
Abstract
Background:
Homecare workers (paid workers without professional qualifications who provide care for people within their own homes) are crucial providers of end-of-life care (the last 6 months of life) but are not part of the healthcare multidisciplinary team. Little is known about the homecare worker role within interprofessional working practices.
Aim:
To explore the experiences of end-of-life homecare provision, from multiple perspectives.
Design:
A qualitative multiple case study using semi-structured interviews, and the option to create a Pictor chart – a visual diagram of relationships between those involved in care provision. Data were analysed using a reflexive thematic analysis. An adaptation of Bronfenbrenner’s ecological systems theory was used to inform the analysis.
Setting/participants:
Homecare workers and managers, people receiving care, carers, social, and healthcare practitioners from three economically and culturally diverse geographical regions within England.
Results:
133 participants were recruited (case 1 = 49, case 2 = 34, case 3 = 49). Although examples of good practice were seen, common barriers to collaboration between health and social care practitioners and homecare workers were identified: lack of healthcare practitioner knowledge/training on homecare workers’ role and its value, and poor communication (gatekeeping by managers, asynchronous working practices, restricted access to documentation and systems).
Conclusion:
The homecare worker role was poorly understood and undervalued with inadequate communication and interaction between practitioners, potentially impacting on quality of care. Collaborative practice is necessary for provision of high-quality care, but we found this was often absent due to knowledge, professional, and organisational barriers. Further research should explore suggested strategies to address the barriers identified.
Keywords
Homecare workers provide a crucial service to people receiving care at end-of-life and wishing to remain in their own homes
Collaborative working between social and healthcare services improves care provision.
Barriers to communication led to ineffective collaborative working, including lack of direct communication systems with gatekeeping by managers, asynchronous working practices, misperception of reactive one-sided communication, and restricted access to respective documentation.
Healthcare practitioners often had poor knowledge of and undervalued the homecare worker role, exacerbating poor communication and collaboration.
Examples of good practice and potential solutions to barriers to interprofessional working
Healthcare practitioners require training to better understand, recognise and appreciate the role of homecare workers
Communication barriers should be addressed to enable the homecare worker to contribute effectively to the multi-disciplinary team.
The homecare workforce’s role in providing high quality end-of-life care will remain constrained without wider professional and societal acknowledgement of its value.
Background
Domiciliary care is crucial for people to remain in their own homes, if preferred, for as long as possible. At the end-of-life (defined here as the last 6 months of life) multiple agencies from health, social care and other providers may be involved. Homecare workers are key care providers. This role has different titles internationally including nurse’s aide, personal care worker, personal assistant, domiciliary carer. Funding sources vary (private means/insurance, state-funded) but the work is similar. In this paper we use the most common UK term, homecare worker, defined as a paid carer with no professional qualification addressing day-to-day care needs in a person’s own home. End-of-life homecare research has often focussed on clinical roles rather than homecare workers’ contributions. 1 They are low-paid and low-skilled, 2 despite some countries requiring qualifications. 3
Multi-disciplinary teams are foundational for the effective delivery of holistic end-of-life care,4,5 with interprofessional working enabling open communication, respect, and joint decision-making. 6 Despite international differences in homecare service delivery models, 7 homecare workers would benefit from interprofessional working to deliver end-of life care. Globally, there is a call for integrated social and healthcare services to better meet changing societal needs equitably. 8 Within the UK, service integration characterises the government’s long-term health plan. 9 The homecare worker role has not always been included in this rhetoric surrounding the integration of social and healthcare, for example in multidisciplinary meetings.10–12
Research studies of multi-disciplinary teams often exclude homecare workers13–15 so we know little about their contribution to, or experience of, end-of-life homecare in the context of interprofessional working.
Aim
We aimed to explore the experiences of end-of-life homecare provision by homecare workers from multiple perspectives.
Methods
Design
We conducted a multiple case study exploring the experiences, training and support needs of homecare workers providing care for people approaching end-of-life. Case studies enable the context, complexity and relationships of an intervention to be described and explained in detail. 16
The study used qualitative interviews, a content analysis of social homecare policy documents, and engagement with homecare worker and client advisory groups and study partners. The qualitative interviews were with people within each case who had experience of receiving or delivering end-of-life homecare. The content analysis reviewed policy documents relating to the role, and training needs, of social homecare workers providing at end-of-life homecare. 17
Case definition and justification
Our study defines ‘case’ as a population within a specific geographical region selected based on ethnic and socio-economic diversity (see Table 1).
Description of cases.
