
Abstract
Background:
Discussing end-of-life care with people with dementia and their family soon after diagnosis is a crucial aspect of professional care. Research in the hospital setting is scarce.
Aim:
To investigate how often end-of-life issues and euthanasia are discussed during hospital consultations with people with dementia; identify who initiates these conversations; explore physicians’ perceptions of their own role in these conversations compared to actual practice and physicians’ views on the family’s involvement.
Design:
Convergent mixed-method study.
Setting/participant:
11 Dutch hospitals involving 31 physicians.
Results:
End-of-life topics were discussed in 36% of consultations (in regional hospitals, 53%; in academic settings, 27%), and predominantly during diagnostic consultations (54%). Euthanasia was discussed in 21%, often initiated by the patient (60%) or the family (31%). Family members were present in 96% of consultations. We identified 3 themes. (1) Struggle to initiate end-of-life conversations. Physicians acknowledged the importance of timely end-of-life discussions, but struggled to initiate those discussions. Introducing euthanasia is considered undesirable. (2) Appreciation and concern about family input. Physicians’ experiences of family involvement were positive in both end-of-life and euthanasia conversations, yet the latter also raised concerns. (3) Moral concerns regarding euthanasia for dementia. Physicians emphasized the importance of raising patient awareness about other end-of-life options.
Conclusions and relevance:
End-of-life conversations with patients with dementia are not standard practice in the hospital setting. The availability of euthanasia can narrow patients’ perspective on other end-of-life options. This hinders physicians from initiating end-of-life conversations and possibly end-of-life decision making and care.
End-of-life conversations with patients are widely recognized as important in dementia care, particularly during the early stages of dementia.
Healthcare professionals, patients, and their families view initiating end-of-life conversations as mostly the responsibility of healthcare professionals.
People with dementia often rely on their family to express end-of-life and euthanasia wishes, which can pressure physicians and lead to moral dilemmas.
End-of-life issues were discussed in 36% of hospital consultations for patients with dementia in this study in the Netherlands, and euthanasia was discussed in 21% of consultations usually at the initiative of the patient or a family member.
Physicians generally have positive experiences with families in end-of-life and euthanasia discussions with minimal reports of familial pressure.
Physicians struggle to initiate end-of-life conversations due to concerns that (the availability of) euthanasia narrows the patient’s perspective, which can hinder end-of-life care and decision making.
Policy must clarify whether hospital doctors or general practitioners hold responsibility for initiating end-of-life conversations in dementia care
Healthcare should remove barriers by providing time, training and structured formats to embed these conversations into routine dementia care.
Further research is needed into the influence of euthanasia on the perceptions of death and the acceptability of natural dying in particular for people with dementia.
Introduction
Talking about the end of life is a crucial aspect in professional care for people with dementia, particularly in the early stages of dementia.1–5 This is reflected in the international guidelines of the European Association for Palliative Care 6 and in the recently updated dementia guidelines from the Dutch Federation of Medical Specialists. The latter states that healthcare professionals in the clinical outpatient setting should actively ensure that end-of-life conversations are initiated shortly after diagnosis of dementia rather than merely inquiring after information needs regarding end-of-life care. 7 Research shows that patients, families and healthcare professionals mostly see initiating end-of-life conversations as the professional’s responsibility.6,8,9 However, reluctance from all parties to initiate these conversations is hindering advance care planning. 10 Other studies point out the difficulty of end-of-life conversations as a result of the moral sensitivity of the subject.11,12 Also physicians feel unprepared due to limitations in training, communication skills, and self-confidence.13,14
In countries where euthanasia or medically assisted dying is legal such as in the Netherlands, end-of-life discussions often involve considering euthanasia. However, euthanasia for people with dementia remains controversial in many of these countries. Legal requirements (Box 1) add complexity, as patients must personally initiate the conversation to ensure their wishes are expressed without external influence.11,15,16
Euthanasia in the Dutch context
In euthanasia, the lethal medication is administered by the physician, whereas in physician assisted suicide the patient, under the supervision of the physician, takes the lethal medication themselves. Both are governed by the same legislation and are subject to identical rules and procedures.
Euthanasia or physician assisted suicide can be requested by the patient only, it cannot be requested on the patients behalf. The following six rules of due care must be met:
1. The request is voluntary and free of external pressure.
2. There must be unbearable suffering with no prospect of improvement.
3. The patient is informed and understands the information.
4. There is no reasonable alternative (e.g. surgery, medication, therapy).
5. At least one other independent physicians has seen the patient to assess the due care criteria.
6. It must be carried out in accordance with the guideline of good medical care.
All cases of euthanasia and physician assisted suicide must be reported and will be reviewed by an independent committee.
