
Abstract
Introduction and objectives:
Lack of consensus regarding how best to define treatment response hinders translation from trials to the clinic. These post hoc analyses examine three commonly used response criteria in six trials of lisdexamfetamine dimesylate (LDX) in children and adolescents with attention-deficit/hyperactivity disorder (ADHD).
Methods:
Data from four short-term randomised controlled trials (RCTs) and two long-term open-label studies were analysed. Children and adolescents with ADHD received either dose-optimised (30–70 mg/day) or fixed-dose (70 mg/day) LDX. The RCTs included osmotic-release oral system methylphenidate (OROS-MPH) or atomoxetine (ATX) as a head-to-head comparator or as a reference treatment. Three definitions of response were used in these analyses: reductions of ⩾30% or ⩾50% in ADHD Rating Scale IV (ADHD-RS-IV) total score plus a Clinical Global Impressions – Improvement (CGI-I) score of 1 or 2, or an ADHD-RS-IV total score of ⩽18.
Results:
At the end point, LDX response rates for the least stringent criterion of ⩾30% reduction in ADHD-RS-IV total score plus a CGI-I score of 1 or 2 ranged from 69.6% to 82.6%. The proportion achieving the more stringent criterion of a reduction in ADHD-RS-IV total score of ⩾50% plus a CGI-I score of 1 or 2 at the end point ranged from 59.8% to 74.8%. An ADHD-RS-IV total score of ⩽18 at the end point was achieved by 56.7–79.9% of participants. Response rates remained stable throughout the long-term open-label studies.
Conclusions:
Response rates were similar for the two more stringent response criteria. The less stringent criterion resulted in higher response rates and may include partial responders.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental disorder, with an estimated prevalence of 5–7% in children and adolescents (Faraone et al., 2003; Froehlich et al., 2007; Polanczyk et al., 2007, 2015). ADHD often persists beyond childhood, with the prevalence in adults reported to be 3–5%, with some variability across countries (Fayyad et al., 2007; Simon et al., 2009). Guidelines from the European Medicines Agency (EMA) recommend that clinical trials of ADHD medications report responder analyses, as well as evaluate symptomatic outcomes at the group level, in order to understand the benefits (or otherwise) of investigational treatments better at the level of the individual participants, thus providing health-care professionals with an indication of the likelihood of success with a particular treatment regimen (European Medicines Agency, 2010).
Clinical response may be based on improvements in symptom scales such as the ADHD Rating Scale IV (ADHD-RS-IV; DuPaul et al., 1998), the Swanson, Nolan and Pelham version IV (SNAP-IV; Bussing et al., 2008; Swanson et al., 2001) and the Conners’ Parent Rating Scale-Revised (Conners et al., 1998), with or without a Clinical Global Impressions – Improvement (CGI-I) score of 1 (very much improved) or 2 (much improved; Banaschewski et al., 2014; Busner and Targum, 2007; Coghill et al., 2013; Dittmann et al., 2013, 2014; Soutullo et al., 2013; Steele et al., 2006). However, there is currently no clear consensus on appropriate thresholds for a clinically meaningful response using these instruments. Thresholds that have been used include a CGI-I score of 1 or 2, either alone or in combination with a decrease in ADHD-RS-IV total score of at least 25% for a partial response or more than 50% for a more robust response (Biederman et al., 2007; Coghill et al., 2013, 2017; Dittmann et al., 2014, 2013; Findling et al., 2010, 2011, 2013; Jain et al., 2011; Mattingly et al., 2013). Some investigators argue that symptom score in responders should be within the range for unaffected individuals. To this end, a 65% reduction in symptom scale score has been proposed (Buitelaar et al., 2009), as has an ADHD-RS-IV total score at the end point of ⩽18 – a score considered by some to represent symptom remission on treatment (Coghill and Seth, 2015; Soutullo et al., 2013).
To inform the selection of response thresholds, we compared post hoc response rates from a series of late-phase clinical trials of different designs that evaluated lisdexamfetamine dimesylate (LDX), the long-acting prodrug of amphetamine, in children and adolescents with ADHD. Several of the studies included active controls, either as a head-to-head comparator or as a reference arm. The evaluation of response was based on three different response criteria: a decrease of at least 30% in combination with a CGI-I score of 1 or 2; at least a 50% reduction in ADHD-RS-IV total score in combination with a CGI-I score of 1 or 2; and an ADHD-RS-IV total score of ⩽18 at the end point.
Methods
Ethics
All studies were conducted in accordance with current applicable international and national regulations and ethical requirements. For all studies, each participant’s parent or legally authorised guardian provided informed consent, and each participant provided assent if applicable.
Study designs
These post hoc analyses were based on six studies: four randomised controlled trials (RCTs) (SPD489-325, SPD489-317, SPD489-405 and SPD489-406) and two open-label (OL) studies of LDX (SPD489-326 and SPD489-404). Osmotic-release oral system methylphenidate (OROS-MPH) was used as a head-to-head comparator in SPD489-405 and SPD489-406, and as a reference arm in SP489-325. Atomoxetine (ATX) was included as a head-to-head comparator in SPD489-317. The study designs are summarised in Table 1. Further details are provided in the online Supplemental Material, and the full methods have been published previously (Coghill et al., 2013, 2014, 2017; Dittmann et al., 2013; Newcorn et al., 2017). These six studies were selected because these were recent studies that all included the same response measures that could be used for post hoc analyses.
