
Abstract
Globally, there has been a significant rise and diversification in fraud that is targeting individual members of the public. Research evidence has shown that victims suffer harm as a consequence of fraud victimisation. However, few studies have focused on how fraud impacts on victim health, despite the importance of health in policy assessments and the design of victim support services. Furthermore, there are conceptual questions on how to operationalise and assess ‘impact’ as it is subjectively experienced by different victims. Using survey data collected from 311 victims of fraud in the United Kingdom, this study uses quantitative and qualitative analyses to explore the health impact of fraud from three perspectives: the type, composition and intensity of health symptoms that are experienced; the wider impact of these on the lives of victims; and the capacity of victims to cope or recover from the experience. The research shows that most victims experience a health symptom (most commonly emotional or psychological), but the profile, intensity, and impact on wider life is highly variable. In addition, a cohort of victims reported symptoms over longer time periods and a significant minority had wanted support or treatment to address the impact on their health. The implications of these findings for further research and policies are discussed.
Keywords
Introduction
Fraud has become one of the most common crimes in many countries (UNODC, 2024). A recent cross-country comparison of 15 countries found that fraud victimisation among the adult population in the years 2021–2023 ranged from 31% in the United States to 8% in Japan, with another 9 countries experiencing victimisation rates above 20%. This amounts to 228 million victims over the duration of the study or 76 million per year (Hyde and Gibson, 2024). There has been a growing number of studies exploring the impact of fraud on individual victims (Button et al., 2014; Cross, 2015, 2016; Hyde and Gibson, 2024). These studies have illustrated the extensive effects fraud generates beyond the financial, including impacts on emotions, relationships, changes in behaviour and various health problems. The health impacts of fraud have not been explored in depth and given there is an evidence base of other crimes impacting on the health of victims, this represents a gap in our knowledge (Hanson et al., 2010; Tan and Haining, 2016).
Frauds (or scams as some use to describe such behaviours) are united by the use of deception to cause a loss to the victim without physical force (Tun and Birks, 2023). They encompass a wide range of forms, from romance frauds, shopping frauds, investment frauds, to credit card frauds to name some of the most common. The impact of fraud is significant, it is crime that has been growing and costs to individual victims are estimated to be £4.7 billion each year, the highest of any property crime targeting the public (Heeks et al., 2018). The impact of fraud is often viewed in terms of this financial detriment and often falls short of accounting for the impact on victims’ health and well-being (Which?, 2021). Understanding the gravity of crime in terms of its impact on victims is increasingly important to guiding policy decisions and jurisprudence in criminal justice systems (Johnston et al., 2018; Paoli and Greenfield, 2018). Moreover, many public authorities have a duty to deliver support services, including emotional and psychological support (e.g. see European Union (EU) Directive 2012/29/EU), and effective and efficient provision of services relies on a clear understanding of victim need.
This study seeks to better develop our understanding of the nature of the health impact on fraud victims. The research is exploratory in nature and seeks to address the following core questions. What are the health symptoms experienced by fraud victims? What is the composition (or profile) of health symptoms experienced by different fraud victims? How are these health symptoms associated with victims’ daily lives and their requirement of support to recover from the experience? This paper will begin by conducting a brief literature review, then explore the methods used before presenting the findings. The paper will end with a discussion and conclusion.
Accounting for the impact of fraud
The health impact is a key dimension of the harm that is caused by crime, and accounting for ‘harm’ is increasingly important to guiding public policies (Greenfield and Paoli, 2013). In seeking to assess the health impact of fraud, a key challenge is to differentiate the subjective reports of impact by different fraud victims. Criminologists and economists have developed standardised frameworks to produce aggregated assessments of the impact of different types of crime; examples include the ‘quality of adjusted life’ (or QALY), ‘life satisfaction’ or ‘standard of living’ (Dolan et al., 2005; Greenfield and Paoli, 2013; Johnston et al., 2018). In these models, the impact on psychological and physical health is subsumed into broader assessments of detriment to ‘wellbeing’; other factors include the impact on finance, relationships, or role functioning (e.g. social or occupation: Hanson et al., 2010; HM Treasury and Social Impacts Taskforce, 2021). There are few studies which have examined the impact of fraud on victim well-being. Sarria et al. (2019) found the economic impact of fraud was significantly associated with a person reporting difficulty in daily life, limited social activities due to health, feelings of chronic pain, being disturbed by negative feelings, and reporting an overall worse quality of life. A study which used the QALY framework to measure the economic and social cost of all crime in the United Kingdom calculated the emotional health cost of fraud to be among the lowest of all crimes included, and the physical health costs were estimated to be zero (Heeks et al., 2018). This low estimate is likely to reflect the limited knowledge and evidence on the health impact of fraud.
These frameworks focus on the ‘standard’ effect on victims because individualised victim assessments and the particularities of criminal acts are too diverse to be accommodated by broad-based assessments (Von Hirsch and Jareborg, 1991). In measuring the ‘standard’ effect, fraud victims are treated as a discrete category of victim to be compared with victims of other categories of crime (e.g. burglary victims). This has several implications for understanding the impact of fraud. First, there is a history of under-estimating the impact on individual victims. Indeed, there are victimology studies that stress the point that fraud is neither a ‘victimless crime’ nor a ‘laughing matter’ (Button et al., 2014, 2021; Cross, 2015). Second, fraud is a high-volume crime and victims report a wide spectrum of experiences and impact. This is illustrated by the crime survey in England and Wales (Office for National Statistics (ONS), 2020) in which a third of victims reported being very affected (10%) or affected quite a lot (23%), whereas one in five (22%) reported not being emotionally affected by the experience (see Button et al., 2021). Finally, as a crime category fraud encompasses an expansive range of criminal behaviours, bound together by the common principle of dishonesty (Beals et al., 2015; UNODC, 2024). And with this range of behaviours there are discrete fraud methodologies that have been shown to provoke severe emotional responses from victims (Modic and Anderson, 2015; Skidmore et al., 2020). A key example is victims of romance fraud, who experience significant emotional distress as a consequence, including the grief of losing an important relationship (Whitty and Buchanan, 2016).
There are many victims who experience an emotional response to a crime and fraud is no exception (Dinisman and Moroz, 2017). One key mediating influence is the ability to cope or adapt to the victimisation experience, and a longer-term effect indicates a greater impact on a victim’s health (Johnston et al., 2018). In this frame, ‘impact’ can be depicted as the level of victim ‘need’ to help them recover emotionally, psychologically, and/or physically. This is mediated by multiple factors beyond the particularities of the fraud, including the personal circumstances of the victim, for example, the degrees of self-blame, the availability of social networks and support, a pre-existing mental and/or physical health condition, and the capacity to recover financially from the loss of money (Buchanan and Whitty, 2014; Button et al., 2014; Cross, 2016; DeLiema et al., 2021). ‘Vulnerability’ assessments provide a means to account for the needs of victims and guide the provision of support services (Bartkowiak-Theron and Asquith, 2015). However, in the context of fraud and cybercrime, vulnerability assessments have often been oriented to crime reduction objectives, such as to address the risk of repeat victimisation, instead of restorative objectives to help a victim recover from the harm they have experienced (Correia, 2021; Skidmore et al., 2020).
