
Abstract
We examined the impact of Covid-19 on service delivery within specialist sexual violence services and the healing journeys of survivors of sexual violence and abuse through the experiences of 22 professionals and 221 service users in England. The pandemic posed challenges across all sectors and economies across the globe, but practices and innovations that emerged at that time could enhance future services and user experiences. Thematic analysis was used to identify key themes within the data. Overall, the negative impacts of Covid-19 outweighed the positive changes: survivors reported increased feelings of depression, anxiety, and worry, exacerbated by isolation and lost connections with friends and family, and access to strategies for managing their mental health. Difficulties/delays in accessing support, service provision, and disruptions to rapport, trust, and safety were widespread in participants’ reports. Conversely, for some, requirements to remain at home provided safety from the world, and space for healing, and even prompted survivors of non-recent abuse to seek help. Remote service delivery was beneficial where clients could be ‘at a distance’ in discussing sensitive issues. Together with insights from professionals about their own isolation, blurred boundaries, and concerns regarding client confidentiality and engagement, this research highlights an agile sector responding to an unprecedented situation. Moving forward, survivors’ preferences for flexible/remote support must be integrated into everyday delivery.
Introduction
Sexual violence continues to represent a significant global public health issue, of which the substantial, lifelong, negative physical, mental health, and social impacts have long been recognised (World Health Organization (WHO), 2013, 2018). Support and a range of interventions for victims and survivors in the aftermath of sexual violence and abuse can be effective in reducing post-traumatic stress disorder and symptoms of depression and anxiety (O’Doherty et al., 2023), enabling victims and survivors to re-engage with many aspects of their lives (Brown et al., 2022). Despite this, victims and survivors often struggle to access appropriate support and interventions throughout their lives (Brown et al., 2022; Independent Inquiry Into Child Sexual Abuse, 2022), with agencies and services that are over-stretched and under-resourced (e.g. Rape Crisis, 2021). Furthermore, inadequate responses to sexual violence are pervasive across legal systems. For example, in England and Wales, there have been significant declines in the charging of rape cases, prosecutions, and convictions (HM Government, 2021). Consequently, victims and survivors of sexual violence and abuse have little confidence in what formal responses they might receive (e.g. in supporting a police investigation) (Molina and Poppleton, 2020; O’Doherty et al., 2022). How victims and survivors are treated by professionals in the aftermath of sexual violence and abuse can influence their psychological recovery (Ullman and Peter-Hagene, 2014). Experiences of insensitive treatment often lead to feelings of powerlessness, shame, and guilt (Campbell, 2008) and the long duration of criminal proceedings and lack of victims’ and survivors’ voices and perspectives in legal proceedings can exacerbate physical, social, and mental health struggles (O’Doherty et al., 2022). These challenges are echoed internationally, with a consensus that change is needed on a global level (e.g. Sentencing Advisory Council, 2021). This background is the setting for the current study, in providing an original investigation of the cumulative impacts that the global pandemic of COVID-19 had on victims and survivors of sexual violence and abuse, and on those working within settings that provide support to them.
There were three lockdown periods in England between 2020 and 2021. It is now well-recognised that lockdown periods, both nationally and internationally, resulted in increases in the incidence of domestic abuse and escalated the risk to those already subjected to abuse (e.g. Kourti et al., 2023; Office for National Statistics, 2020). Described by some as a ‘pandemic within a pandemic’ (Johnson et al., 2020), sexual violence received fewer media attention at the time than domestic violence, but given that most rapes are perpetrated by individuals known to victims and occur in the victims’ or perpetrators’ homes (Office for National Statistics, 2021), it was recognised that it was perpetrated alongside domestic abuse.
Early in the pandemic, research highlighted the challenges faced by victims and survivors of sexual violence and abuse. After the first lockdown in summer 2020, Almeida (2020) reported on the perspectives of frontline Victim Support (an agency that supports victims of any crime in England and Wales) staff on victims’ and survivors’ access to services. Staff said that victims of crime experienced increased barriers to accessing both government agencies and non-government services for multiple reasons including a perception that services were not open, services being overwhelmed and unable to meet needs, and clients not wishing or being unable (e.g. due to digital poverty) to use non-traditional methods of engaging with services. In addition, service providers highlighted increased isolation for survivors (Michaelsen et al., 2022) and that changes in modes of service delivery were perceived to hinder effective communication and rapport between clients and staff (Montesanti et al., 2022). Overall, staff depicted a bleak outlook of the potential impact on survivors, perceiving these changes as significantly diminishing clients’ capacity for healing, especially for sexual violence victims and survivors, and magnified among the most vulnerable (The Survivors Trust, 2020). Given that delayed disclosure, help-seeking, and/or intervention often necessitate more intensive support, concerns about long-term outcomes for survivors were not unfounded (Bicanic et al., 2015; Ruggiero et al., 2004).
While services initially experienced reductions in service use (Muldoon et al., 2021), these quickly returned to usual or increased levels (Majeed-Ariss et al., 2023), alongside greater proportions of vulnerable clients (who had experienced more severe abuse during the pandemic) seeking support (Almeida, 2020; Schrag et al., 2022). The services themselves experienced considerable upheaval, as they sought to provide services in line with COVID-19 safety protocols. The Survivors Trust (an agency that represents sexual violence and abuse services in the United Kingdom and Ireland) surveyed their members in November 2020 and found that 70% of staff reported that work issues were invading home life, and just more than 50% reported concerns about teams feeling less cohesive. Gunby et al’.s (2020) discussion paper about the implications of changes in service delivery highlighted the potential for lost distinctions between the home and the workplace and removing the emotional and physical distance, so vital in this context, between work and home life (see also Wood et al., 2022).
The changes in service delivery, specifically the shift to remote services (i.e. telephone or online), were not necessarily negative. Pre-pandemic, sexual violence researchers were already evaluating different interventions using different modalities (see O’Doherty et al., 2023), with some research suggesting it may be preferable to offer remote care in some circumstances, for example, to avoid traumatic triggers in clinical settings. In relation to military sexual trauma, Acierno et al. (2021) compared home-based telemedicine with in-person care and found no differences in the efficacy of trauma-focused cognitive-behavioural therapy (CBT). However, Smith et al. (2022) pointed out that this research was in its infancy, noting the lack of systematic research into clients’ perspectives on remote methods of delivering psychotherapy. Specifically, they argued that it was important to explore this in the context of the pandemic, where online and telephone support was largely imposed by circumstance, rather than by client choice. Brown et al’.s (2022) qualitative synthesis of the experiences of psychosocial interventions for sexual violence found that the format and delivery of an intervention could impact individuals’ experiences. One study in that review identified the difficulties of delivering trauma-focused CBT to child survivors during the pandemic when parents and children wanted to meet in person (Polk, 2021). The review highlighted the importance of managing expectations about interventions, including preparing victims and survivors and carers for receiving virtual interventions. Hence, while some knowledge exists in relation to the delivery of remote care, there remain many questions, not least in capturing a wider breadth of perspectives and experiences of professionals, victims, and survivors (Storer and Nyerges, 2023).