Overview of studies included in the responder analyses.
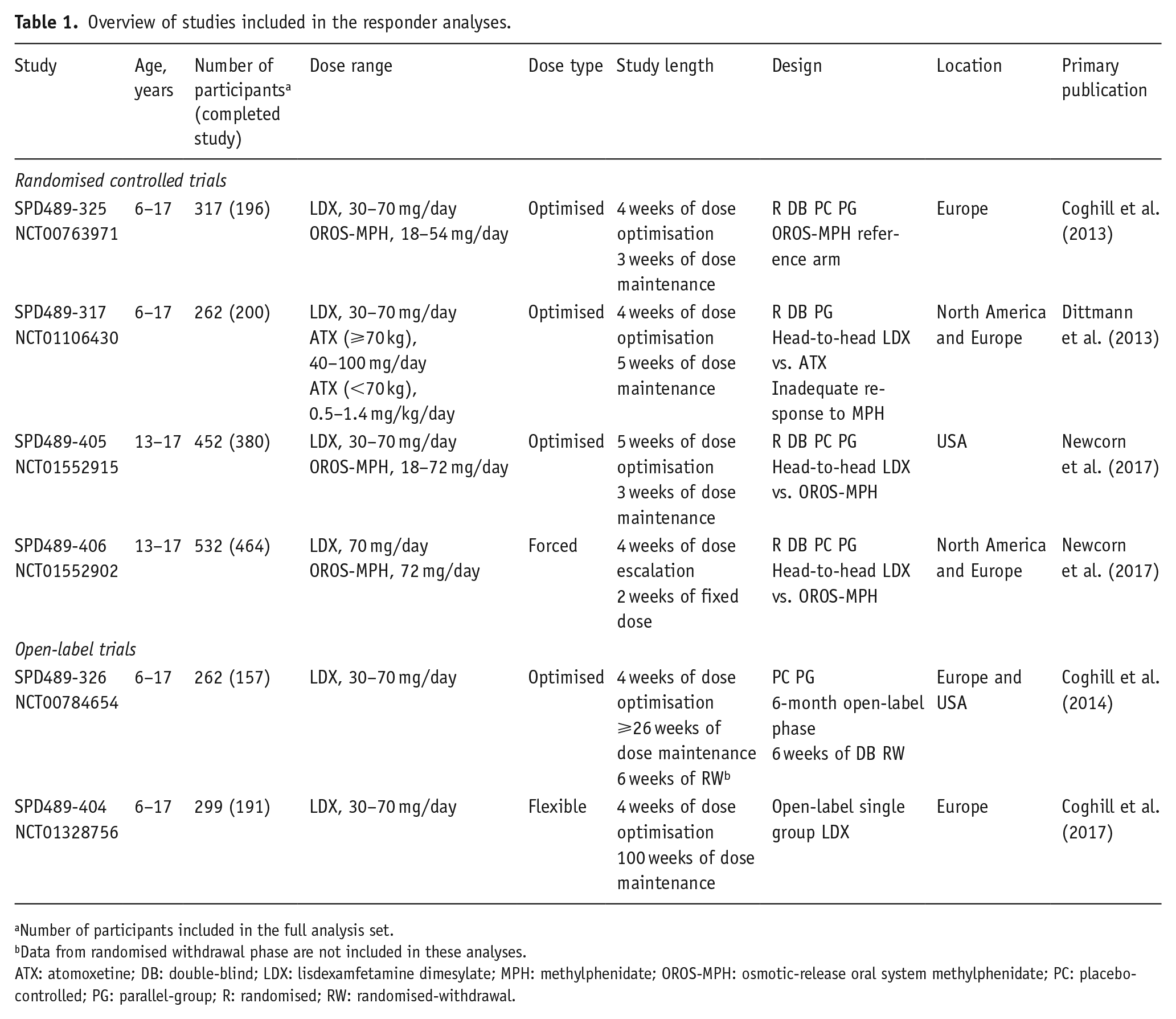
Number of participants included in the full analysis set.
Data from randomised withdrawal phase are not included in these analyses.
ATX: atomoxetine; DB: double-blind; LDX: lisdexamfetamine dimesylate; MPH: methylphenidate; OROS-MPH: osmotic-release oral system methylphenidate; PC: placebo-controlled; PG: parallel-group; R: randomised; RW: randomised-withdrawal.
Measure of response
Response was defined according to three criteria: a reduction from baseline to the end point of at least 30% in ADHD-RS-IV total score in combination with a CGI-I score of 1 (very much improved) or 2 (much improved); a reduction from baseline to the end point of at least 50% in ADHD-RS-IV total score in combination with a CGI-I score of 1 or 2; and an ADHD-RS-IV total score of ⩽18 at the end point.
Statistical analysis
Analyses were based on the full analysis set for each study. This included all participants who were randomised and received at least one dose of any investigational drug. Missing data were handled using the last observation carried forward method. Data from baseline measures were never carried forward into the treatment phase. Participants who had only a baseline assessment and did not have any valid post-baseline data were excluded from the analyses. Proportions of responders were calculated for each treatment, with 95% confidence intervals. No direct statistical comparisons of treatment response were made between investigational drugs.