A defining characteristic of fraud is the use of deception to trick victims into voluntarily parting with their money without recourse to physical force or coercion (see Tun and Birks, 2023). The active role that some victims play in the fraud can lead to self-blame or being blamed by others, which can influence the emotional response to the incident (Cross, 2015; Sorell and Whitty, 2019). Many fraud victims report experiencing an emotional or psychological response; a survey by the European Commission found that 79% of victims of fraud and scams suffered ‘emotionally’ and 6% suffered ‘physically’ (European Commission, 2020). In self-report studies, emotional responses (with variable intensity) include anger, frustration, shock, stress, anxiety, shame, embarrassment, fear, sadness, and loss of confidence (Button et al., 2014, 2025; Cross et al., 2016; Cullina et al., 2014; Nguyen et al., 2021). Research also shows that fraud can lead to an inability to trust people, relationship difficulties, time off work, and in a minority of cases, attempting or committing suicide (Button et al., 2014; Cullina et al., 2014; Ross and Smith, 2011; Watson et al., 2019).
The emotional and psychological effect of a financial loss can also lead to somatic symptoms that deteriorate physical health. Following a fraud, some victims reported physiological effects such as difficulty sleeping, nausea, weight loss, and skin conditions (Button et al., 2014; Cross et al., 2016; Kerr et al., 2013; Watson et al., 2019). In one study, male victims who experienced a severe economic impact were more likely to report adverse health symptoms in the longer term than non-victims; this includes the presence of two or more chronic conditions such as high blood pressure, cardiovascular conditions, respiratory or skin diseases, and/or the presence of at least one pain condition such as chronic back pain, frequent migraines, or headaches (Sanz-Barbero et al., 2020). Fraud victimisation has also been shown to exacerbate pre-existing health conditions such as eczema, Crohn’s disease, or depression, to name some, through the stress caused (Button et al., 2021; Cross et al., 2016).
The current study
The current research seeks to develop our understanding of the nature of the health impact on fraud victims. It builds on earlier work by providing a contemporary picture of a crime that has changed dramatically (and continues to evolve) in response to the Internet revolution and the growth of cybercrime (see Button and Cross, 2017). Furthermore, this research takes a cross-sectional view of victims of all fraud types to examine the breadth of victim experience. The research is exploratory in nature and seeks to address the following core questions:
What are the health symptoms experienced by fraud victims?
What is the composition (or profile) of health symptoms experienced by different fraud victims?
How are these health symptoms associated with victims’ daily lives and their requirement of support to recover from the experience?
Method
The current study builds on prior research by analysing the relationship between the different reported health symptoms to develop a more holistic perspective on the health impacts experienced by victims. Previous research used quantitative survey analysis to identify cohorts of victims who experience fraud differently but adopted a more generalised perspective of ‘vulnerability’ which incorporated indicators for the impact on health (Poppleton et al., 2021).
This study adopted a mixed methods approach to examine the impact of fraud on the health of victims. This included a quantitative analysis of victim responses to a survey on the health impact of fraud, and qualitative analysis of data collected from open-ended responses in a victim survey. Ethical approval was granted from the University of Portsmouth (FHSS 2024-005). Qualitative data is used to contextualise and add descriptive detail on the experiences of victims, the reasons for experiencing a health impact, and their implications for other aspects of daily life and the type of support that was required.
Victim health survey
A survey was designed to explore the nature of the health impact experienced by fraud victims. As the survey was disseminated to potentially vulnerable individuals, to further ensure anonymity of responses it was decided that demographic information would not be collected. Participants first read a participant information sheet and signed a consent form online.
Participants were then asked to select from a list of health symptoms they had experienced as a result of becoming a victim of fraud. These symptoms were compiled based on a review of the published research evidence through the following two approaches. First the types of symptoms included reflected the reported experiences and impacts documented in the existing criminology/victimology literature, specifically that relating to fraud and cybercrime. Second, the questions were also designed to explore a range of theorised dimensions of ‘impact’ taken from victimology and health research – that is, impact as a function of intensity and duration (Dignan, 2005), the capacity to cope and recover (Johnston et al., 2018), or the effect that symptom has on the victim’s wider well-being and quality of life (Heeks et al., 2018) – these principles also informed the thematic analysis of the data.
Victims were presented with three categories of health symptom: emotional or mental health symptoms (20 symptoms), physical health symptoms (9 symptoms) and behaviour changes (11 symptoms). Subsequent questions asked whether the reported symptoms were linked to health conditions they were experiencing prior to the fraud (N/A; None; Some; All); the extent to which the symptoms had impacted on daily life (1: not at all–4: very affected); whether they had wanted to receive support or treatment to address the health impact of the fraud (Yes/No/NA); and whether the fraud had had a significant impact on their personal finances (1: not at all–5: to a great extent).
Participants were asked what they thought had specifically led to the start of the health symptoms, how the fraud had impacted on daily life, and to provide any further information on the impact and how it had affected their health (open responses). In total, 249 (80%) participants wrote a response to at least one of the three open-ended questions. This data was synthesised and analysed using a thematic analysis framework based on themes identified in the existing literature.
The survey was distributed to every fraud victim resident in two neighbouring police regions in England and Wales. The sample included victims who had reported or otherwise come to the attention of the police during a continuous 14-week period (June–September). Dissemination of the survey was facilitated by the support services in the police regions. The survey was sent to a total of 3,424 victims and 311 (9.1%) victims completed and returned a survey. In all, 3,043 surveys were delivered to victims electronically by email or SMS text message (88.9%), 337 victims received the survey by post (9.8%), and 44 were supported by phone to complete the survey (1.3%).
There was a small cohort of victims included in the sample who had received more intensive support from the police, having been assessed as ‘vulnerable’ by the police and to have greater levels of need. This group represented 5.0% of the total sample (n = 172), and due to high support needs, they were approached in-person or over the phone to complete the survey. For this reason, they are likely to be over-represented in the sample. The majority of participants in the sample had come to the attention of the police between 1 and 4 weeks prior to participation in the survey (n = 255); however, a minority of ‘vulnerable’ victims had been receiving support for longer periods of time; the length of time between a participant coming to the attention of the police and completing the survey ranged from 1 day to 6 years.