The current study
Synthesising the perspectives and experiences of professionals, victims, and survivors during the height of the pandemic makes a vital contribution to understanding how practice and support can be shaped for the future. Learning from such instances will ensure that responses to survivors are resilient to future events and will also harness the best practices implemented during these times in order to identify innovations and strengthen responses overall (Johnson et al., 2020; Roesch et al., 2020). The majority of the survivor-centred research has focused on domestic/intimate partner violence (e.g. Mazza et al., 2020), or contained the perspectives of a limited number of professionals (e.g. Bennett et al., 2021; Janse van Rensburg and Smith, 2021). Prior research regarding victims’ and survivors’ perspectives has been only drawn from professionals providing their views of victims’ and survivors’ challenges (e.g. Elliott et al., 2023; Michaelsen et al., 2022). Research that did involve survivors is limited to quantitative data and involved assessments of forms of help-seeking during the pandemic, for example Sorenson et al’.s (2021) assessment of ‘911 calls’. No research has documented the voices of victims and survivors of sexual violence in ‘real-time’ (i.e. during the pandemic). Furthermore, this research draws on professionals’ perspectives regarding the impacts of the pandemic and experiences of service delivery across multiple settings and organisations in England, extending the value of this work. This original research explores the views of those who worked in sexual assault referral centres (SARCs, i.e. medico-legal settings), those who worked at a strategic/commissioning level of the sexual violence services, non-governmental agencies (i.e. the voluntary sector), and the police regarding the changes brought about by the pandemic. These organisations represent the key supporting organisations (and those who shaped those services) for victims and survivors in their help-seeking and subsequent recovery journeys.
This research employs an ecological model to organise the examination of the impact of Covid-19 on victims’ and survivors’ healing and recovery journeys and service delivery in sexual violence and abuse services. This framework has previously been applied to service utilisation and health outcomes as it supports understanding the complex and interconnecting factors that can have a cumulative effect on health (Golden and Earp, 2012). In applying this theory to the experiences of victims, survivors, and professionals, the findings from this study will articulate factors that influence survivor recovery across microsystems, mesosystems, exosystems, macrosystems, and chronosystems (Chynoweth et al., 2020; Stockman et al., 2023). Microsystems refer to the survivor’s immediate environment and interactions, such as interactions with support services and their immediate personal support network. Mesosystems relate to connections between components of the microsystem such as communication between agencies that work with victims and survivors and also service delivery For example, in the context of this current research, changes in modes of service delivery during the pandemic may reduce effective rapport between staff and clients, therefore impacting on clients’ ability to cope and recover (Campbell et al., 2009), with research at this level sparse (Zinzow et al., 2022). The exosystem level is quite removed from the daily experiences of service users but, as Dworkin and Weaver (2021) point out, this does not mean policies, procedures, and practices at that level cannot influence people’s experiences. For example, policies and blanket messaging about locking down communities and nations may have led victims and survivors to perceive that services were simply unavailable. The impact of the pandemic is captured at the macrosystem level in the form of an environmental stressor, with researchers now defining the pandemic as a form of sociocultural-level trauma (e.g. Bridgland et al., 2021). The final level to consider is chronosystem factors, which encapsulate changes that occur over time. In all, the use of this model is extremely effective in capturing the complex interplay between individuals, systems, processes, and culture, as well as changes over time, an approach that has been previously identified as an important focus of future research (e.g. Campbell et al., 2009; Zinzow et al., 2022). Furthermore, using this model has also been highlighted as an effective approach to generating important recommendations for future practice (Eriksson et al., 2018).
Within this organising model, Herman’s (1992) theory for trauma recovery is applied to contextualise the findings in relation to how they may affect survivor recovery (see Campbell et al., 2009). This theory identifies three stages of trauma recovery: safety, remembrance and mourning, and reconnection. Its use in framing the findings will seek to understand how this pathway (while rarely linear) was affected, particularly when the trauma could have been additionally layered with the experiences of the pandemic. At the first stage of recovery, safety is re-established across physical safety, emotional safety, and developing coping mechanisms. Remembrance and mourning involve the narrative of the trauma, recalling and mourning the trauma experience, and confronting and processing trauma in supportive environments. Finally, reconnection involves creating a future for the survivor, reclaiming their empowerment, and reconnecting with themselves, relationships, and communities (Herman, 1992).
This research provides a unique triangulation of perspectives from victims, survivors, and professionals across a range of agencies that supported them during the pandemic.
The research questions were:
How did the pandemic impact on survivors of sexual violence and abuse and their help-seeking and recovery journeys?
What were the impacts of the pandemic on service delivery and staff in sexual violence and abuse services and what challenges and opportunities arose?
Method
Design
This study was developed as part of a longitudinal study into the health and well-being of survivors post-SARC (Multidisciplinary Evaluation of Sexual Assault Referral Centres for better Health (MESARCH), O’Doherty et al., in press) carried out between 2018 and 2023. This qualitative research embedded lived experience perspectives throughout the project from its design and delivery to the interpretation and sharing of the findings. A Patient and Public Involvement group was engaged throughout the project and members’ views shaped the project including the design of research materials, communication, and the development of outputs.
Participants and setting
The experiences of 221 survivors of sexual violence and abuse aged 18 and older are reported. They were recruited into the MESARCH study based on having received care or support from a sexual assault referral centre (SARC (n = 15 sites)) in England between August 2019 and June 2021 (see Table 1).
Descriptive data of participant characteristics.