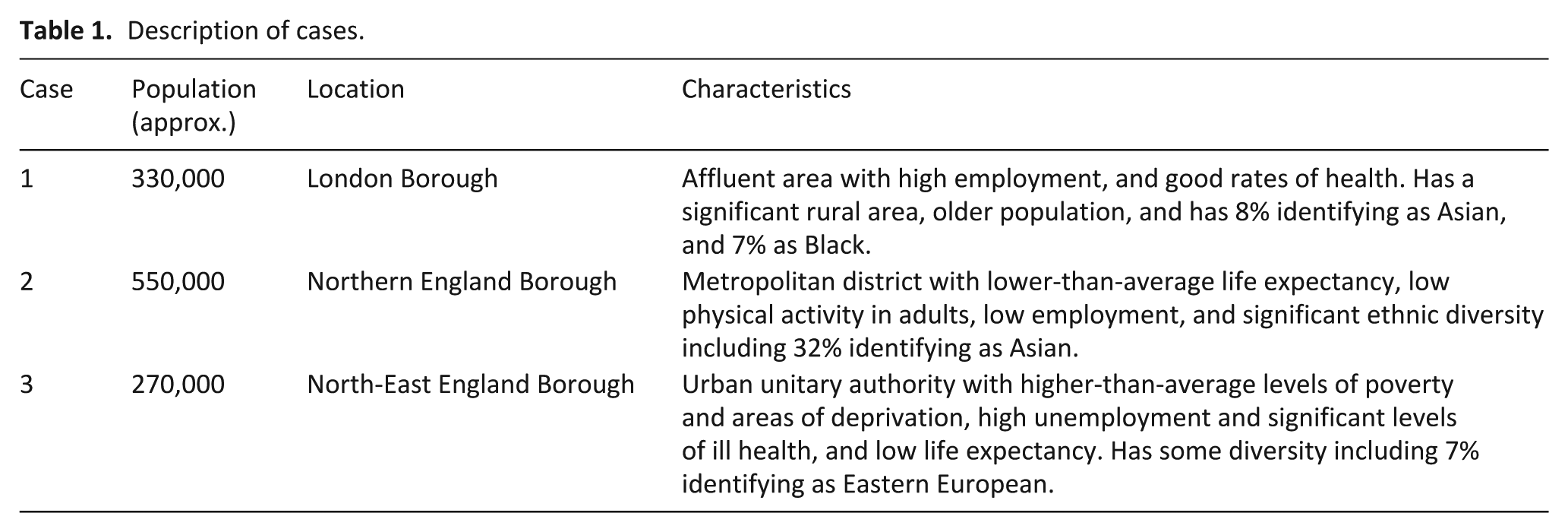
While single case studies may be beneficial beyond their own setting (15), we chose three cases to allow for more breadth, wider applicability, and generalisation. 18
Participants and sampling
Eligible participants were consenting adults (18+ years), able to communicate in English or through an interpreter, with recent (within 12 months) experience of either delivering or receiving end-of-life homecare (see Table 2).
Participants inclusion and exclusion criteria.
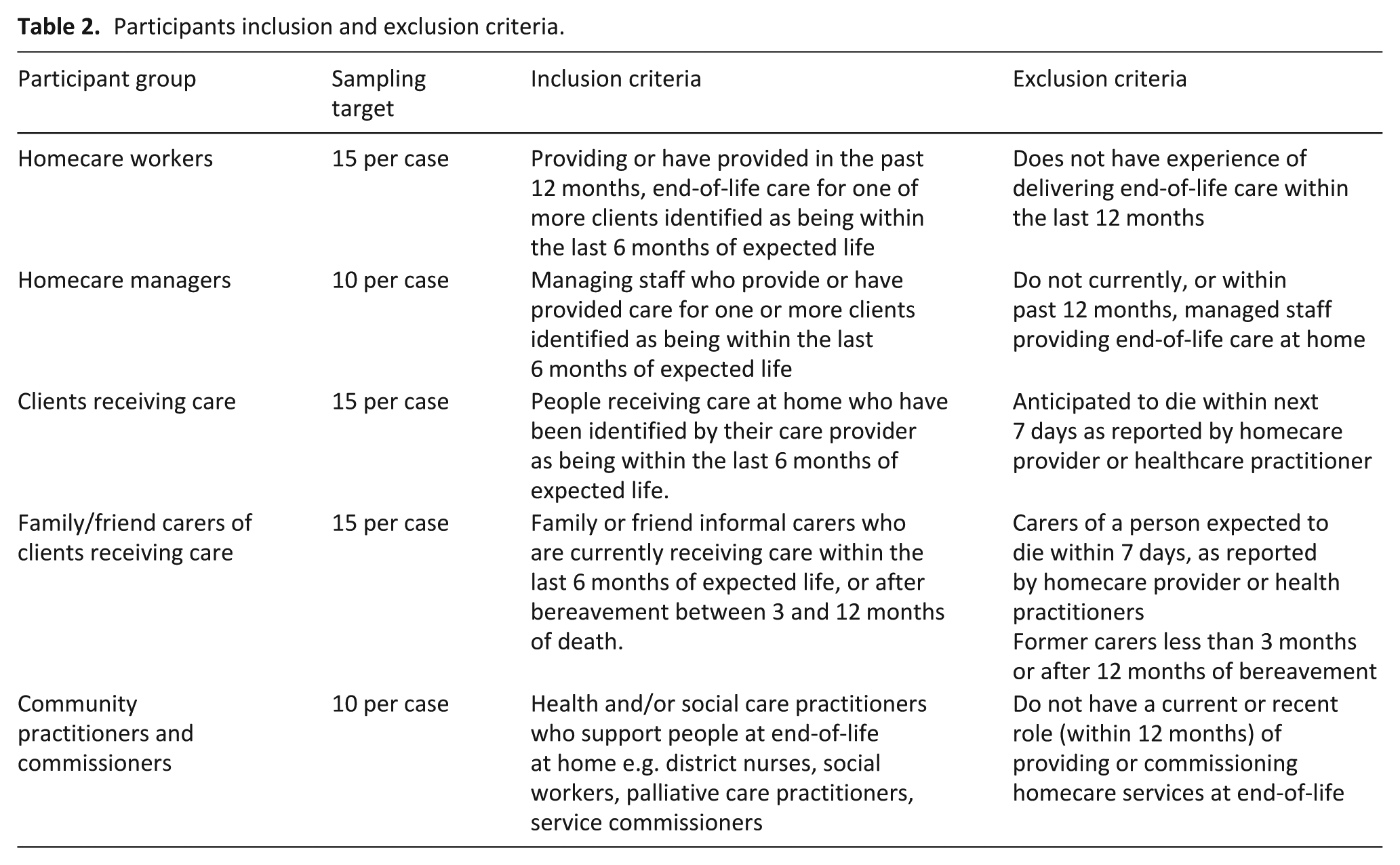
We purposively sampled participants based on participant category (homecare worker, homecare worker manager, social or healthcare practitioner, service commissioner, person receiving care, informal carer) and region, to maximise representation of different experiences of managing, delivering, and receiving care. Participants were provided with information sheets and the opportunity to ask questions prior to giving either written or verbal informed consent.