Euthanasia based on an advance directive is legally possible, but unbearable suffering remains a requirement; in practice, euthanasia in advanced dementia is rare (6–8 times per year).
Complex cases such as dementia or psychiatric disorders, are often referred to the specialized national ‘euthanasia expertise center’. They advise, support and guide physicians who provide euthanasia to a patient. They also provide euthanasia for patients whose own physician does not wish to perform euthanasia. The euthanasia expertise center operates within the same legal framework described above.
Another important and under investigated factor in these conversations concerns the role of informal caregivers, usually family. Research shows that as dementia progresses, their involvement in end-of-life decision making increases. 3 In countries that permit euthanasia family is also involved15–17 in, for example, expressing the patient’s euthanasia wish and subsequently determining the right moment for euthanasia.18–20 Involvement of family members in conversations about the end of life or euthanasia may be desirable or necessary but it can also lead to moral dilemmas for physicians in distinguishing between the patient’s and the family’s wishes.11,14,21
Unlike research in long-term care and hospice settings, research on end-of-life conversations with people with dementia in the hospital setting is sparse. Therefore, the aim of this study is to investigate 1 how often end-of-life issues and euthanasia are discussed during hospital consultations with people with dementia 2 ; who initiated these discussions 3 ; how physicians’ view their role in these conversations and whether actual practice is in line with this view; and 4 physicians’ views on family involvement.
Method
Design
The study employed a mixed-method approach with a convergent design, in which qualitative and quantitative data were collected in parallel, analyzed separately, and subsequently integrated to compare results and provide a comprehensive response to the research questions. 22 First, we conducted a prospective survey among physicians to examine the frequency of discussing the end of life during consultations, who initiated the discussions, and the main focus of discussions, including whether euthanasia was discussed. Second, we interviewed these physicians on their perceptions of their role and the family’s role in end-of-life and euthanasia conversations. The quantitative data report on actual practice, which we integrated with the qualitative interview data for deeper insights into physicians’ opinions. A weaving approach to the discussion ensured a coherent and unified analysis. 22
Setting
The study is conducted across the five regions of Dutch memory clinics in academic hospitals, which primarily focus on diagnostics and second opinions, and in regional hospitals in the same area, which mainly provide follow-up care after diagnoses.
Population
The study targeted physicians with a specialty in either geriatrics or neurology or internal medicine who specialize in geriatric medicine as well as their physician assistants. Below we refer to all groups as ‘physicians’.
Sampling and recruiting
We recruited the participants through personal contacts, snowballing and emailing heads of relevant hospital departments in the selected region. If they expressed interest, we sent an information letter with a consent form. If they were unresponsive after 2 weeks, we reminded them by email or telephone, which frequently resulted in (digital) meetings explaining the study’s goals and procedures.
Survey
Participating physicians each received a set of 10 links to a consultation survey landing page. Two participants requested additional links. Over 2 months, the participants were invited to completed a survey after each consultation with a patient with dementia (Supplemental 1). The survey took 3–5 min and was administered digitally using Castor electronic data capture (Castor edc, Amsterdam). The data were collected between July and December 2024.
Interviews
The first author (TSF, female ethicist and PhD candidate) conducted semi-structured interviews between September and December 2024, on location or digitally (Microsoft Teams) following an interview guide (Supplemental 2). All interviews were audio recorded and then deleted immediately after double-checking the transcription. Names of participants were replaced by codes. Participants received interview summaries for verification; three had minor remarks.
Analysis
The quantitative data were analyzed with descriptive statistics using SPSS version 30 (IBM, 2024). TSF, PS (female ethicist) and JvK (female geriatrician) analyzed the interview data using a reflexive thematic analysis following the six steps of Braun and Clarke.23,24 Atlas.ti 25 (2024) was used to manage and analyze the qualitative data. Codes were identified using an open coding and inductive analysis. PS and JvK independently coded five interviews, while TSF coded all interviews. All authors compared, discussed and revised the codes until consensus was reached, after which TSF recoded all interviews accordingly.
Ethics
The Medical Research Ethics Committee Leiden Den Haag Delft decided the study was exempt from the Medical Research Involving Humans Subjects Act (WMO, reference number 24-3032, 14 May 2024). No patient identifying information or identifying information on family members was collected.
Results
Survey
Of the 5 academic memory clinics, 4 participated with 14 physicians and 1 physician assistant. Of 20 regional hospitals, 7 participated with 17 physicians. Five hospitals did not respond, eight declined due to time constraints or treating a limited number of patients with dementia. We interviewed one physician who initially declined, indicating the department policy was to refer patients with dementia to general practitioners or case managers to discuss euthanasia.
