
Abstract
Background:
The Integrated Palliative Care Outcome Scale for Dementia (IPOS-Dem) was developed to assess symptoms and concerns comprehensively for people with dementia. There is a high demand for comprehensive assessment of people with dementia in China.
Aim:
To translate and culturally adapt the IPOS-Dem into Chinese.
Design:
Conceptual equivalence, forward and backward translations, and expert review were performed to develop a prototype Chinese version. Two rounds of cognitive interviews were conducted to ensure the items and scoring format were clearly expressed in the Chinese version.
Setting/participants:
Professionals, including a physician, a nurse, a linguistic researcher and a humanities researcher, were involved in the prototype Chinese version development. A purposive sample of 12 health care professionals working in three Chinese nursing homes participated in the cognitive interviewing.
Results:
The Chinese version was perceived as clinically useful. Challenges arose regarding comprehension of some items due to difficulties in translating the precise meanings. These included ‘Drowsiness (sleepiness)’, ‘Difficulty communicating’ and ‘Do you think s/he felt at peace?’. Considering how a symptom affects an individual presented was also challenging for respondents, as they needed to judge whether the symptom was present and/or causing distress. Selecting the appropriate term to name the measure elucidated the current understanding of dementia and palliative care in China, both of which remain poorly understood.
Conclusion:
This study highlighted the importance of cultural adaptation in conveying meanings across cultures. Most items were translatable and conceptually equivalent. The term ‘at peace’ and the concept of ‘being affected’ generated the most challenges in comprehension and judgement.
Keywords
People with dementia may experience a high symptom burden due to dementia and multiple co-morbidities.
The Integrated Palliative Care Outcome Scale for Dementia (IPOS-Dem) is a person-centred outcome measure to support comprehensive assessment of symptoms and concerns experienced by people with dementia.
Taking cultural and local contexts into account is essential when incorporating person-centred outcomes across different settings.
We introduce a cultural adaptation of the IPOS-Dem, integrating nuances related to the Chinese language and cultural traits.
This paper underscores the significance of cultural adaptation in elucidating, reformulating, and effectively conveying meanings and concepts across diverse cultures.
The study identifies challenges linked with person-centred outcome measurement for people with dementia in China.
Consistent refinement, ongoing education and essential training are vital for improving the use of IPOS-Dem.
The Chinese IPOS-Dem is ready for further psychometric testing to enhance its validity, reliability, feasibility and acceptability for clinical use in nursing home settings.
Integrating IPOS-Dem into dementia care settings could support person-centred and holistic care, which will require a shared understanding of terms, concepts and philosophies of care among involved parties.
Background
Dementia is a syndrome, usually chronic and progressive, that results in the deterioration of cognitive function (i.e. the ability to process thought) beyond what would be expected from the usual consequences of biological ageing.1,2 Globally, it is estimated that more than 55 million people have dementia, over 60% of whom live in low- and middle-income countries. In China, it is estimated that 15.07 million adults aged 60 years or older live with dementia, accounting for a quarter of people with dementia worldwide. 3
People with dementia may experience a high symptom burden due to dementia and multiple chronic long-term conditions, resulting in a negative impact on quality of life.4,5 However, people with dementia tend to die in residential care, in acute hospitals or at home with limited access to palliative care.6,7 Early identification of palliative care needs and concerns through systematic comprehensive assessment has the potential to benefit individuals. Nonetheless, since people with dementia who are verbally compromised may be unable to express whether they are feeling a symptom, it is challenging to identify symptoms and concerns comprehensively in people with dementia, 4 leading to distress. To fill this gap, the Integrated Palliative Care Outcome Scale for Dementia (IPOS-Dem) was developed as a person-centred outcome measure.
IPOS-Dem is derived from the Palliative care Outcome Scale (POS) and Integrated Palliative care Outcome Scale (IPOS).8,9 IPOS-Dem is a proxy-reported outcome measure allowing comprehensive assessment of symptoms and concerns experienced by people with dementia. 10 It is a brief questionnaire, which is designed to be used by staff who provide direct care in care homes. The extent of common symptoms and problems to which people with dementia are affected is assessed and scored. 10 IPOS-Dem has been demonstrated to be a feasible and acceptable tool for implementation in routine care in the residential care homes in the United Kingdom. 4 It has been adapted to Swedish, 11 German 5 and Swiss German. 12 Different versions are freely available at https://pos-pal.org/.
There is a lack of a comprehensive person-centred outcome measure for people with dementia in China. Therefore, the aim of this study is to translate and culturally adapt IPOS-Dem into Chinese and to develop a Chinese version of the questionnaire as a foundation for psychometric testing.
Methods
The translation and cognitive interviewing were conducted according to the best practice guidance of the Palliative care Outcome Scale (POS) family of measures for translation and cross-cultural adaptation. 13 Figure 1 gives an overview of the different phases, which were conducted from June 2023 to May 2024.