Results
This section will now explore the results from this study. It will begin by exploring the range of impacts experienced by respondents and then examine the relationships between the health symptoms. The impact on the daily life of victims is then assessed followed by their support needs. The results section ends with some qualitative data where quotes from victims are used to further support the findings. Table 1 shows the total number of participants that reported experiencing each impact across the three categories of symptom: emotional or mental health, physical health, and behaviour changes. 283 (91.9%) victims reported experiencing an emotional or mental health symptom (range: 1–19 symptoms), 167 (57.4%) a physical health symptom (range: 1–9 symptoms) and 188 (63.5%) a behaviour change (range: 1–9 symptoms), as a result of becoming a victim of fraud. The mean number of emotional or mental health symptoms reported was 5.72 (SD = 4.75), the mean number of physical health symptoms was 1.56 (SD = 1.89) and the mean number of behaviour changes was 1.52 (SD = 1.90). It is also important to note 42.6% experienced no physical symptoms, 36.5% no behavioural changes and 8.1% no emotional or mental health symptoms.
The emotional, physical, and behavioural impacts reported by victims of fraud.
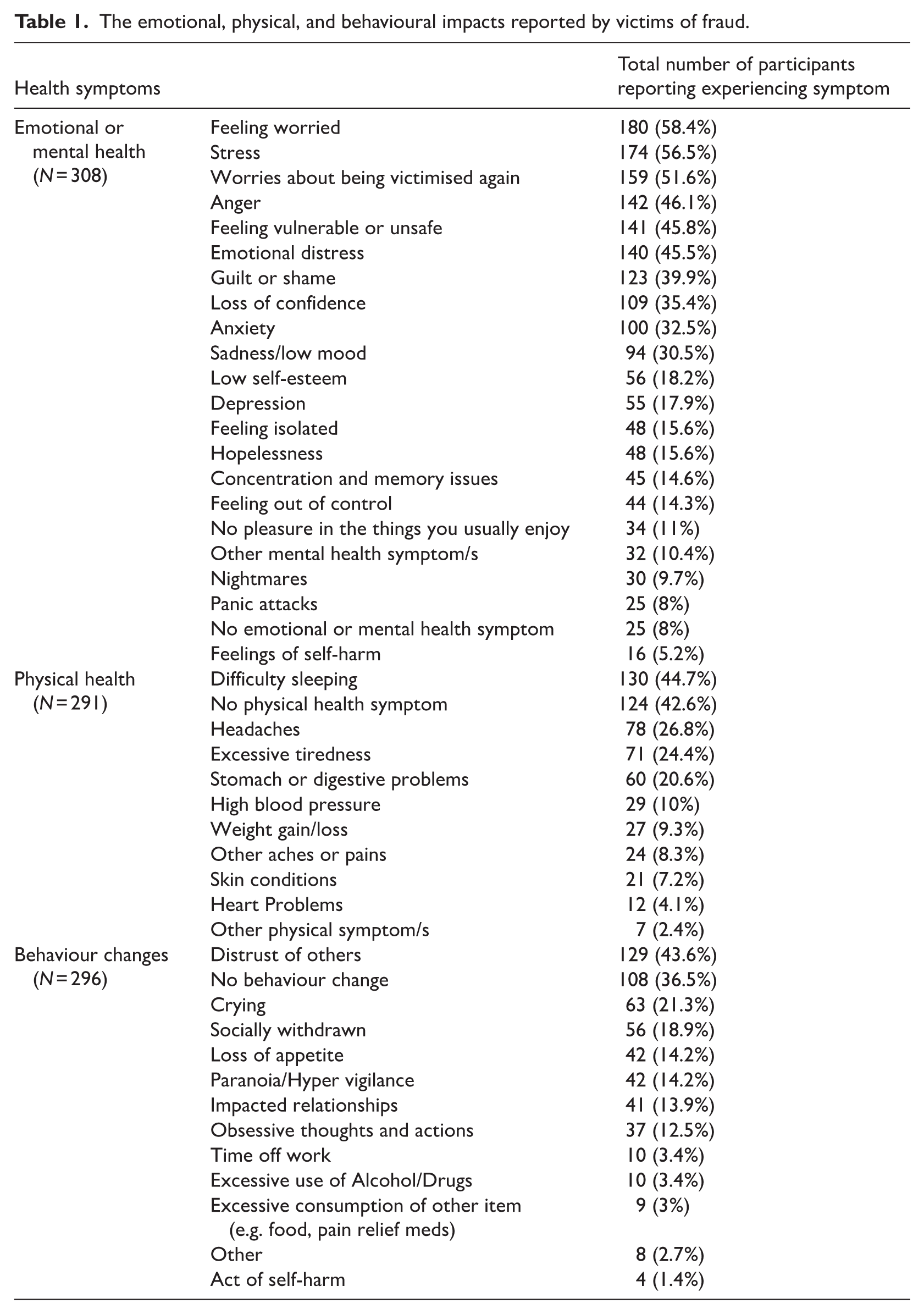
Table 1 shows a wide range of different impacts on victims. The most common emotional/mental health symptoms were feeling worried (58.4%) and stress (56.5%), with just over half of respondents indicating they were worried they might be victimised again (51.6%). The most common physical symptom was difficulty sleeping (44.7%). Approximately a quarter reported experiencing headaches (26.8%) or excessive tiredness (24.4%). The most frequently reported behaviour change was distrust of others (43.6%). Participants were asked whether the health symptoms reported in the survey were linked to health conditions that they were experiencing prior to the fraud: 13 (4.2%) of the participants reported that ‘all’ the symptoms were linked to conditions they had been experiencing prior to the fraud. Most participants reported that either ‘none’ (n = 115, 37%) or ‘some’ (n = 84, 27%) were linked to a prior condition. In all, 88 (28.3%) participants reported that it was not applicable to their situation. It is therefore important to note that some of the symptoms were present prior to victimisation, although for some respondents a pre-existing condition had been worsened by the victimisation.
Relationship between health symptoms
The researchers conducted exploratory factor analysis (EFA) to examine the correlations among the 40 self-reported mental health, physical health and behaviour changes. First, as the data were binary responses, polychoric correlation was conducted using the ‘polycor’ package in R to ensure there were sufficient correlations between each symptom and across symptom dimensions for EFA. To ensure the factorability of the data, Kaiser–Meyer–Olkin (KMO) factor adequacy was tested and Barlett’s test of sphericity. KMO demonstrated high factorability (0.91) and Barlett’s test was significant (p < 0.001). EFA was conducted in R with the maximum likelihood method of extraction, with the oblique rotation method ProMax. ProMax was used to allow for correlation among the symptom variables. The number of factors to be extracted was determined by examining factors with eigenvalues greater than 1 and parallel analysis. Initially, there were 10 factors with eigenvalues greater than one; however, parallel analysis confirmed six factors were appropriate. Analysis of 7, 8, 9, and 10 factors demonstrated that six-factor extraction was the most parsimonious structure. Factor loading cut-off thresholds were set at 0.33 based on the sample size (N = 311) for practical significance (Hair et al., 1998). Five symptoms did not meet the cut-off threshold: stomach or digestive problems, headaches, other aches or pains, excessive consumption of alcohol and drugs, and paranoia/hypervigilance. See Table s1 in supplementary materials for full factor loading table and Table s2 for factor correlations.