Our planned sample size was 50 participants per case, with the greatest proportion being homecare workers and homecare worker managers as the study’s primary focus. The sample size was guided by information power, sample diversity, and data quality. 16
Recruitment
In each case, homecare workers were recruited through homecare agency managers, and snowballing from homecare worker and manager participants. Clients and carers were identified by homecare agencies, homecare workers, and local hospices. Community practitioners were recruited through homecare agencies, social media and direct contact with healthcare practices such as GP surgeries and community health teams, networks, local hospices, and health trusts. Commissioners were identified through information in the public domain and local authority contacts within the research team.
Theoretical frameworks
Our design was informed by the three-stage Design of Case Study Research in Health Care (DESCARTE) case study model. 19 In the first stage we defined our cases, purpose, and situated our study within the current literature, through a study protocol. 20 The second stage comprised data collection and data management, and in the third stage we completed analysis, interpretation, and dissemination. The DESCARTE approach enabled within- and between-case comparison, supporting transferability. 21
We adopted Bronfenbrenner’s human ecological systems theory wherein the homecare worker was seen as the primary person within an ecological environment comprising different systems. 22 We used an adapted version 23 with levels in the environmental system differentiated based on their immediacy to the homecare worker, including time (chronosystem), those directly involved with care (microsystem), the interactions between those caregivers (mesosystem), the organisations relating to those caregivers (macrosystem), and the wider services involved such as government, the health service, and the third sector (exosystem).
Data generation
Interviews were conducted between May 2023 and May 2024 by experienced qualitative researchers, digitally recorded, transcribed verbatim, checked for accuracy by the interviewer, and anonymised. A semi-structured topic guide (Supplement 1), developed from the literature, research team, and service user and homecare worker advisory groups guided the interviews. The guide changed iteratively allowing unforeseen topics to be raised by participants and subsequently included. Participants were asked to describe their experiences of home-based care at end-of-life including a focus on training and support needs for homecare workers. Participants could opt to create a Pictor diagram during the interview process. Pictor is a graphic elicitation technique representing professional and social networks when working on a task. 24
For the document review, we sourced social policy documents from the public domain and through team expertise. A quantitative and qualitative analysis used a READ (readying, extracting, analysing, distilling) approach, 25 which is reported in more detail elsewhere. 17 Interviewees were also asked about any policy documents they used to guide their service provision.
Data analysis