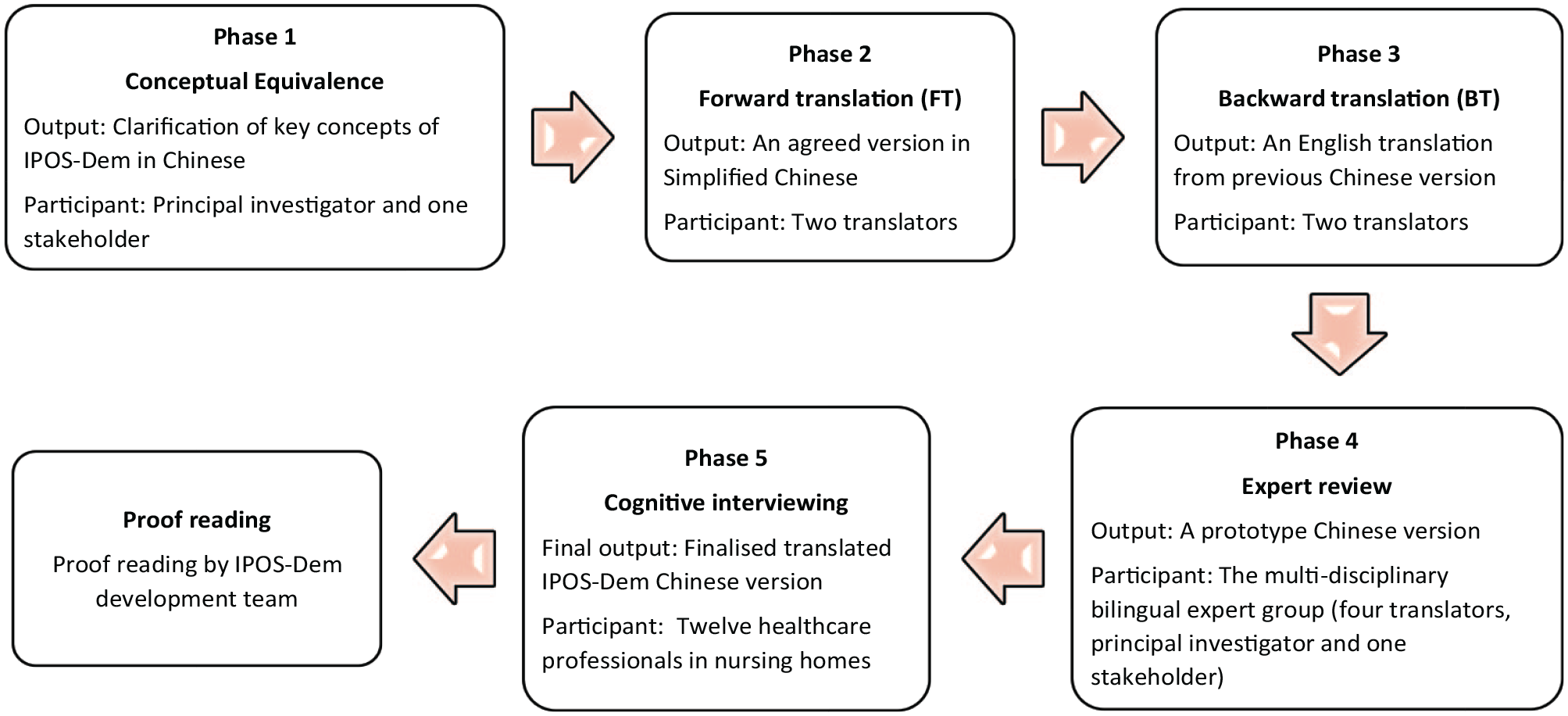
The process of translation and cross-cultural adaption (adapted from POS Family of Measures Manual for Translation, Cross-Cultural Adaptation and Psychometric Testing 13 ).
Phase 1: Conceptual equivalence
Conceptual equivalence ensures that ideas have the same meaning across different cultures or languages. An item-by-item review was conducted by LC and one healthcare professional working in a Chinese nursing home to identify (1) the fundamental concepts for understanding the scope and objectives of IPOS-Dem or (2) items that may be subject to varying interpretations. Then, informal discussions with three healthcare professionals with expertise in caring for older people were used to explore the potential Chinese equivalent definitions for those concepts and items.
Phase 2: Forward translation
Two bilingual translators independently completed two forward translations from English to Simplified Chinese. These two translations (FT1, FT2) were further scrutinised by a research team member and any discrepancies were discussed with the two translators to form forward translation three (FT3: an agreed version in Simplified Chinese).
Phase 3: Backward translation
Two backward translations (BT1, BT2) were completed by two independent bilingual translators blinded to the original English version.
Phase 4: Expert review
The multi-disciplinary bilingual expert group included a member from the research team, one health care professional familiar with IPOS-Dem and all four translators. The group synthesised and consolidated the backward translations into backward translation three (BT3: an English translation from the previous Chinese version). The expert group compared, evaluated, revised and consolidated items and response format between BT3 and initial IPOS-Dem items, which aimed to develop the prototype Chinese version ready for cognitive interviewing.