The six factors were named to depict the underlying construct represented by the contingent symptoms: worry and distrust; hopelessness and self-harming; somatic and obsessive; low mood; anxiety; and withdrawal from important functioning. Table 2 shows the symptoms and factor loadings for each factor.
Factor analysis for the self-reported health symptoms.
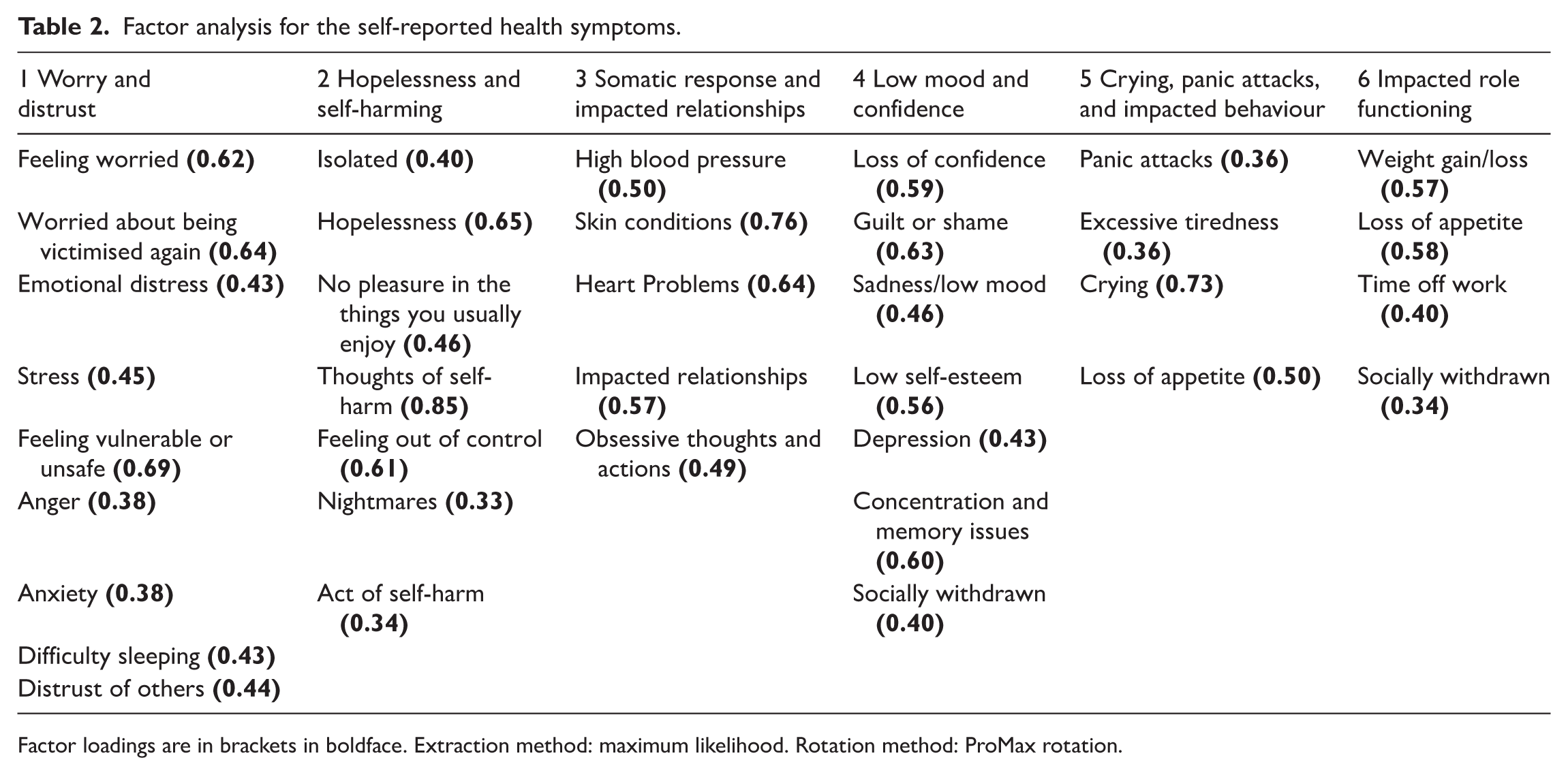
Factor loadings are in brackets in boldface. Extraction method: maximum likelihood. Rotation method: ProMax rotation.
Factor 1 – Worry and distrust
This factor contained nine symptoms, the symptoms with the highest factor loadings (>0.61) being feeling worried, worried about being victimised again, and feeling vulnerable or unsafe. The other symptom loadings ranged from 0.383 to 0.446 and included emotional distress, stress, anger, anxiety, difficulty sleeping and distrust of others. A follow-up reliability analysis found Factor 1 to have good internal consistency (α = 0.80).
Factor 2 – Hopelessness and self-harming
There were eight symptoms present in the hopelessness and self-harming factor. Factor loadings ranged from 0.326 to 0.854 showing ‘thoughts of self-harm’ to be the highest loading symptom. The other symptoms included: feeling isolated, hopelessness, no pleasure in the things you usually enjoy, acts of self-harm, feeling out of control, excessive consumption of other (e.g. food, pain relief pills), and nightmares. Reliability analysis found Factor 2 to have good internal consistency (α = 0.81).
Factor 3 – Somatic response and impacted relationships
Psychological, physical, and obsessive behavioural symptoms were present in the somatic and obsessive factor with six symptoms in total (loadings ranging from 0.486 to 0.761). Skin conditions had the highest loading with the remaining symptoms being high blood pressure, heart problems, impacted relationships, and obsessive thoughts and actions. Reliability analysis found Factor 3 to have medium internal consistency (α = 0.68).
Factor 4 – Low mood and confidence
This factor contained eight symptoms with loadings ranging from 0.326 to 0.626. The symptom with the highest loading was feelings of guilt or shame. The other symptoms included loss of confidence, sadness/low mood, low self-esteem, depression, concentration and memory issues, difficulty sleeping, and socially withdrawn. Factor 4 was found to have good internal consistency (α = 0.84).