Analysis followed a reflexive thematic approach, adopting the six phases outlined by Braun and Clarke. 26 This enabled a deeper engagement with the data alongside an appreciation of the different perceptions and understandings of the participants and the research team. Data were organised using NVivo14 software. The research team worked collectively using reflexive practice including note-taking and open discussions to help reduce bias. Researchers familiarised themselves with the data by re-reading transcripts and where required, listening to audio recordings. The team compared and collected codes inductively from the data which were further developed and examined to form themes. Sense checking was carried out with the wider research team including our service user, family carer, and homecare advisors.
We completed a matrix analysis to compare the similarities and differences between the three cases. Each theme and sub-theme were analysed by site, and summarised with sample quotations recorded, enabling analysis both within and across cases. Pictor diagrams were analysed separately to the interviews and findings synthesised narratively. No loco-regional policy documents were identified, and findings from national documents did not inform our findings and so are not included in the synthesis.
Ethics
This study was registered on the Research Registry (No.8613) and was approved by the Health Research Authority (HRA) West Midlands Research Ethics Committee on 31st March 2023 ref 23/WM/0030.
Results
We interviewed 133 participants online or face-face between May 2023 and May 2024 (Table 3). Interviews varied in length, with two outliers of 7 and 100 min. Forty-one Pictor diagrams were created. Most interviews were individual (n = 126), but five people receiving care expressed a preference for a family carer or homecare worker to form dyads. Identifier codes for illustrative quotations are: site number, type of participant (e.g. HOMECARE WORKER), and number of interview, for example 1-HOMECARE WORKER-4.
Summary of participant characteristics.
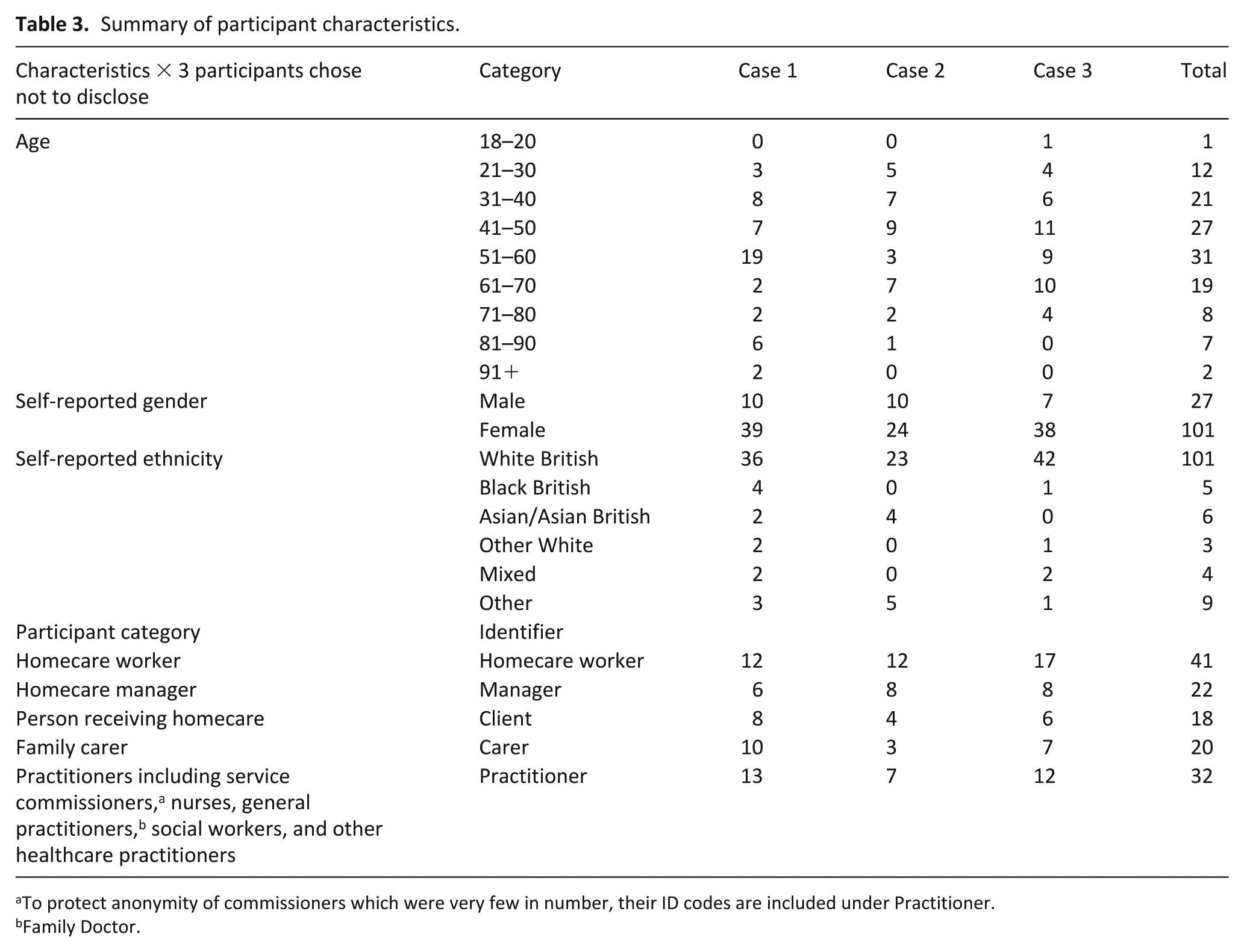
To protect anonymity of commissioners which were very few in number, their ID codes are included under Practitioner.
Family Doctor.
We found no between-case differences in the data, but significant within-case differences were apparent. We therefore present findings from the combined dataset. Consistent with the rich data generated from many interviews, five rich and complex themes were found (see Supplement B). This paper presents the theme of interprofessional working. Other themes are reported elsewhere (refs to preprints).
Interprofessional collaboration throughout the eco-system
This major theme of barriers to interprofessional collaboration was generated consistently across all three sites across the dataset. All environmental systems influenced this issue (Figure 1); including the value and worth of homecare workers (microsystem), the direct interaction and communication between practitioners and homecare workers (mesosystem), the impact of structures and systems within the NHS, local authority, and charitable/private sector (exosystem), the wider societal impact of the lack of understanding and valuing of the homecare worker role (macrosystem), and the changing needs and influences of time on homecare workers, people receiving care, carers, and practitioners, such as asynchronous visits (chronosystem).
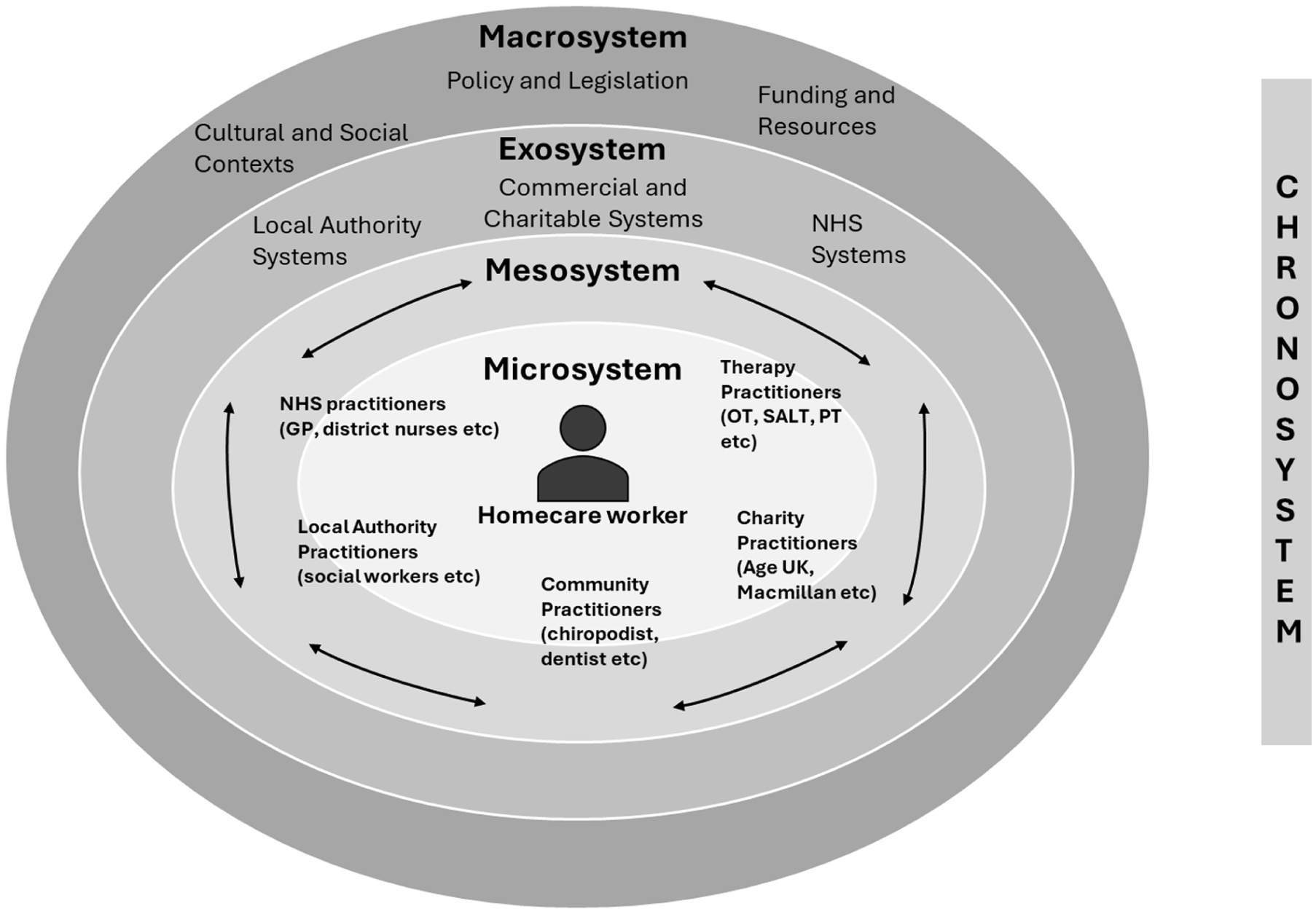
Ecosystem of Palliative Care Homecare Workers. The focus is inter-professional working with homecare worker at the centre of the microsystem. The interactions between clients and family carers and paid care providers was not found to have any influence on the (lack of) collaborative working practice.