Phase 5: Cognitive interviewing
Setting and participants
Participants were purposefully sampled from three nursing homes in South and East China. Participants who (1) provided direct care to people with dementia, (2) were aged 18 years or older, and provided informed consent were recruited in this study. The cognitive interviews were conducted as an iterative procedure. The sample size was determined based on information power 14 and the guidance provided by the POS development team. 13 An initial round of 5–10 individual interviews was conducted. 15 These were analysed and informed revisions. A second round of 5–10 interviews was then conducted to test the revised IPOS-Dem. 15
Data collection
The cognitive interviews were conducted via one-on-one interviews (virtually or in person). Participants were asked to think about a particular person with dementia with whom they are familiar and to whom they provide direct care. Any identifiable details of the person with dementia were not shared with the interviewer. All interviews were video/audio-recorded.
A topic guide informed by Tourangeau’s model of the survey response process was used to conduct the cognitive interviews. This model presents four cognitive steps involved in responding to surveys (comprehension, retrieval, judgement and response) and possible cognitive errors. 16 Participants were asked about their thoughts on what was meant by each item and their response. Both the meaning of the items and responses were to be explored. The techniques ‘think aloud’ and verbal probing 17 were used in the interview. In the ‘think aloud’ procedure, participants were asked to share their thinking as they were answering the questions. Concurrent verbal probing was used to elicit further information regarding the question interpretation and clarity.
Data analysis
The recordings were analysed using directed content analysis. 18 A matrix developed from Tourangeau’s model 16 in Microsoft Excel served to analyse individual interviews and then synthesise the results across all participants. Verbatim quotes were preserved throughout the analysis and synthesis and used to demonstrate the findings.
Stakeholder consultation
A stakeholder group in China, comprising a person with dementia, two family members, a geriatric nurse, and a researcher, was actively engaged throughout the study. We consulted the group as a whole or individual members at different phases, which helped refine and modify items.
Results
Phase 1: Conceptual equivalence
Most terms within the IPOS-Dem are translatable. The terms ‘palliative care’ and ‘outcome measure’, as the fundamental concepts for understanding the scope of IPOS-Dem, offer several translation options. Three items had slightly different conceptual meanings based on different translations, including ‘Sore or dry mouth’, ‘Do you think s/he felt at peace?’ and ‘Has s/he been able to interact positively with others (e.g. staff, family, residents)’. The Chinese conceptual exploration of those concepts and items is listed in the Supplemental 1 Table S1.
Phase 2: Forward translation
Two bilingual translators, a clinical physician and a linguist, independently completed two forward translations (FT1, FT2). There were grammatical and content differences in the two forward translations, regarding question phrasing, item terms and the Likert response categories.
There were some grammar and syntax differences in questions with regard to the length of sentence and request phrasing. The two forward translators suggested different wordings to explain three items: ‘Sore or dry mouth’, ‘Drowsiness (sleepiness)’ and ‘Wandering (as a result of distress or putting person at risk)’. And the two translators suggested different terms for the response endpoints ‘Not at all’ and ‘overwhelmingly’.
After discussion with the translators, these differences were resolved and agreed upon in FT3 (Supplemental 1 Table S2).
Phase 3: Backward translation
Two bilingual translators, a clinical nurse and a humanities researcher, independently completed two backward translations (BT1, BT2). Both backward translations did not reveal significant discrepancies when compared to each other. There were five differences in the backward translation, including three items (‘Weakness or lack of energy’, ‘Drowsiness (sleepiness)’ and ‘Difficulty Communicating’) and two response categories (‘Overwhelmingly’ and ‘Cannot assess’).
Phase 4: Expert review
There were seven main differences between the consensus version of backward translation (BT3) and initial English-language IPOS-Dem items. Main differences were identified among the five previously observed differences in the backward translations, along with an additional two items (‘Lost interest in things s/he would normally enjoy?’ and ‘Do you think s/he felt at peace?’). Supplemental 1 Table S3 presented the main results of backward translation and expert review. The prototype Chinese version was developed based on the discussion of the group with suggested wording revisions.