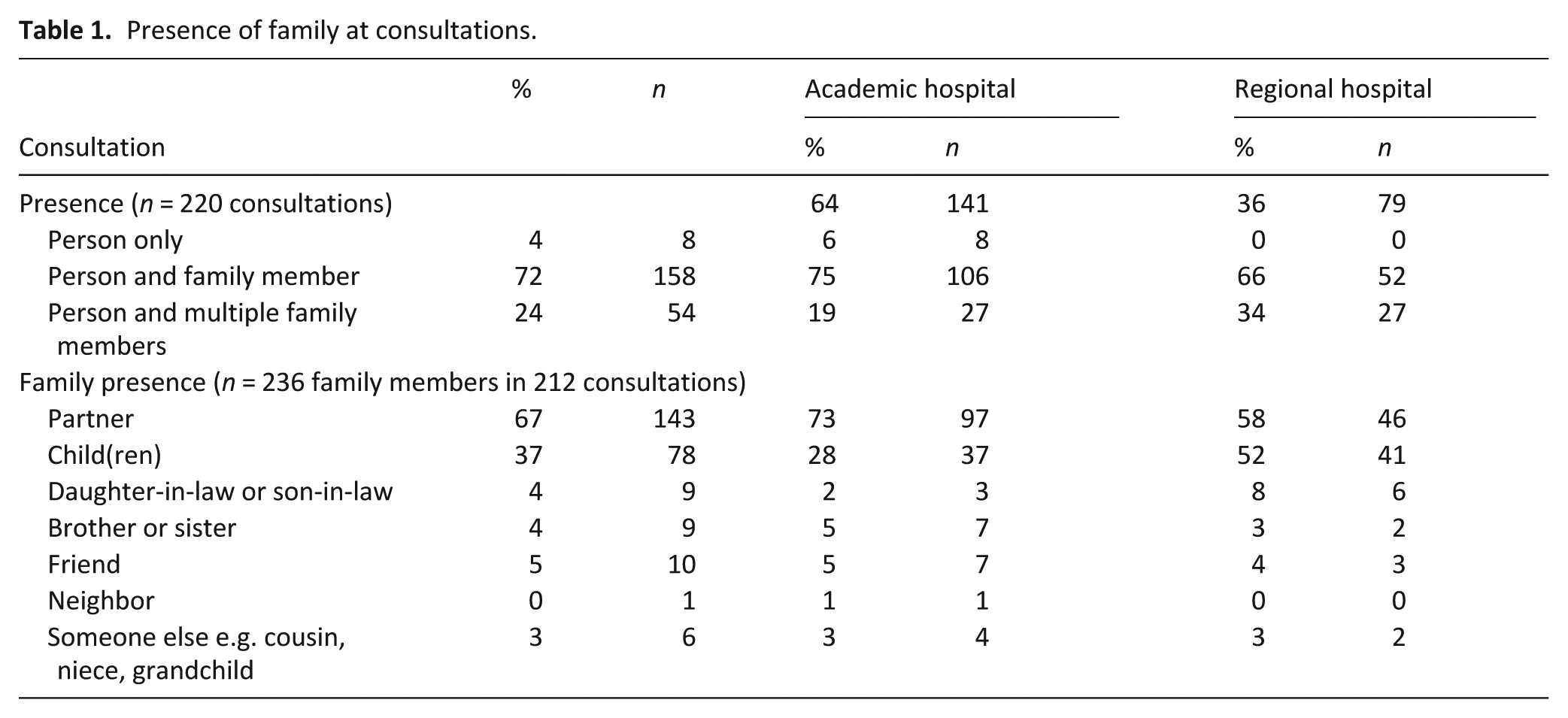
A total of 220 surveys were completed by 31 physicians: 141 surveys at academic hospitals with a median of 6.5 (IQR 8) per physician and 79 surveys at regional hospitals with a median of 4 (IQR 5). Family or other care partners were present in 96% of the consultations, mostly (67%) the patient’s partner (Table 1).
Presence of family at consultations.