Results
Participant disposition and characteristics
In total, 1823 participants received at least one dose of an investigational drug in the six studies and were included in the full analysis set. The LDX group comprised 1181 participants (six studies), the OROS-MPH group comprised 507 participants (three studies) and the ATX group comprised 135 participants (one study). After excluding individuals with no valid post-baseline data, responder analyses based on at least a 30% and at least a 50% reduction from baseline to the end point in ADHD-RS-IV total score included 1809 participants (LDX, n=1171; OROS-MPH, n=506; ATX, n=132); analyses of patients achieving an ADHD-RS-IV total score of ⩽18 at the end point included 1818 participants (LDX, n=1178; OROS-MPH, n=507; ATX, n=133). Baseline characteristics are reported in Table 2. Mean ADHD-RS-IV total scores at baseline were 40.5–42.6 across all treatment groups in the four studies that involved children and adolescents, and 36.6 and 37.8 in the two adolescent-only studies. LDX was generally well tolerated across studies, and all safety results have been published in detail previously (Coghill et al., 2013, 2014, 2017; Dittmann et al., 2013; Newcorn et al., 2017).
Baseline demographics and participant characteristics in the full analysis set.
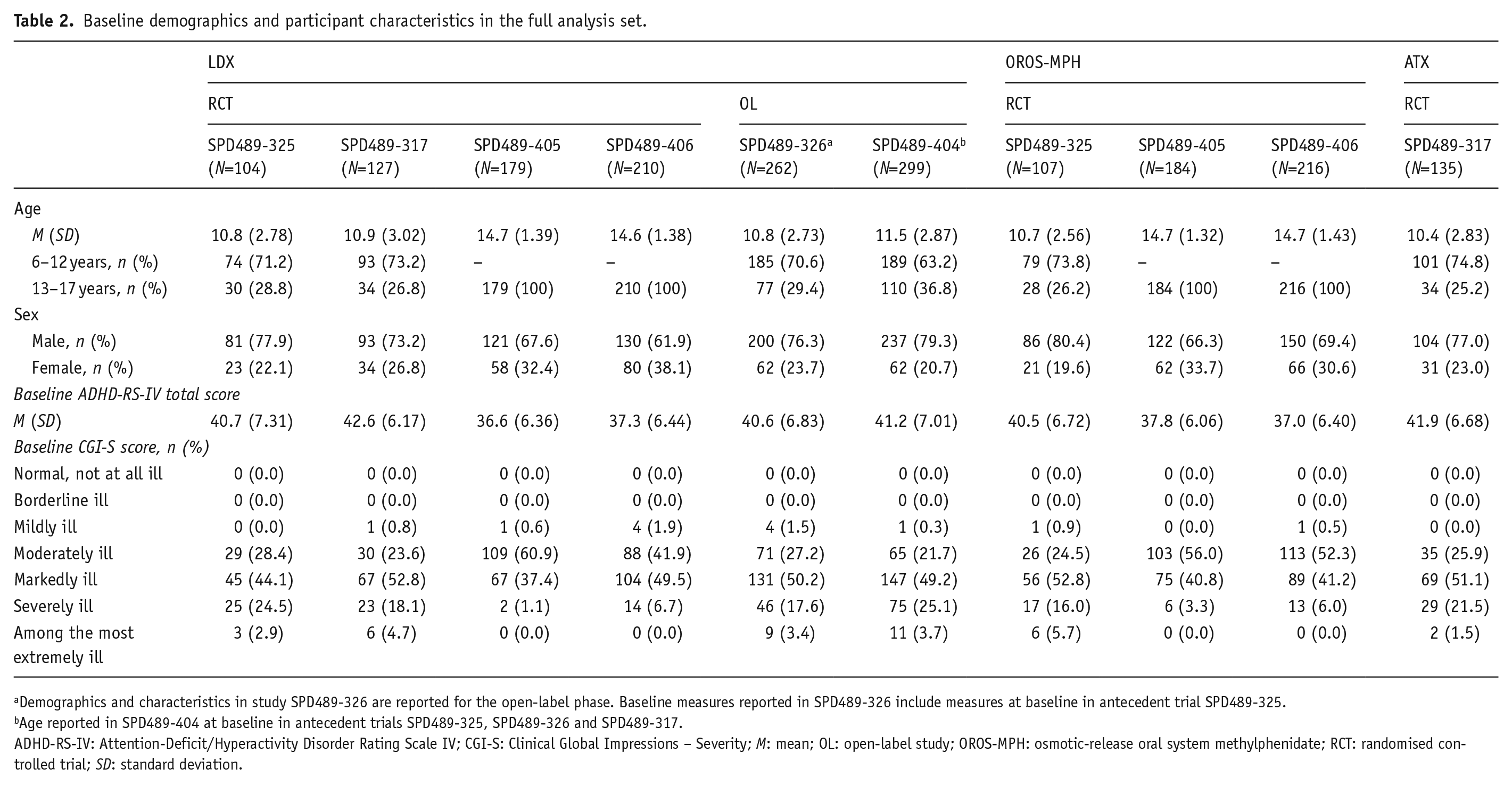
Demographics and characteristics in study SPD489-326 are reported for the open-label phase. Baseline measures reported in SPD489-326 include measures at baseline in antecedent trial SPD489-325.
Age reported in SPD489-404 at baseline in antecedent trials SPD489-325, SPD489-326 and SPD489-317.
ADHD-RS-IV: Attention-Deficit/Hyperactivity Disorder Rating Scale IV; CGI-S: Clinical Global Impressions – Severity; M: mean; OL: open-label study; OROS-MPH: osmotic-release oral system methylphenidate; RCT: randomised controlled trial; SD: standard deviation.