Phase 5: Cognitive interviewing
Participants
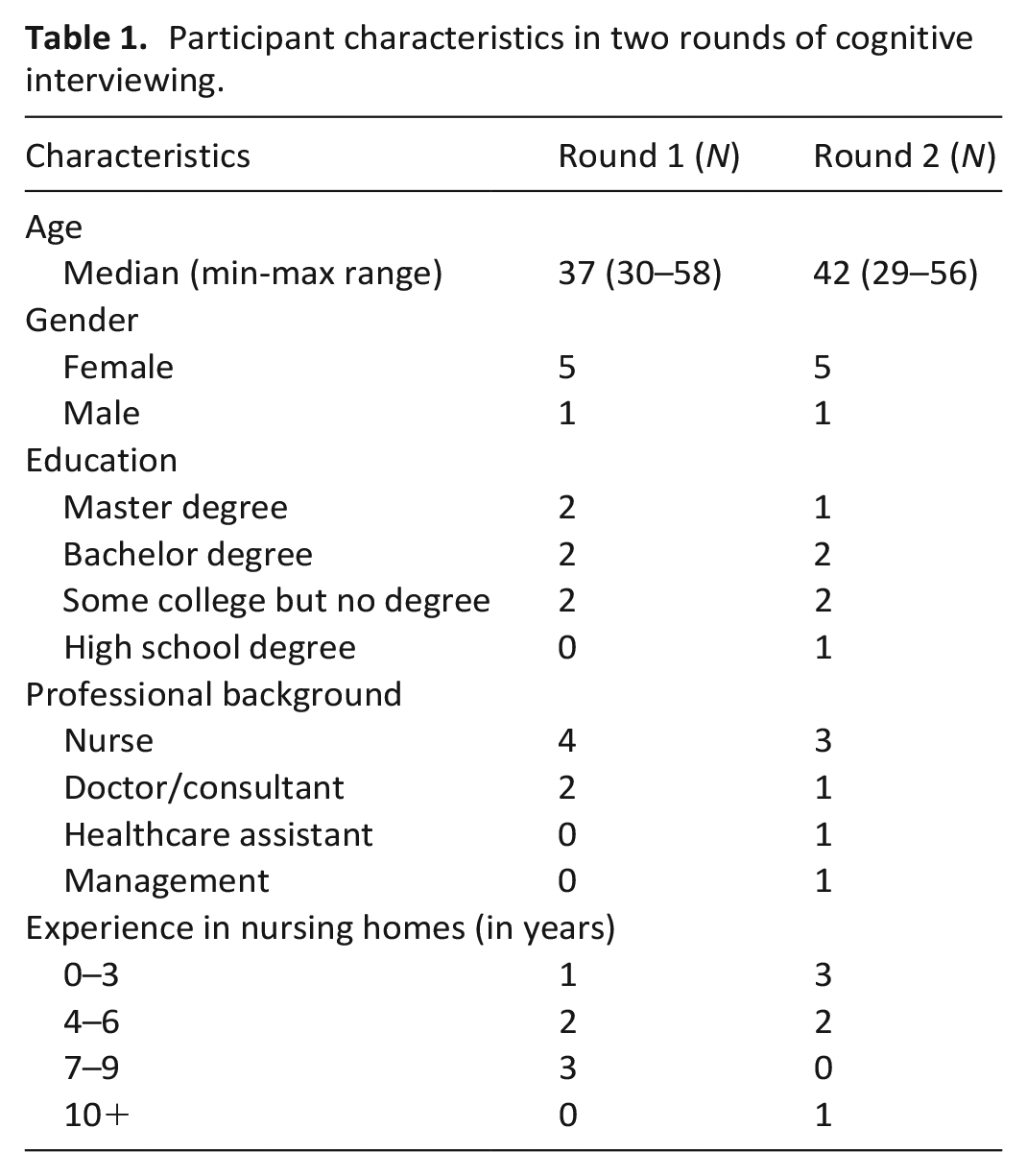
Twelve participants from three Chinese nursing homes participated in two rounds of cognitive interviews, with six in each round. The nursing homes were located in urban areas across different regions of China, including Shanghai, Zhejiang and Fujian. Table 1 lists the demographic characteristics of participants in two rounds of cognitive interviews.
Participant characteristics in two rounds of cognitive interviewing.
Item revision
Two rounds of interviews showed that most items and answer options worked well for the majority of participants. Reported difficulties were focused mainly on comprehension and a few concerned judgement and response. No problems were reported with retrieval. The challenges identified in the prototype version were resolved in the two rounds of cognitive interviewing.
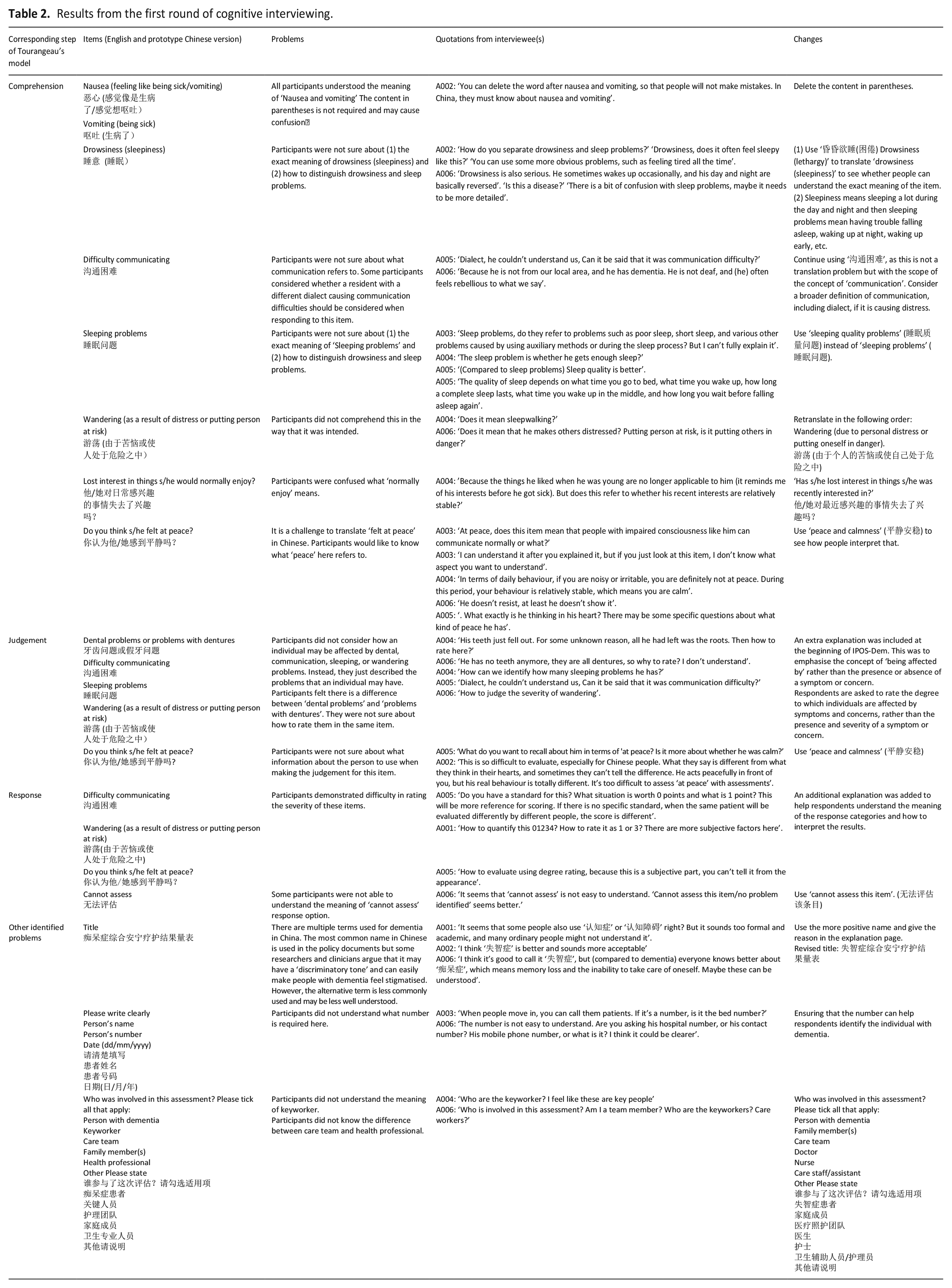
The first round: The results of the first round of cognitive interviewing are presented under comprehension, retrieval, judgement and other concerns (Table 2). Difficulties were identified for comprehension (n = 8 items), judgement (n = 5 items), response (n = 4 items). Three other concerns were identified. Following discussions with the research team (CES, KES, AB), revisions were made ready for the second round of cognitive interviews (Table 2).
Results from the first round of cognitive interviewing.
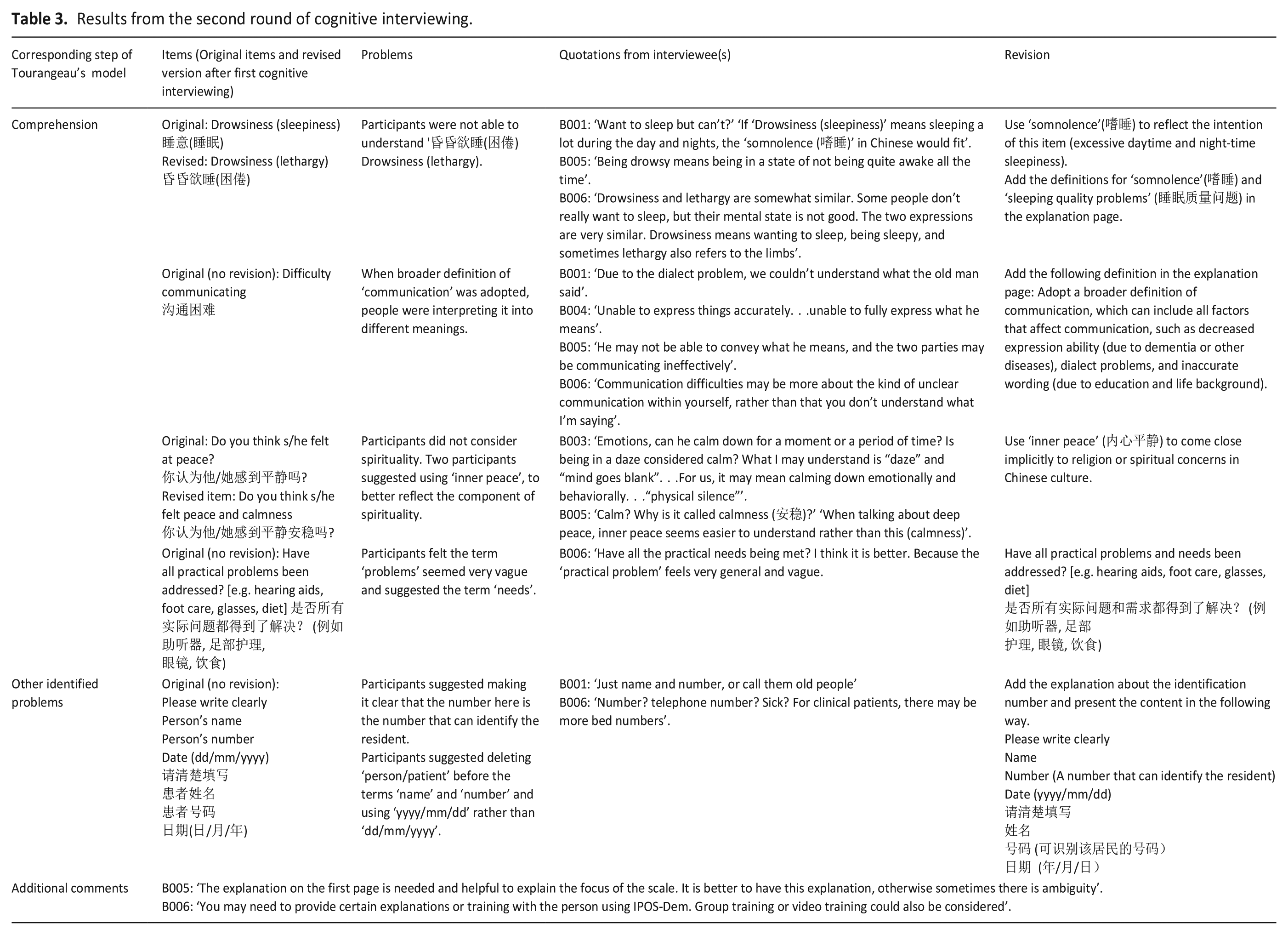
The second round: Most revisions made based on the results of the first round resolved identified problems. Four items were identified with comprehension difficulties. Additionally, one other difficulty was noted. Subsequent to discussions with the research team (CES, KES, AB), revisions were made. Table 3 provides a detailed overview of the interview results and the subsequent modifications made based on them.
Results from the second round of cognitive interviewing.
Stakeholder consultation and final version