Factor 5 – Crying, panic attacks, and impacted behaviour
The anxiety factor included four symptoms: panic attacks, excessive tiredness, crying, and loss of appetite. Loss of appetite also cross-loaded with the sixth factor ‘impacted role functioning’. Factor loadings ranged from 0.355 to 0.731 with ‘crying’ loading the highest. The internal consistency for Factor 5 was acceptable (α = 0.72).
Factor 6 – Impacted role functioning
The withdrawal from important functioning factor included four symptoms (loadings ranging from 0.343 to 0.578) and included the following symptoms: weight gain/loss, socially withdrawn, time off work, and loss of appetite which cross-loaded with the anxiety factor. Reliability analysis found Factor 3 to have acceptable internal consistency (α = 0.70).
Impact on daily life
Participants were asked to report the extent to which their daily lives had been affected by their symptoms (see Figure 1).
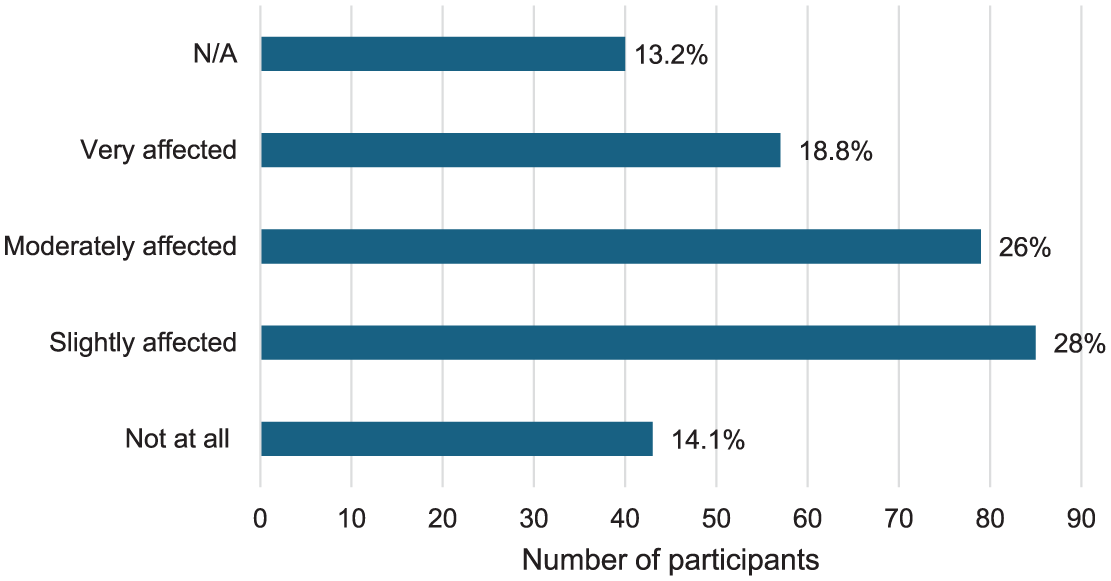
Number of participants that reported an impact on daily life.
To test whether the total number of reported health symptoms predicted the extent to which participants (n = 256) reported an impact on their daily lives ordinal regressions were carried out (using the CLMM function in R). The model included random effects for participants’ ratings and impact on their daily lives as the dependent variable, and the total number of mental health symptoms, physical health symptoms and changes in behaviour as predictors. As shown in Table 3, emotional or mental health symptoms, physical health symptoms, and behaviour changes significantly predicted participants’ ratings on the impact of the fraud on their daily lives, that is, the more symptoms reported, the greater the impact participants reported on their daily lives.
Ordinal regression results for the total number of health symptoms predicting the impact on victims’ daily lives.
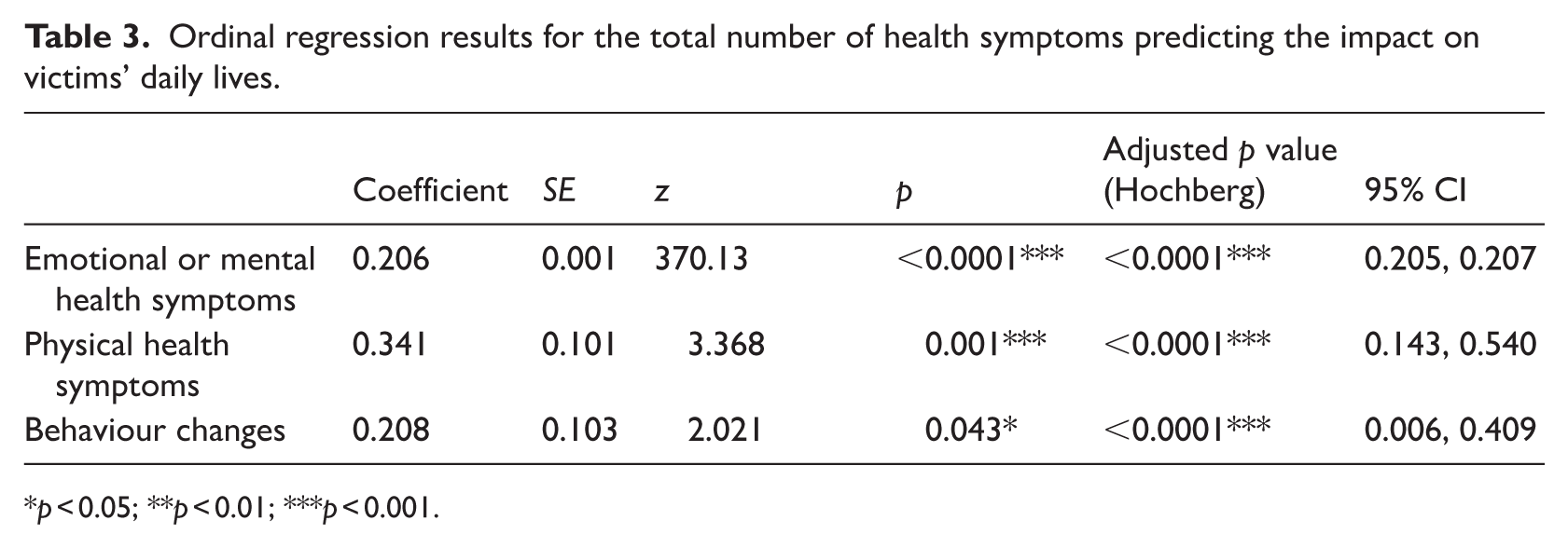
p < 0.05; **p < 0.01; ***p < 0.001.
The support needs of victims
Participants were asked to report whether they had wanted to receive support or treatment to address the health impact of the fraud. In all, 56 participants reported wanting to receive support or treatment (18.4%), 194 stated they did not want to receive help and support (63.6%), and 55 reported NA (18%).