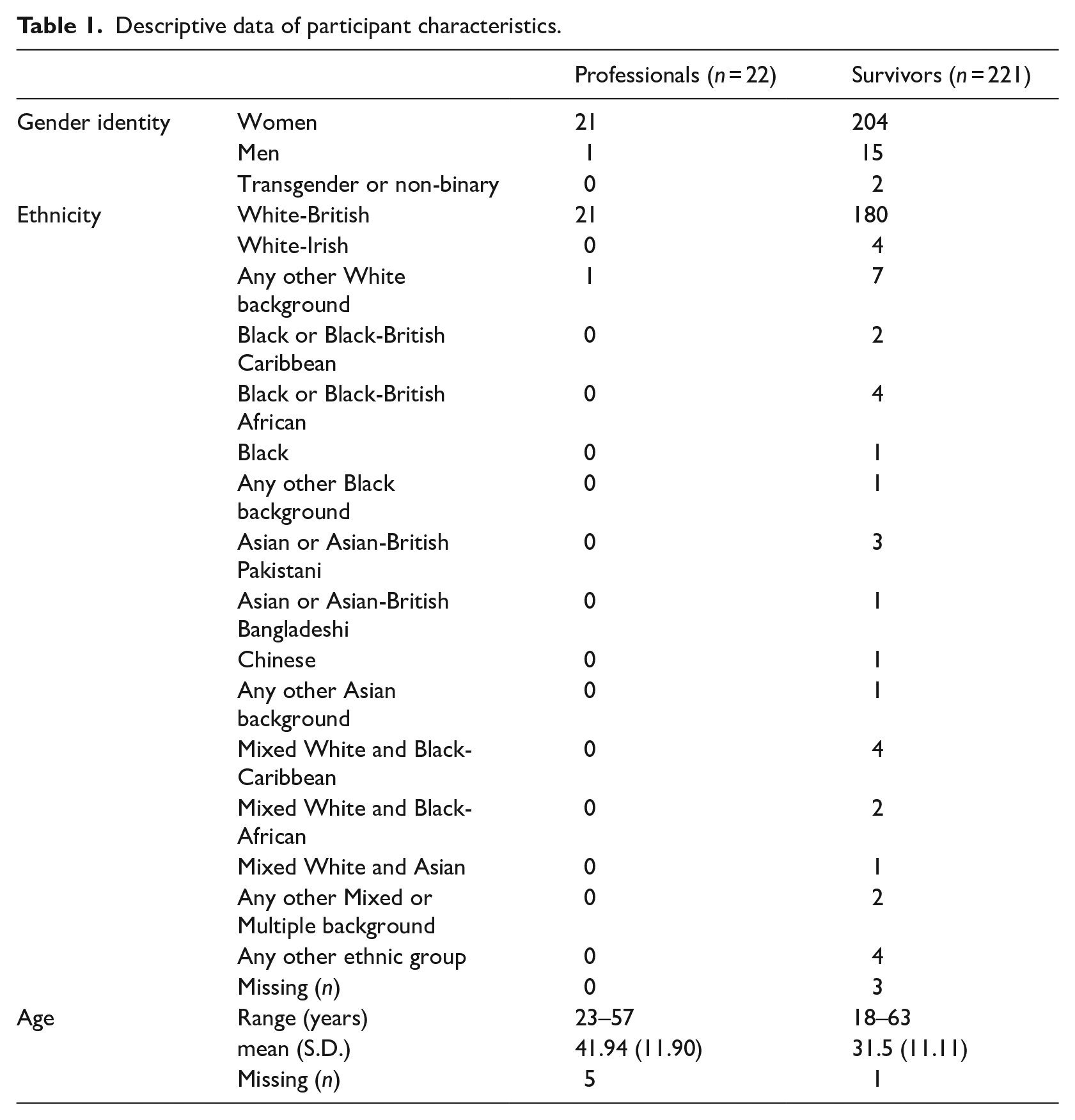
Professional participants worked in the sexual violence sector (n = 22) and were also interviewed as part of the MESARCH study. They were drawn from a wide geographic area in England: Midlands (n = 3), Eastern (n = 7), Southern (n = 11), and Northern (n = 1) areas. They were individuals working in SARCs (n = 14, across four SARC sites); voluntary sector sexual/domestic violence services (n = 4, across three organisations); strategy and commissioning (n = 3, across three geographic areas); and a police force (n = 1). Time working in their current roles ranged from 0.42 to 10 years (M = 3.61 years, SD = 5.15, n = 3 missing data), and in the sexual violence and abuse sector from 0.42 to 22 years (M = 8.02 years, SD = 6.45, n = 3 missing data). Table 1 summarises the demographic details of professional and victim and survivor participants.
Materials
Original interview materials were amended to capture the impact of COVID-19. To this end, an additional question was introduced into the interviews with victims and survivors (baseline, 6 and 12 months) that explored the impact of COVID-19, with only the responses to this question being presented here. This generated 284 responses on how COVID-19 had impacted people’s recovery journeys including access to and engagement with services, and whether there had been any other effects such as self-care in the aftermath of sexual violence and abuse. For the professional sample, additional questions were added to the original interview schedule that explored the impact of Covid-19 in relation to changes to services, the use of new approaches/technologies, and the perceived impacts on clients and themselves.
Procedure
Ethical approval was granted by the project lead universities’ ethics committees, and amendments to the methods of the main study precipitated by the pandemic were approved by the Health Research Authority (IRAS Project ID: 261455, a requirement for research that involves participants recruited through the National Health Service in England). Participants interviewed between April 2020 (the first lockdown started in March 2020) and June 2021 were asked about the impact of Covid-19. Professionals were invited from 15 (out of approximately 50) SARC sites across England that had agreed to be involved in the larger project. Professionals from agencies involved in referring people to SARCs (e.g. the police) and providing post-SARC care to service users (e.g. advocates, counsellors) were also recruited. In recruiting professionals, potential participants were contacted by the lead author, with information about the study to determine if they wished to participate in an interview. Interviews with professionals were audio-recorded and transcribed verbatim. Transcripts were quality-checked for accuracy and pseudonymised prior to analysis.
Service users who had been to SARCs were made aware of the larger project by sexual violence advocates (termed ‘Independent Sexual Violence Advisors’ in England) trained in the project’s research process. They used an introductory video developed by the research team and the lived experience group. For service users interested in hearing more about the study, advocates gathered information on their preferences for contact and interview (e.g. gender of interviewer) and details to ensure their safety (e.g. a phrase to let the research team know it was not a safe time to communicate). The research team then contacted service users and provided a participant information sheet and the opportunity to ask any questions. Participants were asked to agree to a set of consent statements. Interviews were then carried out by telephone and in line with the project’s safety protocol. Each participant’s response to the open-ended question about the impact of COVID-19 was documented verbatim.
Data analysis
Terry et al’.s (2017) analytic process to thematic analysis was followed for the analysis of the data. This approach advocates a ‘Big Q’ approach to thematic analysis that is positioned within a qualitative paradigm of analysis. The analysis was underpinned by a critical realist approach where reality exists that can be partially accessed through research, and knowledge can be produced that can implement change (Braun and Clarke, 2013). An inductive analysis was undertaken focused on being led by the data, with a primarily semantic approach to coding, in which codes and subsequent themes represent the explicit meaning of the data (Terry et al., 2017). The analysis began with familiarisation and code generation, with a subsequent process of theme development. This involved examining the codes for patterns and clustering, resulting in the drawing together of codes into a provisional thematic map. The initial thematic structure was developed by the second author, then reviewed and refined by the first author, and then re-checked again by the other authors. Discussions were held to assess any changes to the thematic structure and to re-check the fit with the data. Through this process, a final thematic structure was developed. This ensured that the analysis was quality checked, that the final themes were distinct and closely aligned with the data, and reflected a fit with the research questions.
Results
Two thematic diagrams (Figure 1 addresses the first research question, and Figure 2 addresses the second) were developed to display the themes generated. Themes that are numbered and are in bold text on the diagrams represent the dominant areas that are explored in detail below.