After the cognitive interviewing (phase 5) was completed, the National Health Commission of the People’s Republic of China released the naming regulation for commonly used clinical medical terms, in which the standard naming of ‘palliative care’ was reidentified. The whole stakeholder group was consulted about the choice of language and final version. The research team decided to adopt the new terminology in line with regulations and some wording changes. The final IPOS-Dem Chinese version was approved by POS development team. Table 4 shows the comparison between the English-language IPOS-Dem and the final culturally adapted Chinese IPOS-Dem version. The Chinese version is freely available at https://pos-pal.org/.
Original English and final culturally adapted Chinese versions of IPOS-Dem – all items.
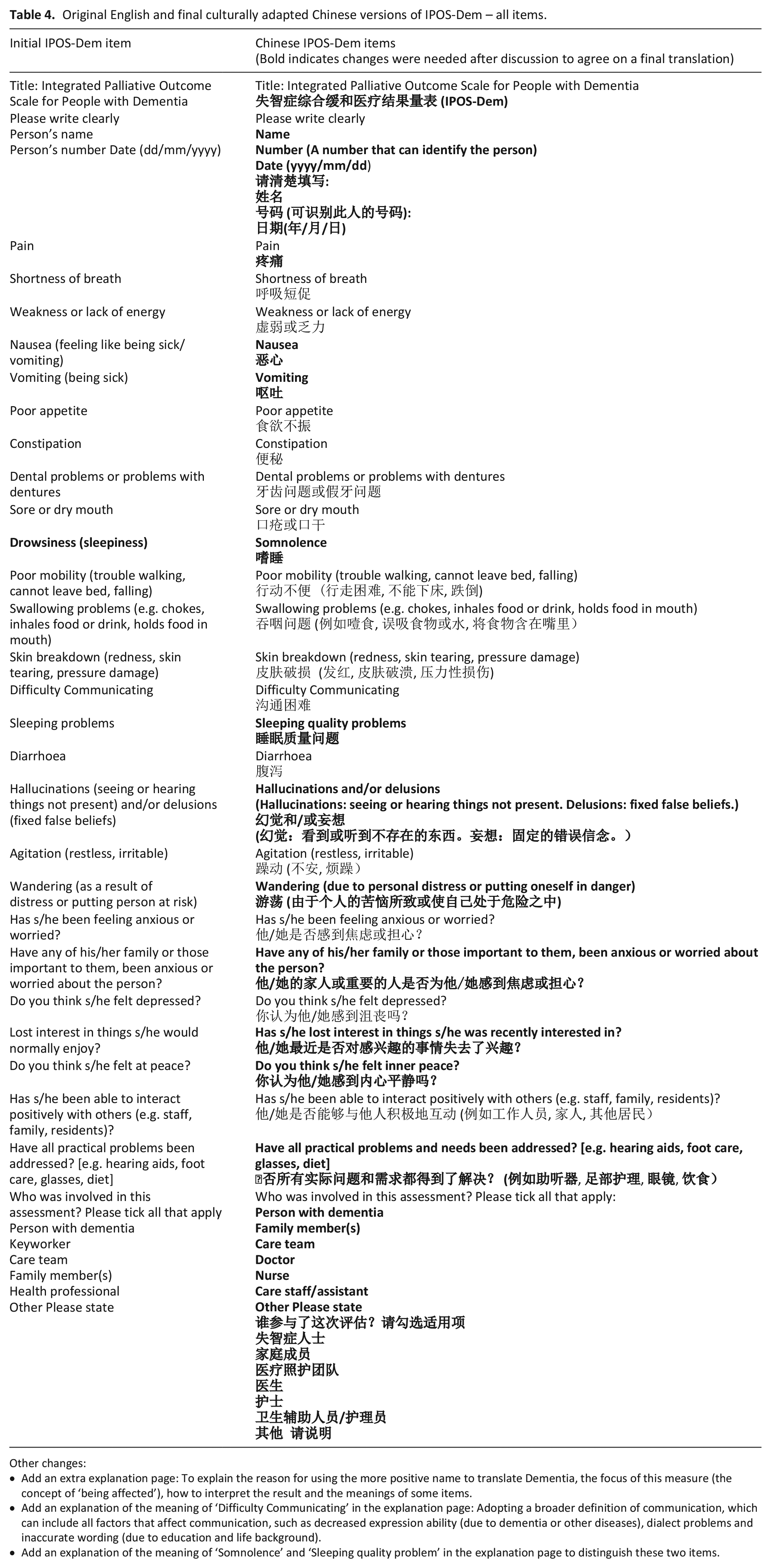
Other changes:
• Add an extra explanation page: To explain the reason for using the more positive name to translate Dementia, the focus of this measure (the concept of ‘being affected’), how to interpret the result and the meanings of some items.
• Add an explanation of the meaning of ‘Difficulty Communicating’ in the explanation page: Adopting a broader definition of communication, which can include all factors that affect communication, such as decreased expression ability (due to dementia or other diseases), dialect problems and inaccurate wording (due to education and life background).
• Add an explanation of the meaning of ‘Somnolence’ and ‘Sleeping quality problem’ in the explanation page to distinguish these two items.
Discussion
Summary
This study describes the translation and cultural adaptation of IPOS-Dem into Chinese, marking the first holistic outcome measure for people with dementia in China. Rigorous translation and cultural adaptation process could enable the IPOS-Dem Chinese version to be equivalent to the original. While most items were conceptually aligned, certain items posed challenges in comprehension and judgement. Additionally, careful consideration was required in naming the measure in Chinese.