We found two key sub-themes of interprofessional collaboration: (i) knowledge of the role of the homecare worker, and (ii) valuing the homecare worker. Although there were good examples of collaborative working, most data identified barriers to effective collaboration in all areas of the ecosystem (Figure 2).
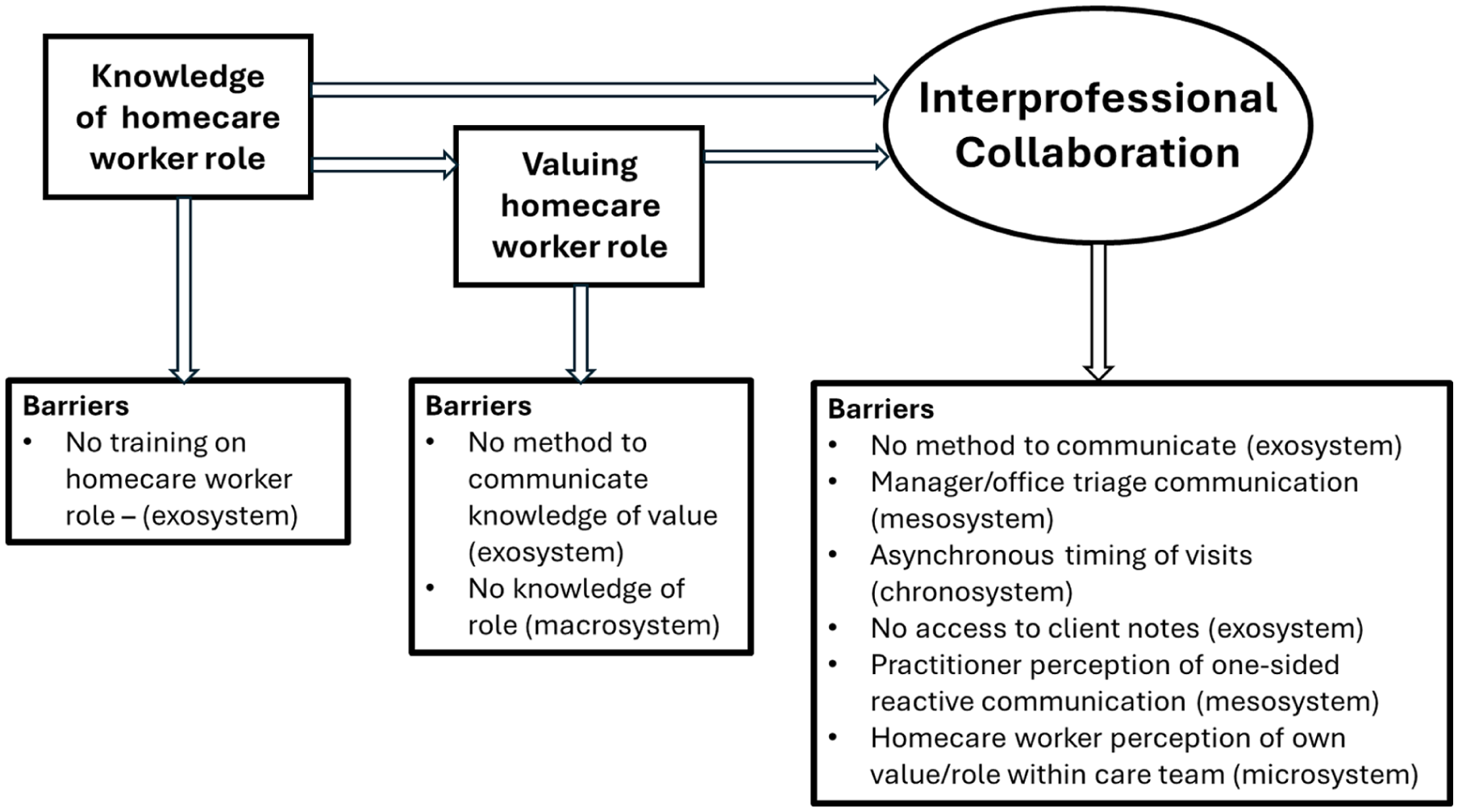
Enablers and barriers to interprofessional collaboration and connection to relevant ecosystem.
Knowledge of homecare worker role
Practitioner knowledge and understanding of the role of homecare workers varied. Some participants did not understand what homecare workers could and could not do, causing difficulties with interprofessional working. There was no understanding of how to develop this knowledge, or how it could improve care. Homecare workers and managers perceived practitioners as showing little recognition of the need to include homecare workers in interprofessional interactions, or the benefits of their role to people receiving care and the wider palliative care community.
If you need a plaster and stuff you’d have to ring (laughs) a district nurse. So they kinda like get annoyed that they have to come out for such little things, but I don’t think they understand the rules of the homecare, that we aren’t allowed. 3-HOMECARE WORKER -17 We are the ones that have the most contact, we are the ones that have that information, they don’t read our notes, they, they’re not interested in what we do, they’re not interested, yet if they were they would know and understand that person that’s lying in that bed much better than what they do. 1-MANAGER-2
(De) valuing the homecare worker role
There was an underlying need for respect and trust, and valuing of the homecare worker role; this empowered homecare workers to interact with practitioners as equals, and for practitioners to adopt a supportive, collaborative ethos. Homecare workers were appreciated by some practitioners, but there was uncertainty around how, or if, to share that view with homecare workers. Some practitioners provided third party expressions of devaluing and lack of respect for the role of homecare worker.