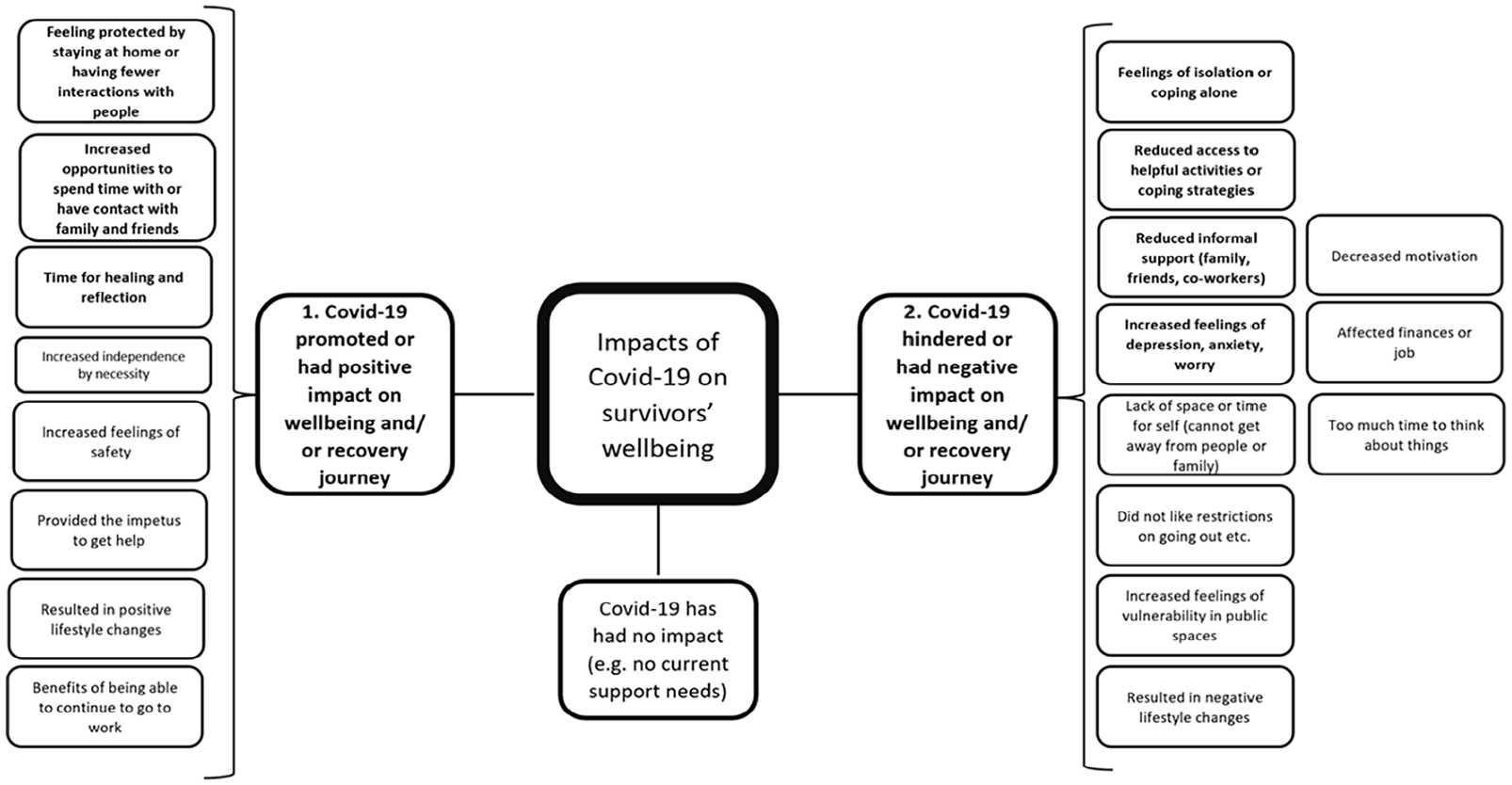
Themes relating to the impact of Covid-19 on survivors’ well-being.
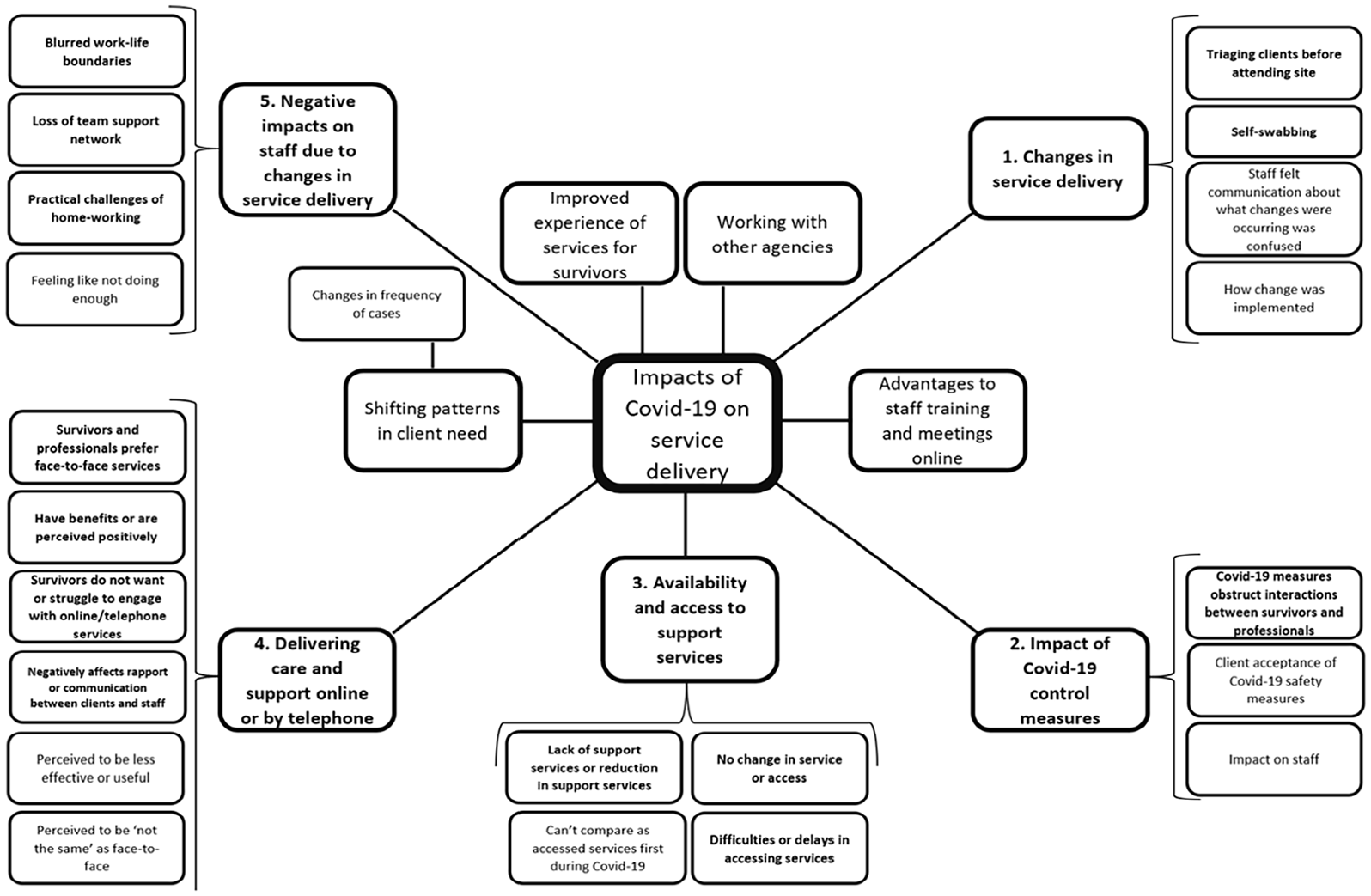
Themes relating to the impact of Covid-19 on service delivery.