Binary logistic regressions were performed (using the glm function in R) to test whether the total number of mental health symptoms, physical symptoms, and behaviour changes predicted the odds of participants wanting to receive support or treatment for their symptoms. As shown in Table 4, all three symptom areas significantly predicted the likelihood that individuals wanted to receive support, that is, the more total symptoms, the more likely participants were to want to receive support and/or treatment for their symptoms. As the number of reported symptoms increased by one symptom, the probability of participants wanting to receive support increased by 11% (mental health symptoms), 26% (physical health symptoms), and 28% (behavioural changes).
Binary logistic regression – total symptoms predicting support needs.
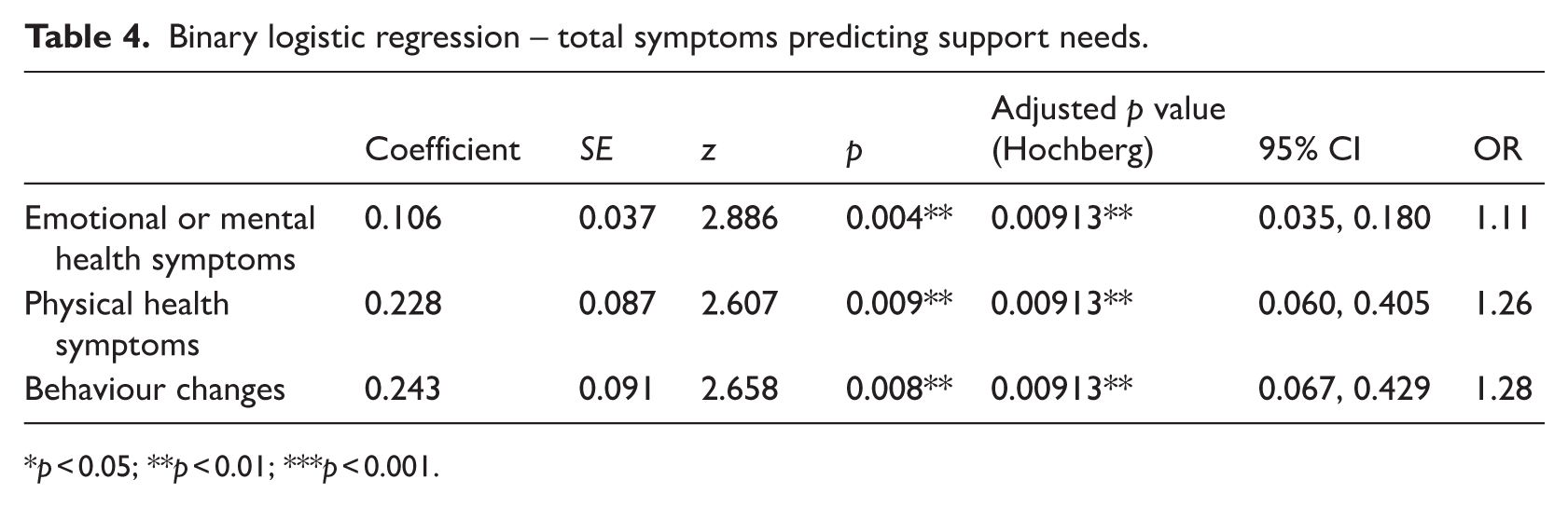
p < 0.05; **p < 0.01; ***p < 0.001.
Analysis of qualitative responses
The emotional and psychological response to the fraud was described in a variety of ways, including different types of symptoms, levels of intensity, and their duration. Victims reported distress the moment they were defrauded and many described the experience of shock, upset, panic, or anger on realising they were a victim of fraud. Some described experiencing a stress response at the time they were communicating with the fraudster, particularly those who experienced fraud methods that are intended to induce fear so to manipulate the victim, for example, the impersonation of an official who threatened adverse consequences if the victim does not comply with their demands.
I feel under pressure too because the company are still asking me for payments and I was told by Action Fraud not to pay any more. The company are making me [feel] threatened because they are saying the interest will go up and affect my credit score. (P175) The caller purported to be from [a legitimate software company] . . . Fortunately I realised after a few minutes, and before I had given him any information, that this was a scam call and shut it down. However, the caller then subjected me to multiple calls to try to make me believe he was genuine. I let most ring out, but found it quite threatening and distressing. (P132)
Some victims reported an intense initial response, but one that abated several days after the incident. The negative emotions could be acute during the period of uncertainty when trying to resolve the incident. The capacity to recover appeared to be mediated by various factors, including successfully preventing the financial loss or recovering lost funds, and feeling supported by others.
I could not properly function that day after I spoke to the police. I was exhausted and couldn’t concentrate yet sleep was not coming. The next day some symptoms started to appear . . . triggered by stress and made my low mood worse. (P182) Eleven days on [and] I am only slightly affected and all symptoms are abating, but in the immediate aftermath of the fraud I was very affected . . . being socially withdrawn and the lack of energy attendant on being physically unwell (stomach upsets), not eating much and being highly stressed. The latter affected my ability to think clearly and to remember things. (P228) Three weeks in, and I personally don’t care, but for the two weeks prior and two weeks after, I was all consumed by this . . . it affected me a lot. (P293)
Others experienced a significant psychological and emotional response over a sustained period of time, lasting weeks or even months after the fraud incident; symptoms that were ongoing at the time of completing the survey. Stress, anxiety, and despair were commonly described, and these foundational responses gave rise to other symptoms such as crying, panic, apathy, inability to sleep, headaches, tiredness, distraction, and an inability to work. There were victims who felt incapable of putting the incident behind them, with some even concerned that they had been changed permanently by the victimisation experience.
I keep getting panic attacks, my anxiety is more worse than ever, I am not eating well and mentally this is all affecting me, as my account is special and somebody pretending to be me is shaming me online. I can’t sleep well at night either, my heart and stress levels go high ever since this fraud attack has happened to me. (P284) When the police became involved and I realised that this was a scam it has affected me immensely. I didn’t feel able to talk to many people about this as I felt ashamed. I had to go to the doctor as I was not sleeping. I started to take sleeping tablets but these made me feel dreadful the following day. My family and friends who know have been supportive and want me to get over it, but this has been easier said than done. (P77) It was a devastating experience. I consider myself an emotionally strong person . . . I fear I will never regain the confidence and trust that I lost. This event was life-changing and significantly altered my perspective as I grow older. (P122)
Victims commonly described obsessive thoughts that fuelled negative emotions associated with the fraud and impacted on daily life functioning; disrupted sleep, an inability to concentrate on other things (e.g. work). Others emphasised the financial impact of the fraud, reflecting either current concerns over making ends meet (e.g. paying bills) or concerns about financial security in the long term.