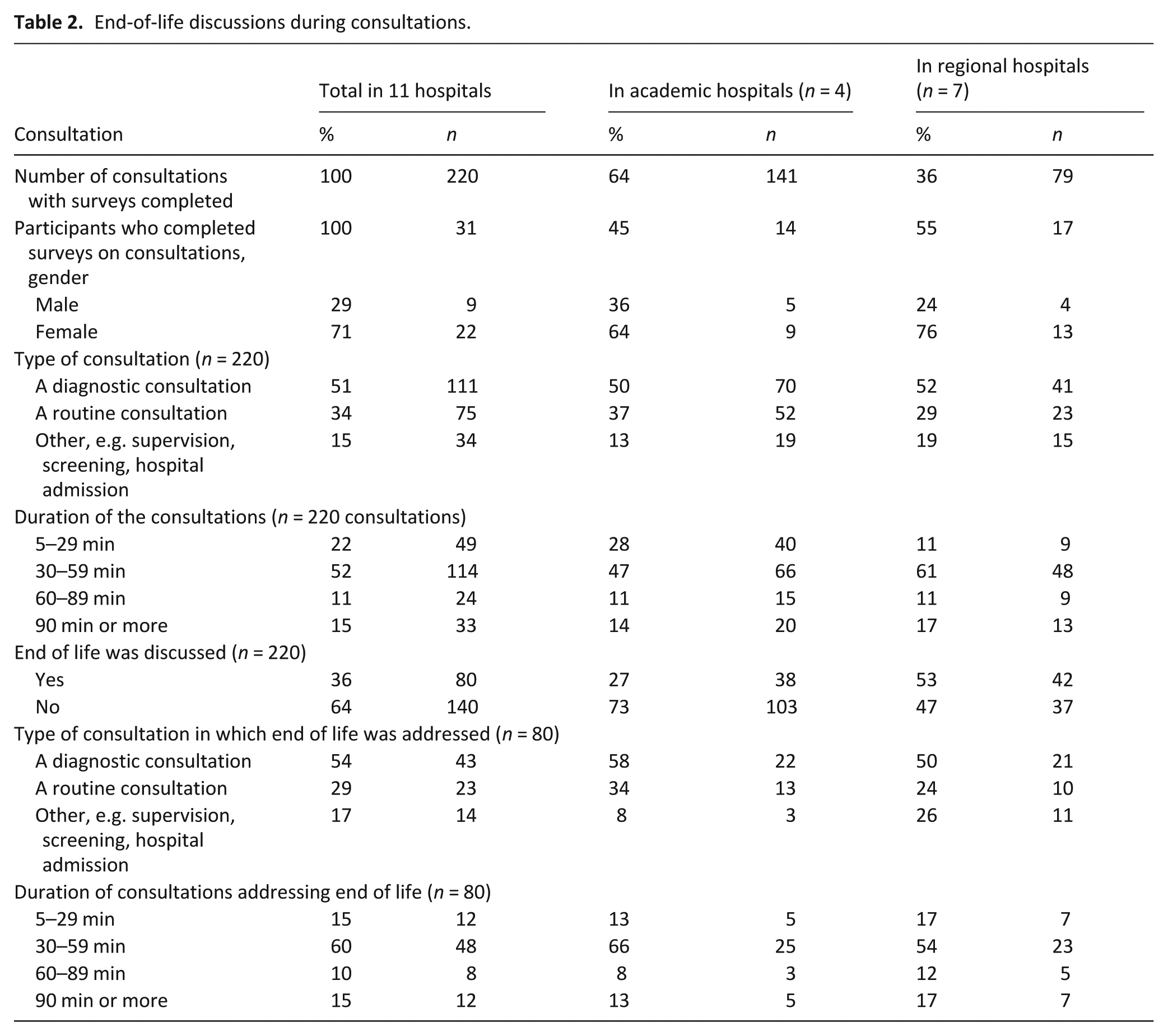
The reported consultations concerned dementia diagnosis (51%), routine consultations (34%) or other (15%; Table 2). End of life was addressed in 36% of these consultations. In academic hospitals the topic was addressed in 27%; compared to 53% in regional hospitals.
End-of-life discussions during consultations.
Euthanasia was discussed in 21% of consultations (Table 3). In these consultations, 62% of patients in academic hospitals expressed a wish for euthanasia, while in regional hospitals, 38% expressed a wish for euthanasia. A follow-up conversation on euthanasia with either a nurse practitioner (42%) or the patient’s general practitioner (36%) was advised in the majority of consultations, usually at a regional hospital. Physicians referred 13% of patients to the euthanasia expertise center (academic hospitals,7%; regional hospitals, 25%). There were no other appreciable differences between academic and regional hospitals.
Euthanasia discussion during consultations.