Impacts of Covid-19 on victims’ and survivors’ recovery journeys and help-seeking
Victims and survivors emphasised several primary problems in relation to how Covid-19 hindered or had a negative impact on their well-being and help-seeking: (1) Increased feelings of depression, anxiety, or worry; (2) Feelings of isolation or coping alone; (3) Reduced informal support e.g. from family, friends, or co-workers; and (4) Reduced access to helpful activities or coping strategies. Victims and survivors spoke about how COVID-19 intensified or exacerbated their struggles with feelings of depression, anxiety and worry (e.g. ‘[it] made my anxiety and depression a lot worse. I have felt really low, not sleeping and suicidal’ (S237 1 year). These feelings coincided with other worries for some survivors: ‘The abuse happened and then a few months later Covid happened. I felt anxious and worried about health and making ends meet. I would say I was depressed a lot’. (S211 6 months). They also spoke about being alone (e.g. ‘I was stuck here a lot on my own’ S237 1 year) and a lack of contact and interaction with others: ‘I reported to [the ISVA service] and the police and then we went into lockdown. So, I went into a meltdown, facing all of that by myself (I lived alone) and was so isolated, I felt I was crumbling’ (S42 baseline). In terms of help-seeking, victims and survivors often referred to having reduced informal support. There were frequent references to not being able to see friends and family who were considered key sources of support, which affected emotional well-being or mental health: Normally when I’m in a low mood I would surround myself with people who would bring me up again, and just spend time with them, but I couldn’t do that during the first lockdown, so I found it difficult to not have that regular contact. (S168 baseline)
Victims and survivors’ sense of isolation in the aftermath of violence and abuse coincided with increased feelings of depression, anxiety, and worry.
Victims and survivors also experienced Reduced access to helpful activities or coping strategies; exercise was one of these with the closure of gyms during lockdown periods being keenly felt (e.g. ‘Things that I have in place like going to the gym have been taken away’ (S234 6 months)), along with other physical activities: ‘One of the things I love is dance, it’s part of my therapy, it’s been difficult not being able to access dance classes. It’s part of me, it really lights me up’ (S61 baseline).
Victims and survivors spoke about their recovery journeys slowing down, becoming more difficult (e.g. ‘it has been a lot harder trying to work through my issues in lockdown’ (S266 baseline)), or being disrupted or going backwards (e.g. ‘I feel like I’ve gone backwards after I’ve worked so hard for things to get things to normal’ (S254 6 months)).
While this isolation and loss of interaction was experienced negatively by most, just over a fifth of survivors perceived benefits to the national lockdown focusing on feeling protected by staying at home or having fewer interactions with people, and this period being considered a time for healing or reflection or having Increased opportunities to spend time with or have contact with family and friends. These participants found that the COVID-19 restrictions meant that they could avoid the challenges or anxieties associated with being away from home: It has also helped that I am not expected to go out of the house; I am nervous about leaving the house. I don’t want to leave, in that respect it is more sensible to stay at home, so I have an excuse. (S173 baseline)
Some victims and survivors felt that COVID-19 enabled them to have time for healing or reflection due to having more time available and fewer everyday pressures: ‘Yes it definitely has, and I would say very, very surprisingly, I think it has actually given me a lot of opportunities and the ability to do the healing process properly’ (S214 baseline).
Furthermore, this group of survivors perceived that they benefitted from the pandemic in having increased opportunities to spend time with or have contact with family and friends. This particularly focused on the increased availability of people and accessibility through digital methods: ‘I can talk to friends online, it’s been very easy for me to contact people because they’ve always being at home’ (S313 1 year)).
These findings represent the critical interactions between different levels of the ecological model, whereby the implementation of a national lockdown (at the exosystem level), primarily has a negative impact at the microsystem level for survivors in reducing their interactions with their social network and increasing isolation. However, these data also capture the recognisably smaller proportion of participants for whom these changes at the exosystem system represented positive influences on their microsystem with greater time to access their social network and time for healing and reflection.
Impacts of COVID-19 on service delivery
Integrating professional and victims and survivor voices, impacts on service delivery coalesced around the following: (1) changes in service delivery, (2) impact of Covid-19 control measures, (3) availability and access to support services, (4) delivering care and support online or by telephone, and (5) negative impacts on staff due to changes in service delivery.
Changes in service delivery
Participants spoke about how service delivery changed with the advent of Covid-19 representing the mesosystem level of the ecological model, with emphasis on the shift to approaches that reduced face-to-face contact. Professionals who worked in SARCs focused their discussions on the use of self-swabbing
1
and triaging of clients before attending the site, as policies and procedures (exosystem) that were directly introduced to address the advent of the pandemic. As part of this discussion, professionals shared how they determined the appropriateness of remote care to meet the needs of different clients, highlighting how service delivery (mesosystem) was influenced by exosystem elements: If the client has had any needs or disabilities or felt that it wouldn’t be in the client’s best interests to offer that remote over-the-phone assessment, then I’d be advised of that on that initial call from [private forensic services booking service] in which case I’d obviously close down whatever I’m doing this side, go across and get changed and ready into sort of full PPE [Personal Protective Equipment] to meet that client. (Crisis Worker 1)
Impact of Covid-19 control measures
Both professionals and victims/survivors highlighted the specific impact that COVID-19 safety policies and procedures had on service delivery. Professionals discussed the wearing of Personal Protective Equipment, whereas victims and survivors talked about restrictions, for example, they were not permitted to take a supporter with them to appointments. Overarching this was the view that Covid-19 measures obstructed interactions between victims and survivors and professionals. Professionals from SARCs particularly highlighted the triaging of clients (discussed earlier) as having an impact on the rapport and support that they could provide to clients: And you just think wow, because if you’re going in to have such an intimate examination for a disclosure of a sexual assault, and you’ve spoken to people over the phone about your most, private kind of personal information, then you come in and we’re all goggled-up, masked-up, gloves and aprons and stuff, and then you’re swabbed in and out within 20 minutes to half-an-hour. And yeah, you just feel so wrong. (Crisis Worker 2)
These impacts were specifically highlighted in relation to children: ‘we have to wear PPE for every examination, which I think for children can be quite scary and obviously you can’t build that same relationship with them’ (Crisis Worker 3). Participants raised concerns that this impacted on the quality of care being provided: ‘I think that’s the thing, it’s like not being able to give the level of service that I would normally be happy to give’ (Crisis Worker 2). This view was echoed by victims and survivors: ‘I feel nervous and alone but there will be a [unknown] lady in the live link room with me who will sit behind me but she doesn’t know what’s happened, and you can’t grab her hand for support’ (S257 6 months). One survivor reported a particularly negative experience associated with expectations about face coverings and how this impacted on her care when attending for a routine cervical smear test at her family doctor practice: I can’t wear a face mask due to anxiety. I booked in for a smear at GP [general practitioner], I explained to the receptionist, she was lovely and I was offered to try a screen [face shield]. I tried but I couldn’t do it. The nurse came out screaming at me, shouting at me put your mask on. Immediately triggered my Post-Traumatic Stress Disorder, I was deeply upset, I said to her ‘you should know better, you’re a health professional’. The receptionist brought me a cup of tea with sugar. I was so upset I couldn’t do the smear and I still haven’t had it. (S50 baseline)
Availability and access to support services
Access to services during the pandemic was an important theme for participants with nearly 60% of the sample commenting on this. Of these, half reported No change in service or access, however the remainder identified significant Difficulties or delays in accessing services and a Lack of support services or reduction in support services. Both victims and survivors and professionals identified that victims and survivors were experiencing longer waiting times, particularly for therapeutic or counselling services: I have been on a waiting list for counselling and when I joined the waiting list it was like an 18 month wait and [when] that period came I would have been sure to start that in December 2020 but because of Covid, it has all been put back. There have been delays in being able to have that and I don’t know when that will be. It will be coming up two years in May/June time that I will have been on the waiting list. (S232 1 year)
Waiting times to access standard appointments were also longer, specifically in accessing family doctors’ services/general practice: ‘It has been harder to get appointments for the doctors and stuff, it took me a good few months to get an actual appointment with my GP about antidepressants’ (S131 6 months). As services were only contactable online or via the telephone, victims and survivors were unable to make contact ‘I’ve tried and tried calling them and I never get an answer or reply from them’ (S247 1 year). Delays were also experienced in criminal justice processes: ‘It has slowed down the police investigation a lot’ (S26 baseline) and access to justice, with court cases cancelled or delayed on several occasions.