It consumes all of my waking thoughts and I cannot move on from it. (P108) I cannot concentrate on anything else. I am just sitting there hoping that the police is going to find the person. This has taken over my life. (P196) The uncertainty and financial instability have added immense stress to our relationship and well-being. We’re both struggling with anxiety and a sense of betrayal, unsure of what our future holds. (P2)
One of the most pronounced themes was a need to rationalise and resolve the part that they had themselves played in the fraud. Many blamed themselves for what had happened and used terms such as ‘fool’, ‘gullible’, ‘naïve’, ‘stupid’, or ‘idiot’ to describe themselves and their role in the fraud. Some had turned their rationalisation for the incident inwards, redirecting culpability away from the perpetrators and towards themselves. Other emotional or psychological responses could flow from self-blame, including guilt and shame.
The guilt you feel eats away at you, because you feel so stupid for being scammed. (P310) In the back of my mind is the constant ‘nag’ as to why I naively followed the instructions I was being given without questioning them even once, I feel that I would not do that again, but the ‘nag’ is always there. (P52) My family are upset with me about the money I have lost to this investment fraud. I am thinking about it most days and move between angry with myself and the people that carried it out. I don’t have much energy to do much at the moment and ‘feel lost’. (P61)
This self-blame has implications for a victims’ sense of victimhood and help-seeking, with the risk that some consider themselves underserving of help. It may also lie at the root of some of the wider impacts on health and well-being. Some described obsessing over what they had done and what they could have done differently to avert victimisation. Self-blame was not just an explanation for the event, it could alter and diminish a victim’s view of themselves. Some felt guilt and that they themselves were deserving of reproach (from themselves or others). Some expressed a concern that they would become diminished in the eyes of important others in their life, fuelled by feelings of embarrassment and humiliation. This reduced sense of self-worth could contribute to becoming socially withdrawn and eroded confidence in their own judgement and abilities.
Really it was I who isolated myself – couldn’t hold my head up – didn’t wash or dress properly – I was in a [club] and couldn’t go – had no heart to do so – my head was down, feeling ashamed and stupid BUT I had commitments and for those I did get dressed properly, and fulfil them but it was joyless and exhausting. I felt I deserved to feel like this and at any time I started to feel better I remembered I had no right to feel better having been so stupid . . . I had to keep internally not forgetting what I had done and almost punishing myself. (P118) Debts created due to being the victim from scams remind me of the stupidity of falling into the trap. Depressions and the related emotions come back. (P197)
Many participants described a prevailing fear of being victimised again, and a feeling of helplessness to protect themselves, despite having reported to the police. For some this worry was rooted in practical security concerns, such as their personal data still being in the possession of the perpetrators. Others conveyed feelings of being disempowered and a belief that they were incapable of fending off further fraud attempts. Some described feeling ‘exposed’ and ‘vulnerable’ and doubting their own judgement. The invisibility of the fraudsters and their methods appears to be a contributing factor, mixed with a perception of them as highly competent and motivated to target them.
It has added extra stress to my life. I worry about more scams rearing their ugly head. I think I have done all I can to stop what they were doing but they are clearly very clever so who knows what will happen – nothing I hope. (P146) The phishing attack was so well orchestrated with multiple actors over the course of an afternoon, even impersonating the police and using phone numbers that appeared to come from legitimate organisations. It gave me a feeling that a. I couldn’t trust anything / anyone and b. why me? and c. where was it coming from? d. how could I stop it? e. how vulnerable was I?. (P260)
The fear and distrust following the fraud led some to engage in avoidance behaviours. These behaviours could vary depending on the specific methods by which they had been targeted, such as withdrawing from technology and digital life, avoiding certain forms of communication, reluctance to leave the house, or withdrawing from social situations. These areas can be integral to everyday life, and so avoidance behaviours can affect well-being, depending on how restrictive they became and for how long. For example, social isolation and exclusion from services could come as a consequence of certain avoidance behaviours.
I have found I do not want to go on [the social media platform] where I have friends. I feel I do not trust media about anything they say. (P165) Total loss of trust toward people resulted in not wanting to talk to anyone or going out of the house to meet people. (P124) The whole world is being forced to do everything online it is fast becoming impossible to do anything without fighting ever present fraud. Consequently, I am largely forced to withdraw from ‘normal’ life simply to survive – but for what?? I am angry about that. (P292) Not sure I’ll ever be able to trust someone again in a relationship. (P60)
Discussion
This research raises a number of important discussion points. Nearly all participants (91.9%) reported experiencing at least one symptom in response to the fraud. There was a particularly high number of participants who experienced at least one emotional or mental health symptom; for example, over half of victims reported feeling worry, stress, or worry about being victimised again. Overall, the various symptoms associated with physical health or behaviour changes were reported less frequently, though just under half of victims reported difficulty sleeping or distrust of others.
The experience of impact will be qualitatively different for different victims. This is not only in terms of the type of symptom that is experienced, but also its intensity. In victimology research, some have drawn a distinction between the effects and the impact of crime on victims (Dignan, 2005). The symptoms included in the survey represent a range of possible ‘effects’ (e.g. worry or difficulty sleeping), but the intensity and duration of each reported effect will differ between victims; for example, the intensity of a stress response is unlikely to be the same for two different victims. The difficulty lies in positioning the ‘effects’ of crime on to a continuum to gauge the relative intensity of impact on health. In short, when does an ‘effect’ become a health ‘impact’, and relative to other victims, how severe is that impact?
This research adopted several approaches to explore the impact of fraud on health. First, it examined the composition of symptoms that were reported by participants to develop a more complete view of the individual experience. Previous studies have assessed the prevalence of discrete symptoms (e.g. anger) in isolation (Button et al., 2014; Palassis et al., 2021). However, the current research shows that victims frequently experience more than one symptom, so appraising each in isolation may offer only a partial representation of impact. This is demonstrated in the EFA which showed the co-occurrence of symptoms such as worry, anger, stress, anger, and anxiety (i.e. the ‘worry and distrust’ factor). A similar pattern was found for some of the lower frequency symptoms, that is, victims who reported somatic symptoms such as heart problems were more likely to report experiencing other somatic symptoms (e.g. high blood pressure), impacted relationships, and obsessive thoughts and action (i.e. the ‘somatic response and impacted relationships’ factor).
To understand the impact of the reported symptoms, there is a need to consider both the volume and type of symptom experienced. There may be cumulative effects whereby each additional symptom increases the impact on health, but also the intensity of impact may be variable across different types of symptom. For example, participants are likely to have interpreted ‘worry’ as a lower intensity (or at least more wide-ranging) symptom than a ‘panic attack’. The EFA shows that certain high-intensity symptoms coalesced. Feelings of hopelessness were associated with symptoms such as feeling out of control, thoughts of self-harm, and nightmares (see Factor 2). Understanding the relationships between these symptoms is important to assessing the impact or risk of impact.