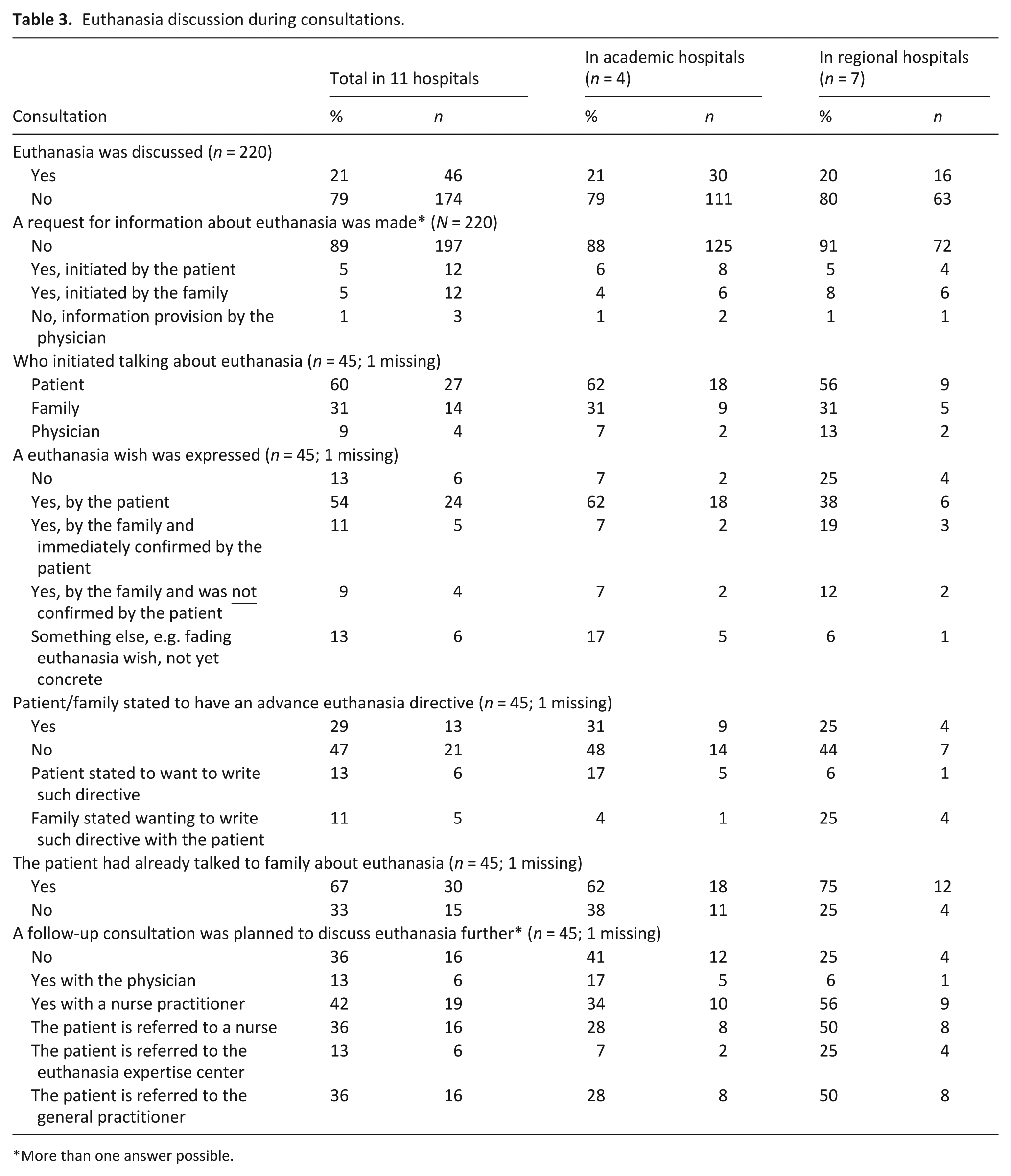
More than one answer possible.
Interviewees
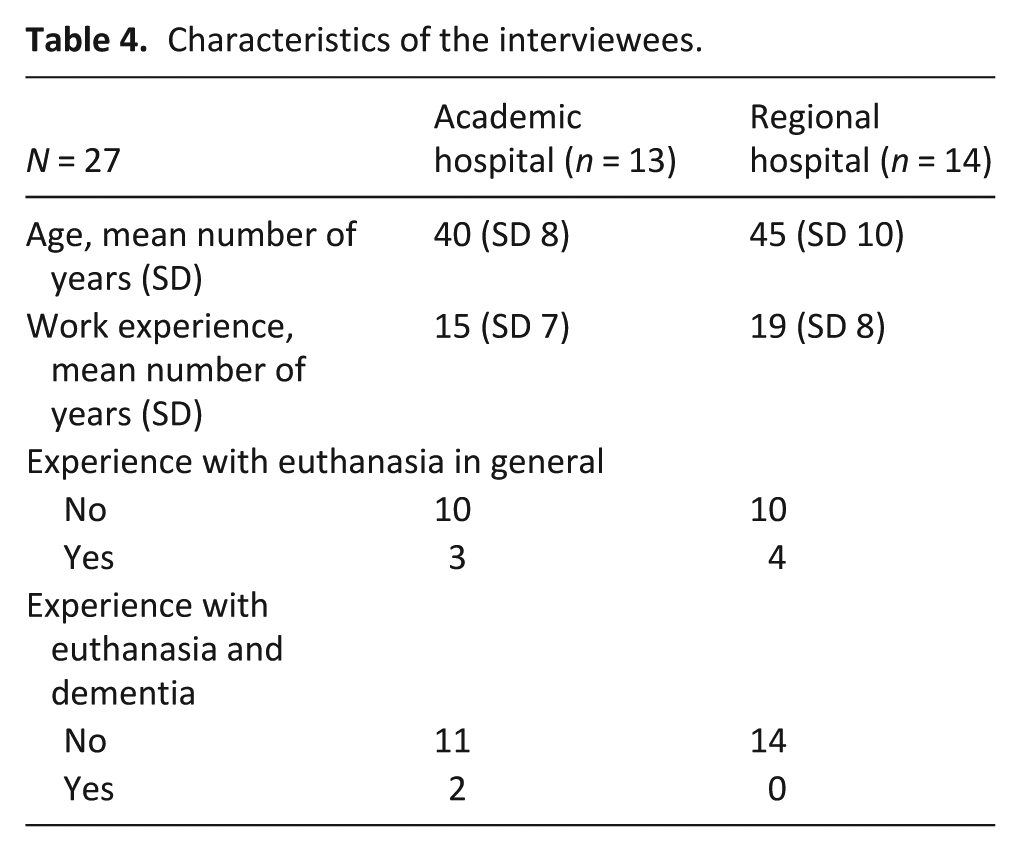
27 of the 31 survey participants were interviewed (14 academic, 13 regional). Three participants declined due to time constraints and one was on leave. The interviews lasted 30–45 min. Participants provided additional information about their age, years of work experience, experience with euthanasia and euthanasia with dementia (Table 4).
Characteristics of the interviewees.
Interview findings
Three themes were identified regarding physicians perceptions of their own role and that of family in end-of-life and euthanasia conversations involving dementia.
Struggle to initiate end-of-life conversations
The physicians emphasized the importance of discussing end-of-life care with patients with dementia to determine their preferences regarding, for example, intensive care admission, do-not-resuscitate orders, and treatment refusal. When patients or their families bring up such topics, physicians would engage in conversations, address concerns, and provide support.
However, in practice, physicians found it challenging to initiate these conversations themselves. Many indicated feeling hindered by time constraints and found diagnostic consultations too overwhelming and stressful for the patient. Since physicians typically interact with the patient once or twice, and only for diagnostic purposes, they often stated that general practitioners should conduct advance care planning conversations.
‘Yes, I find that very difficult. In an ideal world we should definitely do that (. . .) In practice I don’t discuss it much because I see people in the outpatient clinic and I make a diagnosis, that is very emotional and then also to talk about the end-of-life. . . That is too intense for them, so I don’t do that. But I don’t let them come back either. But I do think that there should be more attention on this’ (P27)