Responder analysis
In the RCTs, the proportion of participants receiving LDX who achieved a reduction in ADHD-RS-IV total score of at least 30% with a CGI-I score of 1 or 2 at the end point ranged from 69.6% to 82.6%; the proportion achieving the more stringent criterion of a reduction in ADHD-RS-IV total score of at least 50% with a CGI-I score of 1 or 2 at the end point ranged from 59.8% to 74.8% (Table 3).
Proportions of responders for LDX and comparators at the end point.
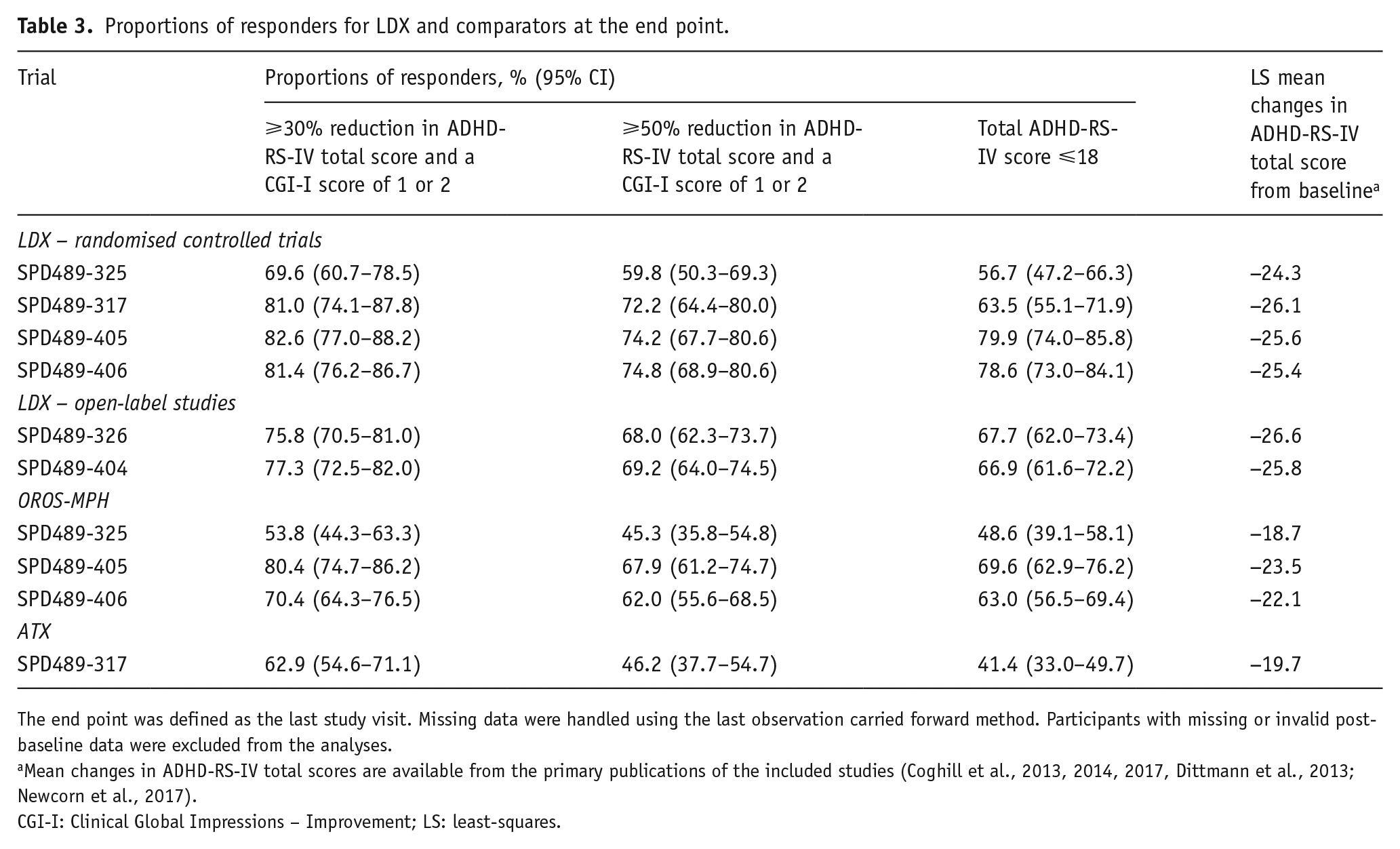
The end point was defined as the last study visit. Missing data were handled using the last observation carried forward method. Participants with missing or invalid post-baseline data were excluded from the analyses.
Mean changes in ADHD-RS-IV total scores are available from the primary publications of the included studies (Coghill et al., 2013, 2014, 2017, Dittmann et al., 2013; Newcorn et al., 2017).
CGI-I: Clinical Global Impressions – Improvement; LS: least-squares.
In the OL studies, the response rate for a reduction in ADHD-RS-IV total score of at least 30% with a CGI-I score of 1 or 2 at the end point was at least 75%, and almost 70% achieved a reduction in ADHD-RS-IV total score of at least 50% with a CGI-I score of 1 or 2 at the end point (Table 3).
The proportions of participants receiving LDX who achieved an ADHD-RS-IV total score of ⩽18 at the end point ranged from 56.7% to 79.9% in the RCTs, and were 67.7% and 66.9% in the OL studies (Table 3).