I would love to tell each individual care provider how valuable I find them, but I also am not sure that it’s just my responsibility to do that, or healthcare professionals’ responsibility to do that. 1-PRACTITIONER-4 It feels as though caring is a job that people go to when they can’t do any other job. 2-PRACTITIONER-3 They [other practitioners] don’t listen, they put their nose up a lot [to show rejection of something that’s unworthy] of the time to the carers, these nurses and that. 2-HOMECARE WORKER -3
This was perceived to impact practice, with practitioners and homecare workers working separately and without mutual support. The lack of understanding and appreciation of roles created and exacerbated interprofessional divides and poor communication.
We have had district nurse teams where the carer has been there and incontinence has happened but the district nurse will refuse to assist the carer to help the person because that’s not their job to do personal care, they’ll arrive and they change a dressing, but they’ve been incontinent they won’t change the dressing until we send another member of staff to assist with personal care. So, it creates a real divide. 3-MANAGER-2
Achieving effective collaboration between practitioners and homecare workers requires knowledge and valuing of the role.
Barriers to interprofessional collaboration
Direct communication with homecare workers was a key challenge. Many agencies managed all communication centrally through office staff or managers, rather than homecare workers talking directly to practitioners. This was justified as ‘protecting’ the homecare workers, and a practical solution to the limited time available for phone calls.
We’ve always said if they’ve got any concerns. . . or they think anything could be changed, then to speak to us and we’ll do the phone calls for them. 1-HOMECARE WORKER -9
This, and the lack of synchronous working can be frustrating for all care providers as it reduces direct communication, and opportunities for supporting homecare workers by providing valuable ad hoc learning. This situation also limited the valuable contribution homecare workers could make to clinical care and planning, given their daily contact.
I think if we could look at a way to try and (sighs) have more joint visits with carers there, and if we could maybe give carers some confidence in end- of- life care and to be able to speak to us and raise a few more things than they do; I think probably [we] maybe need something where we approach them as well, I think. 3-PRACTITIONER-3
Trying to arrange joint visits proved problematic due to different approaches to scheduling, highlighting the challenges seen in the chronosphere of care provision. Homecare workers often have no set visit times but instead have multiple clients within a work shift. Similarly, other healthcare practitioners such as district nurses and General Practitioners (family doctors) would visit as part of a scheduled round of calls, making it impractical to coordinate simultaneous visits.
They don’t have time to sit for the community nurse to get there. . . sometimes their care calls are only half an hour/twenty minutes. 3-PRACTITIONER-8
One homecare agency based within the third case illustrated highly effective interprofessional working relationship with practitioners, with regular communication, meetings, sharing expertise, resources, and support.
The system that we use is used by all the nurses, all the admins, all the care, you know, our staff, we all access the same details, and you’ve also got physios that have been and documented notes and then you’ve got information about equipment or profiling beds that have been put in, cos we’re provided with them. 3-HOMECARE WORKER -5
This was enabled by this particular agency operating within a statutory healthcare provider - an exception within our overall sample, and unique to that case. Most homecare worker participants were employed outside the health authority within private organisations, often subcontracted by local authorities. Access to, and communicating through, patient records was thus impossible. Both homecare workers and practitioners noted how difficult it was to access and share patient information: We’ve [healthcare practitioners] got a system where we can look behind the scenes and kind of see if a speech and language therapist has been in or an OT [occupational therapist]; we can have a little look behind the scenes to see their assessment, which is really helpful. . . For carers going in I suppose it’s a little bit more feeling in the dark because they’re not seeing that assessment, they’re just hearing it from the family, and sometimes families distort things to how they want it to be, or they forget things, or they can’t feed it back. So, the carers don’t quite get relayed the information that we can. 2-PRACTITIONER-1
When homecare workers were able to interact with other practitioners, there were significant benefits. Homecare workers commented on receiving support and training to help provide aspects of care, for example, how to move people safely, use equipment, or manage specific needs such as catheters: We would discuss with carers if they were there at the visit anything that maybe they weren’t doing or they needed extra support with, we would support the carers with that as well, like teaching and things like that, like how to use the slide sheet correctly, catheter care, anything else that basically they were unsure about. 3-PRACTITIONER-8
Practitioners often felt their relationships with homecare workers were reactive, with no consideration by practitioners of allocating time to interact or work collaboratively proactively. They perceived it was the homecare workers’ responsibility to initiate contact for specific needs or when requiring assistance from practitioners, perceiving them to be peripheral to healthcare provider teams.
We’ve already got lots of people to speak to on a daily basis and teams and services, so, you know unless there’s a need for it, we probably wouldn’t be going to reach out to the care teams, but we’re always there if ever they wanted to speak to us as well, you know, if they needed to. 1-PRACTITIONER-3 If I wanted to give them a heads up about something I could just phone their care manager who would then pass the message onto the carers 2-PRACTITIONER-9
A two-way flow of communication was needed for effective collaboration. Both homecare workers and practitioners experienced frustration at not being able to talk directly, and therefore potentially not receiving enough information.
When you ring the care company it’s not actually the carer you’re speaking to, you’re speaking to a manager. . . so it’s difficult to even speak to the actual person that raised the concerns, for example, and sometimes they might handover to somebody else, especially if they’re going off shift, sometimes they don’t, so even that person might be wondering why was this call made and I have no clue. 1-PRACTITIONER-5
Evidence of interprofessional collaboration challenges was also found in the Pictor diagrams (see Figure 3 for an illustrative example). While many different practitioners were recalled as being a part of the microsystem around the person receiving care, homecare worker interactions focussed on the client, their family, and the care agency. Even qualified social work professionals did not appear to have direct contact with homecare workers, highlighting their isolation from other social and healthcare practitioners.