In an emergency situation where decisions must be made quickly and there had not been a timely end-of-life discussion, physicians reported feelings of stress, anger, and powerlessness. The physicians considered end-of-life care a sensitive subject, which they said they discuss in indirect terms. Some reported that the subject was insufficiently covered in their medical training and that they learned it ‘on the job’. Older physicians, in particular, indicated that having more experience enabled them to emphasize end-of-life care and adopt a more thoughtful approach to treatment.
‘You have to be a bit more seasoned and have a bit more flying hours because it is difficult. You avoid it more easily when you are young. I did that when I had just graduated. Then you are inclined to treat everything. (. . .) I myself have already lost both my parents and you also notice that this does something to you. How you look at what is still humane and what is quality and that kind of thing.’ (P25)
All physicians were aware of the guidelines of the Dutch Federation of Medical Specialists. When asked to reflect on a specific section regarding the physician’s role in discussing end-of-life topics, most stated that they agree with it, as long as it aligns with the relationship they have with their patient and when end-of-life is not a mandatory topic during a diagnostic consultation.
Regarding euthanasia, most physicians said they do not want to initiate the conversation because this can give patients the impression that euthanasia is a reasonable option. The few who do initiate a discussion on euthanasia said they use indirect or veiled language. When patients bring up the topic, the physicians provided information, advised on legislation, and referred them to their general practitioner or the euthanasia expertise center.
Appreciation and concern about family input
The physicians’ experience with family in end-of-life conversations was positive. They felt that family are mostly supportive and give essential insight into the patient’s life story, values and wishes regarding end-of-life care, especially when a patient reaches a more advanced stage of dementia. The physicians were concerned that family might not act in the patient’s best interest or pressure them to accept or refuse treatment. However, most had not actually experienced this.