The proportion of participants receiving OROS-MPH who achieved a reduction in ADHD-RS-IV total score of at least 30% plus a CGI-I score of 1 or 2 ranged from 53.8% to 80.4%, and was 62.9% for ATX (Table 3). The more robust response threshold of a reduction in ADHD-RS-IV total score of at least 50% and a CGI-I score of 1 or 2 was achieved by 45.3–67.9% of participants receiving OROS-MPH and by 46.2% of those receiving ATX (Table 3). An ADHD-RS-IV total score of ⩽18 was achieved by 48.6–69.6% of participants receiving OROS-MPH and 41.4% of those receiving ATX (Table 3).
In the RCTs and OL studies, response rates for all criteria increased during dose optimisation and escalation, and remained stable for the remainder of the trials – for up to two years in SPD489-404 (Figure 1). In the RCTs, response rates (all criteria) for OROS-MPH and ATX also increased during dose optimisation and escalation, and remained stable for the remainder of the trials (Figure 2).
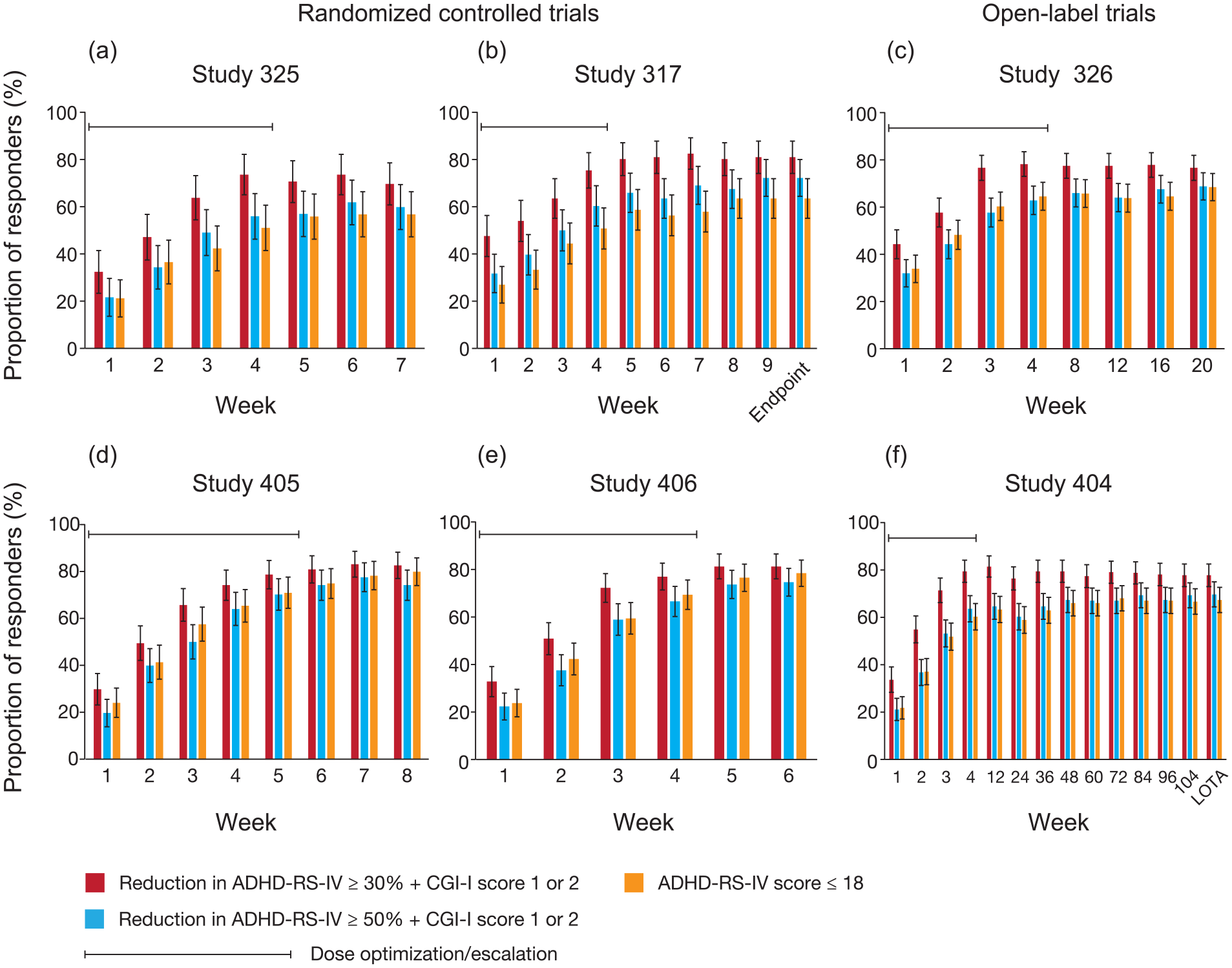
Time course of response rates to LDX across all studies. ADHD-RS-IV: Attention-Deficit/Hyperactivity Disorder Rating Scale IV; CGI-I: Clinical Global Impressions – Improvement; LDX: lisdexamfetamine dimesylate; LOTA: last on-treatment assessment. Data are based on the full analysis set using last observation carried forward. Participants without any valid post-baseline data were excluded from these analyses. The proportion of responders at each visit is shown for the randomised controlled trials in (a) SPD489-325, (b) SPD489-317, (d) SPD489-405 and (e) SPD489-406, and for the open-label studies in (c) SPD489-326 and (f) SPD489-404.