While this theme demonstrates the mixed experiences of participants in relation to availability and access to services representing exosystem factors, this theme should be carefully considered in the context of the next theme, whereby the mode or nature of interactions between survivors and service providers (microsystem) has changed significantly.
Delivering care and support online or by telephone
Half of the participants explored their perceptions of the shift to remote care and support, of these, nearly two-thirds of the victims, survivors, and professionals were negative about online/telephone service delivery, with strong preferences for face-to-face service delivery, particularly for counselling but also in relation to other services like family doctors/general practice and the police. For these participants, online/telephone service delivery reduced engagement in help-seeking and support (e.g. ‘Yes because of coronavirus, I can’t go in person so I’m waiting for when the clinic opens because I am not really wanting to speak about this over the phone’ (S23 baseline)) and victims and survivors reported not wanting this mode of support: ‘The therapist referred me to a mindfulness course which I started but I have stopped as it’s online’ (S255 6 months). Professionals spoke about clients who they believed had disengaged from services due to not being able to engage in online/telephone services. The appropriateness of this mode of care for younger and older clients also raised concerns. The issue of interactions between victims and survivors and professionals was also a feature of this theme (as seen in the Covid-19 control measures), where participants said remote care created new challenges in building rapport, which could impact on the trust/therapeutic relationship and presented a barrier between victims and survivors and professionals. Victims and survivors talked about the need to ‘have a proper chat’ (S161 baseline), that there was ‘more of a disconnect over the phone’ (S181 baseline), and that ‘It’s harder to build relationships online and [it] makes people’s body language harder to read’ (S26 6 months). Professionals echoed these concerns and said they worried they were missing important communication cues from clients: You can’t see how someone is, you know; some people we’ve spoken to over the phone have gone quite quiet at different points and you don’t know whether they’re just actually distracted by something and they’re fine or they make themselves a drink or something. Or actually they’re upset, and they’re struggling to answer the question or struggling to speak. (Deputy SARC Manager 1)
While a large proportion voiced negative views of this mode of care and support, 14% of survivors identified benefits of remote care, particularly in making services easier to engage with. In contrast to the views above, these participants felt that talking over the phone/online was easier because they felt ‘more relaxed’ (S50 baseline), that ‘the distance of a telephone call is better for me’ (S188 baseline) when talking about difficult topics, and that ‘it [speaking over the phone] didn’t feel like such a big deal’ (S37 baseline). Linking the mode of delivery with accessibility, victims and survivors welcomed not needing to travel and that appointments could fit more easily into a day, a view echoed by professionals who noted the ease of accessibility, and that this worked for particular types of clients (e.g. older adolescents).
SARC staff emphasised how triaging clients by phone reduced the time needed on-site at the SARC, where shorter attendance times were viewed again to increase the accessibility of services, particularly for clients with caregiving responsibilities. Staff reported feeling better prepared for clients when they arrived: ‘because we’ve done all that over the phone and got more info over the phone than we usually would, it means that we’re able to set up and prepare prior to the victim arriving’ (Deputy SARC Manager 1). Specifically in relation to children, staff talked about more opportunities to allay concerns of parents/guardians before attending and to learn about things that may make the visit easier for children to undertake: ‘We can think about, you know, if they say “oh, she loves Paw Patrol”, then we load up the iPad with a Paw Patrol video’ (Clinical Director 1).
Negative impacts on staff due to changes in service delivery
Professionals working in sexual abuse and violence services experienced a considerable shift from being co-located with their teams and colleagues at their usual service premises to individual home-working. In reflecting on this change, professionals reported Blurred work-life boundaries, demonstrating important organisational challenges to the segmentation between work and home, and the specific challenges given the nature of their work: I think an additional impact from this whole situation is like now that we’re doing email referrals from home, it kind of brings it into my kind of safe space and when I get home from work, I want to be home from work, I don’t want to be thinking about it and . . . it’s here, it’s in my house now, like, I’m reading about these awful things happening to people in my home. (Crisis Worker 3).
Participants referred to other negative impacts of lone-working and transition to home offices focusing on the loss of team support network, demonstrating challenges at the mesosystem level.
I think I’ve got more used to it now but I think in early lockdown I was really struggling because normally I’d be in the office and if I was on a really hard call or, you know, it sounded quite heavy, there would usually be someone in the office that would be like, ‘oh, are you okay? Do you want to go for a walk and a break?’ (Triage Worker 1)
While professionals talked about approaches that had been implemented in recognition of this issue (e.g. WhatsApp groups, more frequent check-in with managers), there was still a sense that self-care suffered in a context of home-working ‘when you’re in person in the office, at the minute [you feel you need to talk to someone], you get to just stop and talk about stuff’ (ISVA 1). This demonstrates the importance of mesosystem-level factors for the resilience of professionals, which ultimately impacts on quality and availability of care and support provided to survivors. Other impacts explored the practical challenges of home-working including the need to acquire suitable equipment and to access confidential, sensitive client information at home securely.
Discussion
The pandemic produced a recalibration of health and care service delivery and insights and applications that will be vital for buffering services and service users, including survivors of sexual violence (Majeed-Ariss et al., 2023)., against extraordinary events of the future. This study contributes to this knowledge having gathered in ‘real-time’ the voices of people who had been seeking support for exposure to SV when the pandemic hit, or were victimised during the pandemic period. Its novelty is in hearing directly about the experiences of sexual violence and abuse victims and survivors in accessing and engaging in remote care and how the pandemic was perceived to have affected their recovery journeys. The study additionally presents the perspectives of professionals from a range of health and support organisations to highlight the impacts of the wide-scale changes to service delivery and uncover new potential opportunities and challenges for the future of service delivery in this area. Discussion papers (e.g. Gunby et al., 2020) and research providing a snapshot of the impact of COVID-19 (e.g. Almeida, 2020) anticipated some of these challenges, however, this research grounds those factors in data provided by victims and survivors of sexual violence and abuse, augmented by professionals in the sexual violence sector. Although based in an English context, these impacts and their implications are relevant internationally; for example, the shift to remote care and support was undertaken globally (e.g. Polk, 2021).