Comprehension challenges
Several distinct differences in comprehension were found in items ‘Do you think s/he felt at peace?’ and ‘Difficulty communicating’.
The term ‘at peace’ generated most of the controversy in the cognitive interviews. The term was debated for its meaning, which was similar to other IPOS translation groups.19 –21 People often associated calmness in emotion and behaviour with the term ‘peace’, missing the spiritual aspect of peace. However, in the Chinese context, it was necessary to exercise discretion when addressing spiritual matters. Therefore, based on the insights gathered from participants, we used ‘inner peace (内心平静)’ to come close implicitly to religion or spiritual concerns in Chinese culture.22,23
The item ‘Difficulty communicating’ was unequivocal in the translation process. However, during cognitive interviewing, individuals interpreted it diversely, setting it apart from other IPOS-Dem translation groups.5,11,24,25 Since any cause of communication problems may lead to distress, a broader definition of communication was adopted in the Chinese version to reflect the holistic nature of IPOS-Dem, which can include all factors that affect communication, such as decreased expression ability (due to dementia or other diseases), dialect problems and inaccurate wording (due to education and life background).
Judgement challenges
Judgement challenges surfaced predominantly in how to comprehend and apply the concept of ‘being affected’ when answering the items. The presence and severity of the symptoms and concerns were first considered, while the subjective burden experienced tended to be overlooked when participants made judgements. It implies that person-centredness, the cornerstone of palliative care, is not yet well-grounded, similar to findings of other translation groups in other cultural contexts.5,19 