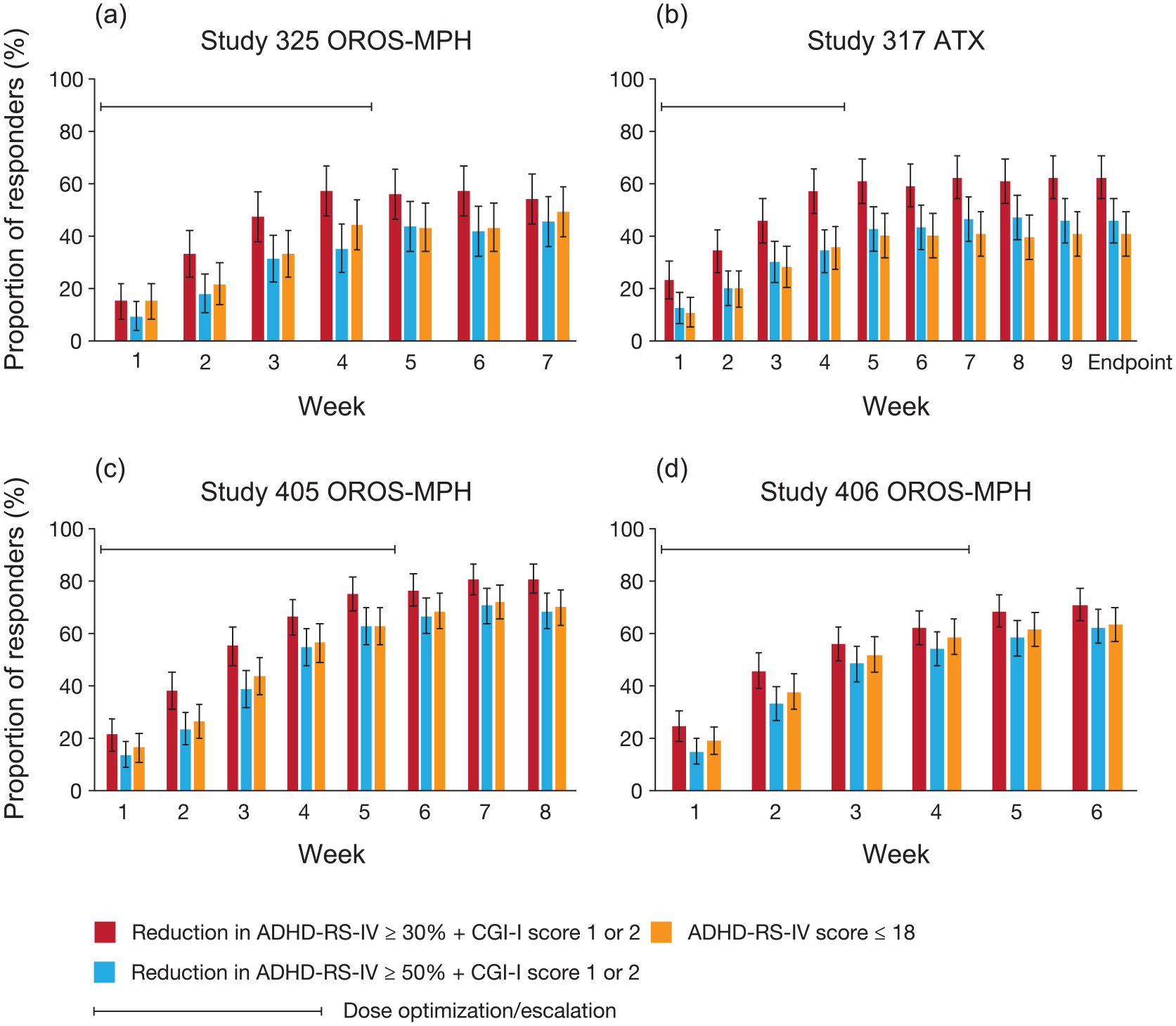
Time course of response rates to ATX and OROS-MPH across the four randomised controlled trials. ADHD-RS-IV: Attention-Deficit/Hyperactivity Disorder Rating Scale IV; ATX: atomoxetine; OROS-MPH: osmotic-release oral system methylphenidate. Data shown are based on the full analysis set using last observation carried forward. Participants without any valid post-baseline data were excluded from these analyses. The proportion of responders to OROS-MPH at each visit is shown for (a) SPD489-325, (c) SPD489-405 and (d) SPD489-406. The proportion of responders to ATX at each visit is shown for (b) SPD489-317.
Discussion
To provide an estimate of the clinical impact of treatment on individual patients, the EMA recommends that clinical trials evaluate the proportion of responders based on symptom improvement in combination with functional improvements (European Medicines Agency, 2010). Therefore, we evaluated treatment response across six clinical trials of LDX in children and adolescents with ADHD, using three different criteria. The observed response rates for LDX for the criterion of at least a 30% decrease in ADHD-RS-IV total score plus a CGI-I score of 1 or 2 was higher than for the more stringent thresholds of at least a 50% decrease in ADHD-RS-IV total score plus a CGI-I score of 1 or 2, or an ADHD-RS-IV total score of ⩽18 at the end point. Response rates for LDX were similar across RCTs and, based on OL studies, were stable for up to two years. Although less extensive, the available data suggest similar rank orders in responder rates for the comparators OROS-MPH and ATX, with the highest proportion of responders observed for the least strict response criterion.