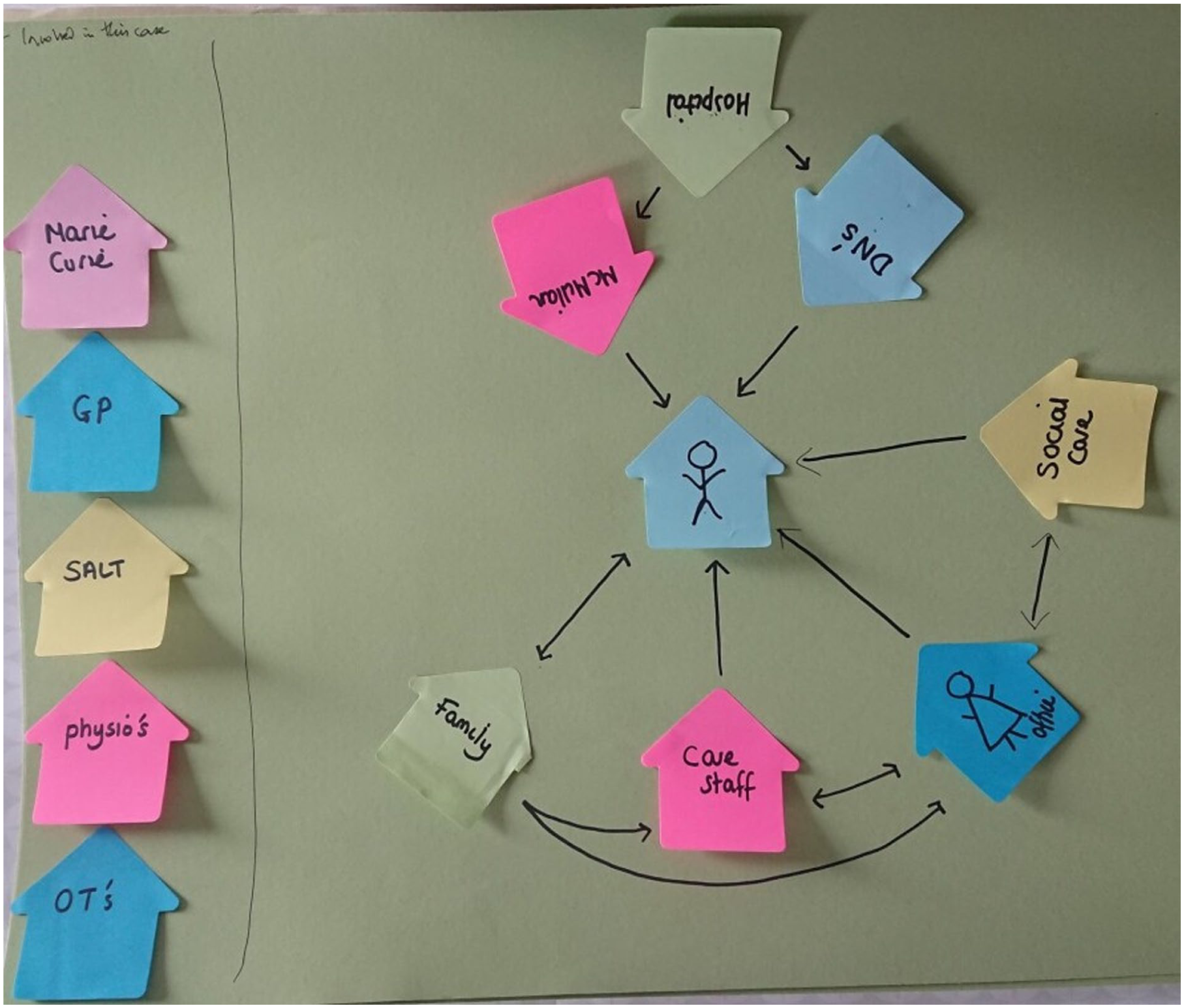
PICTOR 3-MAN-6. The ‘stick person’ at the centre, represents the person receiving care.
Discussion
Main findings
We found that effective interprofessional working was challenging, impacting all environmental system levels. Despite good practice examples, the homecare worker role within end-of-life care appears to be poorly understood and under-valued by other social and healthcare practitioners, and sometimes the homecare workers themselves. Inadequate collaboration caused feelings of isolation and eroded mutual trust. Barriers to effective interprofessional working included lack of training about the homecare role and its value, lack of effective communication systems, gatekeeping of communication by managers, asynchronous working practices, misperception of reactive one-sided communication, and restricted access to respective documentation. Situation of a homecare service within the statutory healthcare service provider enabled direct communication, access to joint documentation and effective integration where staff benefitted and care recipients benefitted, but was only found in one service. Interaction between homecare workers and other practitioners enhanced respect, mutual learning, and enabled homecare workers to contribute their knowledge of the person receiving care to other practitioners.