Contributions to theory/model
In the context of the current study, the rupturing of normal daily life had serious implications for the coping mechanisms and help-seeking use by victims and survivors. In doing so, this demonstrates how the additional impacts of the pandemic disrupted recovery journeys. Victims and survivors reported worsening symptoms of depression, anxiety or worry, as well as increased feelings of isolation and depleted resources (e.g. reduced access to coping strategies such as exercise) and opportunities for recovery. In establishing safety, Herman (1992) identifies how survivors can oscillate between surrounding themselves with people at all times and isolating themselves entirely. In relation to the former, the pandemic significantly disrupted the opportunities that survivors had for contact with friends and family, frequently well-understood to promote positive well-being for sexual violence and abuse victims and survivors (e.g. Littleton, 2010). For the latter, a small number of survivors identified the benefits of the pandemic in relation to safety seeing the pandemic restrictions as a way to feel protected, reducing their interactions with other people, and considering this a time for healing. Alongside the impacts of the pandemic on well-being, the pandemic also disrupted usual pathways to support (e.g. shift to remote care), potentially undermining or protracting the remembrance and mourning stage of recovery. Victims and survivors reported reduced access to care, delays to care, and poor perceptions/experiences of remote care. In contrast, as with the findings in relation to safety, a smaller number of survivors reported benefits to the shift to remote care enhancing their ability to engage and process their trauma through remote means. Finally, in relation to reconnection, the impacts of the pandemic are clearly visible across the data in hindering a survivor from engaging more actively in the world. In summary, Herman’s (1992) trauma theory contextualises these findings in relation to how the pandemic may have slowed or protracted recovery. Furthermore, trauma researchers have determined that the pandemic itself, was experienced as a form of trauma or traumatic stress (Bridgland et al., 2021), adding further complexity to the recovery journeys for survivors of sexual violence during this time.
Previous research has identified a need for a more detailed understanding of the different factors of the ecological model and importantly, how these different factors interact (Campbell et al., 2009; Zinzow et al., 2022). This research delivers this by capturing interactions across multiple layers of the model and so extends our understanding of the ecological model in relation to help-seeking and recovery journeys. It demonstrates how the pandemic context exacerbated or produced barriers and facilitators to recovery for survivors by highlighting interactions between policies and procedures, such as Covid-19 safety measures as exosystem factors, and how these impact microsystem factors in the quality of interactions between victims and survivors and service providers. Of significance for this research was the importance of mesosystem factors, as an individual factor (e.g. interactions between professionals) but also in its interactions with other layers of the ecological model, specifically exosystem (e.g. accessibility of services) and microsystem factors (e.g. interactions between victims and survivors and professionals). Therefore, the data offer multiple instances of interplay and influence between the levels of these factors. In doing so, it presents a more detailed and nuanced comprehension of how these levels may exacerbate or worsen health outcomes for victims and survivors of sexual violence and abuse.
The ecological model was also relevant to findings relating to professionals. Concerns were raised in the early literature published in the pandemic regarding service delivery at the mesosystem level (e.g. Gunby et al., 2020). These data document those findings, but also highlight the critical need to resolve the associated challenges facing professionals at this mesosystem level linking theory to practice, specifically in relation to blurred work-home life boundaries and reduced access to team support, which are magnified among those working in the sexual violence and abuse services (Crivatu et al., 2021). While many organisations returned to face-to-face services as pandemic restrictions reduced or were removed, the majority continue to deliver their services using a blended approach (The Survivors Trust, 2020). Urgent consideration therefore needs to focus on how these staff will be supported, to reduce the likelihood of them experiencing the negative impacts of working in this sector, for example compassion fatigue, burnout. Factors such as organisational culture and supervisor and co-worker support represent potentially interacting factors across macrosystems and mesosystems, so it is important to understand the role of such factors in the specific context of those who work in the sexual violence sector. For example, supervisors should consider their role in supporting staff in this new way of working to manage their work-life domains. Ultimately, the resilience of this sector impacts on the quality of the support provided to survivors of sexual violence and abuse. Given the findings of this study suggest that there may be increased service use by victims and survivors of sexual violence and abuse in the longer term as a result of the pandemic, this issue is of critical importance to ensure there is a robust and resilient sector.
Contribution to practice
In the context of the current study, the rupturing of normal daily life had serious implications for victims and survivors. Not being able to address the mental health sequelae of abuse and the cumulative effects of experiencing the pandemic, are likely to have knock-on effects for economic and social well-being, for education, and in respect of caring responsibilities and looking after children. If victims and survivors experience longer periods where they need help (e.g. waiting for their legal case to be heard in court), service providers are likely to find that clients remain with them longer and/or may require more intensive support and therapy where disclosure has been delayed and ‘early’ intervention has therefore not been forthcoming (e.g. Bicanic et al., 2015; Ruggiero et al., 2004). Post-pandemic service providers have continued to adapt, but consideration of longer-term plans for their service is needed, specifically focusing on how the pandemic has shaped the needs of clients and the timing of disclosure (e.g. survivors reporting historic abuse; victims of sexual offences where there are complex needs linked to social and housing circumstances, disability, and substance use). Such changes in the length of support and nature of presenting or comorbid issues are likely to add further strain to a sector that was already over-stretched and under-funded prior to the pandemic (e.g. Rape Crisis, 2021).
Changes to modes of service delivery (e.g. the shift from in-person to remote care) raised multiple concerns in our participants, suggesting an inefficient mechanism for supporting recovery, but these negative perceptions need to be set in context. First, the provision of remote care was unlikely to have caused more harm than not providing the care at all. Second, and as noted by Smith et al. (2022), these changes in delivery were imposed on clients, rather than selected by choice, which may have affected how clients perceived them. Brown et al. (2022) argued that if services are to be delivered through remote technology platforms or simply by telephone, it is critical to prepare victims and survivors and their carers appropriately and manage people’s expectations, suggesting a pathway to where clients may find this mode of delivery more acceptable. Furthermore, in these data, positive responses about remote care emphasised ease of engagement and factors that could increase the accessibility and quality of services provided to sexual violence and abuse victims and survivors, while also reducing rates of cancelled appointments (of particular relevance when resources are stretched). There are many considerations in selecting remote or in-person care including the stage the person is at vis-à-vis disclosure, and the complexity of their needs and their circumstances (can a client achieve safety and confidentiality at home?); and importantly the nature of the care and support being delivered. On the one hand, providing advocacy and low-intensity emotional support remotely may work quite effectively for providers and clients alike. For therapy and counselling, some therapies, for example, trauma-focused CBT in Acierno et al. (2021) do lend themselves to remote delivery, however, others (e.g. EMDR) may require in-person interaction. The resulting message from this current study is that victims and survivors are not a homogeneous group and differ in their needs and support requirements. The sector itself frequently recognises this, but more broadly, commissioning frameworks need to acknowledge that a one-size-fits-all approach specifically in relation to the mode of delivery, that is that either in-person or remote care should be provided, is unlikely to represent best practice in supporting clients. Therefore, commissioners may need to facilitate processes that enable organisations to consider how to extend client options in respect of how support is provided–it need not be a dichotomous set of possibilities. Within organisations, establishing the needs and preferences of clients could encompass aspects set out in Box 1.
Considerations in selecting an approach to service delivery.