The proportions of participants in the RCTs achieving a reduction of at least 30% in ADHD-RS-IV total score in combination with a CGI-I score of 1 or 2 at the end point ranged from approximately 70% to 83% for participants receiving LDX. These response rates are similar to those previously reported using the same criterion (Findling et al., 2010; Jain et al., 2011; Mattingly et al., 2013) but are lower than those observed when response was defined as a CGI-I score of 1 or 2 only (Biederman et al., 2007; Findling et al., 2011, 2013). As would be expected, smaller proportions of participants achieved the more stringent response criterion of a reduction of at least 50% in ADHD-RS-IV total score plus a CGI-I score of 1 or 2, and similar proportions of participants achieved symptom scores within the range of unaffected individuals (i.e. ADHD-RS-IV score of ⩽18).
LDX treatment in the RCTs and OL studies included in these post hoc analyses resulted in group mean reductions in ADHD-RS-IV total score of about 25 points (range 24.3–26.6 points) from baseline scores of about 40 points (range 36.6–42.6 points; Coghill et al., 2013, 2014, 2017; Dittmann et al., 2013; Newcorn et al., 2017). This reduction equates to a decrease of about 63%, and would result in an average ADHD-RS-IV total score within the range of unaffected individuals (i.e. a score of ⩽18 points). Despite this substantial and highly statistically significant decrease in mean ADHD-RS-IV score, the present data indicate that a sizeable minority of participants (⩾17.4%) did not meet any of the defined response criteria. Thus, by enabling the evaluation of the clinical impact of a treatment in individual patients, response rates provide distinct but complementary information about treatment efficacy in addition to mean changes in symptom scale scores.
An important consideration when using proportional reductions in symptom scales as a measure of treatment response is that the score at the end point depends on the score at baseline. It has been shown that patients with higher symptom severity at baseline tend to have a larger response to immediate-release MPH than patients with lower symptom severity at baseline (Victor et al., 2014). However, an individual with the maximum ADHD-RS-IV total score of 54 at baseline would still experience significant symptoms at the end point, despite a 50% reduction in score. Rather than a proportional reduction in symptom score, it has therefore been argued that achieving symptom scale scores within the range of unaffected individuals (ADHD is considered unlikely if the ADHD-RS-IV total score is ⩽18 for the combined subtype; Coghill and Seth, 2015) should be the target of treatment (sometimes termed symptom remission on treatment; Steele et al., 2006). Achieving an ADHD-RS-IV total score of ⩽18 will be more difficult for individuals with a high baseline score because they will need to achieve a larger improvement than individuals with lower scores. Choosing a realistic target for treatment response may also inform the choice of response criterion that will be used in a clinical setting. An ADHD-RS-IV total of ⩽18 may not always be achievable, in which case a percentage reduction in ADHD-RS-IV total score plus a CGI-I score of 1 or 2 may be the more appropriate criterion.
In the RCTs included in the present analyses, the proportions of LDX-treated participants who achieved an ADHD-RS-IV total score of ⩽18 (57–80%) were similar to previously reported values (Findling et al., 2010; Mattingly et al., 2013), and were generally lower than the proportion achieving at least a 30% decrease in ADHD-RS-IV total score plus a CGI-I score of 1 or 2, but broadly similar to response rates based on at least a 50% reduction from baseline in ADHD-RS-IV total score plus a CGI-I score of 1 or 2.
The increase in response to LDX in RCTs occurred largely during dose optimisation/escalation, mirroring the time course of the mean change from baseline in ADHD-RS-IV total scores previously reported for these trials (Coghill et al., 2013, 2017; Dittmann et al., 2013; Newcorn et al., 2017). Similar maximum response levels to those observed in the RCTs were observed in the OL studies, and mean response rates remained stable for up to two years. Whereas the longitudinal analyses of response in the OL studies provide no information about whether the proportion of responders at each time point comprise the same individuals, a previous one-year OL study of LDX in children with ADHD found that 96% of participants who completed dose optimisation met the clinical response criteria (a decrease of at least 30% in ADHD-RS-IV total score plus a CGI-I score of 1 or 2) at one or more visits, and about 63% met the criteria at each subsequent visit (response maintenance; Findling et al., 2010). Similarly, in a one-year OL study of LDX in adults with ADHD, more than 95% of participants met the response criteria at least once, with 75% meeting the criteria at all subsequent visits (Mattingly et al., 2013). It should be noted that treatment response is reliant on continuous treatment, and a randomised withdrawal trial of LDX has shown that symptoms return after treatment cessation (Coghill et al., 2014).
We did not attempt to compare responses between LDX and either OROS-MPH or ATX, which were included in the RCTs here as either a head-to-head comparator or a reference treatment. For completeness, results are reported for these head-to-head comparators and reference treatments when they were included in studies. It should be noted that each trial was designed and optimised to investigate the efficacy and safety of LDX rather than the comparators. Nevertheless, the rank orders of response to OROS-MPH and ATX based on each of the response criteria were similar to those observed with LDX, with the highest proportion of responders found for a reduction in ADHD-RS-IV total score of at least 30% in combination with a CGI-I score of 1 or 2. Published response rates for OROS-MPH based on this criterion (62% and 66%) are within the range of response rates found in the present analyses (Biederman et al., 2006, 2010). Likewise, published values for the proportions of OROS-MPH-treated participants who achieved symptom remission based on SNAP-IV scores (69.3% and 73.2%) are similar to the proportions of participants in the present analyses who achieved an ADHD-RS-IV total score of ⩽18 at the end point (Su et al., 2015). With regard to ATX treatment, the proportion of participants achieving at least a 30% reduction in ADHD-RS-IV total score plus a CGI-I score of 1 or 2 in the present analyses was similar to the 60% who achieved a 25% reduction in ADHD-RS-IV total score in a large retrospective study (1069 patients) that investigated predictive factors for response to ATX (Newcorn et al., 2009).