What this study adds to the literature
Our findings are consistent with literature showing ineffective homecare worker collaboration with other care providers.27,28 This exacerbates homecare workers’ own difficulties in recognising their value within end-of-life care. 29 Worldwide, collaborative practice improves quality of care, and care recipient experience30,31; thus seen as integral to palliative care. 4
We build on this literature by demonstrating that, despite pockets of good practice, the overwhelmingly dominant narrative is of homecare worker isolation, with scarce direct contact with social and healthcare practitioners. We describe a lack of knowledge of the homecare worker role and undervaluing (by practitioners and homecare workers). Social and healthcare practitioners need to understand the roles of all providing end-of-life homecare, and vice versa32–34 for effective interprofessional working. In our data, even when some practitioners stated they valued and respected homecare workers, they felt unable to express this due to workplace systems and organisational cultures. 31
We demonstrated little interaction between practitioners and homecare workers, due to the triaging of communication by homecare agency managers or office staff and a lack of supportive structures and systems. Reliance on one form of communication, for example, telephone, negatively affects working relationships, and poor communication has often been noted within palliative care. 35 We confirmed that other forms of communication (e.g. electronic clinical records) can be a barrier 36 ; particularly challenging for homecare workers outside health and social care structures. One connected communication system, as an exosystem change, could enable greater flow of information and communication within the extended multi-disciplinary team. 37 This would improve the chronosystem, as visits could focus on the current needs of the care recipient, which often change rapidly approaching death. The use of everyone’s expertise and experience is a key component to providing holistic palliative care. 29 We showed a reliance on reactive communication by practitioners. Interprofessional communication and collaboration fosters a sense of security for care recipients and family carers. 38 A communication block from homecare worker to healthcare practitioners leaves a clinically important gap.
There were barriers to interprofessional working within the chronosystem due to the asynchronous timing of practitioner visits. Homecare workers were not aware of, or able to be present when other practitioners provided care and vice versa. Where this did occur, it enabled reciprocal communication and collaborative working, including training opportunities. The lack of integration of resources such as time has been noted within palliative care 31 and can be an issue at institutional and structural levels within the exosystem due to working practices, impacting on mesosystem interactions between practitioners.
The World Health Organisation identified education as a crucial component of palliative care provision. 39 The need for education impacts on the meso-, macro-, and exo-systems in relation to accessing appropriate training within the workforce. Within society there is a need for wider recognition of the importance and value of the role of the homecare worker, and their inclusion within key documentation and policy where they have been overlooked in the context of end-of-life care. 17
Strengths and limitations
We had good representation across all participant categories, within three diverse regions in England, with rich data providing sufficient information power to address our research questions despite not reaching our indicative sample size. We used our public contributors to sense check the findings. Although only a third of participants created a Pictor diagram, these complemented interview findings.
There is potential selection bias in this study. Agencies and workers who may not be aware of the importance of homecare at end-of-life, or who may have been suspicious of poor practice being highlighted, may not have participated, and the use of snowballing techniques can impact on diversity and representativeness.
We acknowledge the structure of community-based end-of-life care varies across England and other countries, limiting the relevance of our findings to other areas with more health and social care integration. However, we offer robust insight into homecare provision, an under-researched and timely topic given the current crisis in in this field globally.40,41
Recommendations for practice and policy
We raise important challenges for commissioners and providers of end-of-life homecare services. There is a need for practitioner education around the homecare worker role and their value in community-based care. We also suggest consideration of wider institutional and organisational changes including timing of visits, sharing of records, and direct two-way communication streams. This would require transformation across all systems and organisations providing care31,37 to empower homecare workers as an integral part of end-of-life care provision. 39 This will need cultural change to enable collaboration and interprofessional working. 36
We found only one example of effective interprofessional working across all three cases. This was enabled by the care provider being sited within the local health organisation, allowing shared communication systems, joint training, synchronised visits to people receiving care, and staff physically working in the same building aiding relationships and rapport between disciplines, and supporting a collaborative culture . We argue a whole ecosystem change is needed, incorporating different systems and levels of care within the health sector, social care, community support, and wider societal networks, 36 for example, inclusion of home care workers in multi-discplinary team meetings
Our findings could be applicable to all home-based care; many barriers identified are not unique to end-of-life, or to England. Issues around interprofessional collaboration may have broader implications for community-based care within people’s homes. Finally, a wider societal acknowledgement, including policy, of the value of homecare workers is long overdue 34 ; the significance of their contribution should not be underestimated.
Conclusion
Effective collaborative social and healthcare practice is necessary for high quality care is hampered by inadequate communication systems and poor understanding and undervaluing by social and healthcare practitioners. Mutual education of roles, and facilitation of direct contact between homecare workers and other practitioners helps address shortfalls. However, definitive improvement will need far-reaching organisational, political and societal changes to overcome serious barriers resulting from different working structures. Further research should explore strategies to address the barriers identified.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163251383385 – Supplemental material for Addressing barriers to interprofessional working with homecare workers in community palliative care: Insights from a multi-site qualitative case study
Supplemental material, sj-docx-1-pmj-10.1177_02692163251383385 for Addressing barriers to interprofessional working with homecare workers in community palliative care: Insights from a multi-site qualitative case study by Zana Bayley, Cat Forward, Caroline White, Helene Elliott-Button, Justine Krygier, Liz Walker, Mark Pearson, Jamilla Hussain, Paul Taylor, Jane Wray, Helen Roberts, Alison Bravington and Miriam J Johnson in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163251383385 – Supplemental material for Addressing barriers to interprofessional working with homecare workers in community palliative care: Insights from a multi-site qualitative case study
Supplemental material, sj-docx-2-pmj-10.1177_02692163251383385 for Addressing barriers to interprofessional working with homecare workers in community palliative care: Insights from a multi-site qualitative case study by Zana Bayley, Cat Forward, Caroline White, Helene Elliott-Button, Justine Krygier, Liz Walker, Mark Pearson, Jamilla Hussain, Paul Taylor, Jane Wray, Helen Roberts, Alison Bravington and Miriam J Johnson in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank the participants of the study who generously shared their time and expertise with the research team. We would also like to thank the wider research team including Jill Manthorpe for supporting the study design, conceptualisation and acquisition of financial support for the project, Kathryn Harvey of Hull York Medical School, Joan Bothma of Cera Care, and the people with lived experience who contributed to the research.
ORCID iDs
Author contributions
ZB drafted article. All authors read, commented on, and approved the final manuscript. Conceptual design of study MJJ, LW, AB, PT, MP, JW and CW. Data collection and analysis ZB, CF, JK, HE-B, AB, CW, LW, MJJ.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study/project was funded by the NIHR HSDR Programme (project reference NIHR135128). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data is not available publicly due to the sensitive nature of content.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.