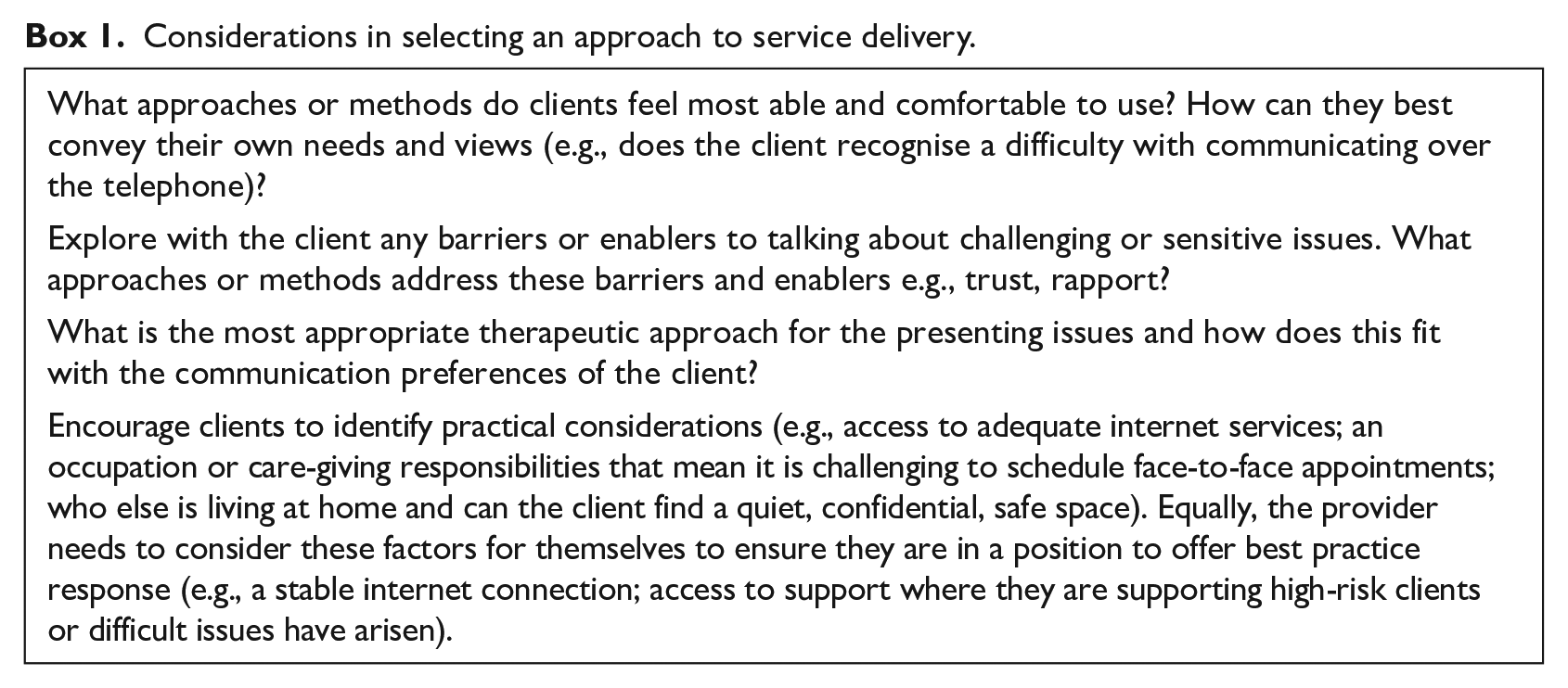
This decision-making process is most important at the beginning of service use; however, organisations will know that clients’ needs can change over the course of service engagement. This means that services should reflect on whether and how they can/will provide support flexibly, where clients may shift modes of delivery according to their changing needs on their recovery journey. These are not small considerations, particularly in the context of resource constraints; however, the professionals within this study recognised the cost-effectiveness of ubiquitous technology-based support solutions.
Limitations
While the research was possible due to an existing research infrastructure (ongoing longitudinal study with survivors of sexual violence post-SARC), the exploration of the impact of COVID-19 on victims' and survivors’ journeys was a small component of the full interview. A greater focus on the impact of Covid-19 may have uncovered additional experiences. We interviewed victims and survivors post-contact with a SARC and there were variations in their recovery journeys and experiences. For example, not all were involved in criminal justice processes and there was great variation in the stage of this process in those that were, so most had not experienced court trials, and so would not have been able to comment on these aspects. The participants in the MESARCH study represent a specific, help-seeking sample and, as such, do not represent victims and survivors of sexual violence and abuse across the English population. For example, SARC users more often seek help for stranger and acquaintance sexual assault (Lovell et al., 2021), which may carry less stigma and therefore promote capacities to seek help. Finally, as the responses were documented verbatim by interviewers, rather than being audio recorded, there is the small potential for loss of meaning or misunderstanding of content in the contemporaneous noting of these responses.
Conclusion
This study has identified important implications of the pandemic for victims and survivors, professionals, and service use in the future, spanning both theory and practice. COVID-19 amplified the challenges of living as a victim and survivor of sexual violence and abuse, impinging and interacting across multiple levels of the ecological model and subsequently diminishing pathways to help-seeking across health services, voluntary sector support, and criminal justice. Experiencing sexual violence and abuse significantly disrupts people’s lives (WHO, 2013) and the challenges to recovery journeys of victims and survivors identified in our research (of which seeking access to justice and therapy are key parts) means that those impacts continue to ripple across the lives of victims and survivors, their families, children, and other supporters. Future research exploring the longer term impact of the pandemic on victims’ and survivors’ recovery journeys is needed to provide a comprehensive understanding of their experiences. This research also needs to include victims and survivors who did not access SARC services as their experiences may be different from the specific help-seeking sample in our study.
The pandemic amplified the ‘emotional’ work associated with providing services to victims and survivors of sexual violence and abuse, with less recourse to sources of support for staff against a backdrop of blurred work-life boundaries and a changed mix of clients accessing services. Organisations need to consider carefully how they can support staff to mitigate any potential negative impacts to the new ways in which they work, reducing the likelihood of burnout and compassion fatigue and avoiding further reductions in staffing and resources in the sector. The research has highlighted some positive developments as a result of adapting to the pandemic, in terms of identifying new methods and strategies that may be integrated into best practice responses to sexual violence and abuse. For example, triaging clients before attending a SARC may increase the accessibility of the services for clients with particular needs. This evidence can inform service responses to future global crises, and remains important, even now, to increase the accessibility and ease of availability of services for some clients. This remains an important consideration for victims and survivors of sexual violence and abuse, who frequently experience barriers to care and support.
In summary, empowerment through offering ‘options’ is a hallmark of a good practice response in this context; the experiences of victims and survivors and organisations adapting to pandemic conditions has uncovered advantages of cost-effective, ubiquitous technology solutions for providing information, advocacy, and short and long-term support. There is significant scope for these opportunities to be captured and integrated into service delivery more long-term. However, these come with the important caveat that any novel service improvement should be underpinned by client choice, robust infrastructure (e.g. staff are supported; confidentiality is guaranteed on both sides), and monitoring and flexibility to ensure that the service meets the changing needs of the client.
Footnotes
Acknowledgements
The authors would like to acknowledge the support of Rosie Stone and Olufunmilola C. Ladeinde for their support in preparing the data for analysis.
Furthermore, the authors would like to extend our thanks to all professional and survivor participants who gave their valuable time to provide their important insights that have shaped this paper. We would also like to thank our lived experience group in continuing to provide invaluable perspectives that have enabled us to shape our research in a way that is trauma-focused and survivor-informed.
This project is funded by the National Institute for Health Research (NIHR) (HSandDR programme (16/117/04)). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.