The strengths of these post hoc analyses are the large number of participants for whom data were analysed and the relatively consistent results across several clinical trials. However, several factors should be considered when interpreting these data. First, the inclusion criteria and design differed between trials, and so data could not be pooled. Specifically, the differences in maximum doses of OROS-MPH across studies (maximum of 54 mg/day in Europe and 72 mg/day in the USA and Canada) are an important limitation because it has been established that many patients need more than 54 mg/day. Second, the OROS-MPH and ATX data sets were smaller than that for LDX, and the included trials were designed and powered to investigate LDX rather than comparator medications. So, direct comparisons of responder rates for the different treatments were not possible. It should also be noted that not all participants completed the trials they were in. There are caveats with using a last observation carried forward method, and maintenance of treatment response should be considered carefully in light of this methodology. Finally, with response based on ADHD-RS-IV and CGI-I scores, the present data largely focus on symptomatic improvement rather than on treatment efficacy (Adamo et al., 2015). The importance of including non-symptomatic outcome measures in clinical trials of ADHD medications is increasingly recognised (Wong et al., 2019). Unfortunately, such measures are not yet consistently applied to clinical trials of ADHD medications, and appropriate functional and health-related quality-of-life response thresholds have yet to be agreed.
In summary, the present post hoc analyses compared three different commonly used definitions of treatment response in six clinical trials of LDX in children and adolescents with ADHD. The results indicate that treatment with LDX and the comparator medications, OROS-MPH and ATX, all resulted in high response rates that are consistent across different study designs and populations. Further, there is no evidence to suggest that specific response criteria favour the different treatments. Response rates were higher for a ⩾30% reduction from baseline in ADHD-RS-IV total score plus a CGI-I score of 1 or 2 than for a ⩾50% reduction in ADHD-RS-IV total score plus a CGI-I score of 1 or 2 and an ADHD-RS-IV total score of ⩽18, suggesting that the first criterion is a measure of partial response in these six clinical trials, at least in some individuals. Based on these findings, it should be possible to reach a significant improvement in approximately 60% (ATX) to 80% (LDX and OROS-MPH) of patients and – more importantly – to achieve substantial improvement or symptom scores within the range of unaffected individuals in around 2/5 (ATX) and 2/3 (LDX and OROS-MPH) patients. Therefore, the stricter response criteria may be more appropriate in a clinical setting when aiming to find the optimal response for patients compared to the less strict criterion, even if this may be difficult to achieve in routine clinical practice. Symptom severity at baseline should of course be considered when assessing improvement in relation to symptom reduction scores. For example, an individual with a particularly high baseline score will find it challenging to achieve the lowest possible absolute score. Consistent use of response rate criteria is required to understand treatment response better at the level of the individual.
Supplemental Material
Supplementary_methods – Supplemental material for Post hoc analyses of response rates to pharmacological treatments in children and adolescents with attention-deficit/hyperactivity disorder
Supplemental material, Supplementary_methods for Post hoc analyses of response rates to pharmacological treatments in children and adolescents with attention-deficit/hyperactivity disorder by David R Coghill, Jeffrey H Newcorn, Jie Chen, Tamara Werner-Kiechle and Tobias Banaschewski in Journal of Psychopharmacology
Footnotes
Acknowledgements
We thank the participants and investigators involved in the studies. This post hoc analysis and the six original studies were funded by the sponsor, Shire Development LLC, a member of the Takeda group of companies. Under the direction of the authors and funded by Shire International GmbH, a member of the Takeda group of companies, Dr TJ van Hartevelt and Dr E Southam of Oxford PharmaGenesis provided writing assistance for this publication. Editorial assistance in formatting, proofreading, copy editing and fact checking was also provided by Oxford PharmaGenesis. Although employees of the sponsor were involved in the study design, data collection, analysis and interpretation, and fact checking of information, the content of this manuscript, the interpretation of the data and the decision to submit the manuscript for publication in Journal of Psychopharmacology was made by the authors independently.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J Chen and T Werner-Kiechle are employees of Shire, a member of the Takeda group of companies and own Takeda stock/stock options. The following authors have received compensation for serving as consultants or speakers for the companies or organisations indicated, or they or the institutions they work for have received research support or royalties: T Banaschewski (Actelion, Hexal Pharma, Lilly, Lundbeck, Medice, Neurim Pharmaceuticals, Novartis, Shire [a member of the Takeda group of companies] and Vifor Pharma); DR Coghill (Eli Lilly, Janssen-Cilag, Medice, Novartis, Oxford University Press and Shire [a member of the Takeda group of companies]); JH Newcorn (Akili Interactive, Alcobra, Cingulate Therapeutics, Enzymotec, Medice, National Football League, NLS, Pfizer, Rhodes, Shire [a member of the Takeda group of companies], Sunovion and Supernus).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.