Physicians generally found it helpful or even desirable when family mentions euthanasia, but they emphasized the importance of refocusing the conversation to the patient. Some physicians felt pressured by the family to end the life of the patient. Nevertheless, these physicians displayed empathy with the distress that arises from witnessing a loved one’s suffering and the desire to do something about it.
‘Yes, of course there is sometimes a fuss about it, in the sense that for example it takes too long for the family member to reach the natural end of life. That they can no longer bear it.’ (P8)
The physicians noticed that patients and family often have limited or incorrect knowledge about end-of-life care and available medical interventions. They reported common misconceptions that euthanasia on the mere basis of an advance directive is possible or that family can request euthanasia on the patient’s behalf. They indicated that this can lead to disappointment when euthanasia cannot be effectuated.
‘Some family members made a promise to the patient. [The patient] said: ‘if I can no longer do this, I want euthanasia’. So family members sometimes feel responsible for carrying out or initiating the wishes of the patient and are sometimes powerless in that.’ (P30)
Moral concerns regarding euthanasia in dementia
The physicians expressed having moral problems with euthanasia in dementia, because of the difficulty in assessing, as dementia progresses, the following: (1) unbearable suffering, (2) decision-making competences and (3) changes in personality and wishes. Some physicians indicated a change in their own moral evaluation from a permissive to a more reserved perspective.
‘I found it quite difficult, especially when it first came up. Because I was always quite an advocate of euthanasia. I still am in some cases, but also in many cases not.’ (P19)
All respondents stated euthanasia, in principle, should be accessible for people with dementia; however, only a few were willing to perform it themselves. Several physicians expressed concern that the original intention of euthanasia as a last resort is gradually shifting in society to normalizing euthanasia as a reasonable option in medical care.
‘I find euthanasia really complicated because personally, (. . .) it would truly be a last resort, only if there’s absolutely no other option. But of course, that’s entirely shaped by my perspective on life.’ (P10)
Several physicians highlighted that while the media encourage open discussions about euthanasia, it also spreads inaccurate information and distorted portrayals. Other concerns included society’s lack of attention to the intrinsic value of people with dementia, tendencies to want to control all aspects of life and death, and lack of awareness of the complexity and pressure for those who actually have to perform euthanasia.
‘It is not normal medical practice. Legally not, but of course also ethically. I would find it really sad if euthanasia were to become an easy access, threshold-free option. I think that it does not do justice to the value of the life of a patient with dementia or any other disease, but above all it does not do justice to the pressure, the burden and the complexity that it places on the healthcare professional who has to do it.’ (P1)
Some physicians emphasized the importance of increasing patients’ awareness about less invasive and complicated options for dying, such as refusing treatment or food. This was illustrated in a case in which the son of an older patient with dementia who was hospitalized with pneumonia insisted on euthanasia immediately after admission to relieve his father’s suffering. The physician explained that euthanasia is not an option in this case because the rules of due care cannot be met.
‘But then that man [the patient] suddenly went into pulmonary decline, so his lungs deteriorated. And then I talked to the patient and his son about whether he wanted to be treated for the pneumonia or not. Well, then they chose not to treat and the man died within a day. And this was an easier way than going down the euthanasia path. That is something that is often forgotten by ordinary people, that it can also be done that way.’ (P14)
Discussion
Main findings and comparison with other studies
The physicians who were interviewed agree that timely advance care planning or end-of-life conversations are important in the hospital, as recommended in current medical guidelines.3,7,8 Our quantitative shows, however that in practice, these conversations occur in approximately one-third of the consultations. The interview data offer explanations for this as physicians mention feeling constrained to actually initiate the conversations by time pressure and insufficient training. They consider the diagnostic consultation an inappropriate time for such a sensitive topic. However, our quantitative findings show that diagnostic consultations in which the end of life is discussed last no longer than standard consultations. Moreover, in the regional hospitals, end of life topics were addressed more frequently than in academic hospitals (53% vs 27%). This might be explained by a more long-standing doctor-patient relationship in the regional hospital. Expressions of a wish for euthanasia were more frequent in the academic hospitals (62% vs 38%), possibly triggered by the shock of a diagnosis, 25 which is more often delivered in those settings. Physicians appreciate the involvement of family and feel responsible for their well-being. The quantitative data confirms this. Family is present in almost all (96%) consultations and they are sometimes (31%) the ones to initiate the end-of-life discussions. In 67% of the consultations on euthanasia, the patient and family had already discussed euthanasia together beforehand.
