatment with antihypertensive drugs (Falhammar et al., 2020), proton pump inhibitors (Falhammar et al., 2019c), opioids (Falhammar et al., 2019a) and antiepileptics (Falhammar et al., 2018). Hyponatremia following thiazide treatment may be the most well-known example that, according to experimental studies, can affect susceptible individuals within days of exposure (Filippone et al., 2020; Friedman et al., 1989). In a study with a similar setting and study design as the present one, we found that the risk for hospitalization was almost 60-fold increased during the first week of thiazide treatment and then gradually declined (Mannheimer et al., 2021). Although an increased risk for adverse effects seems plausible in the beginning of a new drug treatment, the mechanism with regard to the time-dependent risk associated with SSRIs remains unclear. This also accounts for the unexpected decreased association associated with long-term SSRI treatment. We can only speculate that factors, yet to be identified, predispose some individuals for severe hyponatremia, shortly after initiation of serotonergic treatment, resulting in a population more resilient to hyponatremia.
The study has important clinical implications. Firstly, it should prompt prescribing physicians to be attentive of symptoms consistent with hyponatremia when initiating SSRI treatment. Hyponatremia with SSRIs are known to occur among elderly females (Barber et al., 2015), as illustrated by the present study where the vast majority of cases were females (72%) with a median age of 76 years and a substantial frailty. Consequently, caution is particularly warranted among these groups of patients. Thus, even subtle symptoms occurring the first weeks after SSRI treatment initiation possibly indicating hyponatremia, should prompt measurement of sodium levels. Also important, the results of the current study support that the risk of hyponatremia is exclusively related to newly initiated treatment with SSRIs. Consequently, in patients with ongoing use of SSRI, recent onset of hyponatremia is unlikely to be coinciding with this treatment, and other causes should primarily be sought.
Finally, we found that SSRIs attributed to 3.2% of all individuals hospitalized due to hyponatremia during the study period. We have previously found that thiazides attributed to 27% of such cases (Mannheimer et al., 2021). Thus, the results further underscore drugs as a major cause of severe hyponatremia.
A major strength of the present study is its population-based design and the inclusion of all individuals with SSRI-associated hospitalizations due to hyponatremia in the Swedish population as a whole. The main limitation is the lack of available plasma sodium concentrations. However, since we only considered patients with a main diagnosis of hyponatremia, we made sure that only patients with clinically relevant hyponatremia were included. Clinically, the principal reason for hospitalization may be more adequate as compared to studies depending on hyponatremia as a secondary diagnosis, diagnoses made outside the hospital setting in the secondary or primary care (Coupland et al., 2011) or inclusion based on low sodium values, regardless of associated symptoms (Leth-Moller et al., 2016). To further motivate our study design, a validation of the principal diagnosis of hyponatremia was assessed. We found that 89% had been hospitalized mainly due to symptoms of hyponatremia. The mean plasma sodium concentration was 121 mmol/L – that is, profound hyponatremia – further emphasizing the clinical relevance of the study design (Farmand et al., 2018). Although hyponatremia as the main reason for hospitalization is a clinically relevant outcome, the focus of the current study may not include other relevant outcomes such as less severe hyponatremia. Another limitation of the present register-based study relates to the fact that adherence to oral medications is not complete in all patients. However, the most likely outcome of non-adherence is an under-estimation of the hyponatremia risk associated with SSRIs. Finally, while adjusting for a wide range of variables that may be related to hyponatremia, we cannot exclude the possibility of residual confounding.
In conclusion, this study revealed a dramatically increased risk of hyponatremia exclusively related to newly initiated treatment. Consequently, even subtle symptoms consistent with hyponatremia during the first weeks of SSRI treatment should prompt analysis of sodium levels. In patients treated with SSRIs for several months or years, other causes should primarily be sought in the event of hyponatremia.
Supplemental Material
sj-docx-1-jop-10.1177_02698811211001082 – Supplemental material for Time-dependent association between selective serotonin reuptake inhibitors and hospitalization due to hyponatremia
Supplemental material, sj-docx-1-jop-10.1177_02698811211001082 for Time-dependent association between selective serotonin reuptake inhibitors and hospitalization due to hyponatremia by Buster Mannheimer, Henrik Falhammar, Jan Calissendorff, Jakob Skov and Jonatan D Lindh in Journal of Psychopharmacology
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Jakob Skov and Buster Mannheimer report previous consultancy fees from Otsuka Pharma Scandinavia AB, outside the submitted work. No other authors had any conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The cost for retrieval, analysis and presentation of the data was funded by a clinical trial investigating the development of diabetic neuropathy (Cebix Incorporated, grant number CBX129801-DN-201) and the Stockholm County Medical Committee (grant number HSTV18048).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.