A second perspective to consider is the importance of health to well-being and quality of life, with the impact considered a function of the wider effects on the victims’ life (Greenfield and Paoli, 2013; Hanson et al., 2010; Layard and Oparina, 2021). The descriptions provided by victims indicate that not all health symptoms included in this study represent responses that are experienced in parallel, but rather responses experienced in a sequence (or cycle) that can escalate the impact. Negative thoughts and emotions could interrupt other areas of daily life, including sleeping patterns, social life and work. The qualitative nature and gravity of ‘impact’ is not necessarily reflected by discrete symptoms (e.g. stress), but rather by the sum of the victims’ experience. Each individual symptom can manifest differently, with considerable variation in the intensity, duration, and effects on the victim’s wider life. The relationship between the health impact and other aspects of well-being such as finances, relationships, and role functioning is bi-directional, or in some cases cyclical; for example, social withdrawal could exacerbate the impact of a fraud on health, but also the impact on psychological or emotional health could lead the victim to become socially withdrawn.
Some high-frequency symptoms such as stress were depicted as foundational responses that led to somatic symptoms such as headaches or an inability to sleep, but not for all victims. Similarly, the category of symptoms included as behaviour change also provide a window on impact; for example, 18.9% of participants reported becoming socially withdrawn, 13.9% impacted relationships, and a minority (1.4%) an act of self-harm in response to the fraud. The EFA showed that for some victims, multiple aspects of their life were affected; it showed the co-occurrence of loss of appetite, weight gain/loss, taking time off work, and becoming socially withdrawn (see Factor 6). Furthermore, as the number of reported health symptoms increased, participants reported a greater impact on their daily life. This highlights the importance of considering health in quality of life frameworks for assessing the impact of fraud. It also highlights the need for evidence-based frameworks to taxonomize and weight the various effects (or symptoms) of fraud.
A final perspective to consider in gauging the impact on victim health was the individual’s capacity to cope and recover from victimisation (Jansen and Leukfeldt, 2018). This is in part determined by not only the resilience of the individual, but also the gravity of the fraud offence. An inability to cope or recover from the fraud can lead to effects that are experienced over a longer time period, and thereby increases the impact (Johnston et al., 2018). And from a more pragmatic perspective, this analytical frame can help to determine which victims merit access to support services, that is, which victims have the greatest need of support to mitigate longer-term effects. The latter perspective is highlighted in policies that are focused to identify fraud victims who are ‘vulnerable’ (Skidmore et al., 2020).
In describing their responses to the fraud, some depicted high-intensity responses to victimisation (e.g. stress or becoming socially withdrawn) that abated within days or weeks of victimisation, whereas others were continuing to experience symptoms when completing the survey. A minority (18.4%) reported they had wanted to receive support or treatment to address the health impact. This indicates the victims’ own perspective on their capacity to cope and recover without additional help. And the more symptoms that were reported, the more likely a victim wanted support or treatment. However, the sampling methodology in this study missed a longitudinal perspective; most victims had reported to the police only 1–4 weeks prior to completing the survey. There are few studies that that have assessed the impact of fraud in the longer term or employed standardised clinical assessment tools to assess the psychological impact on victims (Sarriá et al., 2019; Weissberger, 2022). One prior study found an association between earlier exposure to financial fraud and a greater mental health need (Sarriá et al., 2019). A small number of studies identified fraud victims who went on to experience a major depressive disorder, general anxiety disorder, or post-traumatic stress disorder (Ganzini et al., 1990; Spalek, 1999). There remains a gap in the research and our understanding of the long-term impacts of fraud victimisation.
In exploring the nature of the health impact on victims, a next step is to consider which factors determine whether victims’ experience certain types or severity of symptom. An improved understanding of the causal factors would improve assessments of risk and help practitioners pre-empt more damaging impacts on victims. Research has shown that the effects and impact can vary based on the individual characteristics of the victim such as age or gender (Button et al., 2014; Home Office, 2025), the victims’ social or financial circumstances (Poppleton et al., 2021), and the different methodologies and circumstances of the fraud (Kerr et al., 2013; Modic and Anderson, 2015; Skidmore et al., 2020). There are likely to be interdependencies between these various factors in determining the impact. Our research offers a health perspective, and victims described obsessive thoughts and self-blame that fuelled other symptoms such as guilt, shame, social withdrawal, or an inability to sleep. Victims also described financial stress, feeling unable to resolve the incident (e.g. reimbursement), and supportive social environments as important to mediating the impact of fraud. The indication is that the impact is not only a function of the crime, but also their treatment in the aftermath. These are important factors to consider in designing response systems.
Limitations
Participants were recruited from only two regions in the United Kingdom within a fixed period of 14 weeks. Most had reported the fraud to the police, and a minority had been identified by the police or other organisation (e.g. the bank). It is therefore unclear how generalisable the findings are based on this specific sample. Furthermore, participation was based on self-selection. It is not known the extent to which the range of victim experiences are over- or under-represented by the participants in this study. These are important considerations in interpreting the data because research has shown that a high proportion of fraud victims choose not to report and remain hidden to the police; patterns in offending and victimisation are variable in different regions of the world; and fraud offending is a fast-evolving area of crime, and the impact of changing criminal methods may be variable over time (ONS, 2024; UNODC, 2024). And finally, as previously described, this data provides a short-term perspective of the impact of fraud and cannot account for the health impacts in the long term.
Conclusion
This research builds on the growing body of evidence which demonstrates that many victims suffer harm as a consequence of fraud (Button et al., 2014; Cross, 2015; Home Office, 2025). However, while previous studies have adopted more generalised definitions of impact, the focus of this research was the impact on victims’ health. This offers a sharper analytical focus to understand the experiences of fraud victims, and target more specific points of intervention. Furthermore, the impact on health is a central component of wider frameworks for measuring harm or the effects on well-being, which are important for policymaking in the criminal justice system (Greenfield and Paoli, 2013; Heeks et al., 2018). It also is clear from this study that much more research is needed to understand the health impacts of fraud and the means to support victims in relation to this through clinical measures.
Supplemental Material
sj-docx-1-irv-10.1177_02697580261417364 – Supplemental material for Exploratory research to examine the impact of fraud on victim health
Supplemental material, sj-docx-1-irv-10.1177_02697580261417364 for Exploratory research to examine the impact of fraud on victim health by Michael Skidmore, Felicity O’Connell, Ruth Halkon, Amy Meenaghan and Mark Button in International Review of Victimology
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study/project is funded by the NIHR Public Health Research programme (NIHR154927). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.