An additional concern arose regarding how proxy reporting reflects person-centeredness, specifically in gauging whether proxy reporters accurately convey individuals’ perspectives on their health. This aspect could be further explored through psychometric testing, including inter-rater reliability testing. Drawing from the experiences of another IPOS translation groups, both patient self-report and staff proxy-report versions of IPOS have been approved to be valid and reliable. 9 Nonetheless, the agreement between patient and proxy reports varies across different contexts.9,26,27
We found that training and education could be pivotal in overcoming the judgement challenges that became apparent from cognitive interviews, in line with the findings of German IPOS-Dem translation group. 5 Acquiring a solid understanding of palliative care, person-centred care and outcome measures would shape users’ perspectives on the measures themselves. Moreover, a shared understanding of the purpose and significance of the measure, along with practical training on how to use, report and interpret IPOS-Dem would support the successful application of IPOS-Dem in the clinical setting and help reduce subjectivity.5,28 –30
Measure naming
Palliative care is a core term in the name of the measure. China has previously used ‘安宁疗护’ as an inclusive term to collectively describe hospice care, terminal care, palliative care and other terms related to palliative care.31,32 However, in March 2024, the National Health Commission of the People’s Republic of China released the naming regulation for commonly used clinical medical terms, 33 in which ‘安宁疗护’ is used to describe ‘hospice care’ and ‘缓和医疗’ is used to describe palliative care. As such, we consulted with five stakeholders and IPOS-Dem development team. Given that the importance of adhering to policy guidance and the long-term timeliness of future use, we decided to use the redefined term ‘缓和医疗’ as the name for the measure.