Another explanation of the discrepancy between the qualitative data that shows the alleged importance of end-of-life conversations in dementia care and the quantitative data that shows the actual practice seems the prevailing division of medical tasks between hospital doctors (diagnosis) and general practitioners (care after diagnosis). The brevity of contact with patients in the hospital would hinder discussion of sensitive topics. However, in other research, general practitioners also mention these as inhibiting factors in talking about end-of-life care.9,12,26,27 In our study, the physicians described being confronted with the negative consequences of this limited discussion in emergency care: families an patients experience stress, powerlessness and sometimes anger. This observation reinforces the conclusions in other studies that end-of-life communication in high-pressure, acute settings is extremely challenging, due to for example, complex family dynamics and a reluctance to address end-of-life issues. 28 This results in lower patient and family satisfaction, fragmented information and limited understanding of the dying process among families. 29
Together, these studies point to the urgency for policymakers to move from awareness to action. Clearer agreements are needed about the division of tasks between hospital doctors and general practitioners. Obstacles such as lack of time or training should be taken away by, for example, developing a dedicated type of consultation for end-of-life topics, that is separate from the diagnostic consultation 6 and aligns with the doctor-patient relationship, or making end-of-life conversations a default topic in collegial consultations.
In the Netherlands, euthanasia is legal under strict conditions. It is an established, and for most people, accepted practice. Talking about the end of life with people with dementia implies talking about euthanasia.25,30 However, our interviews show this results in a delicate balancing act for physicians. They feel responsible for discussing of the end of life, but they avoid initiating conversations about euthanasia because this could be perceived as encouragement, which they find undesirable. All physicians in our study stated that euthanasia, in principle, should be accessible to people with dementia. However, euthanasia in hospitals is rare (2.2% in 2024), it mostly occurs at home. 31 This may explain why only 7 out of 27 respondents had performed euthanasia themselves. Moreover, most respondents indicated they were hesitant to perform euthanasia for people with dementia and reluctant to bring up euthanasia in cases of patients with dementia. This corresponds with other research that shows 40% of Dutch physicians would consider euthanasia for a patient with early-stage dementia, and 29%–33% would consider it for patients at an advanced stage.21,32 In our study, physicians observed a societal shift from euthanasia as a last resort to a reasonable option, sometimes leading to less attention to natural dying. Although refuted and still requiring further research, a common argument is that euthanasia legislation hinders the development of, and access to palliative care. 33 The legalization of euthanasia influences people’s views of a ‘good death’ and end-of-life care, as it introduces an option that requires consideration. Having this option may result in less reflection on the option of natural dying. More research is needed on these ethical implications, particularly for people with dementia.
Strengths and limitations
A strength of this study is its first-hand data from physicians about their consultations. However, this also implies that the physicians who agreed to participate may represent a select sample of those interested in end-of-life issues. Despite instructions to complete a survey for every dementia patient, time constraints or study prompts might have led some participants to only fill out surveys when end-of-life themes were discussed. This could mean that we overestimated the frequency of end-of-life discussion in consultations.
Research on sensitive issues in end-of-life care is often predominantly qualitative, with limited studies on the actual practice of initiating end-of-life conversations. Research on advance care planning or end-of-life communications in cases of dementia within hospital settings is particularly scarce. 28 Furthermore, studies specifically focused on the role of family in euthanasia situations involving people with dementia are sparse.17,34 Our research is therefore crucial for gaining a deeper understanding of how end-of-life care operates in practice with various discussion partners, ultimately aiming to improve this care.
Conclusion
End-of-life discussions with patients with dementia in hospitals are not standard practice, despite hospital doctors feeling responsible for these discussions and emphasizing the importance of these discussions. Regarding euthanasia, physicians have moral reservations about initiating this discussion with patients with dementia. They also express concerns about how the topic is addressed in society. The involvement of family sometimes brings specific challenges but is generally perceived and experienced as positive. Future research could focus on comparing the perspectives of hospitalists, patients and their families across countries with a view to identifying best practices.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163261416275 – Supplemental material for Bringing up the end of life and euthanasia. A mixed method study on consultations with people with dementia and their families in the hospital setting
Supplemental material, sj-docx-1-pmj-10.1177_02692163261416275 for Bringing up the end of life and euthanasia. A mixed method study on consultations with people with dementia and their families in the hospital setting by Trijntje M. Scheeres-Feitsma, Petruschka Schaafsma, Janneke van Kempen and Jenny T. van der Steen in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163261416275 – Supplemental material for Bringing up the end of life and euthanasia. A mixed method study on consultations with people with dementia and their families in the hospital setting
Supplemental material, sj-docx-2-pmj-10.1177_02692163261416275 for Bringing up the end of life and euthanasia. A mixed method study on consultations with people with dementia and their families in the hospital setting by Trijntje M. Scheeres-Feitsma, Petruschka Schaafsma, Janneke van Kempen and Jenny T. van der Steen in Palliative Medicine
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: European Research Council (ERC) Consolidator grant number 771483.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.