Translating the term ‘outcome’ presents a significant challenge. Currently, most Chinese literature uses ‘结局’ as the translation.34 –36 However, in English ‘outcome’ refers to a ‘change in current or future health status attributable to a preceding healthcare intervention’. 37 The term ‘结局’ does not fully capture the concept of ‘change’ inherent in ‘outcome’, as it typically denotes the final or last stage in a story’s plot or situation. 38 Thus, we have chosen to use ‘结果’ as the translation, which better conveys both the notion of a phenomenon arising from other phenomena and the final state of development and change at a certain stage. 39
Another critical term in naming the measure is dementia. There are several Chinese translations for this term. The most commonly used name and most widely understood, ‘痴呆症’ in Chinese, was perceived to have a ‘discriminatory tone’ and easily made people with dementia feel stigmatised. 40 The participants suggested using the less common term ‘失智症’ to diminish stigmatisation. We embraced this suggestion with the aim of reducing stigma, aligning with the perspective of some Chinese researchers.41,42 However, we acknowledge that not everyone may be familiar with the new term and further explanation is required. In addition, the chosen name may not be perfect in completely achieving de-stigmatisation. De-stigmatisation is a gradual process, during which the terminology may evolve to aid in stigma reduction.
The naming of the measure reflects the context and cultural considerations, shedding light on the understanding of palliative care and dementia care within the current context. We propose that naming the measure should not be seen as a definitive endpoint determined by a single decision, but rather as a dynamic process that acknowledges and embraces cultural and contextual changes.
Strengths and limitations
The study followed the precise methodology set by the POS development team for cross-cultural adaptation. Stakeholders became collaborative partners in the study. They played a significant role in guiding decisions to ensure the study’s outcomes were more likely to benefit patients and the wider community. We purposefully selected participants from three nursing homes located in different cities to enhance geographical and care experience diversity. Although the Chinese IPOS-Dem was tested with nursing home staff, it is likely to be relevant in broader settings. The relatively small sample size in the cognitive interviewing phase needs to be acknowledged. Nevertheless, it’s worth noting that this sample size was aligned with the guidance provided by the POS development team 13 and wider research.21,43 –45 Given that cognitive interviewing yields rich data, it’s not uncommon to have small sample sizes in such studies.46 –48
Conclusion
The IPOS-Dem was translated and culturally adapted for Chinese. This study proved essential in refining the translation of IPOS-Dem to ensure the interpretation of and potential responses to each item by Chinese users in Chinese contexts reflect the original English IPOS-Dem item’s meaning. This study presents the first person-centred outcome measure for the substantial population of individuals with dementia in China, offering the potential for improved care and outcomes for this population. Education and training are required to improve the use of IPOS-Dem.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163251347826 – Supplemental material for Translation and cross-cultural adaptation of Integrated Palliative Care Outcome Scale for Dementia
Supplemental material, sj-docx-1-pmj-10.1177_02692163251347826 for Translation and cross-cultural adaptation of Integrated Palliative Care Outcome Scale for Dementia by Linghui Chen, Katherine E Sleeman, Huichan Huang, Yihan Mo, Andy Bradshaw and Clare Ellis-Smith in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank all stakeholders involved in this study and all staff at the participating site for supporting the study. The authors thank peers at Cicely Saunders Institute of Palliative Care, Policy and Rehabilitation for their support and suggestions on conducting the study and arranging the findings: Wilailak Sakharang (PhD student), Dr. Yuxin Zhou, Xiamin Lu (Master student).
Authorship
LC planned the study, administered the project, performed the data collection and analysis and wrote the paper. KES supervised the data collection and analysis and revised the paper. HH contributed to data access and analysis and revised the paper. YM contributed to data analysis and revised the paper. AB supervised the data collection and analysis. CES administered the project, supervised the data collection and analysis and revised the paper.
Data management and sharing
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Linghui Chen is funded by PGR International Studentship by King’s College London (21140830). Katherine E Sleeman is the Laing Galazka Chair in Palliative Care at King’s College London, funded by an endowment from Cicely Saunders International and the Kirby Laing Foundation. Yihan Mo is supported by King’s College London and China Scholarship Council (K-CSC-202106370016).
Ethical approval
The study was approved by the King’s College London PNM Research Ethics Panel (LRS/DP-22/23-35633). Site permission was obtained. Informed consent was obtained from all participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.